

 , James Livesay 1,†, Raj Baljepally 1,†
, James Livesay 1,†, Raj Baljepally 1,†1 Department of Medicine, University of Tennessee Graduate School of Medicine, Knoxville, TN 37920, USA
†These authors contributed equally.
Academic Editors: Abdul Hakeem, Bobby Ghosh, Gianluca Rigatelli and Peter Kokkinos
Abstract
The diagnostic accuracy and clinical benefits of instantaneous wave-free ratio (iFR) compared to fractional flow reserve (FFR) have been well-established in the literature. Despite the advantages of non-hyperemic pressure indices, approximately 20% of iFR and FFR measurements are discordant. Efforts have been made to establish the mechanisms as well as identify causative factors that lead to such a discordance. Recent studies have identified many factors of discordance including sex differences, age differences, bradycardia, coronary artery stenosis location, elevated left ventricular end-diastolic pressure, and diastolic dysfunction. Additionally, discordance secondary to coronary artery microcirculation dysfunction, as seen in diabetics and patients on hemodialysis, has sparked interest amongst experts. As more interventional cardiologists are utilizing iFR independent of FFR to guide percutaneous coronary intervention an emphasis has been placed on identifying factors leading to discordance. The aim of this review is to outline recent studies that have identified factors of FFR and iFR discordance.
Keywords
- fractional flow reserve
- instantaneous wave-free ratio
- discordance
- microcirculation dysfunction
Fractional flow reserve (FFR) is a diagnostic pressure index that is used to
assess the physiological significance of a coronary artery stenotic lesion in
stable ischemic heart disease (SIHD). It is defined as a ratio of maximal blood
flow in a coronary artery with stenosis compared to the maximal blood flow
through a normal coronary artery [1, 2]. Using a pressure wire during coronary
angiography, FFR is obtained by simultaneously measuring the coronary pressure
distal to a stenotic lesion and the aortic pressure [1]. FFR is the ratio of the
distal coronary pressure (P
FFR has been used by many clinicians to guide percutaneous coronary intervention
(PCI) of intermediate (40% to 70%) coronary artery stenosis in SIHD [5]. The
use of FFR-guided PCI in patients with stable coronary artery disease (CAD) has
been associated with better long-term outcomes when compared to angiographically
guided PCI [6, 7]. Two large clinical studies, the FAME and FAME2 trials, found
that FFR in patients with multivessel CAD undergoing PCI reduces combined
endpoints of mortality, myocardial infarction, and need for urgent
revascularization. In addition to improving long-term outcomes in SIHD, FFR
guided PCI is also economically attractive compared to medical management [8, 9].
Multiple studies have also demonstrated that deferring PCI in patients with
hemodynamically non-significant coronary lesions (FFR
Despite guideline recommendations, the use of FFR has been limited in clinical practice due to increased procedural costs, difficulties with reimbursement, and the side effects of inducing hyperemia with adenosine [12, 13, 14]. Studies have found that the commonly used hyperemic agent, adenosine, has been associated with clinically significant adverse effects including tachyarrhythmias, bradyarrhythmias, interactions with other medications, and prolonged procedure times [12, 13]. For these reasons, non-adenosine requiring indices such as instantaneous wave-free ratio (iFR) to guide PCI of intermediate stenotic coronary lesions were developed. Like FFR, iFR can determine the hemodynamic significance of intermediate coronary artery stenosis in SIHD. However, iFR differs from FFR in that it does not require the use of hyperemic agents [15, 16]. Instead, iFR is obtained by simultaneously measuring the pressure distal to a stenotic lesion and the aortic pressure during a specific time interval in cardiac diastole known as the “wave-free period” [15, 17]. During this naturally occurring period, capillary resistance is stable and minimal, while coronary blood flow is maximal [18, 19]. Therefore, while at a stable coronary resistance, the change in pressure across a stenotic lesion is approximately equal to the change in blood flow across the coronary lesion [17, 18]. Compared to the FFR cutoff value of 0.80, an intermediate coronary lesion is deemed hemodynamically significant when the iFR is less than or equal to 0.89 [20].
Multiple studies have compared the diagnostic accuracy and the clinical outcomes of iFR to FFR [20, 21, 22, 23]. The ADVISE study was one of first to conclude that iFR was comparable to FFR in producing a severity index of coronary artery stenosis [21]. The diagnostic accuracy of iFR compared to FFR was further evaluated in both the ADVISE II and RESOLVE trials. They concluded that iFR strongly correlated with FFR with a diagnostic accuracy of approximately 80% [20, 22]. In addition to its diagnostic accuracy, one of the primary benefits of iFR is that it is calculated by measuring a natural wave-free period during diastole. Through this measurement, the use of hyperemic agents as well as their potential side effects are avoided. Given the many side effects of hyperemic agents, the use of iFR may be preferred over FFR in the elderly population and patients with baseline sinus node dysfunction [13].
Two large studies have compared the impact of iFR on clinical outcomes to FFR [12, 24]. The DEFINE-FLAIR trial was a large multicenter randomized controlled study that compared the outcomes of patients undergoing iFR-guided PCI to patients undergoing FFR-guided PCI [12]. They concluded that iFR-guided coronary revascularization was noninferior to FFR-guided coronary revascularization regarding 1-year major adverse cardiac events (MACE) [12]. Another multicenter randomized control trial, iFR SWEDEHEART, also concluded that the use of an iFR-guided revascularization strategy in SIHD was noninferior to FFR, with respect to 1-year MACE [24]. Although both the DEFINE-FLAIR and iFR SWEDEHEART trials demonstrated that iFR is noninferior to FFR, questions remain about the use of iFR without also measuring FFR. We believe that the primary concern is likely driven by an iFR to FFR discordance rate of approximately 20% as well as limited data on the causative factors leading to discordance.
Discordance is considered when iFR or FFR is positive, and the other is
negative. Negative discordance is defined by a FFR
Multiple studies have found that the agreement between iFR and FFR is around 80%, which indicates that approximately 20% of iFR and FFR measurements are discordant [20, 21, 22, 23, 24, 25]. Experts have recently shifted focus to further understand the etiology of iFR and FFR discordance as well as factors leading to negative (FFR+/iFR–) or positive (FFR–/iFR+) discordance.
Measurement variability has been found to be a major source of discordance
between iFR and FFR, primarily around the cutoff values of
There are many pathophysiological factors reported in the literature that can lead to iFR and FFR discordance (Table 1 and Fig. 1, Ref. [25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38]). Sex differences have been associated with both positive and negative discordance [25, 26, 27, 28]. Specifically, females are more commonly found to have positive discordance while males are more likely to have negative iFR and FFR discordance [25, 26, 27, 28]. In a large post hoc analysis, Dérimay et al. [29] demonstrated that younger age was associated with negative discordance while older age was associated with positive discordance. Similarly, Goto et al. [30] also concluded that younger age correlated with negative discordance.
| Study | Study type | No. of patients | Factors of discordance | Negative or positive discordance |
| Aoi et al. [25] | Single-center, retrospective study | 423 | Male sex. | Negative |
| Female sex. | Positive | |||
| Dérimay et al. [29] | Post hoc analysis | 587 | Stenosis location (left main or proximal LAD), more severe stenosis, younger age, and slower heart rate. | Negative |
| Absence of a beta-blocker, older age, and less severe stenosis. | Positive | |||
| Satomi et al. [26] | Retrospective study | 225 | Lower heart rate, lower double products, and lower cardiac index. | Negative |
| Female sex, higher heart rate, and higher double products. | Positive | |||
| Goto et al. [30] | Post hoc analysis | 156 | Younger age, absence of diabetes and higher hemoglobin levels. | Negative |
| Hemodialysis, peripheral artery disease, left main and LAD artery stenosis. | Positive | |||
| Kobayashi et al. [31] | Multicenter, prospective, investigator-initiated observational study | 763 | Left main/ proximal LAD artery stenosis. | Negative |
| Warisawa et al. [33] | Analysis of international multicenter registry | 345 | Focal pattern of CAD. | Negative |
| Diffuse pattern of CAD. | Positive | |||
| Arashi et al. [27] | Retrospective study | 225 | Not being on hemodialysis. | Negative |
| Female sex and high rate-pressure product. | Positive | |||
| Scarsini et al. [34] | Prospective, observational study | 66 | Aortic valve stenosis after TAVI | - |
| Ge et al. [35] | Computational model | - | Aortic valve disease, regurgitation and stenosis. | Positive |
| Lee et al. [28] | Post hoc analysis | 393 | Male sex, absence of diabetes and lower percent diameter stenosis. | Negative |
| Female sex, diabetes, smaller reference vessel diameter and higher percent diameter stenosis. | Positive | |||
| Tahir et al. [37] | Single-center, nonrandomized both retrospective and prospective study | 65 | Elevated left ventricular end diastolic pressure | - |
| Tahir et al. [38] | Single-center nonrandomized retrospective observational study | 100 | Left ventricular diastolic dysfunction | - |
| Abbreviations: CAD, coronary artery disease; LAD, left anterior descending; TAVI, transcatheter aortic valve implantation. | ||||
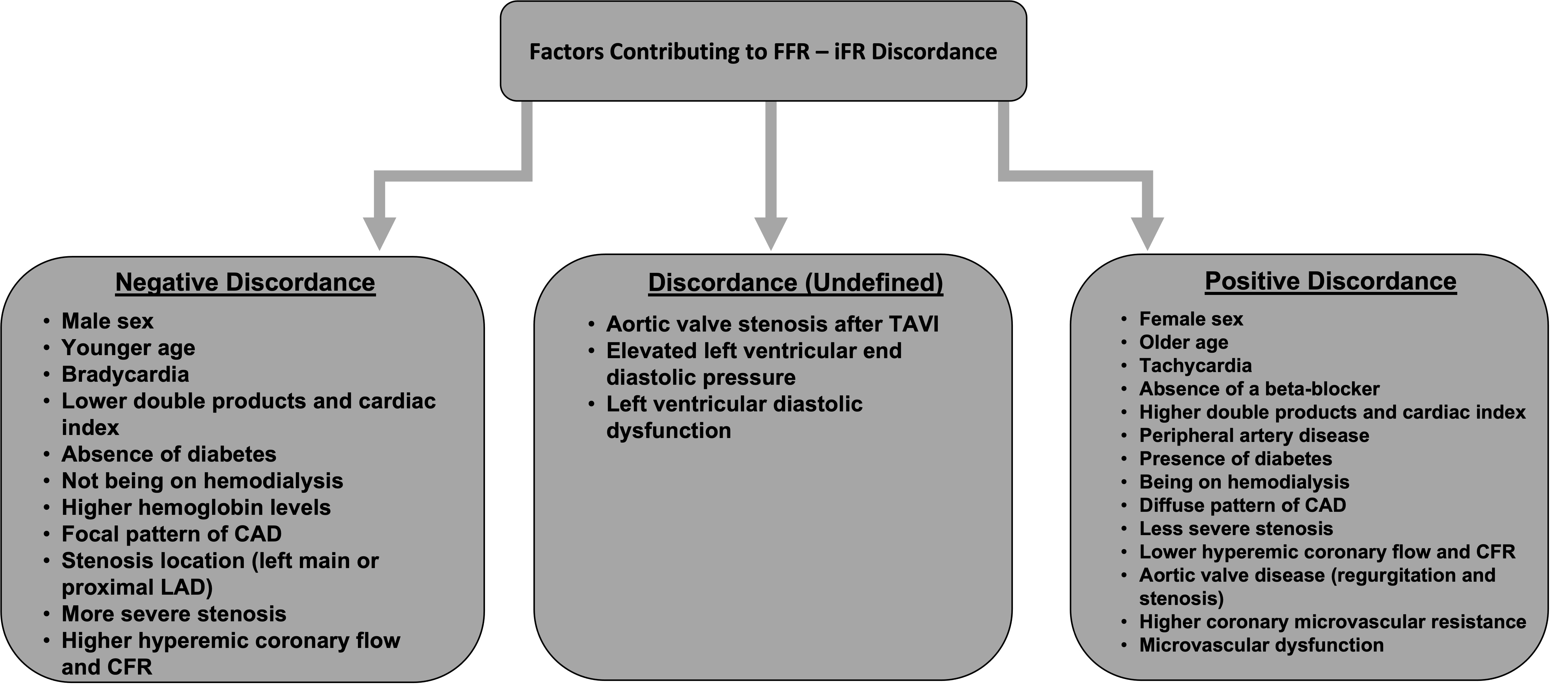 Fig. 1.
Fig. 1.Factors reported by various studies contributing to positive discordance (FFR–/iFR+), negative discordance (FFR+/iFR–), or undefined discordance. Abbreviations: CAD, coronary artery disease; LAD, left anterior descending; TAVI, transcatheter aortic valve implantation; CFR, coronary flow reserve.
The impact of coronary artery disease on iFR and FFR agreement has also been investigated including the location of coronary stenosis, severity of stenosis, and overall extent of coronary disease [29, 30, 31, 32, 33]. Dérimay et al. [29] demonstrated that left main coronary artery or proximal left anterior descending (LAD) artery stenosis was associated with negative discordance. A large multicenter prospective observational study also found that left main coronary artery and proximal LAD artery stenosis were significant factors leading to negative discordance [31]. In contrast, Goto et al. [30] found that left main coronary artery and proximal LAD artery stenosis contributed to positive discordance. The discrepancies between these studies are unclear, however they demonstrate the underlying complexity of CAD pathophysiology.
There is conflicting data regarding the impact of coronary artery stenosis severity on iFR and FFR discordance. Lee et al. [32] found lower percent diameter coronary artery stenosis was associated with negative discordance whereas smaller coronary artery diameter/ higher percent diameter stenosis led to positive discordance. Dérimay et al. [29] found the opposite, in that more severe stenosis correlated with negative discordance while less severe stenosis was associated with positive discordance. In addition to the location and severity of stenosis, the extent of coronary artery disease can contribute to iFR and FFR discordance. Warisawa et al. [33] concluded that patients with a focal pattern of CAD were associated with negative discordance whereas a diffuse pattern of CAD correlated with positive discordance.
Valvular heart disease has also been linked to iFR and FFR discordance. Scarsini et al. [34] found that transaortic gradient pressure changes induced by transaortic valve intervention caused significant variations in iFR measurements. Similarly, a computational model that evaluated the effects of aortic valve disease on iFR and FFR discordance found that aortic stenosis and regurgitation led to positive discordance [35]. Overall, data on the effects of valvular heart disease on iFR and FFR discordance is limited and necessitates further investigation.
Central venous pressure (Pv) is ignored in calculating FFR as it is assumed to be close to zero. This can be a problem in conditions where Pv is significantly elevated. For example, right and left heart conditions associated with high central venous pressure can theoretically result in erroneous calculation of FFR. In practice, the impact has been demonstrated to be trivial [36]. Such studies, however, did not focus on iFR and FFR discordance. In our own experience, elevated LVEDP resulted in a graded, higher discordance between iFR and FFR [37].
We recently published two studies that evaluated the effects of elevated left ventricular end diastolic pressure (LVEDP) and left ventricular diastolic dysfunction on FFR and iFR discordance [37, 38]. We found that approximately 43% of patients with elevated LVEDP had FFR and iFR discordance [37]. Therefore, we concluded that patients with elevated LVEDP were more likely to have discordant iFR and FFR measurements compared to patients with normal LVEDP. Similarly, the impact of left ventricular diastolic dysfunction on FFR and iFR discordance was significant. We found that approximately 45% of patients with discordance had left ventricular diastolic dysfunction based on transthoracic echocardiography [38]. Therefore, we believe that both LVEDP and left ventricular diastolic function should be considered when using FFR and iFR to guide PCI.
The effects of diabetes and hemodialysis on FFR and iFR discordance has been presented in the literature [27, 28, 30, 35]. Goto et al. [30] concluded that diabetics and patients on hemodialysis were commonly found to have positive discordance. Similarly, Lee et al. [32] found that diabetes is associated with positive discordance while the absence of diabetes is associated with negative discordance. The effects of diabetes on discordance have been linked to dysfunctions in coronary artery microcirculation [17, 32, 35, 39]. Recent studies have attempted to further understand the impact of the coronary microcirculation dysfunction on FFR and iFR discordance (Table 2, Ref. [32, 35, 39, 40]). According to van de Hoef et al., both healthy and dysfunctional coronary microcirculation can contribute to discordance. They further explain that healthy coronary microcirculation allows for adenosine-mediated vasodilation during periods of hyperemia causing a significant pressure gradient that was not present during non-hyperemic states [17]. Therefore, patients with non-flow-limiting CAD and normal coronary microcirculation can have a positive FFR but a negative iFR [17, 39]. In contrast, adenosine-mediated coronary vasodilation is inhibited in patients with microcirculation dysfunction, such as diabetics, and therefore are more likely to have a normal FFR but an abnormal iFR [39]. Lee et al. [40] concluded that patients with negative discordance were found to have higher hyperemic myocardial blood flow, higher coronary flow reserve, and a significantly higher reduction of microvascular resistance at hyperemia. These findings are likely secondary to the presence of healthy microcirculation allowing for coronary vasodilation and thus large pressure gradients across coronary lesions during hyperemia. In a computational model, Ge et al. [35] concluded that diabetic patients with secondary coronary microcirculation dysfunction had higher coronary microvascular resistance and lower coronary flow during hyperemia. Similarly, Lee et al. [32] concluded that male sex and a lower probability of predictors of microvascular dysfunction are associated with negative discordance while older age, female sex, diabetes, and possible microvascular dysfunction are associated with positive discordance. We believe that coronary microcirculation dysfunction contributes significantly to FFR and iFR discordance, however, additional studies are needed.
| Study | Study type | No. of patients | Factors and associated findings of discordance | Negative or positive discordance |
| Ge et al. [35] | Computational model | - | Diabetes, higher coronary microvascular resistance, lower coronary flow | Positive |
| Cook et al. [39] | Post hoc, retrospective analysis | 454 | Higher hyperemic coronary flow and CFR, and lower prevalence of diabetes. | Negative |
| Lower hyperemic coronary flow and CFR, and higher prevalence of diabetes. | Positive | |||
| Lee et al. [40] | Retrospective analysis | 113 | Higher coronary flow, higher CFR and significantly higher reduction of microvascular resistance during hyperemia | Negative |
| Lee et al. [32] | Post hoc, retrospective analysis | 393 | Male sex and lower probability of predictors of microvascular dysfunction. | Negative |
| Older age, female sex, diabetes, and microvascular dysfunction. | Positive | |||
| Abbreviations: CFR, coronary flow reserve. | ||||
Despite the many benefits of iFR, its use in the catheterization lab, independent of FFR, is variable. To determine the hemodynamic significance of an intermediate coronary lesion, iFR is commonly measured and then confirmed with FFR. The use of FFR to confirm iFR is primarily due to the known 20% diagnostic inaccuracy of iFR compared to FFR as well as its novelty. To support the independent use of iFR, studies have compared long-term clinical outcomes of patients with concordant iFR and FFR indices to those with discordant measurements. While initial studies demonstrated no increased risk in vessel-oriented composite outcomes (VOCO) or Patient-oriented composite outcomes (POCO) for patients with discordant values, more recent studies have challenged these conclusions [32, 41, 42]. Lee et al. [43], found that patients with discordant iFR and FFR values, in which revascularization was deferred, demonstrated a similar risk of VOCO when compared to all revascularized lesions up to 5 years of follow-up. Given these findings, the authors concluded that lesions with discordant physiologic indices require close follow-up and medical management [43].
While the decision to revascularize is straightforward with concordant FFR and iFR values, interpreting discordant values is more complex in the clinical setting [44]. Overall, discordance has complicated the management of intermediate coronary lesions. Currently, there is no clear evidence to support whether iFR or FFR should be used to guide PCI in the setting of discordance. Therefore, when iFR and FFR discordance is encountered in the clinically setting, the decision to revascularize is left to the proceduralist. Depending on prior training and comfortability with iFR, some operators will revascularize a positive discordant (FFR–/iFR+) intermediate coronary lesion if their clinical suspicion is high that it is the culprit. However, many proceduralist question the clinical equivalency of iFR to FFR given the frequency of discordant measurements and are thus, faced with the dilemma on whether to revascularize. Most commonly, operators follow FFR to guide their decision to revascularize an intermediate coronary lesion in the setting of negative discordance (FFR+/iFR–). As previously discussed, this is secondary to the operators’ prior experience with iFR as well as uncertainties due to the lack of standardized guidelines and inconsistent clinical outcome data on the revascularization of iFR and FFR discordant lesions.
While some have concluded that iFR is a suitable and cost-effective alternative
to FFR, others have adopted iFR-FFR hybrid models [14]. These hybrid models have
expanded the standard cutoff value for iFR, which has increased confidence in its
use and decreased the frequency of having to interpret discordant values. With
most hybrid strategies, revascularization is performed on lesions with an iFR of
The diagnostic accuracy and clinical benefits of iFR compared to FFR in stable ischemic heart disease have been clearly outlined in the literature and supported by multiple large randomized clinical trials. However, given that the percentage of FFR and iFR discordance was not negligible in these studies, it must be considered when using these measurements to guide PCI. Recently, efforts have been made to identify the factors leading to FFR and iFR discordance. Common factors identified include gender, coronary artery stenosis severity and location, heart rate, and valvular heart disease. More recent studies found that elevated LVEDP and the presence of diastolic dysfunction are important factors of discordance that should be considered when interpreting iFR and FFR. Additionally, the presence of diabetes as well as hemodialysis have been identified as discordance causing factors primarily through their effects on the coronary microvasculature. Although multiple causative factors have been identified and presented in the literature, we believe that further studies are necessary to identify additional factors of discordance and to further investigate the impacts of coronary microvascular dysfunction.
All authors reviewed the literature and helped write the manuscript. BF, HT, JL, and RB—performed critical revisions of the article and approved the final version of manuscript.
Not applicable.
We would like to express our gratitude to all those who helped us during the writing of this manuscript. We would also like to thank all the peer reviewers for their opinions and suggestions.
This research received no external funding.
The authors declare no conflict of interest.