




1 Department of Cardiology, Toulouse University Hospital (Hopital Rangeuil), 31400 Toulouse, France
2 Department of Cardiology, Centre Hospitalier Intercommunal Castres-Mazamet, 81108 Castres, France
3 Faculty of Sciences, Paul-Sabatier Toulouse III University, 31062 Toulouse, France
4 Faculty of Medicine, Holy Spirit University of Kaslik, 446 Jounieh, Lebanon
Academic Editors: Teruo Inoue and Daniel I. Simon
Abstract
Introduction: Up to date, the management of coronary artery aneurysm
(CAA) is not well defined and depends on local heart team decision. Data reported
in literature are scarce and controversial. We aim to compare the long-term
outcomes of different therapeutic strategies of CAA (medical vs percutaneous
coronary intervention (PCI) vs coronary artery bypass graft(CABG)).
Materials and Methods: A retrospective cohort study was conducted on 100
consecutive patients who underwent coronary angiography at Toulouse University
Hospital, Toulouse France and fulfilled the diagnostic criteria of CAA. Coronary
angiograms were reviewed, and all necessary data were collected. CAA was defined
by a coronary dilation exceedingly at least 50% of reference coronary diameter.
Results: We identified 100 patients with CAA with a mean age of 67.9
Keywords
- coronary artery aneurysm
- medical
- percutaneous coronary intervention
- cardiac surgery
- coronary artery disease
Coronary artery aneurysm (CAA) is defined as an abnormal focal enlargement of the coronary artery exceedingly at least 50% of the reference vessel diameter [1]. The reported incidence of CAA is rare and varies between 0.02 to 5.3% [2, 3, 4] with predilection to men over women and to proximal over distal coronary segments [4]. CAA is mainly divided into 2 types according to the anatomical morphology: fusiform aneurysms when longitudinal diameter is larger than transverse diameter and saccular aneurysms in the adverse case (Fig. 1). An aneurysmal dilation exceeding four folds the diameter of adjacent normal coronary segment forms a giant CAA [5] (Fig. 1). The pathogenesis of CAA is not well understood, and causal agents include atherosclerosis, genetic susceptibility, inflammatory disorders, infectious diseases, connective tissue disorders, trauma, drug reactions and iatrogenic conditions (stent angioplasty, atherectomy) [6, 7, 8]. In general, CAA is a silent disease incidentally detected by coronary angiography; however, it may lead to life-threatening complications such as thrombus formation, distal embolization, coronary steal syndrome, acute rupture and mechanical compression of adjoining structures. To date, there is no agreement on the proper management of CAA. Data from literature are controversial and limited to few small studies, case series and anecdotal evidence. Different therapeutic approaches based on medical treatment, percutaneous coronary intervention and cardiac surgery have been reported [2, 6, 9, 10]. The long-term outcomes of CAA and the prognostic value of each therapy remain unclear, thereby decision to intervene on CAA is individualized depending on its characteristics (form, size, location), clinical implication, technical challenges, coexistence of obstructive coronary artery disease and physician experience. The impact of antithrombotic therapy and the outcome of different available regimens remain unclear and not yet defined [6]. Herein, we conducted a retrospective cohort study comparing the long-term major cardiac and cerebrovascular events (MACCE) of patients with CAA who were treated conservatively versus those who underwent invasive interventions (PCI or surgery) over a 46-months follow-up period.
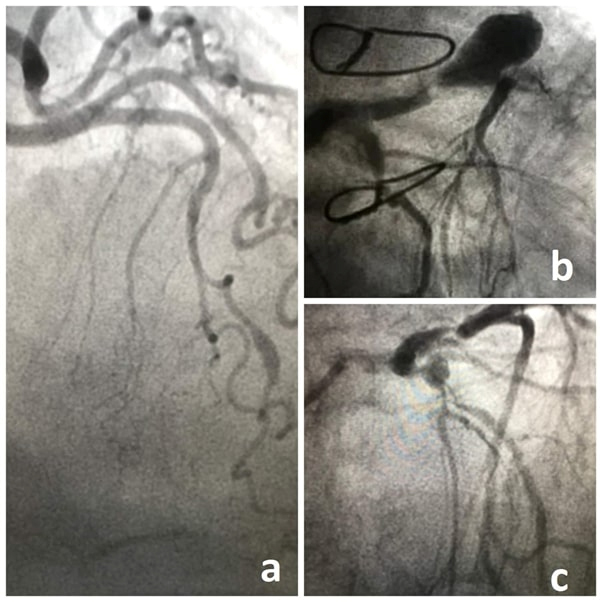 Fig. 1.
Fig. 1.Coronary angiograms showing fusiform aneurysm of the left anterior descending (LAD) (a), giant saccular aneurysm of the LAD (b) and saccular aneurysm of the bifurcation LAD/diagonal (c).
An observational retrospective cohort study was conducted on patients referred to coronary angiography at Toulouse University Hospital, Toulouse-France between September 2013 and April 2021. We searched in our digital database for all coronary angiography reports including the term coronary aneurysm. Coronary angiograms were reviewed and patients with coronary artery ectasia were excluded from the study. A total of 100 patients (108 CAAs) were included in this study. According to the performed therapeutic approach, the study participants were divided into two groups: the conservative group including those treated medically versus the invasive group including those treated by percutaneous coronary intervention (PCI) or cardiac surgery.
We searched for medical reports including the term aneurysm in our digital
database for cardiac catheterization. Coronary angiography films of the 100
included patients were reviewed by the same physician “AM”. Data concerning the
anatomical details of CAA (type, transverse and longitudinal diameters,
location), coexistence of significant CAD (
Frequency and percentage were calculated for categorical variables while
continuous variables were expressed by means and standard deviation. Continuous
variables were compared with the use of t-test or Mann & Whitney
(Medical vs Invasive) or ANOVA (Medical vs PCI vs CABG), as appropriate, and
categorical variables with the use of Chi-square test or Fischer’s exact test, as
appropriate. Normality tests for continuous variables were performed. Adjusted
stepwise logistic regression were conducted to assess the association between the
performed therapeutic strategies and MACCE. Kaplan-Meier curves and log Rank test
were used for survival analysis. A two-sided p-value
The mean age of the study population was 64.9
| Studied population (N = 100) | Conservative approach (N = 47) | Invasive approach (N = 53) | p-value | |||
| PCI (N = 42) | CABG (N = 11) | |||||
| Age (years) | 64.9 |
66.1 |
64.8 |
60 |
0.364 | |
| BMI (kg/m |
27.4 |
27.6 |
26.8 |
28.9 |
0.464 | |
| LVEF (%) | 52.3 |
52.7 |
51.4 |
54.2 |
0.276 | |
| Women (n, %) | 18 (18) | 8 (17) | 9 (21.4) | 1 (9.1) | 0.810 | |
| Dyslipidemia (n, %) | 52 (52) | 20 (42.6) | 25 (59.5) | 7 (63.6) | 0.199 | |
| Diabetes mellitus (n, %) | 25 (25) | 10 (21.3) | 10 (23.8) | 5 (45.5) | 0.256 | |
| Hypertension (n, %) | 62 (62) | 30 (63.8) | 24 (57.1) | 8 (72.7) | 0.611 | |
| Smoking (n, %) | 28 (28) | 9 (19.1) | 15 (35.7) | 4 (36.4) | 0.171 | |
| Chronic kidney disease (n, %) | 34 (34) | 18 (38.3) | 12 (28.6) | 4 (40) | 0.589 | |
| Significant CAD (n, %) | 78 (78) | 30 (63.8) | 37 (88.1) | 11 (100) | 0.003 | |
| Single-vessel disease (n, %) | 30 (30) | 16 (34) | 14 (33.3) | 0 (0) | ||
| Two-vessels disease (n, %) | 29 (29) | 12 (25.5) | 14 (33.3) | 3 (27.3) | ||
| Three-vessels disease (n, %) | 19 (19) | 2 (4.3) | 9 (21.4) | 8 (72.7) | ||
| Type of CAA (n, %) | 0.548 | |||||
| Fusiform | 54 (50) | 27 (52.9) | 22 (48.9) | 5 (41.7) | ||
| Saccular | 54 (50) | 24 (47.1) | 23 (51.1) | 7 (58.3) | ||
| Longitudinal aneurysm diameter (mm) | 10.4 |
10.7 |
10.2 |
9.7 |
0.276 | |
| Transverse aneurysm diameter (mm) | 7.2 |
7.4 |
6.7 |
8.5 |
0.039 | |
| Giant CAA (n, %) | 21 (19.4) | 13 (25.5) | 4 (8.9) | 4 (33.3) | 0.042 | |
| Involved coronary (n, %) | 0.051 | |||||
| LAD | 36 (36) | 21 (44.7) | 11 (26.8) | 4 (36.4) | ||
| RCA | 34 (34) | 11 (23.4) | 20 (48.8) | 3 (27.3) | ||
| CX | 24 (24) | 12 (25.2) | 10 (24.4) | 2 (18.2) | ||
| LM | 5 (5) | 3 (6.4) | 0 (0) | 2 (18.2) | ||
| MACCE (n, %) | 13 (13) | 6 (12.8) | 6 (14.3) | 1 (9.1) | 1 | |
| Follow-up (months) | 46.2 |
47.1 |
47.3 |
38 |
0.495 | |
| Anti-thrombotic treatment (n, %) | 0.009 | |||||
| None | 5 (5) | 5 (10.6) | 0 (0) | 0 (0) | ||
| Aspirin or P2Y12- | 40 (40) | 21 (44.7) | 11 (26.2) | 8 (72.7) | ||
| Dual anti-platelet | 30 (30) | 10 (21.3) | 19 (45.2) | 1 (9.1) | ||
| Oral anticoagulant | 25 (25) | 11 (23.4) | 12 (28.6) | 2 (18.2) | ||
| *BMI, body mass index; LVEF, left ventricular ejection fraction; CAD, coronary artery disease; CAA, coronary artery aneurysm; LAD, left anterior descending; RCA, right coronary artery; CX, circumflex artery; LM, left main; MACCE, major adverse cardiac and cerebrovascular events. | ||||||
The prevalence of MACCE was 13% over a mean follow-up period of 46.2
| Studied population (N = 100) | MACCE-group (N = 13) | No MACCE-group (N = 87) | p-value | ||
| Age (years) | 64.9 |
70.3 |
64.1 |
0.099 | |
| BMI (kg/m |
27.4 |
25.8 |
27.6 |
0.267 | |
| LVEF (%) | 52.3 |
48 |
52.9 |
0.116 | |
| Women (n, %) | 18 (18) | 4 (30.8) | 14 (16.1) | 0.243 | |
| Dyslipidemia (n, %) | 52 (52) | 2 (15.4) | 45 (51.7) | 0.886 | |
| Diabetes mellitus (n, %) | 25 (25) | 2 (15.4) | 23 (26.4) | 0.508 | |
| Hypertension (n, %) | 62 (62) | 9 (69.2) | 53 (60.9) | 0.761 | |
| Smoking (n, %) | 28 (28) | 3 (35.7) | 25 (28.7) | 0.171 | |
| Chronic kidney disease (n, %) | 34 (34) | 7 (53.8) | 27 (31.4) | 0.128 | |
| Acute coronary syndrome as initial presentation (n, %) | 32 (32) | 5 (38.5) | 27 (31) | 0.533 | |
| Significant CAD (n, %) | 78 (78) | 11 (84.6) | 67 (77) | 0.727 | |
| Type of CAA (n, %) | 0.357 | ||||
| Fusiform | 54 (50) | 9 (60) | 45 (48.4) | ||
| Saccular | 54 (50) | 6 (40) | 48 (51.6) | ||
| Longitudinal aneurysm diameter (mm) | 10.4 |
13.5 |
9.98 |
0.074 | |
| Transverse aneurysm diameter (mm) | 7.2 |
7.2 |
7.23 |
0.974 | |
| Giant CAA (n, %) | 21 (19.4) | 2 (12.5) | 19 (20.6) | 1 | |
| Therapeutic strategy (n, %) | 1 | ||||
| Medical | 47 (47) | 6 (46.2) | 41 (47.1) | ||
| PCI | 42 (42) | 6 (46.2) | 36 (41.4) | ||
| CABG | 11 (11) | 1 (7.7) | 10 (11.5) | ||
| Conservative approach (n, %) | 47 (47) | 6 (46.2) | 41 (47.1) | 0.948 | |
| Invasive approach (n, %) | 53 (53) | 7 (53.8) | 46 (52.9) | ||
| Anti-thrombotic treatment (n, %) | 0.170 | ||||
| None | 5 (5) | 0 (0) | 5 (5.7) | ||
| Aspirin or P2Y12- | 40 (40) | 7 (53.8) | 33 (38) | ||
| Dual anti-platelet | 30 (30) | 1 (7.7) | 29 (33.3) | ||
| Oral anticoagulant | 25 (25) | 5 (38.5) | 20 (23) | ||
| *MACCE, major adverse cardiac and cerebrovascular events; BMI, body mass index; LVEF, left ventricular ejection fraction; CAD, coronary artery disease; CAA, coronary artery aneurysm. | |||||
The 13 study participants who develop adverse clinical outcomes or MACCE during
the follow up period were older (70.3
| OR | 95% CI | p-value | ||
| Age | 1.033 | [0.970–1.101] | 0.313 | |
| Longitudinal diameter | 1.109 | [1.014–1.214] | 0.024 | |
| LVEF | 0.935 | [0.880–0.994] | 0.032 | |
| Chronic kidney disease | 2.958 | [0.616–14.211] | 0.176 | |
| Smoking | 1.656 | [0.312–8.791] | 0.554 | |
| Treatment | 0.787 | |||
| PCI | 1.642 | [0.402–6.719] | 0.490 | |
| CABG | 1.410 | [0.120–16.515] | 0.784 | |
| *LVEF, left ventricular ejection fraction; PCI, percutaneous coronary intervention; CABG, coronary artery bypass graft. | ||||
Lastly, the Kaplan-Meier Curve and log-Rank test failed to detect a significant difference in survival between the study groups [Conservative vs Invasive, p = 0.821 (Fig. 2)] and subgroups [Medical vs PCI vs CABG, p = 0.957 (Fig. 2)], respectively. Pointing on the antithrombotic regimen, 40% received single antiplatelet, 30% dual antiplatelet and 25% oral anticoagulant without significant different distribution between study participants who developed MACCE and others (MACCE- vs No MACCE – groups) (Table 2). As expected, dual antiplatelet treatment was more frequent among PCI-subgroup (Table 1). There was no significant difference for MACCE free survival in favor of those receiving oral anticoagulant, p = 0.557 (Fig. 3).
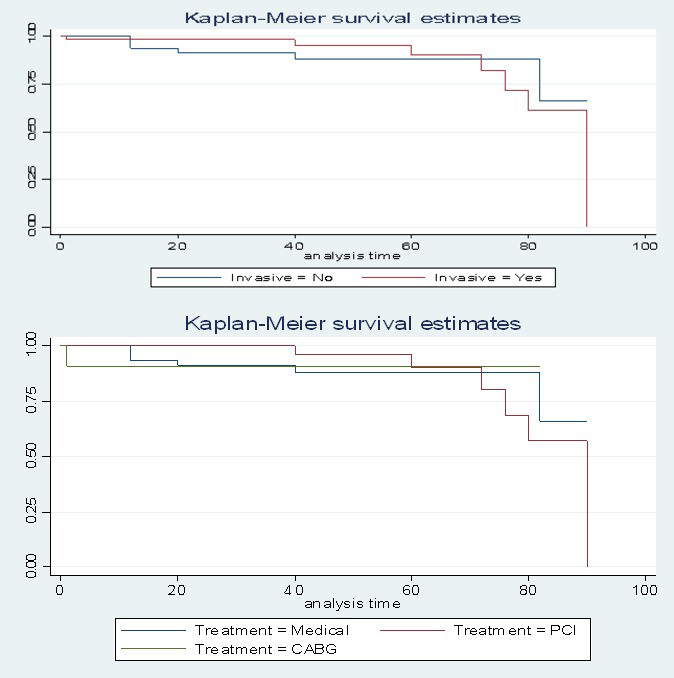 Fig. 2.
Fig. 2.Kaplan-Meier survival analysis for freedom of major adverse cardiovascular and cerebrovascular events (MACCE) in patients with invasive versus conservative treatment and in patients with medical management versus PCI versus CABG.
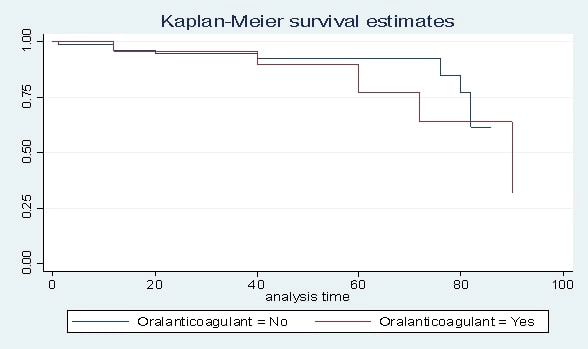 Fig. 3.
Fig. 3.Kaplan-Meier survival analysis for freedom of major adverse cardiovascular and cerebrovascular events (MACCE) in patients who received oral anticoagulant versus others.
The results of this study showed an absence of significant difference in MACCE free survival at 46 months follow up between the different proposed treatment strategies in patients with CAA. However, the longitudinal aneurysm diameter was positively associated to MACCE. The presence of obstructive CAD and coexistence of multi-vessels coronary disease were in favor of invasive approach. The prevalence of CAA was 0.37% of the total catheterization reports and it is close to the previously reported ones in literature that range between 0.2% to 5.3% [11, 12].
In line with recently published studies [9, 11, 12], LAD was the most common involved coronary artery and atherosclerosis was predominantly associated to CAA. They share multiple histological features such as focal calcification, lipid deposition, fibrosis and alteration of vascular layers [13, 14]. In fact, atherosclerosis is a chronic inflammatory disease affecting the transmural vascular wall from the tunica intima to the external elastic lamina, thereby modifying the architecture of coronary artery walls in a manner to decrease the resistance to intraluminal pressure ending with progressive dilation and aneurysm formation [13, 14, 15, 16]. Up to date, the exact pathophysiological mechanism of CAA is not well known, but atherosclerosis is the main reported cause in adults and Kawasaki disease in children [2]. Also, vasculitis, proteolytic imbalance, genetic susceptibility, infectious diseases and iatrogenic conditions (post-percutaneous coronary intervention) may contribute to CAA formation. The coexistence of CAD plays a pivotal role in the choice of therapeutic strategy [6] and constitutes the main determinant parameter for invasive approach as shown by this study result. Herein, 100% of patients treated with CABG (N = 11) have diffuse CAD (27.2% two- and 72.7% three vessels disease). Noteworthy that these interventions were not exclusively performed for the treatment of CAA, but also for the associated obstructive CAD. Studies comparing the outcomes of invasive versus conservative management of CAA are scarce in literature. In our study, no significant differences between conservative and invasive (PCI+CABG) strategies and between medical, PCI and CABG subgroups have been found. In parallel, data from the International Coronary Artery Aneurysm Registry (CAAR) reported similar rates of mortality and MACCE among those treated by CABG or PCI. A similar finding was revealed by a smaller study conducted on 42 patients who underwent CABG (18/42) and PCI (24/42) for CAA [17]. The study by Khubber et al. [11], including 230, 176 and 52 participants in medical, CABG and PCI groups, respectively has attributed a better outcome to CABG over medical treatment but like that of PCI. In our study, the prevalence of MACCE was lower in CABG group (9.1%) than that in PCI (14.3%) and medical (12.8%) groups, but without reaching the level of statistical significance. The overall low prevalence of MACCE (13%) in the studied population and the small number of patients who underwent cardiac surgery (11%) may limit the power of this study to detect a statistical difference in favor of CABG. According to previously published data, larger aneurysm size and coexisting of heart failure are predictors of poor prognosis [11, 18, 19]. Indeed, we showed a positive association between the occurrence of adverse clinical outcomes, longitudinal aneurysm diameter and reduced LVEF. Lastly, no benefits for anticoagulant regimen over single or dual antiplatelet therapy have been observed. Results from previously published studies concerning antithrombotic therapy in CAA patients are conflicting. Thereby, some studies describe a similar finding to this study result while others conclude for positive effects of anticoagulation [6]. In fact, anti-thrombotic regimens were influenced by the therapeutic strategy and most probably by other co-morbidities. Thus, dual antiplatelet therapy was largely overexpressed in the PCI-subgroup, and this makes sense. Among patients treated with anticoagulants, 7% had atrial fibrillation and 3% had thromboembolic event as a reason for oral anticoagulant.
The observational retrospective study design that may predispose to selection bias and immortal time bias. The low prevalence of adverse clinical outcomes limits the power of the study to determine the potential predictive factors of MACCE. Also, the small sample size makes difficult to clearly conclude on the impact of anti-thrombotic therapy. In parallel, the number of study participants in CABG group is low which subsequently reduces the risk to detect a statistical difference in favor of this approach. Invasive versus conservative therapy was chosen based on the Heart Team’s clinical judgment in the best interest of the patient at the time of the procedure. We can suppose that most severe patients with coexisting CAD were treated by CABG or PCI.
CAA is frequently associated with CAD. Patients with multi-vessels disease are more predisposed to undergo invasive therapeutic approach (PCI and CABG). Data analysis of long-term MACCE free survival showed similar outcomes in medical, PCI and CABG groups. Longitudinal aneurysm diameter was positively associated with MACCE. Also, no additional benefits have been observed with oral anti-coagulant regimen. However, this conclusion must be carefully interpreted in view of the limitation of retrospective study design and the small sample size, thereby larger randomized prospective multi-centric trials are required to better understand and optimize the management of CAA.
AM, FCP contributed to conception, design and writing of the article; VN, TL, FB, SB, ME and JR contributed to conception and design; DC conrtributed to design and writing of the article and provided important intellectual contribution to the manuscript. All authors have read and agreed to the published version of the manuscript.
The cohort was registered by the Ministry of Research and the Regional Health Agency Occitanie (no. DC-2017-298).
Not applicable.
This research received no external funding.
The authors declare no conflict of interest. Anthony Matta and Jerome Roncalli are serving as the Guest editors of this journal. We declare that Anthony Matta and Jerome Roncalli had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Daniel I. Simon and Teruo Inoue.
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.