




 , Ana Carolina A. CARVALHO 2,†, Marilia A. CORREIA 3,†, Breno Q. FARAH 4,†, Raphael M. RITTI-DIAS 5,†, Aline M. GERAGE 1,†
, Ana Carolina A. CARVALHO 2,†, Marilia A. CORREIA 3,†, Breno Q. FARAH 4,†, Raphael M. RITTI-DIAS 5,†, Aline M. GERAGE 1,†1 Post-graduate Program in Physical Education, Federal University of Santa Catarina, 88040-001 Florianópolis (SC), Brazil
2 Sports Center, Federal University of Santa Catarina, 88040-001 Florianópolis (SC), Brazil
3 Post-graduate Program in Medicine, Universidade Nove de Julho, 01525-000 São Paulo (SP), Brazil
4 Post-graduate Program in Physical Education, Federal University of Pernambuco, 52171-900 Recife (PE), Brazil
5 Post-graduate Program in Rehabilitation Sciences, Universidade Nove de Julho, 01525-000 São Paulo (SP), Brazil
†These authors contributed equally.
Abstract
Background: This study aimed to identify the blood pressure (BP)
responses during different types of isometric exercises (IE) in adults and to
evaluate whether BP responses according to IE is influenced by the
characteristics of participants and exercise protocols. Methods: The
search was conducted in PubMed, Cochrane Central, SPORTDiscus, and LILACS
databases in June 2020. Random effects models with a 95% confidence interval and
p
Keywords
- physical exercise
- acute pressure response
- cardiovascular safety
Handgrip strength has been considered a marker of general strength due to positive association with lower limb strength [1] and also has been associated with several health outcomes as mortality [2] health-related quality of life [3] and cognitive performance [4] in clinical populations. In addition, it has been used as an indicator of muscle strength in intervention studies in different populations [5, 6].
Otherwise, the isometric handgrip training has been used to improve cardiovascular health [7, 8, 9], given the reduction in blood pressure (BP) and improvement in endothelial function after a few weeks of intervention. The most commonly used handgrip protocol consists of four two-minute sets of contractions at 30% of maximal voluntary contraction (MVC) with a recovery interval of one to four minutes [9, 10, 11]. This modality of exercise appears to be safe from a cardiovascular point of view [12, 13], but there is no clarity about the magnitude of BP increase identified during its performance.
In addition, lower limb isometric exercises, involving larger muscle masses, have also been shown to be effective for chronic BP reduction [14, 15, 16]. However, the BP responses during these modalities of isometric exercise (IE) are unclear. Therefore, there are no recommendations for their adoption as a safe antihypertensive strategy.
Regarding the characteristics of the exercise protocol, greater muscle mass [17, 18], intensity [19, 20], frequency, and duration of contraction [21] seem to promote greater increases on the BP response during dynamic strength exercise. However, the influence of these factors on BP responses to IE still needs to be confirmed.
Moreover, the influence of subjects’ personal characteristics on acute BP responses to IE also needs to be investigated, trying to identify which groups of subjects would be at increased risk of acute events. Some studies show that men and older individuals present greater BP responses to IE compared to their pairs [22, 23, 17] while others have observed no difference [18].
Although isometric handgrip has recently been included as a complementary non-pharmacological strategy for the prevention and treatment of hypertension [24, 25, 26], there is still reluctance by international organizations to add this exercise modality in exercise guidelines to the same extent as dynamic resistance exercise [13, 27], since its cardiovascular safety is not yet well established, especially considering other exercises involving larger muscle mass.
In this context, to the best of our knowledge, there are no review studies that evidence the BP responses during the execution of different types of IE in adults. Thus, this systematic review with meta-analysis aimed to identify the BP responses during different types of IE in isolation and compared to handgrip in adults, and to identify such responses according to the characteristics of participants and exercise protocols.
This study protocol was previously registered with PROSPERO (CRD42020190823) and followed PRISMA guidelines [28].
Studies with any experimental design (randomized or not and controlled or not)
were included, respecting the eligibility criteria established according to the
acronym PICO (Population, Intervention, Comparator, and Outcome) [28]. Inclusion
criteria were: adult participants (
Exclusion criteria were: adults with any comorbidity (except hypertension) or specific condition (e.g., pregnant women); studies with other interventions associated with IE; investigating the effects of medications; with IE performed after or randomly with other exercise modalities; that performed several stress tests on the same day before IE (without randomization), and with incremental testing; comparing IE with another exercise modality, without having a separate group for IE; with SBP and/or DBP measurements only after the exercise and only mean BP data.
The search for articles was conducted in the PubMed, Cochrane Central, SPORTDiscus, and LILACS databases in the month of June 2020. The search strategy, used for all databases, is available in Supplementary Material 1.
The EndNote® X9.3.3 software (Philadelphia, PA, USA) was used to manage references and remove duplicates. First, the selection of articles was based on title and abstract reading by two independent researchers (GTB. and JCC.). The next step consisted of reading the full texts and selecting the studies according to eligibility criteria. In both steps, if there were disagreements between researchers, a third researcher (AMG) was consulted to reach a consensus.
Data extraction was performed by the same researchers, in a standardized and independent way. The following information regarding the participants was extracted: number of participants, percentage of women in the sample, age, ethnicity/race, training status, body mass, body mass index (BMI), and BP level classification. For the BP level classification, we considered the report of each study and not the resting BP value. If the study did not clearly report this information, we considered it as “not reported”. For the exercise protocol, it was considered: number and duration of sets, interval between sets, and intensity of effort. Regarding the outcome of the studies, the following were considered: SBP and DBP before (rest measurement) and during exercise or the difference between the two moments (delta), with mean and dispersion measures.
The risk of bias analysis was feasible only for the studies that compared handgrip with other IE, due to the various types of study designs included in this systematic review. In this case, the risk of bias was assessed by the same researchers who screened the studies and extracted the data, according to the Cochrane Handbook for Systematic Reviews of Interventions [29], considering random sequence generation, allocation concealment, blinding of participants and professionals, blinding of outcome assessors, incomplete outcomes, selective outcome reporting, and BP measurement method (other bias). It was classified as high, unclear or low risk [30]. Also, the criteria were classified as not applicable when it was not possible to be assessed due to the study design.
All descriptive data are presented as mean and standard deviation (SD). Delta
values for BP were calculated (BP during exercise - baseline BP). The overall
effect for each type of exercise and the subgroup analyses were calculated from
the mean difference between the pre-exercise BP and the BP during exercise. The
comparison of BP between the IE types was performed using the mean values for
each exercise type. Also, the effect of the comparison between the handgrip
exercise and other exercise types was calculated from the mean difference in BP
change between them. The SD of change was calculated from the pre-exercise and
during-exercise SD values, adopting a correlation coefficient of 0.5.
Meta-analyses were calculated using random effects models. Statistical
heterogeneity between studies was assessed by the I
Initially, 3201 articles were found (Pubmed = 2170, Cochrane = 381, Lilacs = 237, and SPORTDiscus = 413) and 102 studies were, finally, included in the systematic review. Of these, seven were included in the meta-analysis comparing handgrip with others IE (Fig. 1).
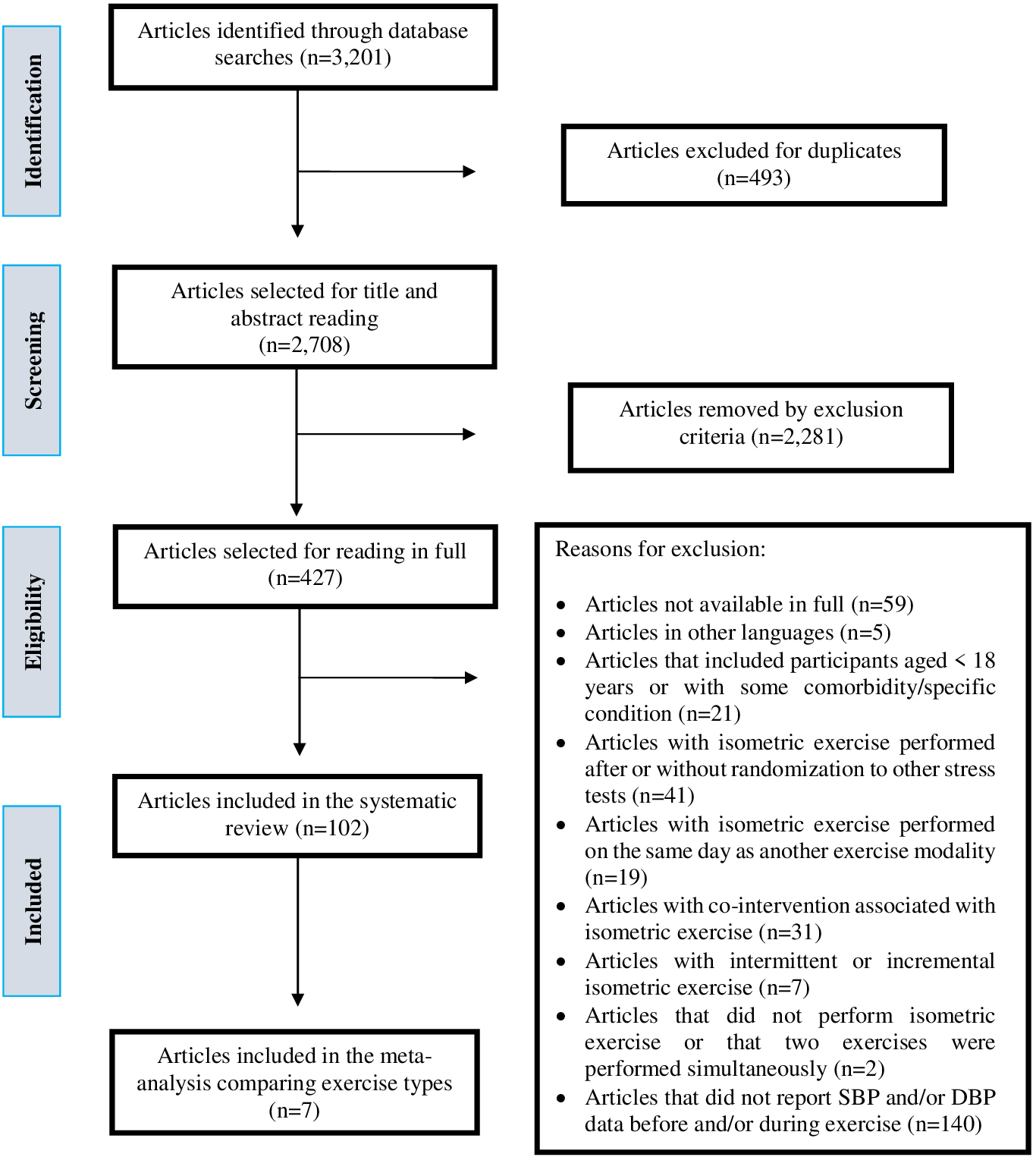 Fig. 1.
Fig. 1.Flowchart of the different steps of the systematic review.
In summary, the studies of this systematic review included 12 types of IE and some of them evaluated more than one type of IE. Among these studies, the vast majority (76.5%) performed the handgrip, followed by knee extension (13.7%) (Table 1, Ref. [8, 13, 18, 19, 20, 22, 23, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88, 89, 90, 91, 92, 93, 94, 95, 96, 97, 98, 99, 100, 101, 102, 103, 104, 105, 106, 107, 108, 109, 110, 111, 112, 113, 114, 115, 116, 117, 118, 119, 120, 121, 122, 123, 124, 125]).
| Author and year | Country of origin | Modality | Sample (%women) | Age (years) | Ethnicity/race | Trainability status | Body mass (kg) | BMI (kg/m |
BP level classification |
| Almeida et al. (2021) [8] | Brazil | Handgrip | 14.0 (79.0%) | 24.5 |
NR | Sedentary | NR | 22.8 |
Normotensive |
| 14.0 (50.0%) | 26.6 |
24.2 |
|||||||
| Aoki et al. (1983) [31] | Japan | Handgrip | 18.0 (0.0%) | 38.7 |
Japanese | NR | 64.1 |
NR | Normotensive |
| 50.0 (0.0%) | 40.5 |
61.6 |
Hypertensive | ||||||
| Auerbach et al. (2000) [32] | Israel | Whole-body isometric exercise | 18.0 (0.0%) | 51.1 |
NR | NR | 80.5 |
NR | Normotensive |
| Bakke et al. (2007) [33] | Norway | Handgrip | 11.0 (64.0%) | 24.2 |
NR | NR | 66.6 |
23.3 |
Normotensive |
| 11.0 (36.0%) | 62.7 |
77.4 |
25.0 |
||||||
| Bakke et al. (2009) [34] | Norway | Handgrip | 9.0 (33.0%) | 23.6 |
NR | NR | 68.0 |
22.5 |
Normotensive |
| Balmain et al. (2016) [35] | Australia | Handgrip | 19.0 (0.0%) | 23.0 |
NR | NR | 70.9 |
NR | Normotensive |
| Ben-Ari et al. (1992) [36] | Israel | Two-hand pulling | 25.0 (0.0%) | 47.0 |
NR | Untrained | NR | NR | Normotensive |
| Bentley and Thomas (2018) [37] | Canada | Handgrip | 20.0 (100.0%) | 57.7 |
NR | Moderately active | NR | 26.9 |
Normotensive |
| Borghi et al. (1988) [38] | Italy | Handgrip | 16.0 (37.5%) | NR | NR | NR | NR | NR | Normotensive |
| Bosisio et al. (1980) [39] | Italy | Handgrip | 8.0 (0.0%) | NR | NR | Trained (non-athlete) | NR | NR | Normotensive |
| Cottone et al. (1998) [40] | Italy | Handgrip | 12.0 (42.0%) | 38.0 |
NR | NR | NR | 25.7 |
Normotensive |
| 15.0 (47.0%) | 43.0 |
26.0 |
Hypertensive | ||||||
| Davies and Starkie (1985) [41] | England | Elbow flexion | 11.0 (0.0%) | 21.5 |
NR | NR | NR | NR | Normotensive |
| Plantar flexion | |||||||||
| Da Silva et al. (2013) [20] | Brazil | Leg press (45°) | AI: 8.0 (0.0%) | 30.6 |
NR | Physically active | 74.4 |
24.7 |
Normotensive |
| MI: 8.0 (0.0%) | 31.6 |
72.3 |
24.2 |
||||||
| BI: 8.0 (0.0%) | 27.5 |
74.2 |
25.5 |
||||||
| Dias and Polito (2015) [42] | Brazil | Squat | 19.0 (53.0%) | 26.8 |
NR | Sedentary | 72.3 |
24.7 |
Normotensive |
| Ehsani et al. (1981) [43] | United States | Handgrip | 14.0 (14.0%) | NR | NR | NR | NR | NR | Normotensive |
| Ehsani et al. (1982) [44] | United States | Handgrip | 12.0 (8.0%) | NR | NR | NR | NR | NR | Normotensive |
| Ferguson and Brown (1997) [45] | England | Handgrip | 5.0 (0.0%) | 22.0 |
NR | Athlete | NR | NR | NR |
| 10.0 (0.0%) | 20.0 |
Sedentary | |||||||
| Fu et al. (1981) [46] | Japan | Handgrip | 20.0 (NR) | 54.9 |
NR | NR | NR | NR | Normotensive |
| 35.0 (34.0%) | 56.3 |
Hypertensive | |||||||
| Fu et al. (2002) [47] | United States | Handgrip | 5.0 (0.0%) | 41.0 |
NR | NR | 84.0 |
NR | Normotensive |
| Fujisawa et al. (1996) [48] | Japan | One-knee extension | 7.0 (0.0%) | 24.0 |
NR | NR | 63.9 |
NR | Normotensive |
| Gois et al. (2020) [49] | Brazil | Handgrip | 15.0 (NR) | 53.0 |
NR | Insufficiently active | 75.0 |
25.0 |
Normotensive |
| Goldstein and Shapiro (1988) [50] | United States | Handgrip | 20.0 (0.0%) | 20.4 |
NR | NR | NR | NR | Normotensive |
| Goldstraw and Warren (1985) [51] | England | Handgrip | 12.0 (NR) | 30.0 |
NR | NR | NR | NR | NR |
| 12.0 (NR) | 73.0 |
||||||||
| Goulopoulou et al. (2010) [52] | United States | Handgrip | 23.0 (43.5%) | 22.0 |
NR | Physically active | 76.9 |
26.0 |
Normotensive |
| Graafsma et al. (1989) [53] | Netherlands | Handgrip | 10.0 (50.0%) | 42.6 |
NR | NR | NR | 23.3 |
Normotensive |
| 13.0 (46.0%) | 39.1 |
24.1 |
Hypertensive | ||||||
| Greaney et al. (2013) [18] | United States | Handgrip | 10.0 (0.0%) | 24.0 |
NR | NR | 75.0 |
23.2 |
Normotensive |
| 9.0 (0.0%) | 59.0 |
87.0 |
28.5 |
||||||
| Greaney et al. (2014) [54] | United States | Handgrip | 11.0 (45.5%) | 23.0 |
NR | Physically active | 71.0 |
23.0 |
Normotensive |
| 12.0 (41.7%) | 60.0 |
81.0 |
26.2 |
||||||
| Greaney et al. (2015) [55] | United States | Handgrip | 23.0 (NR) | 60.0 |
NR | NR | NR | 26.7 |
Normotensive |
| 15.0 (NR) | 63.0 |
27.6 |
Hypertensive | ||||||
| Grossman et al. (1989) [56] | United States | Handgrip | 18.0 (33.0%) | 53.0 |
NR | NR | NR | NR | Hypertensive |
| Hallman et al. (2011) [57] | Sweden | Handgrip | 21.0 (90.5%) | 40.8 |
NR | NR | NR | 24.3 |
Normotensive |
| Heffernan et al. (2005) [58] | United States | Handgrip | 10.0 (50.0%) | 27.5 |
NR | Sedentary/moderately active | 75.3 |
26.6 |
Normotensive |
| Heng et al. (1988) [59] | United States | Handgrip | 12.0 (0.0%) | 29.0 |
NR | NR | 67.0 |
NR | Normotensive |
| Hickey et al. (1993) [60] | United States | Two-knee extension | 8.0 (0.0%) | 24.0 |
NR | Trained | 77.6 |
NR | Normotensive |
| Hirasawa et al. (2016) [61] | Japan | One-knee extension | 12.0 (67.0%) | 21.0 |
NR | NR | 58.0 |
NR | Normotensive |
| Huikuri et al. (1986) [62] | Finland | Handgrip | 13.0 (54.0%) | 25.0 |
NR | NR | NR | NR | Normotensive |
| Ichinose et al. (2006) [63] | Japan | Handgrip | 13.0 (23.0%) | 23.0 |
NR | NR | 62.4 |
NR | Normotensive |
| Iellamo et al. (1993) [64] | Italy | Handgrip | 10.0 (0.0%) | NR | NR | NR | NR | NR | Normotensive |
| Iellamo et al. (1999) [65] | Italy | One-knee extension | 11.0 (0.0%) | 26.0 |
NR | Untrained | NR | NR | Normotensive |
| Incognito et al. (2018) [66] | Canada | Handgrip | 29.0 (0.0%) | 24.0 |
NR | NR | NR | 24.0 |
Normotensive |
| Kadetoff and Kosek (2007) [67] | Sweden | One-knee extension | 17.0 (100.0%) | 37.4 |
NR | NR | NR | NR | Normotensive |
| Kadetoff and Kosek (2010) [68] | Sweden | Two-knee extension | 16.0 (100.0%) | 38.3 |
NR | NR | NR | NR | Normotensive |
| Kagaya and Homma (1997) [69] | Japan | Handgrip | 7.0 (100.0%) | 22.3 |
NR | Physically active | 54.4 |
NR | Normotensive |
| Kahn et al. (1997) [70] | France | Handgrip | 12.0 (0.0%) | 23.6 |
NR | NR | 73.0 |
NR | Normotensive |
| Kalfon et al. (2015) [71] | United States | Handgrip | 16.0 (0.0%) | 23.7 |
NR | Sedentary | 86.8 |
29.3 |
Normotensive |
| Kamiya et al. (2001) [72] | Japan | Handgrip | 22.0 (0.0%) | 22.0 |
NR | NR | 65.0 |
NR | Normotensive |
| Koletsos et al. (2019) [73] | Greece | Handgrip | 28.0 (42.9%) | 43.8 |
NR | Minimally and moderately active | NR | 26.6 |
Normotensive |
| 27.0 (40.7%) | 47.5 |
27.6 |
Hypertensive (masked) | ||||||
| 31.0 (48.4%) | 47.6 |
26.8 |
Hypertensive (true) | ||||||
| Kordi et al. (2012) [74] | Iran | Handgrip | 20.0 (60.0%) | 19.3 |
NR | NR | NR | NR | NR |
| Koutnik et al. (2014) [75] | United States | Handgrip | 20.0 (0.0%) | 22.1 |
NR | Not regularly active | 84.7 |
27.1 |
Normotensive |
| Kramer et al. (1983) [76] | Germany | Handgrip (unilateral e (bilateral)) | 4.0 (0.0%) | NR | NR | NR | NR | NR | NR |
| Lewis et al. (1985) [77] | United States | Handgrip | 6.0 (0.0%) | 27.0 |
NR | NR | 74.60 |
NR | Normotensive |
| Two-knee extension | |||||||||
| Lindquist et al. (1973) [78] | United States | Handgrip | 21.0 (0.0%) | 32.0 |
NR | NR | NR | NR | Normotensive |
| Lykidis et al. (2008) [79] | England | Handgrip | 9.0 (44.4%) | 21.8 |
NR | Physically active | NR | NR | NR |
| Maiorano et al. (1989) [80] | Italy | Handgrip | 50.0 (0.0%) | 19.3 |
NR | Trained and | 68.88 |
22.92 |
Normotensive |
| 50.0 (0.0%) | 19.2 |
untrained | 68.66 |
22.99 |
|||||
| Majahalme et al. (1997) [81] | Finland | Handgrip | 28.0 (0.0%) | 39.5 |
NR | NR | 81.7 |
25.4 |
Normotensive |
| 14.0 (0.0%) | 40.7 |
87.6 |
26.9 |
Hypertensive (borderline) | |||||
| 24.0 (0.0%) | 40.0 |
81.9 |
26.5 |
Hypertensive (mild) | |||||
| Mäkinen et al. (2008) [82] | Finland | Handgrip | 10.0 (0.0%) | 22.5 |
NR | NR | 72.4 |
22.3 |
Normotensive |
| Matthews et al. (2017) [83] | United States | Handgrip | 16.0 (100.0%) | 22.0 |
NR | - | NR | 22.0 |
Normotensive |
| 16.0 (100.0%) | 22.0 |
- | 22.0 |
||||||
| McCoy et al. (1991) [84] | United States | Handgrip | 9.0 (0.0%) | NR | NR | NR | 71.5 |
NR | NR |
| McDermott et al. (1974) [85] | United States | Handgrip | 10.0 (0.0%) | 25.3 |
NR | Untrained | 78.4 |
NR | Normotensive |
| 12.0 (0.0%) | 46.8 |
80.9 |
|||||||
| Metelitsina et al. (2010) [86] | United States | Handgrip | 19.0 (63.2%) | 64.7 |
White - 18 (94.7%) | NR | NR | NR | Normotensive/Hypertensive |
| Mizushige et al. (1997) [87] | Japan | Handgrip | 14.0 (42.9%) | 59.0 |
NR | NR | NR | NR | Normotensive |
| Momen et al. (2010) [88] | United States | Handgrip | 11.0 (0.0%) | NR | NR | NR | NR | 23.0 |
Normotensive |
| 11.0 (100.0%) | 22.0 |
||||||||
| Mortensen et al. (2016) [89] | England | Elbow flexion (unilateral) | 75.0 (49.3%) | 38.8 |
NR | NR | NR | 25.1 |
Normotensive |
| Muller et al. (2011) [90] | United States | Handgrip | 10.0 (50.0%) | 25.0 |
NR | NR | 73.0 |
NR | Normotensive |
| Nagle et al. (1988) [91] | United States | Handgrip | 10.0 (0.0%) | 24.0 |
NR | Untrained | 71.0 |
NR | Normotensive |
| Two-knee extension | |||||||||
| Deadlift | |||||||||
| Nakamura et al. (2005) [92] | Japan | Elbow flexion (unilateral) | 8.0 (0.0%) | 63.0 |
NR | NR | NR | 23.1 |
Normotensive/Hypertensive |
| Notay et al. (2018) [93] | Canada | Handgrip | 200.0 (54.5%) | 22.0 |
Caucasian (non-Hispanic) = 192 | Recreationally active | 69.0 |
23.0 |
Normotensive |
| Hispanic = 5 | |||||||||
| Black = 3 | |||||||||
| Notay et al. (2018b) [94] | Canada | Handgrip | 66.0 (0.0%) | 22.0 |
NR | Recreationally active | 77.0 |
24.0 |
Normotensive |
| 66.0 (100.0%) | 21.0 |
63.0 |
23.0 |
||||||
| Nyberg (1976) [95] | Australia | Handgrip | 10.0 (0.0%) | 30.6 |
NR | NR | NR | NR | Normotensive |
| 9.0 (100.0%) | 30.4 |
Hypertensive (untreated) | |||||||
| 9.0 (0.0%) | 45.3 |
Hypertensive (treated) | |||||||
| 12.0 (100.0%) | 46.8 |
||||||||
| 12.0 (0.0%) | 46.9 |
||||||||
| 5.0 (100.0%) | 48.4 |
||||||||
| Park et al. (2012) [96] | United States | Handgrip | 12.0 (33.3%) | 28.9 |
Caucasia= 6 | NR | 62.8 |
21.7 |
Normotensive |
| 12.0 (41.7%) | 32.3 |
Hispanic= 3 | 82.9 |
27.4 |
|||||
| Asian= 3 | |||||||||
| Caucasian= 7 | |||||||||
| Hispanic = 4 | |||||||||
| Asian= 1 | |||||||||
| Parmar et al. (2018) [23] | Canada | Handgrip | 11.0 (0.0%) | 24.0 |
NR | Physically active | 75.0 |
23.7 |
Normotensive |
| 9.0 (100.0%) | 22.0 |
61.0 |
22.0 |
||||||
| 10.0 (100.0%) | 22.0 |
61.0 |
22.3 |
||||||
| Pepin et al. (1996) [97] | United States | Handgrip | 25.0 (64.0%) | 34.3 |
NR | NR | NR | NR | NR |
| Petrosfsky and Laymon (2002) [98] | United States | Handgrip | 20–30 years = 15.0 (NR) | NR | NR | Untrained | 81.8 |
NR | NR |
| Two-knee extension | 31–40 years = 10.0 (NR) | 83.4 |
|||||||
| 41–50 years = 12.0 (NR) | 83.5 |
||||||||
| 51–65 years = 13.0 (NR) | 85.1 |
||||||||
| Piccolino et al. (2018) [99] | Italy | Handgrip | 25.0 (8.0%) | 43.2 |
Caucasian | NR | NR | NR | Normotensive |
| Plotnikov et al. (2002) [100] | Russia | Handgrip | 48.0 (100.0%) | NR | NR | NR | NR | NR | Normotensive |
| Torso effort | |||||||||
| Quarry and Spodick (1974) [101] | United States | Handgrip | 10.0 (0.0%) | NR | NR | Physically active | NR | NR | Normotensive |
| Riendl et al. (1977) [102] | United States | Finger adduction | 10.0 (0.0%) | 25.1 |
NR | Untrained | NR | NR | Normotensive |
| Plantar flexion | |||||||||
| Sagiv et al. (1985) [103] | United States | Handgrip | 10.0 (0.0%) | 52.0 |
NR | NR | NR | NR | Normotensive |
| Deadlift | |||||||||
| Sagiv et al. (1988) [104] | Israel | Deadlift | 10.0 (0.0%) | 28.0 |
NR | Physically active | 82.0 |
NR | Normotensive |
| 10.0 (0.0%) | 67.0 |
80.0 |
|||||||
| Sagiv et al. (1988b) [105] | Israel | Deadlift | 25.0 (0.0%) | 27.4 |
NR | Physically active | 82.3 |
NR | Normotensive |
| 25.0 (0.0%) | 51.0 |
79.5 |
|||||||
| 25.0 (0.0%) | 67.8 |
80.0 |
|||||||
| Sagiv et al. (1988c) [106] | Israel | Handgrip | 10.0 (0.0%) | 28.0 |
NR | Physically active | 81.7 |
NR | Normotensive |
| Deadlift | 10.0 (0.0%) | 67.0 |
79.5 |
||||||
| Sagiv et al. (1995) [107] | United States | Handgrip | 5.0 (0.0%) | 33.0 |
NR | Physically active | NR | NR | Normotensive |
| Deadlift | |||||||||
| Sagiv et al. (2008) [108] | Israel | Deadlift | 15.0 (0.0%) | 40.0 |
NR | NR | 80.5 |
NR | Normotensive |
| Samora et al. (2019) [109] | Brazil | Handgrip | 20.0 (0.0%) | 21.0 |
NR | Physically active | 78.0 |
24.9 |
Normotensive |
| 20.0 (100.0%) | 23.0 |
61.4 |
23.0 |
||||||
| Seals (1989) [110] | United States | Handgrip (unilateral and bilateral) | 9.0 (33.0%) | NR | NR | NR | NR | NR | Normotensive |
| Seals et al. (1983) [111] | United States | Elbow extension | 6.0 (0.0%) | NR | NR | Untrained and trained (untrained and trained members after a training period) | Untrained | NR | Normotensive |
| One-knee extension | 72.7 |
||||||||
| 71.7 |
|||||||||
| Seals et al. (1985) [112] | United States | Handgrip | 10.0 (40.0%) | 62.0 |
NR | Untrained and trained | Before: 74.0 |
NR | Normotensive |
| Somani et al. (2018) [22] | Canada and England | Handgrip | 26.0 (50.0%) | 25.0 |
NR | Recreationally active/non-active | 72.0 |
24.0 |
Prehypertensive/Normotensive |
| Two-knee extension | 20.0 (50.0%) | 22.0 |
NR | 73.0 |
25.0 | ||||
| Stewart et al. (2007) [113] | United States | Handgrip | 16.0 (56.3%) | 24.5 |
NR | NR | 70.0 |
24.0 |
Normotensive |
| Tan et al. (2013) [114] | United States | Handgrip | 11.0 (45.5%) | 25.0 |
NR | NR | NR | NR | Normotensive |
| Taylor et al. (2017) [115] | England | Wall squat | 25.0 (0.0%) | 44.6 |
NR | Physically inactive | 89.1 |
NR | Prehypertensive |
| Turley (2005) [116] | United States | Handgrip | 35.0 (0.0%) | 20.2 |
NR | Untrained | 78.1 |
24.6 |
Normotensive |
| 35.0 (100.0%) | 19.9 |
62.8 |
23.0 |
||||||
| Umeda et al. (2009) [117] | United States | Handgrip | 23.0 (100.0%) | 20.0 |
NR | Physically active | NR | NR | Normotensive |
| Umeda et al. (2015) [118] | United States | Handgrip | 14.0 (36.0%) | 22.1 |
African-Americans | Recreationally active | NR | 26.02 |
Normotensive |
| 14.0 (36.0%) | 21.9 |
White (non-Hispanic) | 24.06 |
||||||
| Van Huysduynen et al. (2004) [119] | Netherlands | Handgrip | 41.0 (0.0%) | 32.6 |
NR | Untrained/Trained | NR | NR | Normotensive |
| Vaz et al. (1993) [120] | India | Handgrip | 8.0 (NR) | NR | NR | NR | NR | NR | Normotensive |
| Vianna et al. (2012) [121] | Brazil | Handgrip | 8.0 (0.0%) | 25.0 |
NR | NR | 78.0 |
NR | Normotensive |
| Vitcenda et al. (1990) [122] | United States | Deadlift | 16.0 (0.0%) | 27.0 |
NR | Untrained | 75.0 |
NR | NR |
| Weippert et al. (2013) [123] | Germany | Leg press | 23.0 (0.0%) | 25.5 |
NR | Physically active | 84.0 |
24.3 |
Normotensive |
| Wiles et al. (2018) [13] | England | Wall squat | 26.0 (0.0%) | 45.0 |
NR | Physically inactive | 89.7 |
NR | Hypertensive |
| Williams (1991) [124] | United States | Handgrip | 6.0 (0.0%) | 26.0 |
NR | NR | NR | NR | NR |
| Two-knee extension | |||||||||
| Wright et al. (1999) [125] | United States | One-knee extension | 15.0 (0.0%) | 21.6 |
African-American | NR | 82.5 |
NR | Normotensive |
| 15.0 (100.0%) | 27.7 |
Asian American | 62.1 |
||||||
| 15.0 (0.0%) | 27.8 |
Caucasian American | 69.0 |
||||||
| 15.0 (100.0%) | 27.0 |
54.7 |
|||||||
| 15.0 (0.0%) | 26.4 |
83.2 |
|||||||
| 15 (100%) | 25.2 |
60.0 |
|||||||
| Yamaji et al. (1983) [19] | Japan | Elbow flexion | 20.0 (0.0%) | 20.4 |
NR | NR/Trained | 64.8 |
NR | Normotensive |
| One-knee extension | |||||||||
| Note: Data presented as mean | |||||||||
The total number of participants was 2695, with a mean age ranging from 19.2 to 73.0 years. Most of the studies included only men (47.1%). More than half of the studies (56.9%) did not report the trainability status of the participants, and among the studies that reported this information, only 18.2% included trained participants and/or athletes.
Regarding BP level classification, 76.5% included only normotensive participants. In addition, only eight studies reported information regarding the number of users of antihypertensive medications. Regarding BP measurement protocols during exercise, the auscultatory, automatic, and finger photoplethysmography (Finometer) methods presented similar frequencies in the studies (30%). Concerning the moment of BP measurement, 66 studies (64.7%) performed it at the end of the exercise contraction, with 21 studies reporting that this measurement was performed in the final minute or final seconds of exercise, but it is not clear at what exact time this was done. In the other studies, the BP measurement was taken at different moments during exercise.
Most studies used a single set (72.6%) and performed sets lasting up to 180
seconds (74%). Regarding exercise intensity, 61.9% of the studies performed
sets with low intensities (i.e.,
All the details regarding the BP responses to the handgrip or other IE are shown in the Supplementary Material 3, 4, 5 and 6.
Table 2 shows the overall effects for each type of IE on the BP response. The
greater increases in SBP were +64.5 mmHg (p
| Type of exercise | N | Mean difference | Standard error | Variance | 95% CI | Z-value | p* | I |
p |
|---|---|---|---|---|---|---|---|---|---|
| SBP (mmHg) | |||||||||
| Handgrip | 127 | +33.4 | 1.8 | 3.2 | 29.9–36.9 | 18.6 | 0.0 | 99.2 | 0.0 |
| Elbow flexion | 8 | +47.3 | 12.8 | 163.7 | 22.2–72.4 | 3.7 | 0.0 | 99.1 | 0.0 |
| One-knee extension | 17 | +34.3 | 2.1 | 4.3 | 30.2–38.3 | 16.4 | 0.0 | 84.7 | 0.0 |
| Two-knee extension | 11 | +64.5 | 5.9 | 35.2 | 52.8–76.1 | 10.9 | 0.0 | 96.1 | 0.0 |
| Leg press | 4 | +51.5 | 11.0 | 121.1 | 29.9–73.0 | 4.7 | 0.0 | 94.7 | 0.0 |
| Squat | 3 | +46.3 | 10.9 | 117.8 | 25.0–67.5 | 4.3 | 0.0 | 97.1 | 0.0 |
| Plantar flexion | 2 | +23.3 | 4.0 | 15.9 | 15.5–31.1 | 5.8 | 0.0 | 53.4 | 0.1 |
| Deadlift | 13 | +61.6 | 2.7 | 7.2 | 56.4–66.9 | 22.9 | 0.0 | 66.4 | 0.0 |
| Torso effort | 3 | +20.8 | 6.9 | 47.8 | 7.2–34.3 | 3.0 | 0.0 | 99.9 | 0.0 |
| DBP (mmHg) | |||||||||
| Handgrip | 112 | +25.1 | 1.0 | 1.1 | 23.0–27.1 | 24.0 | 0.0 | 98.4 | 0.0 |
| Elbow flexion | 8 | +22.4 | 2.7 | 7.6 | 17.0–27.7 | 8.1 | 0.0 | 83.8 | 0.0 |
| One-knee extension | 17 | +26.4 | 1.9 | 3.6 | 22.7–30.1 | 14.0 | 0.0 | 87.3 | 0.0 |
| Two-knee extension | 11 | +52.2 | 5.4 | 29.5 | 41.5–62.8 | 9.6 | 0.0 | 97.3 | 0.0 |
| Leg press | 4 | +34.4 | 8.1 | 66.1 | 18.4–50.3 | 4.2 | 0.0 | 92.2 | 0.0 |
| Squat | 2 | +43.4 | 6.5 | 42.2 | 30.7–56.2 | 6.7 | 0.0 | 94.5 | 0.0 |
| Plantar flexion | 2 | +22.4 | 1.9 | 3.6 | 18.7–26.2 | 11.8 | 0.0 | 0.0 | 0.4 |
| Deadlift | 13 | +34.4 | 1.9 | 3.7 | 30.6–38.1 | 17.8 | 0.0 | 79.0 | 0.0 |
| Torso effort | 3 | +23.8 | 3.2 | 10.4 | 17.5–30.1 | 7.4 | 0.0 | 99.6 | 0.0 |
| Note: Analyses performed with the random effects model. N, number of studies and
subgroups per study analyzed; CI, confidence interval; I | |||||||||
For SBP, the largest differences were found between two-knee extension and torso
effort (–48.6 mmHg; p
Two-knee extension promoted greater increases in SBP (+9.8 mmHg;
p = 0.017; I
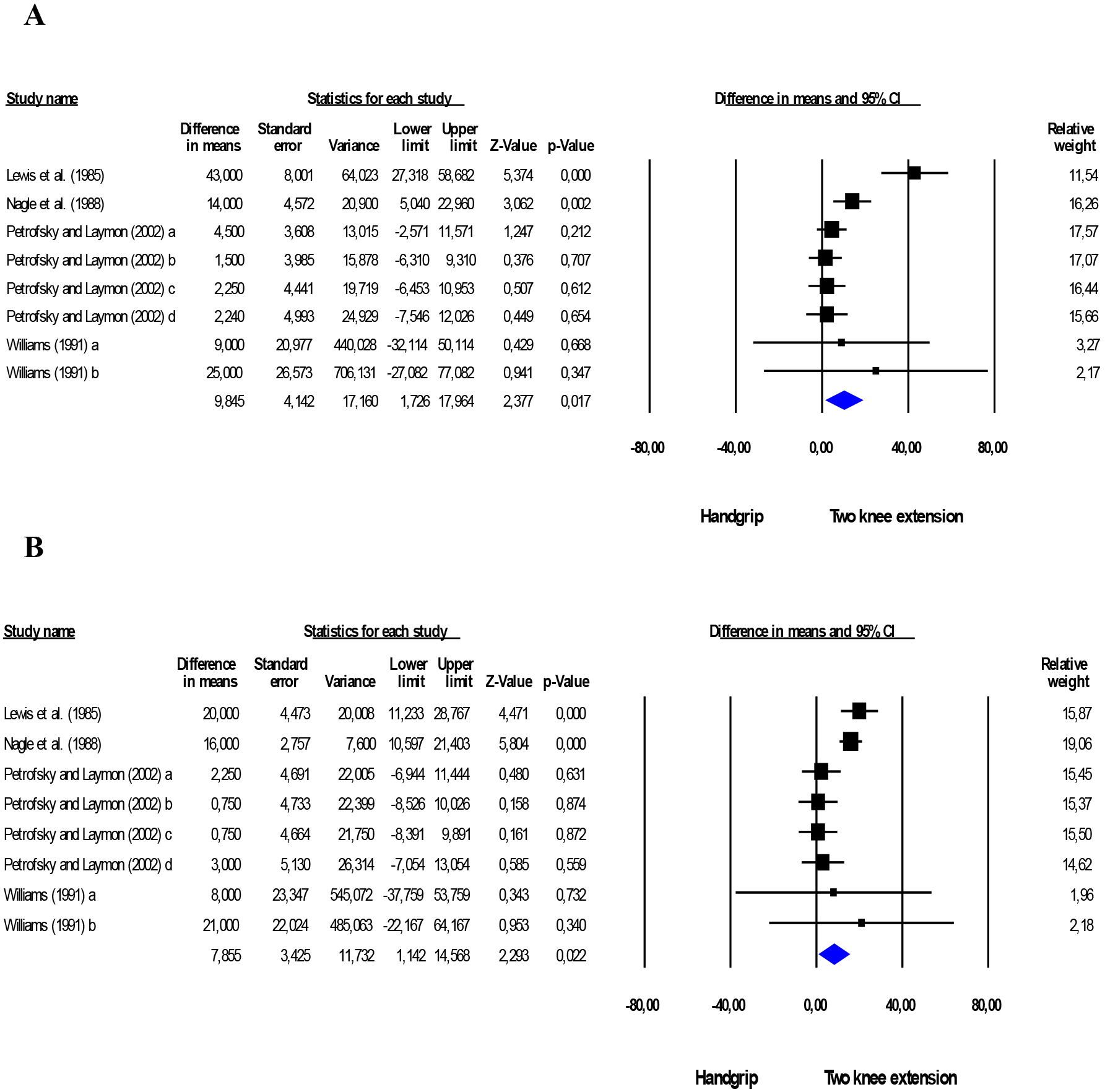 Fig. 2.
Fig. 2.Comparison between isometric handgrip and two-knee extension
exercises. Mean difference in systolic (A) and diastolic (B) BP between
isometric handgrip and two-knee extension exercises. Estimation per study (black
square). Overall estimate from random effects analyses (blue diamond). 95% CI
indicates confidence interval. I
Comparing handgrip and deadlift, greater increases were observed in SBP (+26.8
mmHg; p
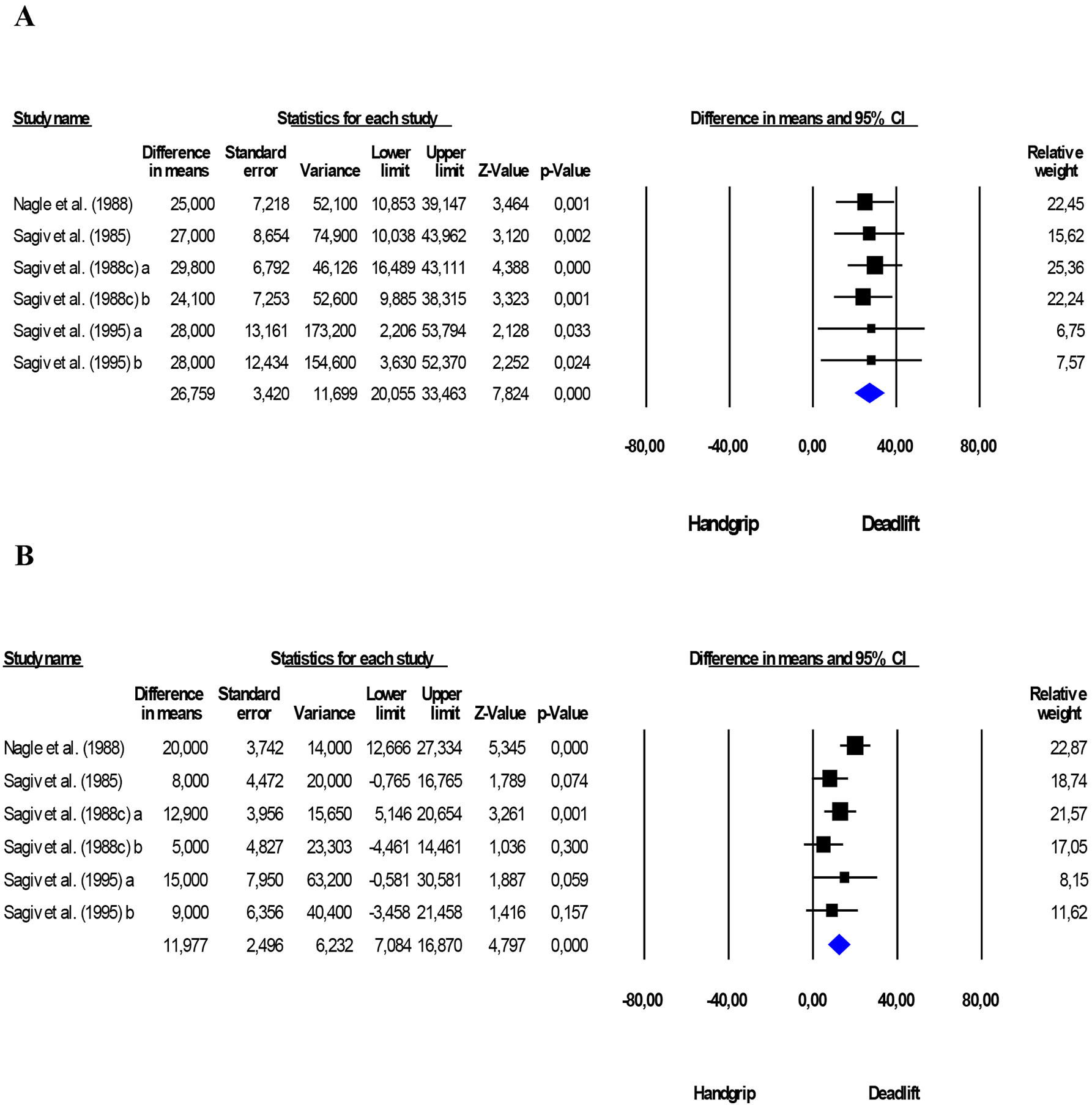 Fig. 3.
Fig. 3.Comparison between isometric handgrip and deadlift
exercises. Mean difference in systolic (A) and diastolic (B) BP between
isometric handgrip and land lift exercises. Estimation per study (black square).
Overall estimate from fixed effects analyses (blue diamond). 95% CI indicates
confidence interval. I
For SBP, men (+34.5 mmHg; p
| Subgroup | N | Mean difference | Standard error | Variance | 95% CI | Z-value | p* | I |
p | |
|---|---|---|---|---|---|---|---|---|---|---|
| SBP (mmHg) | ||||||||||
| Sex | ||||||||||
| Men | 59 | +34.5 | 2.1 | 4.5 | 30.3–38.6 | 16.2 | 0.0 | 94.6 | 0.0 | |
| Women | 14 | +26.1 | 3.9 | 15.2 | 18.4–33.7 | 6.7 | 0.0 | 99.6 | 0.0 | |
| Age | ||||||||||
| Young | 62 | +31.3 | 2.1 | 4.5 | 27.2–35.5 | 14.7 | 0.0 | 95.9 | 0.0 | |
| Middle-aged/elderly | 37 | +41.3 | 2.1 | 4.4 | 37.1–45.4 | 19.6 | 0.0 | 95.0 | 0.0 | |
| BP level classification | ||||||||||
| Non-hypertensive | 95 | +30.7 | 2.1 | 4.3 | 26.7–34.8 | 14.9 | 0.0 | 99.3 | 0.0 | |
| Hypertensive | 13 | +39.6 | 2.2 | 4.7 | 35.3–43.8 | 18.2 | 0.0 | 71.8 | 0.0 | |
| DBP (mmHg) | ||||||||||
| Sex | ||||||||||
| Men | 50 | +26.6 | 3.1 | 9.5 | 20.5–32.6 | 8.6 | 0.0 | 98.4 | 0.0 | |
| Women | 14 | +20.4 | 2.9 | 8.4 | 14.7–26.0 | 7.0 | 0.0 | 99.3 | 0.0 | |
| Age | ||||||||||
| Young | 55 | +23.4 | 1.5 | 2.3 | 20.4–26.3 | 15.4 | 0.0 | 94.7 | 0.0 | |
| Middle-aged/elderly | 36 | +29.6 | 2.6 | 6.6 | 24.6–34.6 | 11.5 | 0.0 | 98.8 | 0.0 | |
| BP level classification | ||||||||||
| Non-hypertensive | 80 | +22.1 | 1.0 | 1.0 | 20.2–24.1 | 22.6 | 0.0 | 97.9 | 0.0 | |
| Hypertensive | 13 | +30.8 | 8.9 | 78.4 | 13.5–48.2 | 3.5 | 0.0 | 99.5 | 0.0 | |
| Note: Analyses performed with the random effects model. N, number of studies and
subgroups per study analyzed; Young, studies that included adults with mean age
up to 40 years; Middle-aged/elderly, studies that included adults with a mean 40
years; Non-Hypertension, studies that classified participants into normotensives
and/or prehypertensive; CI, confidence interval; I | ||||||||||
Higher intensities (
| Subgroup | N | Mean difference | Standard error | Variance | 95% CI | Z-value | p* | I |
p | |
|---|---|---|---|---|---|---|---|---|---|---|
| SBP (mmHg) | ||||||||||
| Intensity | ||||||||||
| 76 | +27.5 | 1.7 | 2.9 | 24.2–30.9 | 16.3 | 0.0 | 98.6 | 0.0 | ||
| 44 | +40.7 | 1.9 | 3.5 | 37.0–44.3 | 21.8 | 0.0 | 92.7 | 0.0 | ||
| 7 | +55.8 | 9.1 | 83.3 | 37.9–73.7 | 6.1 | 0.0 | 92.9 | 0.0 | ||
| Duration | ||||||||||
| 45 | +35.5 | 2.6 | 6.8 | 30.4–40.7 | 13.6 | 0.0 | 96.6 | 0.0 | ||
| 48 | +32.6 | 2.0 | 3.9 | 28.7–36.5 | 16.5 | 0.0 | 94.5 | 0.0 | ||
| 27 | +33.6 | 3.1 | 9.3 | 27.6–39.6 | 11.0 | 0.0 | 99.4 | 0.0 | ||
| DBP (mmHg) | ||||||||||
| Intensity | ||||||||||
| 69 | +20.1 | 1.6 | 2.5 | 17.0–23.2 | 12.6 | 0.0 | 98.7 | 0.0 | ||
| 39 | +31.9 | 1.5 | 2.2 | 29.0–34.8 | 21.4 | 0.0 | 93.8 | 0.0 | ||
| 4 | +52.4 | 11.9 | 141.0 | 29.1–75.6 | 4.4 | 0.0 | 94.1 | 0.0 | ||
| Duration | ||||||||||
| 42 | +24.5 | 1.4 | 1.9 | 21.8–27.2 | 17.9 | 0.0 | 94.2 | 0.0 | ||
| 42 | +26.8 | 3.1 | 9.6 | 20.8–32.9 | 8.6 | 0.0 | 98.6 | 0.0 | ||
| 21 | +24.5 | 2.5 | 6.1 | 19.6–29.3 | 9.9 | 0.0 | 99.1 | 0.0 | ||
| Note: Analyses performed with the random effects model. N, number of studies and
subgroups per study analyzed; Intensity, percentage of MVC or MR; Duration,
contraction time in seconds; CI, confidence interval; I | ||||||||||
Fig. 4 describes the risk of bias for the seven studies included in the meta-analyses comparing BP response to handgrip and other IE.
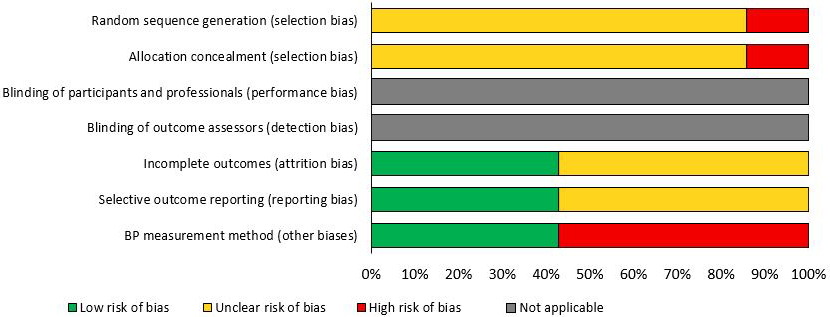 Fig. 4.
Fig. 4.Risk of bias analysis of studies that compared the BP response to handgrip exercise and other types of isometric exercise (n = 7).
This study showed that exercises involving large muscle groups promoted the highest increases in BP among all IE types. These findings support the hypothesis that muscle mass interferes with the BP response to IE [27, 110, 126] possibly because of the greater activation of the central command, intramuscular pressure, and vascular occlusion generated [111, 127]. However, this relationship is still controversial since some studies suggest that the size of the muscle is not a determining factor for BP responses [42, 124], which are mainly influenced by the magnitude of the force exerted during contraction, especially when high percentages are reached [128].
Although the overall results of the present study for each IE alone showed higher increases for the exercises involving larger muscle groups, important characteristics of the exercise protocols, such as intensity, were not considered in the analyses. Thus, some studies adopting higher intensities may have accentuated these overall BP responses, since few studies were included in the analyses and the heterogeneity among them was high. Otherwise, in the analyses comparing handgrip and two-knee extension and deadlift exercises, the exercise protocols used were similar, which reduces the possible effect of the intensity and reinforces the role of muscle mass on the BP response.
Although the exercises with larger muscle groups showed greater increases than those with smaller muscle masses, when analyzing the studies individually, only the study by Williams [124] promoted an average increase in SBP above 250 mmHg, which is the cutoff point considered safe. However, this study performed an intensity of 100% MVC, had a small sample size and measured BP with the intra-arterial method, which affect the BP response identified. Moreover, adopting 120 mmHg as the safety value for DBP [129], some studies that showed values higher than this limit included hypertensive participants [31, 81, 95], high intensity exercise [44, 101, 124], long duration of contraction (above 120 seconds) [60, 98], very small sample sizes (6 and 7 participants), and sedentary individuals performing six sets of the exercise [42]
In the subgroup analyses, men showed higher increases for SBP and DBP in response to handgrip than women. It could be explained by the fact that the majority of studies included young men and women, since premenopausal women seem to present attenuation of sympathetic nervous activity, catecholamine release, mechanoreflex, and the degree of vasoconstriction during exercise compared to men of the same age [130, 131]. Otherwise, analyzing the studies that directly compared men and women, greater increases were observed for men only for DBP.
Furthermore, middle-aged/elderly adults showed higher mean increases for SBP and DBP than younger adults for the handgrip exercise. The elevated pressure response with age is still not a consensus, since some studies suggest that there is no exacerbation of this mechanism during healthy aging. However, it is known that the aging process is associated with several structural, hormonal, and functional changes, including increased arterial stiffness, peripheral vascular resistance, and sympathetic activity, as well as deterioration of endothelial function [132], which increases the risk of developing hypertension with advancing age [133]. Thus, in studies that included older participants, the prevalence of hypertension was also higher, which would help to explain, in part, these findings.
Higher increase in SBP was observed for hypertensive compared to non-hypertensive individuals during handgrip exercise, but not for DBP. Such response was expected since hypertensive individuals present autonomic imbalance, with sympathetic hyperactivation [134]. Nevertheless, it must be emphasized that we included in this review studies with medicated and non-medicated hypertensive individuals. The use of different classes of antihypertensive medications, at different times of the day, may have influenced the BP responses to IE. However, it was not possible to perform an analysis considering this variable due to the lack of information available in the studies.
Regarding the characteristics of the exercise protocol, only intensity
influenced SBP and DBP during handgrip. These findings support the hypothesis
that higher intensities promote BP responses to exercise [20, 128]. Although the
studies with high intensities (
Concerning the practical application of the present study, it should be
considered that even those IE that involve greater muscle mass do not seem to
bring great cardiovascular risks to the practitioner. Such findings contradict
our initial hypothesis that exercise involving large muscle groups would cause
exaggerated responses in BP. On the other hand, those exercises with smaller
muscle masses promoted lower BP responses, proving to be even safer from the
cardiovascular point of view. Furthermore, during handgrip exercise, it is
relevant to have a special attention for men, hypertensive and elderly
population, and for the exercise performed at higher intensities (
Therefore, when using IE as a strategy for the treatment of hypertension, it is necessary to considerer some characteristics of the patient. For those hypertensive individuals controlled by medication and/or who do not have other comorbidity, the choice of the type of IE is more flexible, and exercises with different muscle masses can be adopted, as long as the general precautions regarding the prescription of exercises for hypertensive individuals are taken (i.e., avoid the Valsalva maneuver during the effort). However, if the hypertensive individual is not controlled and/or presents complications or comorbidities, it seems more cautious to choose exercises involving smaller muscle masses.
Considering this, IE can be considered as a complementary non-pharmacological strategy for the prevention and treatment of hypertension in public health recommendations. However, more studies are needed to ensure the cardiovascular safety of different types of this exercise and, thus, to add it in exercise guidelines to the same extent as dynamic resistance exercise [35].
This systematic review has some limitations. The studies included in this review
were conducted at different time periods and considered different guidelines for
classifying subjects as hypertensive, which may result in different criteria for
classifying hypertension. This, however, cannot be corrected considering BP
means, since these must be influenced by antihypertensive medications. The
heterogeneity among the majority of studies was high (I
The strength of the present study is its originality, since this is the first systematic review with meta-analysis that sought to investigate the BP responses during the performance of different types of IE and to compare them with handgrip. Considering this, it was not possible to compare the findings of this review with those of other systematic reviews.
In conclusion, IE involving larger muscle groups elicit greater BP responses than those involving smaller muscle masses, especially in men, middle-aged/elderly adults and hypertensive individuals. The present study supports the literature regarding the cardiovascular safety of IE involving small muscle groups, especially at low intensities, and shed light on the investigation regarding cardiovascular safety during the performance of other types of IE in adults. However, due to the high heterogeneity of the studies, the results of this systematic review should be interpreted with caution, and further investigations are needed. Prospective studies should directly compare BP responses during various types of IE in different populations and different exercise protocol.
JCC—Conception and Design, Analysis and Interpretation, Data Collection, Writing the Manuscript. GTB—Analysis and Interpretation, Data Collection, Writing the Manuscript. ACNB, ACAC—Data Collection, Writing the Manuscript. MAC, BQF—Critical Revision. RMR-D—Critical Revision. AMG—Conception and Design, Critical Revision, Overall responsibility. All authors read and approved the final manuscript.
Not applicable.
On behalf of the co-authors we would like to express our appreciation to the reviewers for their contribution through constructive criticisms in improving the quality of our scientific work.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.