













 , Andreea Catarina Popescu 1,2,*, Serban Mihai Balanescu 1,2
, Andreea Catarina Popescu 1,2,*, Serban Mihai Balanescu 1,21 Cardiothoracic Medicine Department, “Carol Davila'' University of Medicine and Pharmacy, 020021 Bucharest, Romania
2 Department of Cardiology, Elias Emergency University Hospital, 11461 Bucharest, Romania
Academic Editors: Zhonghua Sun and Michael Dandel
Abstract
Cardiomyopathies are a challenging pathology and echocardiography is essential for diagnosis and prognosis. The most frequent cardiomyopathies are the dilated cardiomyopathy (DCM) and the hypertrophic cardiomyopathy (HCM), followed by the less frequent restrictive (RCM) and arrhythmogenic right ventricle cardiomyopathies (ARVC). Echocardiography can identify diagnostic features, and guide further testing for a definitive diagnosis. Echographic parameters are involved in risk score computing and prognosis assessment. While the most prevalent hallmark of HCM is the asymmetric left ventricular hypertrophy and systolic anterior motion of the mitral valve with the obstructive phenotype, DCM shows dilated left ventricle with different degrees of systolic dysfunction, and RCM is usually characterized by undilated ventricles associated with atrial enlargement. The aim of this review is to display and compare the most frequent cardiomyopathies encountered in clinical practice and highlight their most characteristic features in a useful way for the practicing clinician.
Keywords
- restrictive cardiomyopathy
- dilated cardiomyopathy
- speckle tracking
- arrhythmogenic right ventricle cardiomyopathy
- ventricular non-compaction
- stress cardiomyopathy
- Takotsubo syndrome
- deep learning
Echocardiography is the main diagnosis and monitoring technique for various types of heart diseases. It has a favorable cost-efficiency ratio, low risk, allows follow-up, and offers increasingly more accurate information due to continuous development in terms of technique, imaging methods, and pharmacology-associated assessment. Moreover, ultrasonography machines have undergone significant development in recent years Thus echocardiography continues to present several advantages over others imaging diagnostic techniques [1].
Cardiomyopathies represent a variety of myocardial disorders with damage to the heart muscle as a common feature. There are various functional and structural phenotypes with or without hereditary transmission [1, 2]. Heart muscle damage is associated with the primary impairment, therefore structural and functional changes that appear secondary to ischemic, congenital, or valvular heart disease are not considered to be part of the “cardiomyopathy” spectrum. Approved by the World Heart Federation in 2013, the most complete classification of cardiomyopathy is MOGE(S) [2]. Each one of the four capital letters represents a framing feature of cardiomyopathies referring to morphologic and functional characterization (M), the presence of other organs involvement (O), the pattern of hereditary transmission or in other words the genetic status (G), etiology (E) and stage of the evolution (S) [2]. From a morphological point of view five types of cardiomyopathies are described: dilated, hypertrophic, restrictive, arrhythmogenic right ventricle cardiomyopathy and unclassified cardiomyopathy including ventricular non-compaction and stress (Takotsubo) cardiomyopathy [3].
In the majority of cases, the diagnosis of cardiomyopathy is established after the onset of symptoms, which can be related to heart failure, and atrial or ventricular arrhythmias. Therefore, the first imaging investigation used to assess a patient with suspicion of cardiomyopathy is echocardiography, which is widely available, usually reliable and reproducible, cost-effective, and risk-free [4]. From the estimation of left and right heart filling pressures to the evaluation of the systolic and diastolic function of the left ventricle through several complex techniques, the cardiac ultrasonography can provide information related to the diagnosis, staging, and response to treatment or prognostic parameters in different cardiomyopathies [1, 5]. Bi-dimensional and three-dimensional echocardiography may be used and provide information for complex characterization of the heart in cardiomyopathies from basic parameters, like anatomic measurements or estimation of the systolic and diastolic function of the ventricles, to a more particular assessment of the muscle tissue through techniques like speckle tracking and tissue Doppler imaging [1].
This review aims to summarize the different echocardiographic characteristics observed in the above-mentioned cardiomyopathies and highlight the specific use of echocardiographic techniques in particular situations.
Dilated cardiomyopathy (DCM) is defined by dilatation associated with impaired contraction of one or both ventricles. The definition of cardiomyopathy refers to primary myocardial dysfunction of unknown etiology, with autosomal or sex-linked, dominant or recessive genetic inheritance, or as an acquired disorder with infectious (post myocarditis) or toxic origin. Both American and European Societies’ classification systems do not consider the ischemic cardiac disease, with criteria for dilation and impaired systolic function of the left ventricle (LV), as a cause of cardiomyopathy. This association between ischemia and myocardial dilatation and dysfunction is described as a separate disease [1, 2, 6].
Dilated cardiac chambers due to ischemic heart disease are associated with specific echocardiographic anomalies, like regional wall contractility disturbances or regional remodeling. However, this kind of limited wall segment motion abnormality can also be found in idiopathic DCM. For example, other diseases that can be characterized by regional wall motion abnormalities include sarcoidosis or tuberculosis. Ischemic cardiomyopathy may also present areas of endocardial brightening or scarring in infarcted areas [7].
The initial imaging evaluation comprises of two main 2D echocardiography parameters: left ventricle ejection fraction (LVEF) less than 40% or fractional shortening less than 25% [6]. However, the comprehensive diagnosis of DCM should consider aspects of the clinical presentation, patient examination and other test results. Dilatation of the LV, especially end-diastolic and end-systolic transverse diameter enlargement (spherical remodeling), associated with reduced wall thickness, is easily recognized with 2D echocardiography in parasternal long-axis view (See Fig. 1 and Appendix Video 1).
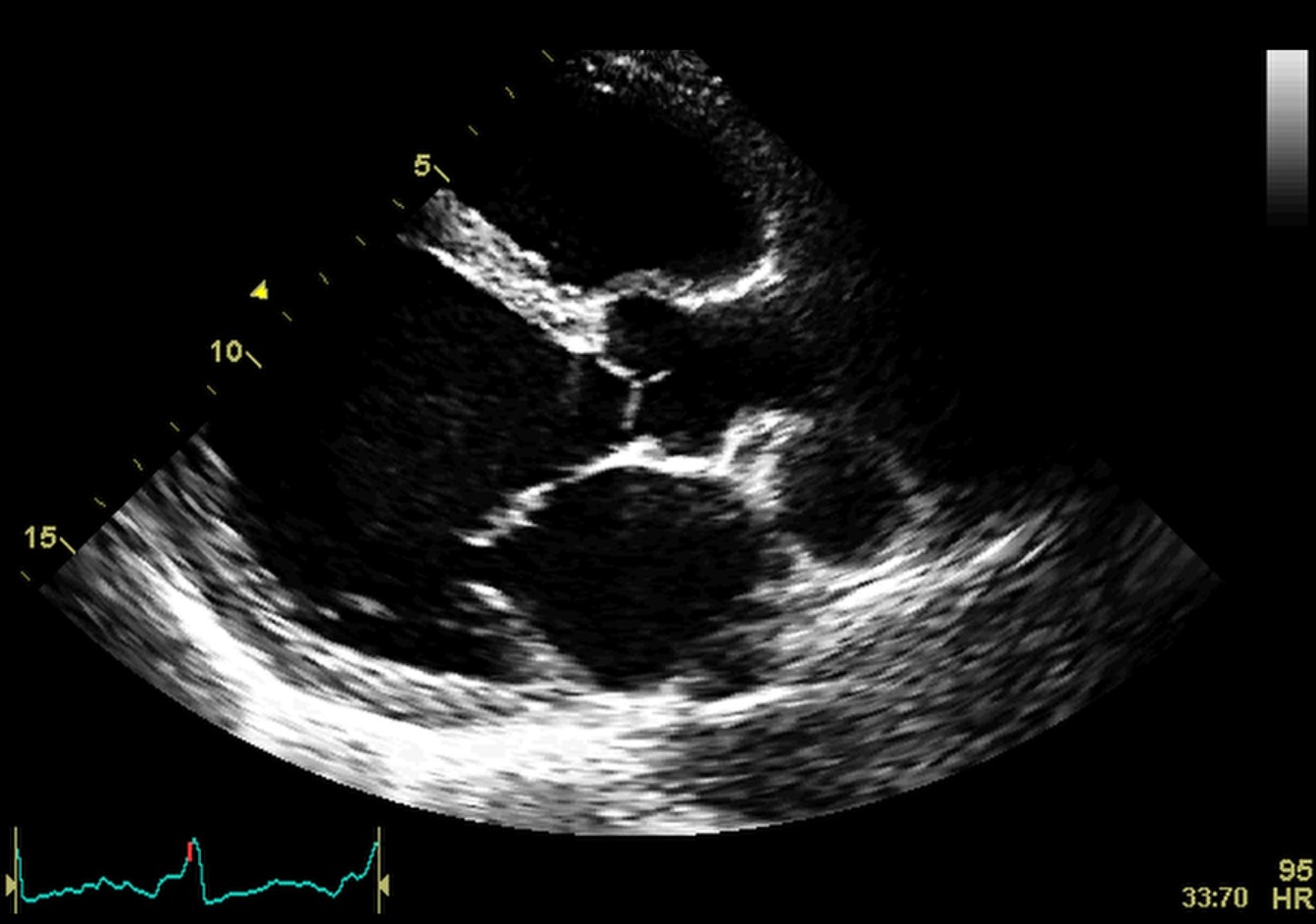 Fig. 1.
Fig. 1.Echocardiographic aspect of DCM. Parasternal long-axis view showing a dilated left atrium and left ventricle in diastole. An online video of this patient with idiopathic dilated cardiomyopathy is available (Appendix Video 1).
Cardiac chamber enlargement is often present, but linear volumetric estimation
is no longer recommended. According to the American Society of Echocardiography
quantitative parameters should be obtained for an accurate assessment. Thus, DCM
is defined by an LV end-diastolic volume index above 100 mL/m
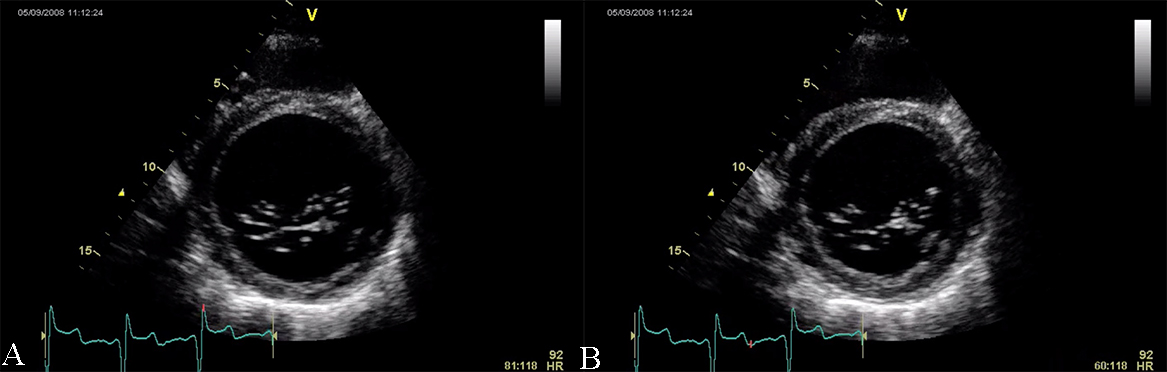 Fig. 2.
Fig. 2.Echocardiographic aspect of DCM in a patient with idiopathic dilated cardiomyopathy. (A) Parasternal short axis at the level of the mitral valve, diastolic frame showing a dilated left ventricle. (B) Parasternal short axis at the level of the mitral valve, systolic frame showing the small difference between the end-diastolic and end-systolic diameter of the left ventricle due to reduced contractility.
Left atrial volume index (LAVi) is estimated from 2D echocardiography 4
chamber-view. A value above 50 mL/m
The evaluation of the anatomy and function of the right ventricle (RV) is mandatory, given the fact that the prognosis is considerably worse when there is RV dilatation and/or RV systolic dysfunction. RV systolic power is defined by the tricuspid annular plane systolic excursion (TAPSE) in 2D apical 4-chamber view, ejection fraction and fractional area change. For TAPSE, a reported value of 14 mm, is associated with poor prognostic in patients with DCM [3, 4]. RV dysfunction is not essential for the diagnosis of DCM but when present, it is an adverse prognostic marker.
Color and spectral Doppler echocardiography is of limited use in the diagnosis
of DCM, except for atrioventricular valve incompetence. One constant feature is
the presence of mitral regurgitation, secondary to the annulus dilation with
abnormal leaflet tethering. Mitral regurgitation can present with different
degrees of severity and is an additional prognostic factor (see Fig. 3 and
Appendix Video 2 and 3). The pathophysiology of mitral regurgitation in DCM is usually
due to abnormal leaflet tethering mandated by the change in LV shape from
ellipsoid to spherical. As cardiomyopathy progresses, the point of leaflet
coaptation migrates from its normal basal location to a spot deeper in the LV
cavity this leading to also to an apposition defect with the generation of an
eccentric regurgitant jet. Moreover, DCM patients present with an abnormally low
diastolic function [5]. Restrictive or pseudo-normal diastolic inflow patterns
impact the patients with DCM, with an associated poor prognosis [10, 11]. The
assessment of the pulmonary vein flow signal as an adjunct to the mitral inflow
pattern is very important in the echographic evaluation of DCM. Abnormal
pulmonary venous systolic flow patterns have been shown to correlate with the
future development of pulmonary hypertension. Loss of the systolic dominant flow
pattern suggests elevated filling pressure and the difference between the
pulmonary venous flow reversal duration and the mitral inflow duration during
atrial contraction greater than 30 ms predicts mortality and hospitalization [9].
Studies evaluating diastolic compliance with Doppler echocardiography have shown
also an altered mitral diastolic flow with a short deceleration time
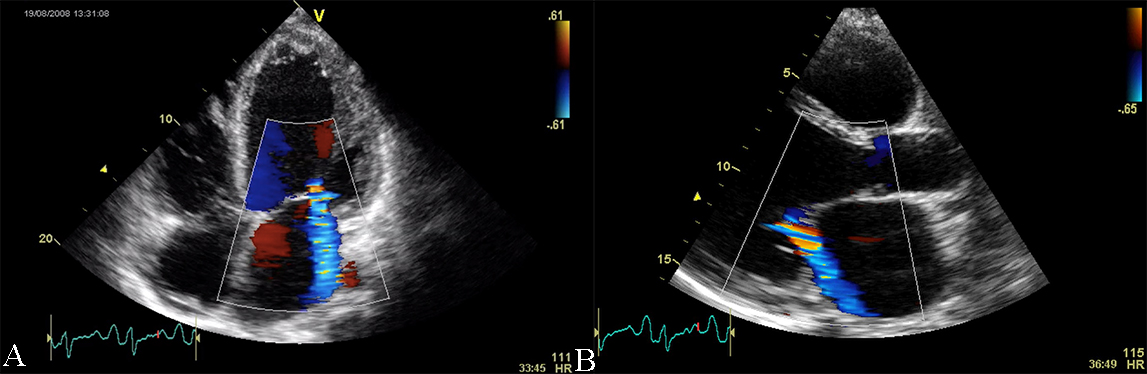 Fig. 3.
Fig. 3.Echocardiographic aspect of DCM in a patient with idiopathic dilated cardiomyopathy. (A) Apical 4 chamber view, showing dilated left ventricle, dilated left atrium, and significant secondary mitral regurgitation flow with Coanda effect. (B) Parasternal long-axis view, showing dilated left ventricle, dilated left atrium, and significant secondary mitral regurgitation flow with Coanda effect. An online video of this patient with idiopathic dilated cardiomyopathy is available (Appendix Video 2 and 3).
TDI is a technique used to characterize diastolic dysfunction but also gives
important information about the global and regional systolic function of the
myocardium. By TDI can be assessed displacement velocities of small samples of
the tissue, values which are directly proportional to the contractility force of
the region of interest but it is also correlated with the global systolic
function of the LV or RV. The mean normal value of the velocity contraction (S
wave) for the septal annulus is 8.1
Speckle tracking is also useful in the evaluation of DCM. Left ventricle global longitudinal strain (GLS) is more sensitive compared to the ejection fraction in the detection of impaired systolic function. Moreover, the GLS is a prognostic parameter for the left ventricle reverse remodeling. A higher GLS is associated with a better reverse remodeling, even with a similar left ventricle ejection fraction. A GLS value more negative than –10%, which is reported as a cut-off, is related to better reverse remodeling and consequently with better long-term prognosis [13].
Some cases of DCM with severe systolic dysfunction (left ventricular ejection
fraction
Interventricular dyssynchrony is determined by the temporal phase shift between the contraction of the two ventricles. There are several useful parameters to define dyssynchrony at the level and they can be obtained by conventional pulsed-wave Doppler or Tissue Doppler imaging. A difference higher than 40 ms between left ventricular and right ventricular pre-ejection time (measured by pulsed-wave Doppler), and also a delay greater than 56 ms between the onset of systolic motion in the basal right ventricular free wall versus the most delayed basal LV segment (measured by tissue Doppler) are the most used parameters for defining the interventricular dyssynchrony, but they also have limited value for predicting CRT response.
Intraventricular dyssynchrony defined as inhomogeneity in myocardium contractility can be evaluated by conventional echocardiography, tissue velocity measurements, and deformation imaging. The temporal difference between septal to posterior wall contraction can be assessed by M-mode echocardiography, from a parasternal short-axis view at the papillary muscle level, by measuring the delay in systolic thickening of the myocardium [17, 19]. It is calculated as the interval between the maximal posterior displacement of the septum and the maximal displacement of the left posterior wall. Another parameter used for establishing intraventricular dyssynchrony is the value of the pre-ejection time, measured from QRS onset to aortic flow onset. The recognized cut-off values are septal to posterior wall motion delay above 130 ms and left ventricular pre-ejection time higher than 140 ms [8, 20]. There is no demonstrated predictive role for these parameters. In contrast to the described parameters related to the timing of myocardial velocity peaks, myocardial deformation parameters (strain, strain rate) may help in distinguishing active contraction from passive one caused by tethering of adjacent myocardial regions [8, 14, 15, 21]. These parameters may also be used during follow-up for highlighting the reverse remodeling process, and some of them as prognostic features for patients with DCM and LV systolic dysfunction [14, 15, 17, 20].
Ventricular remodeling describes structural changes in the left ventricle in response to chronic alterations in loading conditions. Current therapeutic strategies for systolic heart failure aim to slow or halt the remodeling process. Reverse remodeling refers to a concept, where progressive LV dilatation and deterioration in contractile function are not simply arrested, but partially reversed is defined as a process characterized by a reduction in LV volumes with improvement in systolic and diastolic function. Right ventricular function normalization is part of a global hemodynamic improvement induced by therapy and precedes LV reverse remodeling.
Hypertrophic cardiomyopathy (HCM) is defined by increased regional or global LV mass. The histological characterization includes cellular disarray and fibrosis which lead mainly to diastolic dysfunction. Systolic dysfunction is related to reduced preload with hypertrophied myocardium and reduced end-diastolic LV chamber. Proper systolic dysfunction may occur late in the course of the disease, when heart dilation may ensue. Echocardiography is the main method of diagnosis, severity classification and risk estimation in HCM [3, 4]. Echocardiographic parameters such as LV wall thickness, LA size, LVOT gradient, or the presence of apical aneurysm are included in the assessment of the 5-year sudden cardiac death risk model, as part of the protocol for primary prophylaxis of sudden cardiac death, and ICD implantation decision [22]. An IVS thickness above 30 mm is recognized as one of the criteria in decision-making for ICD implantation, as recommended by the current guidelines [23]. Also, reverse septal curvature, associated with septal HCM, predict SCD and may be included in future guidelines for ICD implantation [24, 25, 26].
Echocardiography is the first-line diagnostic method for differential diagnosis
in HCM, to identify LV hypertrophy from secondary causes. Severe hypertrophy is
diagnosed when the LV mass is above 130 g/m
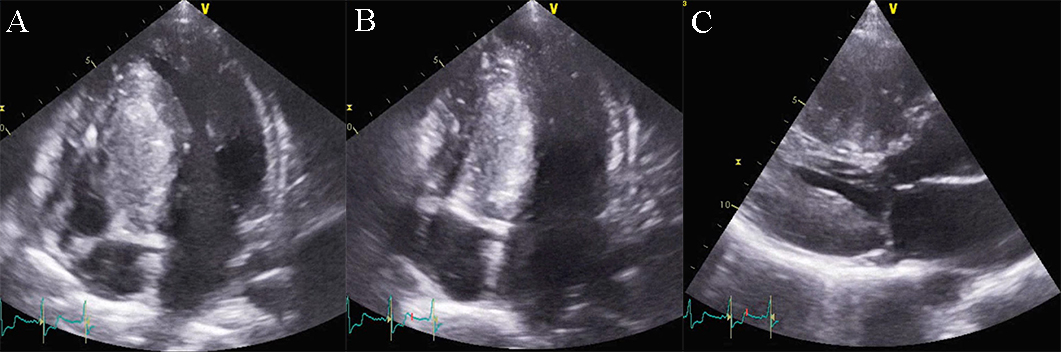 Fig. 4.
Fig. 4.Echocardiographic aspect of HCM. (A) Apical 4 chamber view systolic frame, showing increased septum thickness. (B) Apical 4 chamber view diastolic frame. (C) Parasternal long-axis view- evidence of systolic anterior motion of the mitral valve. An online video of this patient with HCM is available (Appendix Video 4).
2D echocardiography in HCM detects a septal wall thickness higher than 14 mm as
a diagnostic criterion for HCM, after excluding all the other causes of LV
hypertrophy. The severity and distribution of hypertrophy in HCM are highly
variable [23]. It may be concentric or localized (septal, apical, free LV wall,
or right ventricle hypertrophy) with or without intraventricular obstruction
(medio-ventricular, LV outflow). One pathognomonic echocardiographic feature is
the asymmetric septal hypertrophy, with a ratio of septal to the posterior wall
thickness of 1.5/1 [29]. The first echocardiographic criterion for the diagnosis
of LV hypertrophy is the LV mass obtained by M-mode and defined by an LV mass
index
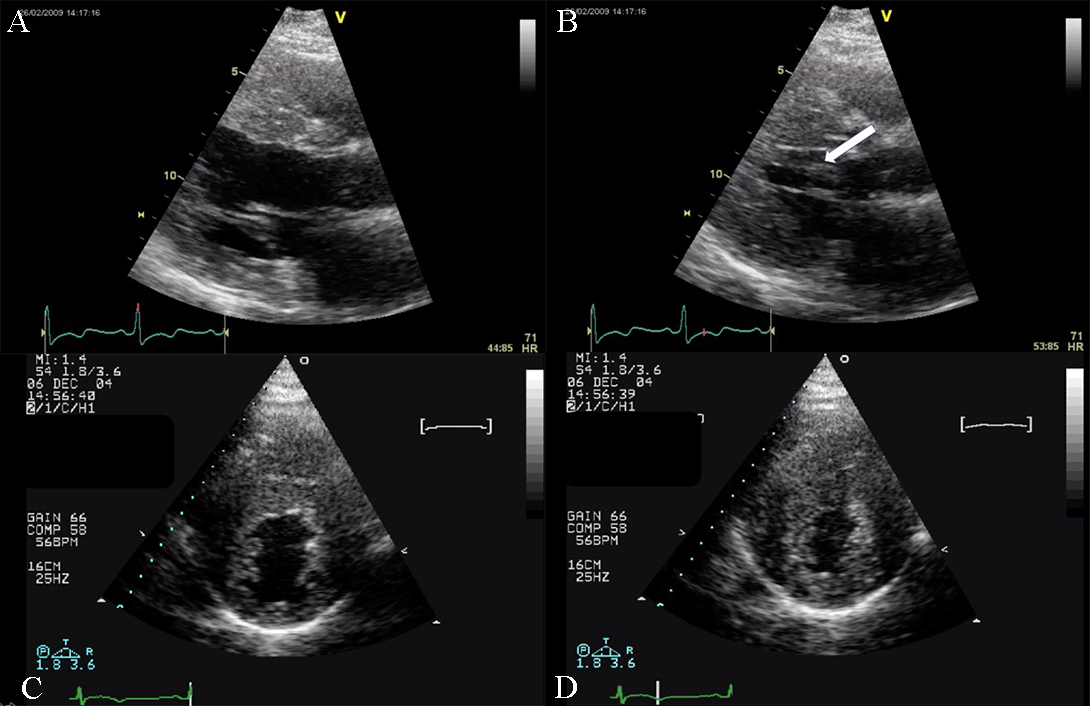 Fig. 5.
Fig. 5.Echocardiographic aspect of HCM. (A) Parasternal long-axis view diastolic frame showing increased thickness of septum and inferolateral wall. (B) Parasternal long-axis view systolic frame showing (arrow) systolic anterior motion of the anterior mitral valve. (C) Short axis view diastolic frame showing significant left ventricular hypertrophy. (D) Short axis view systolic frame showing reduced left ventricular end-systolic diameter.
Echocardiography may also identify a phenotype of HCM associated with small apical aneurysms, not due to ischemia. These patients frequently present with malignant ventricular arrhythmias and resuscitated cardiac death or systemic cardioembolism [31]. Thus, the presence of apical aneurysms in the setting of HCM is associated with an ominous outcome and needs prompt implantation of an ICD [32].
Doppler echocardiography allows assessment of the intraventricular gradient and associated mitral regurgitation. One specific feature is the variability of the LV outflow gradient according to the hydration status, heart rate, the Valsalva maneuver (preload), and blood pressure (afterload). Conditions or pharmacologic interventions that increase preload and increase LV end-diastolic volume may reduce LVOT obstruction. Reduced preload and tachycardia responsible for a reduction in LV end-diastolic volume are associated with an increase in intraventricular gradient. Stress echocardiography is a method that employs different agents (exercise, dobutamine, isoproterenol, amyl nitrite) which alter LV diastolic volume, to highlight the dynamic intraventricular gradient [5, 27, 33]. The degree of mitral regurgitation severity in HCM can vary from mild to severe. The mechanism of mitral regurgitation is related to the geometry change of the valve due to the malposition of the anterolateral papillary muscle, the abnormal attachment of primary chordae tendineae and SAM. The latter is favored by the elongated leaflets of the mitral valve which are a usual feature of the mitral valve in HCM. Moreover, some studies establish a direct linear relationship between the left ventricular outflow tract area and the mitral valve area, with a positive correlation with the severity of outflow tract obstruction (see Fig. 6) [27, 33].
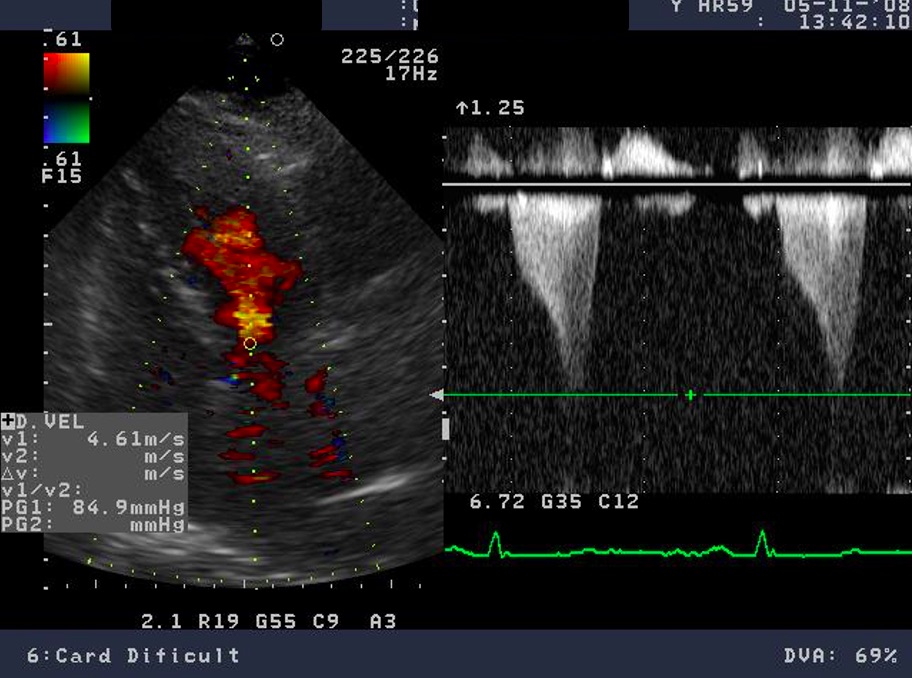 Fig. 6.
Fig. 6.Echocardiographic aspect of HCM. CW Doppler in a patient with obstructive hypertrophic cardiomyopathy shows typical systolic flow with a late peaking gradient of 85 mm Hg at end-systole. The aspect of the continuous Doppler curve is typical for obstructive HCM, with an early peak and major increase of meso-telesystolic velocities when intraventricular obstruction occurs. This is most obvious in relatively bradycardic patients who display the typical “pulsus bisferiens” pattern.
TDI offers important and early information about the subclinical systolic
dysfunction showed by under normal values of the myocardium velocity contraction
[34]. The explanation for this is the disarray among the myocytes and the
increased fibrotic tissue. An early diagnosis and prognostic parameter assessing
the systolic function of the LV in HCM is the longitudinal dysfunction by an S
lateral value under
The most specific feature of the myocardium in HCM is the reduced contractile stress (the force per unit area) because of the cardiomyocyte disarray and interstitial fibrosis [33, 37]. A maintained ejection fraction is explained by the increased end-diastolic wall thickness that produces an augmented thickening, but the histopathology of this disease is characterized by myocardial hypertrophy, fiber disarray, increased loose connective tissue, and fibrosis, which are all thought to interfere with force generation and relaxation of the cardiac muscle. Both speckle tracking and tissue Doppler highlight this feature, with a significantly lower longitudinal systolic strain, systolic strain rate, and early diastolic strain rate (see Fig. 7) [27, 28, 30, 37]. GLS is independently associated with outcomes in HCM patients. A GLS with a value higher than –10 percent is associated with a higher risk of adverse events. This depressed contractility function of the LV correlates also with myocardial fibrosis and predicts ventricular arrhythmias. Through strain echocardiography an important prognostic parameter can be obtained: the mechanical dispersion, defined as the standard deviation of time from the onset of the QRS to peak negative strain. This is related to the amount of fibrosis and is also an independent predictor for arrhythmias [28].
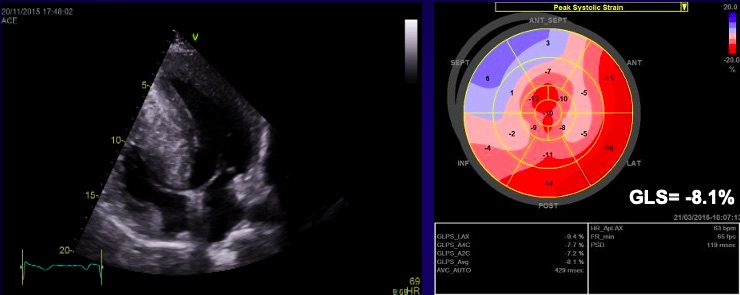 Fig. 7.
Fig. 7.Echocardiographic aspect of HCM. (A) Apical 4 chamber view shows left ventricular hypertrophy. (B) The longitudinal strain bull’s eye plot derived from 2-D speckle tracking imaging shows a significantly reduced GLS (global longitudinal strain) of –8.1%, the most abnormal region is the basal septum, corresponding with the greatest wall thickness.
Restrictive cardiomyopathy (RCM) is characterized by non-dilated ventricles, mild or no myocardial hypertrophy with impaired ventricular filling, thus it is defined by abnormal ventricular diastolic function with a normal size LV (see Fig. 8). In the early stages of the disease, the systolic function of the LV is also normal [38].
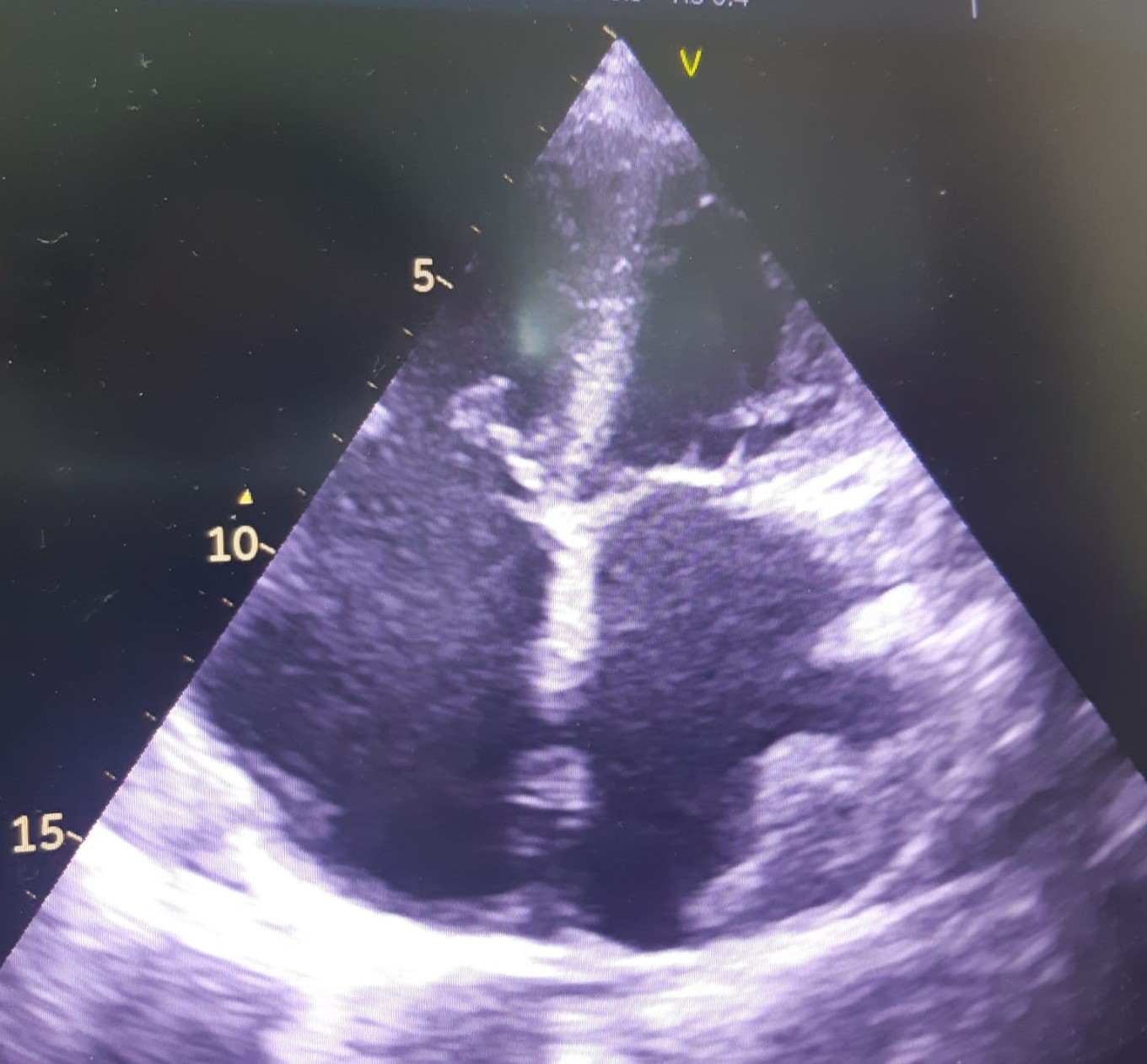 Fig. 8.
Fig. 8.The echocardiographic aspect of RCM in an elderly patient presenting with signs and symptoms of heart failure. Apical 4 chamber view showing severe biatrial enlargement, with left atrial thrombus and non-dilated left and right ventricles.
The causes of RCM can be classified as non-infiltrative (familial) or infiltrative (storage diseases), but the same pattern can be found in other disorders like diabetic cardiomyopathy, scleroderma, and endomyocardial fibrosis [38, 39, 40]. An accurate myocardial investigation by MRI and myocardial scintigraphy allows the diagnosis of different types of myocardial amyloidosis which is increasingly observed in the elderly either by transthyretin (aTTR) or by AL–light immunoglobulin chains in different plasmacytomas [41]. Another type of RCM is found in sarcoidosis and it can cause global or regional LV wall motion abnormalities. In some cases, the changes are specifically revealed on the basal posterior and lateral wall of the LV [42, 43, 44]. The most common finding is myocardial thinning, but RCM can also present with hypertrophy or it can include myocardial aneurysms [38, 45, 46, 47]. In some RCMs such as endomyocardial fibrosis or hypereosinophilic syndrome apical intraventricular thrombosis may be recognized; this may be responsible for pulmonary or systemic cardioembolism [48]. In RCM due to amyloidosis, apart from hypertrophy and wall motion abnormalities (Fig. 9), valvular involvement may also be noted with thickened aortic cusps or mitral leaflets determined by local deposition of amyloid [49].
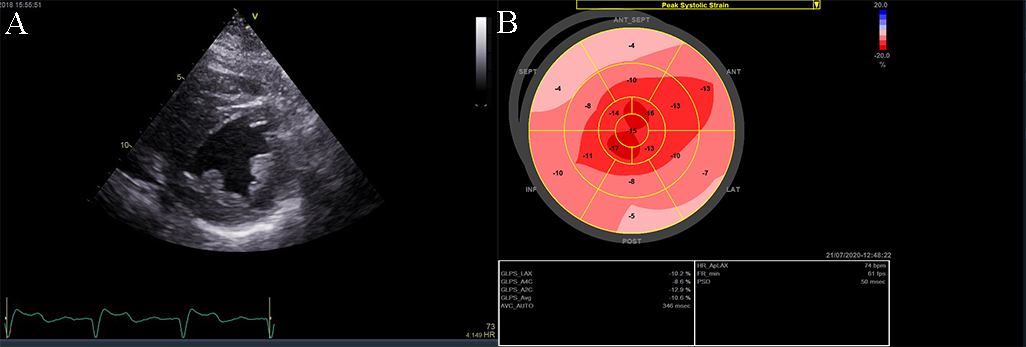 Fig. 9.
Fig. 9.The echocardiographic aspect of cardiac amyloidosis, associated with aortic stenosis. (A) short-axis view, showing left ventricular hypertrophy. (B) Speckle tracking echocardiography obtained by measuring longitudinal strain in apical 4 chamber view, shows a significantly reduced GLS (global longitudinal strain) of –8.6%.
2D echocardiography, as mentioned before, highlights a low or normal diastolic volume of the LV associated with normal or only mildly reduced LV ejection fraction, as criteria for RCM. Also, one or both atrial enlargement is identified, with increased pressures, and normal pericardium. Once the typical pattern of RCM is identified, the echocardiogram can reveal also some features for a specific etiology. For example, in cardiac amyloidosis, the left and right ventricular walls are often mildly and symmetrically thickened, the myocardium may have a granular appearance, and myocardial strain imaging may show preserved apical function. However, it is not sufficient information neither to confirm, nor exclude cardiac amyloidosis [39, 40, 50], and further testing is needed. Moreover, in sarcoidosis global or regional (typically basal posterior and lateral) LV wall motion abnormalities may be observed. The most common finding is myocardial thinning, while less common findings include myocardial aneurysms, hypertrophy, and pericardial effusion [51, 52]. In eosinophilic inflammation of the myocardium or hypereosinophilic syndrome, the echocardiogram is often unrevealing during the initial necrotic stage. In the thrombotic stage of the disease, the damaged endocardium may have associated thrombus, predominantly involving the ventricular apex [3, 5, 38, 52, 53]. During the last, fibrotic stage, increased endomyocardial echogenicity is seen, affecting one or both ventricles, sometimes with overlying thrombus; the ventricular filling can be restricted, and atrioventricular valve leaflets may be tethered [53, 54, 55]. A pattern similar to hypereosinophilic syndrome can emerge in endomyocardial fibrosis. It may be characterized by LV, RV, or biventricular apical fibrosis [53, 54, 55]. In radiation-induced RCM the echocardiogram may show structural abnormalities within the field of radiation, such as calcified heart valves, a thickened pericardium, or focal wall motion abnormalities related or not to radiation-associated coronary artery disease [40, 42, 56, 57].
Doppler echocardiography and tissue Doppler imaging show diastolic dysfunction, frequently with a restrictive pattern. Different aspects of the diastolic function can be revealed, but usually more than grade 2 diastolic dysfunction, with increased filling pressures: an elevated peak mitral inflow velocity (high velocity of E wave), rapid early mitral inflow deceleration (low deceleration time). E/A ratio greater than 0.8, deceleration time of E wave lower than 200 milliseconds, and frequently lower than 160 milliseconds, E/e’ ratio with a value above 9, are features found in the echocardiographic examination of RCM (see Fig. 10 and Appendix Video 5) [1, 4].
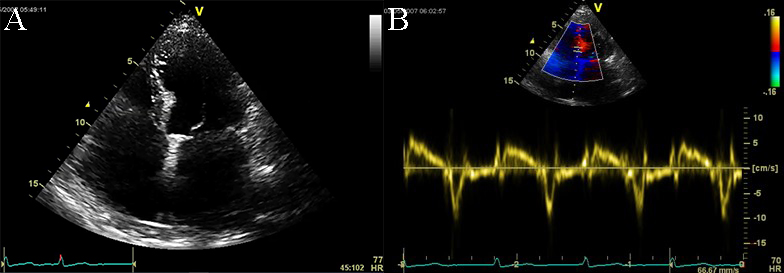 Fig. 10.
Fig. 10.Echocardiographic aspect of RCM. (A) Apical 4c view of an
elderly patient with idiopathic restrictive cardiomyopathy, severe biatrial
enlargement (left atrium
TDI is a valuable method of analysis of the systolic function in patients with
suspected RCM, helping in the differential diagnosis between RCM and constrictive
pericarditis. It offers information related to the contraction power of regional
and global LV myocardium. Reductions in TDI systolic and diastolic parameters
typically occur earlier in the natural history of the amyloid disease and other
types of RCM compared to other traditional echocardiographic measurements. The
diastolic function in TDI assessment has restrictive pattern, with low e’, and
E/e’ (average of septal and lateral mitral annulus)
Strain echocardiography reveals low myocardial velocities with regional function inhomogeneity. In RCM due to cardiac amyloidosis, both LV and right ventricle (RV) walls are often moderately, or even severely, and symmetrically thickened and the myocardium may have a granular aspect. This aspect cannot be explained by secondary causes such as hypertension. In this case, strain echocardiography may show preserved apical function [45, 46, 47]. Regarding the LA function, strain echocardiography may help in the differential diagnosis between RCM and constrictive pericarditis (CP). In both RCM and CP, the reservoir function of the left atrium is normal or may be increased compared to normal due to higher filling pressure. Contrary to this, both active and passive functions are decreased in RCM. This can be evidenced using global and regional strain, which highlights a lower value compared to normal of the septal LA strain rate [61].
Arrhythmogenic cardiomyopathy (AC) is defined by fibrous and fibro-fatty replacement especially of the RV myocardium, affecting the inflow and outflow tract, but also the apex. This process most commonly affects the posterior and inferior areas of the right ventricular inflow tract adjacent to the tricuspid valve, but it also affects the anterior infundibulum and the apex, thus forming what is known as the “triangle of dysplasia”. According to recent data, there is also involvement of the postero-lateral wall of the LV. In the LV the fibro-fatty replacement determines a transmural lesion but the process starts from the subepicardial to the subendocardial LV layers. It has been demonstrated that in left ACM, the scar tissue tends to localize in the inferolateral subepicardial LV wall. In the initial assessment of AC, these typical regional wall motion abnormalities may be detected. Later changes may involve the RV free wall and become global, producing RV dilation (Fig. 11 and Appendix Video 6). Echocardiography is the first line and sometimes a sufficient method of evaluation in patients with AC.
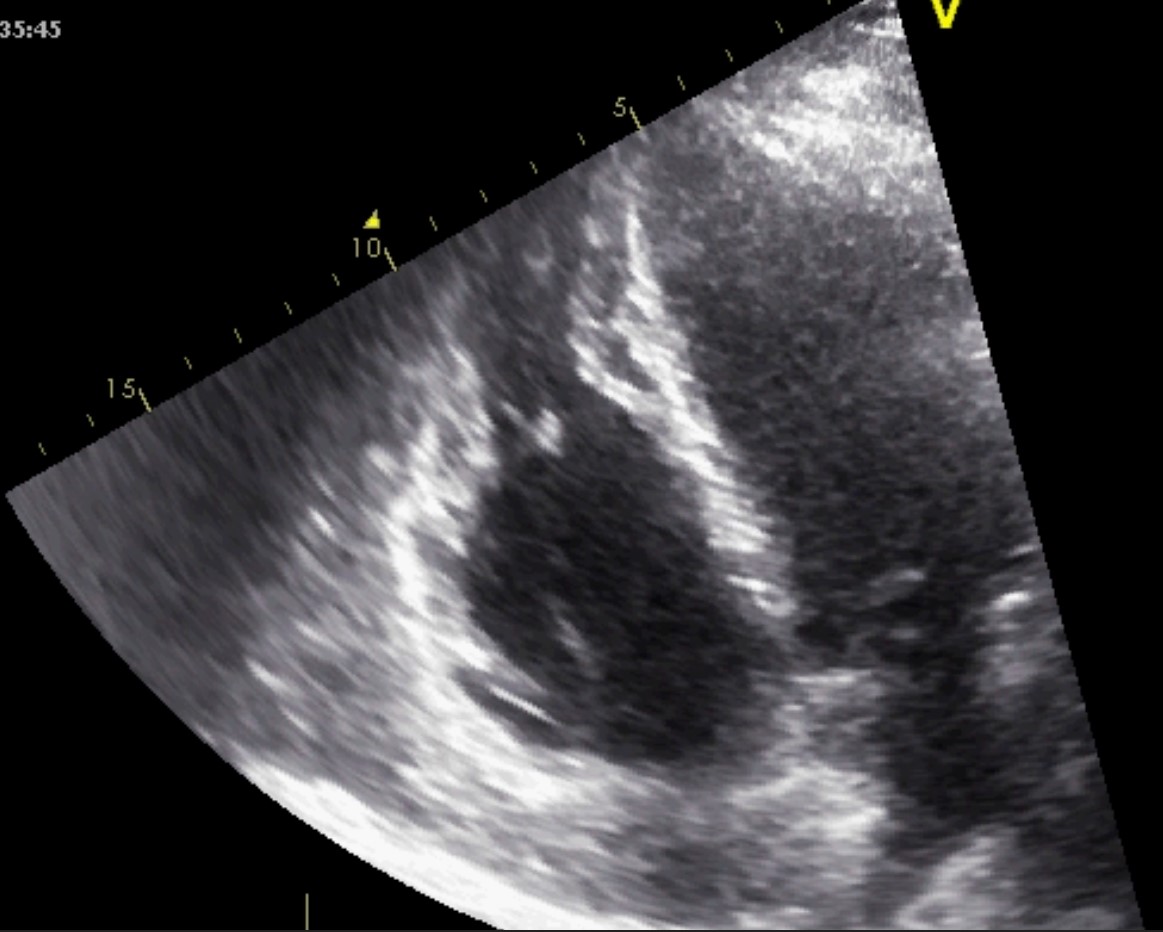 Fig. 11.
Fig. 11.Echocardiographic aspect of AC. Apical 4 chamber view showing dilation and thick right ventricular free wall. A video of the apical 4 chamber view is available online (Appendix Video 6).
The current guideline for a positive diagnosis involves the cardiac evaluation through echocardiography, magnetic resonance, or angiography to detect global or regional dysfunction of the RV and/or structural changes (Table 1, Ref. [62]). The right ventricle myocardial performance index (RV MPI) can be used in the baseline evaluation and follow-up for patients with AC, as it was shown to be a strong predictor for major cardiovascular adverse events, with a cut-off of 0.67.
| Major echocardiographic criteria | RV wall motion abnormality and 1 of the following (end diastole): |
| 1. PLAX RVOT | |
| 2. PSAX RVOT | |
| 3. or fractional area change | |
| Minor echocardiographic criteria | RV akinesia or dyskinesia and 1 of the following (end diastole): |
| 1. PLAX RVOT | |
| 2. PSAX RVOT | |
| 3. Or fractional area change | |
| Modified from Marcus et al., 2010 [62]. | |
TAPSE and fractional area change, as parameters of RV systolic function assessment, are prognostic factors in AC. RV ejection fraction estimation through 3D echocardiography, lateral systolic myocardium velocities by TDI and regional systolic strain have lower values in patients with AC [62, 63, 64, 65]. However, layer-specific GLS can predict arrhythmic risk in AC [66].
Left ventricular non-compaction cardiomyopathy (LVNC) is characterized by an LV
wall with prominent trabeculae and deep intertrabecular recesses filled with
blood resulting in two layers of myocardium: a thickened noncompacted endocardial
layer and an external, subepicardial thin compacted layer. The diagnosis of LVNC
is obtained through morphologic criteria on transthoracic echocardiography (Fig. 12 and Appendix Video 7). The echocardiographic appearance of isolated LVNC is very
heterogeneous and it can include dilated, hypertrophic or restrictive types. The
Jenni criteria for echocardiographic diagnosis of LVNC are the validated imaging
benchmark [67]. The necessary parameters are assessed using the parasternal
short-axis view at the base, midventricular, and apical levels, and for a
positive diagnosis all four of the following criteria must be met: (1) two
myocardial layers: a thin compacted exterior (epicardial) and a markedly
thickened endocardial layer with several prominent trabeculations and deep
recesses with a maximum ratio of noncompacted to compacted myocardium greater
than 2:1 at end-systole in the parasternal short-axis view; (2) evidence of flow
within the deep intertrabecular recesses through color Doppler; (3) presence of
prominent trabecular meshwork in the LV apex or midventricular segments of the
inferior and lateral wall; (4) maximal systolic compact thickness of
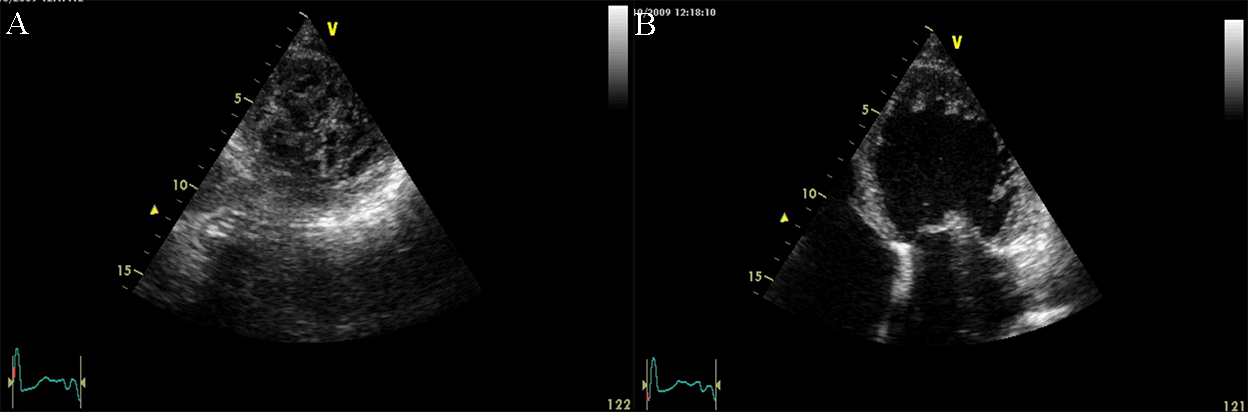 Fig. 12.
Fig. 12.Echocardiographic non-compaction cardiomyopathy. (A) 2D short axis view, at the level of the apex, showing a meshwork of trabeculae. (B) 2D Apical 4 chamber view showing dilation of the left ventricle, and apical trabeculation. A video of the apical 4 chamber view is available online (Appendix Video 7).
Takotsubo syndrome, initially described in 1990 by Sato et al. [72] in Japan, represents a sudden, usually transient, systolic cardiac dysfunction that involves LV apical akinesis and mimics an acute coronary syndrome [73]. Imaging, performed most frequently by echocardiography, shows a typical pattern of LV wall motion abnormality [74]. This includes apical dilatation with akinesia (see Fig. 13 and Appendix Video 8). There are also atypical variants including mid-ventricular, basal, focal (limited to an isolated segment), and global cases of wall contractility disorders that are stress hormone-mediated by abnormal stimulation of the cortical-hypophysis-suprarenal axis and major catecholamine release [75, 76, 77]. The standardized diagnosis uses the Mayo criteria, including clinical, biological, and imaging parameters, and all of them are necessary to complete a positive stress cardiomyopathy diagnosis [73, 78, 79, 80, 81]: (1) transient LV systolic dysfunction (hypokinesis, akinesis, or dyskinesis), apical ballooning or midventricular, basal, or focal wall motion abnormalities. Right ventricular involvement can be present; (2) the takotsubo syndrome can be preceded by an emotional, physical, or combined trigger; (3) other accepted triggers are pheochromocytoma and neurologic disorders (subarachnoid hemorrhage, stroke/transient ischemic attack, or seizures); (4) new electrocardiographic abnormalities (ST-segment elevation/depression, T-wave inversion or QTc prolongation) are usually present, but in rare occasions, no ECG changes are observed; (5) moderate elevation in cardiac troponin is common, as well as marked elevation of brain natriuretic peptide; (6) significant coronary disease may be also observed; (7) absence of the clinical context of myocarditis; (8) the most affected patient category is postmenopausal women [81]. The wall motion abnormalities are typically regional and extend beyond a single epicardial coronary artery distribution; rare exceptions are the focal (within one coronary distribution) and the global type. As described before, in the majority of cases, the regional wall abnormalities involve the apical segments of the LV, as recorded in 81.7% of the patients from the International Takotsubo Registry [80, 82, 83, 84]. The second most frequently encountered phenotype is the mid-ventricular one, with hypokinesia limited to the mid-segments of the LV, with relative sparing of the apex [78, 85]. This is present in approximately 14.6% of patients in the International Takotsubo Registry [80]. Less common phenotypes are basal, focal, or global types. Only 2.2% of patients from the International Takotsubo Registry presented basal hypokinesis with sparing of the mid-ventricle and apex, also called reverse or inverted Takotsubo (basal type) [78, 80, 85, 86]. A rare focal variant, characterized by dysfunction of an isolated segment (most commonly the anterolateral segment) of the LV, is present in 1.5% of the patients. Very rarely, in a few isolated cases, the patients have global hypokinesis [86, 87, 88]. There is a potential life-saving contribution of Speckle-tracking echocardiography (STE) for the early distinction between an acute phase of Takotsubo syndrome (TTS) and acute apical myocardial infarction, which allows avoiding the deleterious effects of catecholamine therapy in patients with Takotsubo-associated acute heart failure. Such a distinction is facilitated by the ability of STE to detect and quantify myocardial shortening (i.e., contraction) in a visually akinetic wall segment [89].
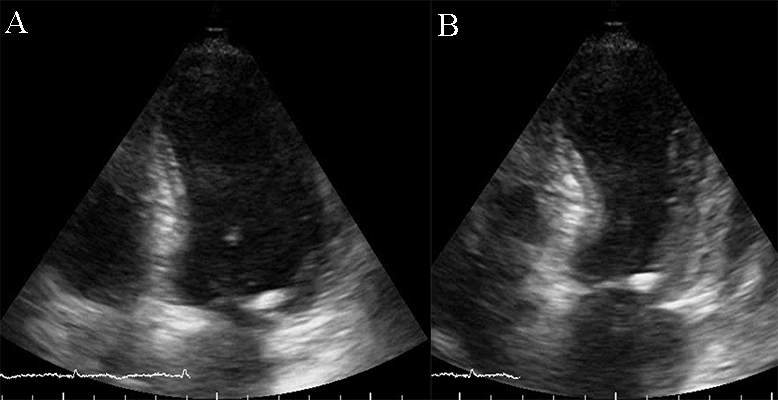 Fig. 13.
Fig. 13.Apical ballooning in a typical form of Takotsubo cardiomyopathy. TTE apical 4 chamber view. (A) end diastolic frame (B) end systolic frame. A video of the apical 4 chamber view is available online (Appendix Video 8).
Recently, automated interpretation of echocardiograms was shown to be a potentially useful method for primary care centers to obtain correct diagnoses in non-expert centers [90]. Neural network-based approaches, with deep learning models such as EchoNet, may help speed up the diagnostic process or evaluate parameters that challenging for human evaluation [91]. As this field is expanding, algorithms can be used not only for ejection fraction evaluation [92], but also for providing a differential diagnosis and etiology for patients with left ventricular hypertrophy [93]. A recent study constructed an automated algorithm that correctly discriminates between hypertensive heart disease, hypertrophic cardiomyopathy, and cardiac amyloidosis, with good sensitivity and specificity [93]. Moreover, another study showed that a machine learning algorithm was able to outperform a committee of cardiologists in discerning between Takotsubo cardiomyopathy and acute myocardial infarction [94]. This field is still in its early days, but shows promise in the diagnosis and follow-up protocols of cardiomyopathies, especially for the ones with a hypertrophic phenotype. However, for dilated cardiomyopathy, magnetic resonance imaging is preferred to echocardiography when constructing deep learning algorithms, as it provides superior spatial resolution [95, 96, 97].
The diagnosis of every cardiomyopathy might be challenging due to the phenotype variability and the multitude of morphological aspects that might appear in each of them. The common ground in all cardiomyopathies is the presentation with heart failure signs and symptoms. Echocardiography is the first method used for evaluation, allowing an exhaustive characterization of cardiac function and morphology. Two-dimensional and Doppler echocardiography is able to define the anatomic and functional characteristics of the heart that are diagnostic of DCM, HCM, ARVC, or RCM.
To compare the different diagnostic and prognostic echocardiographic parameters presented for hypertrophic, dilated, and restrictive cardiomyopathy please refer to Table 2 (Ref. [4, 10, 11, 13, 28, 29, 30, 33, 38, 58, 59, 98, 99, 100, 101, 102, 103]).
| Parameter | HCM | DCM | RCM |
| LVEDV | N | N | |
| IVS (IVS/PWT) | N | Depends on etiology | |
| Systolic function | |||
| RV hypertrophy | |||
| Systolic annular lateral wall velocity (S) | |||
| EF | N | ||
| FAC | |||
| GLS LV | –10% [13] | –7.5% [102] | |
| GLS RV | –8.6 [103] | ||
| Diastolic function | Restrictive [33] | Restrictive, pseudo-normal pattern [10, 11] | Restrictive |
| E tricuspid flow/E’ tricuspid annulus | |||
| Tricuspid EDT | Restrictive pattern (short EDT [58]) | ||
| LA volume | |||
| LA strain | |||
| E/A mitral | |||
| Mitral EDT | |||
| E mitral | |||
| E mitral flow/E’ mitral annulus | |||
| E’ | |||
| Left Ventricular Relaxation Half-Time | |||
| EDT, E wave deceleration time; EF, ejection fraction; FAC, fractional area change; GLS, global longitudinal strain; IVS, interventricular septum; LA, Left atrium; LVEDV, left ventricle end,diastolic volume; N,normal dimension; PWT, posterior wall thickness; RV, right ventricle; SD, standard deviation. In italics, parameters with prognostic values, in normal font, parameters with diagnostic values. | |||
The systolic function of the LV and RV is established through a variety of
echocardiographic parameters, the quantitative bidimensional LV ejection fraction
can be easily performed in medical facilities all over the world. When systolic
dysfunction occurs, cardiac output is initially maintained with two consequences:
left atrium enlargement and increased contractility through the Frank-Starling
mechanism. However, these compensatory mechanisms are eventually exceeded, and
cardiac output decreases, resulting in clinical manifestations of heart failure.
Systolic dysfunction is a main feature of DCM. It is also seen in some patients
with HCM who develop progressive LV wall thinning and a small increase in its
diastolic dimensions. Relative wall thickness (RWT) is defined as two times
posterior wall thickness divided by the LV diastolic diameter, is a measure of LV
geometry and can be a marker for adverse events in patients with LV systolic
dysfunction. Concentric LV hypertrophy (RWT
Diastolic dysfunction can be present with or without associated systolic dysfunction. When systolic dysfunction is described, diastolic dysfunction is always present [4, 108, 109]. Otherwise, in patients with heart failure and normal systolic function, diastolic dysfunction is one of the potential causes. Causes of HF with a normal or near-normal LVEF include many cardiomyopathies with preserved ejection fraction (e.g., HCM, RCM, LV non-compaction) [108, 110]. The LV diastole includes two phases: the first is the relaxation phase, which is a dynamic process that takes place during isovolumic relaxation and the second phase happens during early rapid filling of the ventricle [108, 111]. Later in diastole, after relaxation is complete, further LV filling is a passive process that is dependent on the compliance or distensibility of the myocardium and ends in the atrial active filling phase. Either active relaxation or passive compliance or both may be impaired in a patient with diastolic dysfunction. Echocardiographic evaluation of LV diastolic dysfunction includes Doppler assessment of transmitral flow and pulmonary venous flow, as well as tissue Doppler imaging, which is characteristic of both HCM and RCM [112, 113]. LV dimensions, left atrium maximum volume, LV wall thickness, volumes, segmental function, global longitudinal strain, and LV are parameters needed to assess the diastolic dysfunction. Indices of diastolic function include mitral inflow velocities, mitral annular velocities by tissue Doppler (septal and lateral), and pulmonary vein velocities. Isovolumic relaxation time (IVRT), tricuspid inflow velocities, and color Doppler early diastolic flow propagation velocity (Vp). In addition, the latest recommendation is the assessment of left atrium strain, particularly in cases with incomplete/suboptimal Doppler signals or indeterminate diastolic function [114, 115].
Echocardiography is recognized as a first-line diagnostic method in almost all cardiac diseases. When dealing with a patient with cardiomyopathy, echocardiography is a mandatory tool for both positive or differential diagnostic and follow-up. Although some cases cannot be completely characterized without the aid of genetic testing, MRI, etc., it is essential to have a working diagnosis after the first echocardiographic examination, as this will establish all future testing. Traditional and also newer echocardiographic techniques, that identify diagnostic and prognostic parameters, are the cornerstone in the management of cardiomyopathies. The ability of modern techniques to identify subclinical disease plays an important role in the long-term evolution of cardiomyopathy patients. Machine learning algorithms are the future in the assessment of several pathologies. Related to the echocardiographic evaluation of cardiomyopathies, it is possible to obtain machine algorithms to establish a differential diagnosis and prognostic patterns. However, for the time being, the accuracy of the obtained information is improved when associated with other clinical and paraclinical methods.
LT designed the study. LT and MRP performed the research. ACP and SMB provided help and advice on images and manuscript development. LT and MRP wrote the manuscript. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.