




1 Department of Cardiology, Tianjin Chest Hospital, 300000 Tianjin, China
2 Department of Pneumology, Tianjin Chest Hospital, 300000 Tianjin, China
†These authors contributed equally.
Academic Editors: Brian Tomlinson and Takatoshi Kasai
Abstract
Background: For women presenting with stable chest pain (SCP), the
appropriate risk assessment strategy to identify individuals unlikely to benefit
from further cardiovascular imaging testing (CIT) is debatable. Thus, the present
study intended to compare two risk assessment strategies in these individuals.
Methods: 2592 women with SCP who underwent coronary computed tomography
angiography (CCTA) were divided into low and high risk group according to 2016
National Institute of Health and Care Excellence guideline-determined strategy
(NICE strategy) and 2019 European Society of Cardiology guideline-determined
strategy (ESC strategy), respectively. The associations of coronary artery
disease (CAD), major adverse cardiovascular event (MACE) and other subsequent
clinical outcomes with risk groups and net reclassification improvement (NRI)
were evaluated to compare different strategies. Results: Both NICE
strategy which focused on symptom evaluation and ESC strategy which was based on
pretest probability (PTP) determined by ESC-PTP model and
coronary artery calcium score-weighted clinical likelihood (CACS-CL) model
classified a proportion (34.49% and 63.97%, respectively) of individuals into
the low risk group. Compared to NICE strategy, ESC strategy indicated stronger
associations between risk groups and obstructive CAD (odds ratio: 27.63 versus
3.57), MACE (hazard ratios: 4.24 versus 1.91), more intensive clinical management
as well as a positive NRI (27.71%, p
Keywords
- Risk assessment strategy
- Stable chest pain
- Coronary artery calcium score
- Women
- Pretest probability
- Coronary computed tomography angiography
Coronary artery disease (CAD) is a previously underestimated cause of morbidity and mortality in women [1, 2]. Major differences exist in the risk factors and clinical presentation in women compared to men [3, 4], which influence designing an effective risk assessment strategy and evaluating the potential referral to cardiovascular imaging testing (CIT) [5, 6]. Recently, data from four large CIT-based clinical trials demonstrated the discrepancy among high burden of traditional risk factors, atypical symptom and low prevalence of obstructive CAD, highlighting the need for optimal strateges to the evaluation and diagnosis of obstructive CAD in women presenting with stable chest pain (SCP) [7, 8, 9, 10].
The 2016 U.K. National Institute of Health and Care Excellence (NICE) guideline offered a strategy recommending coronary computed tomography angiography (CCTA) for all individuals with typical and atypical angina or abnormal electrocardiogram (ECG) [11]. However, this symptom-based risk assessment strategy for SCP has been controversial since release [12, 13, 14] and numerous studies has indicated that atypical symptoms were more likely to be a manifestation of SCP in women [3, 4, 7, 8, 9, 10]. Separately, the 2019 European Society of Cardiology (ESC) guideline advocated an updated pretest probability (PTP) model and recommended CIT for individuals with high ESC-PTP [15]. For individuals with borderline ESC-PTP, a new concept of clinical likelihood (CL) incorporating risk factors of CAD other than age, sex, and type of SCP was introduced [15] and Winther et al. [16] developed two models for the estimation of CL: risk factor-weighted CL (RF-CL) model and coronary artery calcium score (CACS)-weighted CL (CACS-CL) model.
2016 NICE guideline-determined risk assessment strategy (NICE strategy) [17, 18], ESC-PTP model [19], RF-CL model and CACS-CL model [16] has been externally validated in general SCP individuals. But to date, no comparative analysis has been conducted to systematically evaluate NICE strategy and 2019 ESC guideline-determined risk assessment strategy (ESC strategy) in women with SCP, for whom the appropriate decision-making of CIT was important but difficult [5, 6]. Thus, we aimed to compare the effectiveness of two newest risk assessment strategies to optimize downstream clinical management in a CCTA-based cohort comprised of women presenting with SCP.
In Tianjin Chest Hospital, 5289 individuals referred to CCTA for assessment of SCP indicative of obstructive CAD were included from December 2015 to December 2017, and details about the total cohort were presented as previously described [20, 21, 22]. In this subgroup analysis, 2592 women were included and followed up until December 2019.
Baseline data including age, hypertension, hyperlipidemia, smoking, abnormal ECG and symptom were collected as described previously [20, 21, 22]. SCP symptom were categorized as nonanginal chest pain, atypical angina, or typical angina [23].
Based on each strategy, CIT should be not referred for an individual at low risk. Details of risk groups in NICE and ESC strategy were as follows [11, 15]:
NICE strategy: Individuals with nonanginal SCP and normal ECG were divided into low risk group. Individuals with typical and atypical angina or nonanginal SCP with abnormal ECG were divided into high risk group [11].
ESC strategy: PTP of obstructive CAD was determined according to the ESC-PTP
model based on age, sex and symptom [15]. Individuals with ESC-PTP
For further investigation of the impact of CACS, we also used RF-CL model which had the same clinical variables as CACS-CL model [16] to classify individuals with ESC-PTP of 5–15%.
The imaging data collection of CACS and CCTA were conducted as described
previously [20, 21, 22, 24]. Obstructive CAD was defined as present if an individual
had at least one lesion with
After CCTA, all individuals were followed at 6, 12, 24, 36 and 48 months by phone call or physician visit. The primary endpoint was major adverse cardiovascular events (MACE) and it was defined as cardiac death and myocardial infarction. Cardiac death was defined as any death caused by cardiac disease or for which no other cause could be found. Myocardial infarction was defined according to the Fourth Universal Definition of Myocardial Infarction [25]. The changes of downstream clinical management within 60 days after CCTA were identified on electronic medical system and the secondary endpoint included increase of medication (IM), invasive coronary angiography (ICA) and coronary revascularization (CR). All endpoints were adjudicated via review of follow-up information and medical records by an independent clinical event committee who were blinded to other data.
R (version 3.2.4; R Foundation for Statistical Computing, Vienna, Austria) and
MedCalc (version 15.2.2; MedCalc Software, Mariakerke, Belgium) were used for all
statistical analyses. Student’s t-test and Mann Whitney U-test were used
to compare differences for continuous data as appropriate. Fisher exact test or
According to NICE strategy, of the 2592 women, 34.49% (894/2592) were divided
into low risk group. Among 855 individuals with ESC-PTP of 5–15%, 529
individuals had a CACS-CL
| Total | NICE strategy | p | ESC strategy | p | ||||
| Low | High | Low | High | |||||
| n = 2592 | n = 894 | n = 1698 | n = 1658 | n = 934 | ||||
| Age |
58.2 |
56.9 |
58.9 |
56.8 |
60.7 |
|||
| Diabetes | 570 (22) | 172 (19) | 398 (23) | 0.0162 | 298 (18) | 272 (29) | ||
| Hypertension | 1166 (45) | 375 (42) | 791 (47) | 0.0268 | 680 (41) | 487 (52) | ||
| Hyperlipidemia | 829 (32) | 250 (28) | 579 (34) | 0.0017 | 448 (27) | 382 (41) | ||
| Smoking | 441 (17) | 125 (14) | 316 (19) | 0.0034 | 199 (12) | 242 (26) | ||
| Family history | 881 (34) | 286 (32) | 595 (35) | 0.1298 | 514 (31) | 367 (39) | ||
| Abnormal ECG | 752 (29) | 0 (0) | 752 (44) | 448 (27) | 304 (32) | |||
| Symptom | ||||||||
| Nonanginal chest pain | 934 (36) | 894 (100) | 40 (2) | 746 (45) | 188 (20) | |||
| Atypical anginal | 1270 (49) | 0 (0) | 1270 (75) | 812 (49) | 458 (49) | |||
| Typical anginal | 388 (15) | 0 (0) | 388 (23) | 99 (6) | 289 (31) | |||
| CACS |
3 (0–79) | 2 (0–48) | 14 (0–175) | 0 (0–25) | 31 (3–254) | |||
| Values are presented as n (%) unless stated otherwise. NICE strategy, 2016 National Institute of Health and Care Excellence guideline-determined risk assessment strategy; ESC strategy, 2019 European Society of Cardiology guideline-determined risk assessment strategy; ECG, electrocardiogram. | ||||||||
As shown in Fig. 1, no, nonobstructive and obstructive CAD was found on CCTA in
493, 804 and 1295 individuals, respectively. Compared to individuals in low risk
group, individuals in high risk group had more obstructive CAD [NICE strategy:
8.39% (75/894) versus 24.62% (418/1698), odds ratio: 3.57, 95% CI: 2.75–4.63,
p
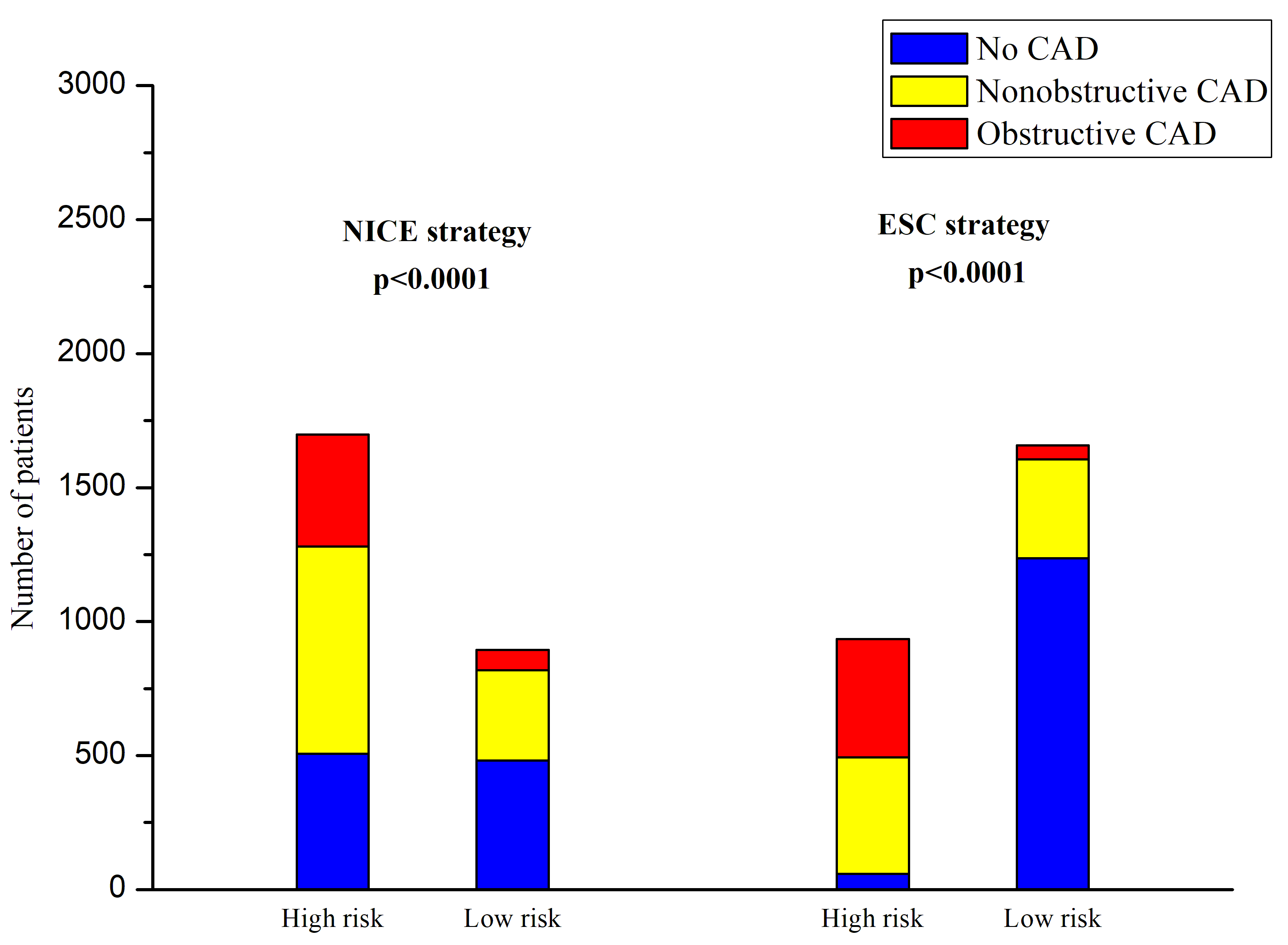 Fig. 1.
Fig. 1.Distribution of CAD in different risk groups. NICE strategy, 2016 National Institute of Health and Care Excellence guideline-determined risk assessment strategy; ESC strategy, 2019 European Society of Cardiology guideline-determined risk assessment strategy; CAD, coronary artery disease.
Individuals were followed for 25 (interquartile range: 20 to 32) months. During
the follow-up, 87 individuals experienced MACE: 11 individuals died from cardiac
cause and 76 individuals suffered from nonfatal MI. Fig. 2 illustrates
Kaplan–Meier estimates of individuals surviving free from MACE. High risk group
according to both NICE and ESC strategy had a significantly higher risk of MACE,
respectively (p for log-rank test: 0.0194 for NICE strategy and 0.0001
for ESC strategy), but the association of ESC strategy-determined risk groups
(high versus low) with MACE was stronger than that of NICE strategy (HR for NICE
strategy: 1.78, 95% CI: 1.09–2.90, p = 0.0221 and HR for ESC strategy:
5.10, 95% CI: 3.15–8.26, p
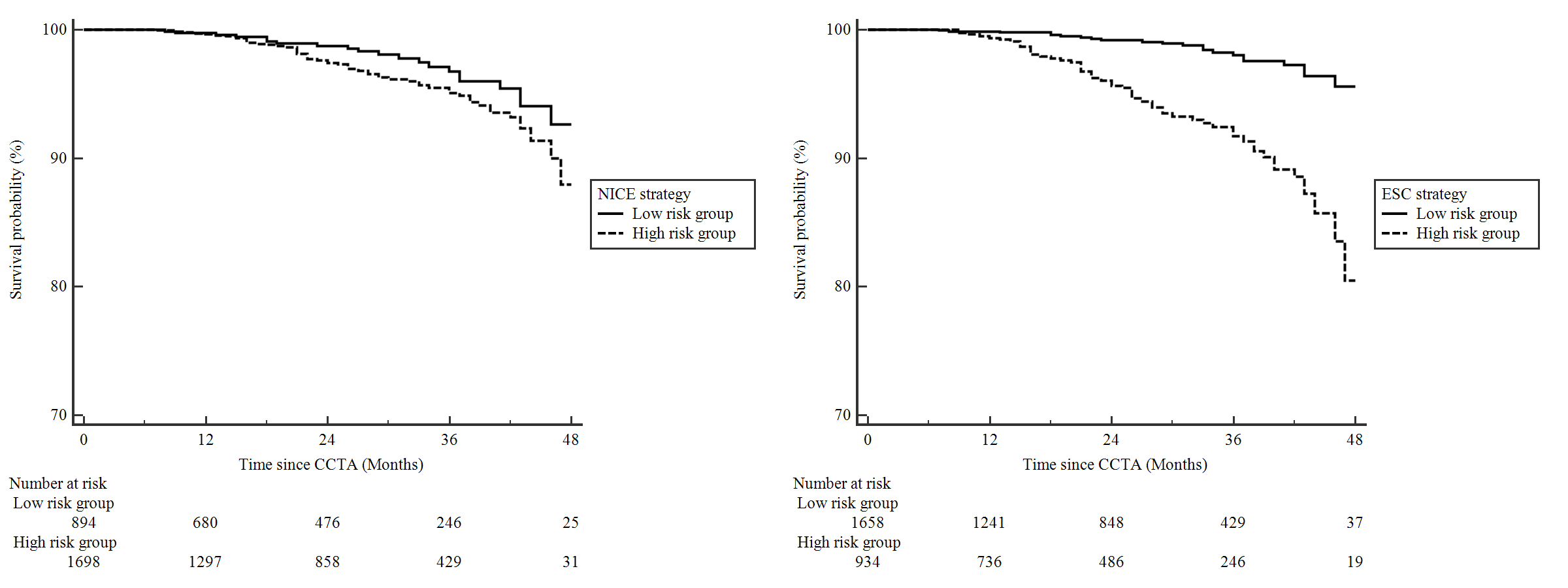 Fig. 2.
Fig. 2.Kaplan–Meier curves comparing high and low risk groups determined by NICE and ESC strategy. Abbreviations as in Fig. 1.
As shown in Fig. 3, 761 individuals were referred to ICA after CCTA and 163
individuals underwent CR. In both strategies, rates of three secondary endpoints
were significantly (p
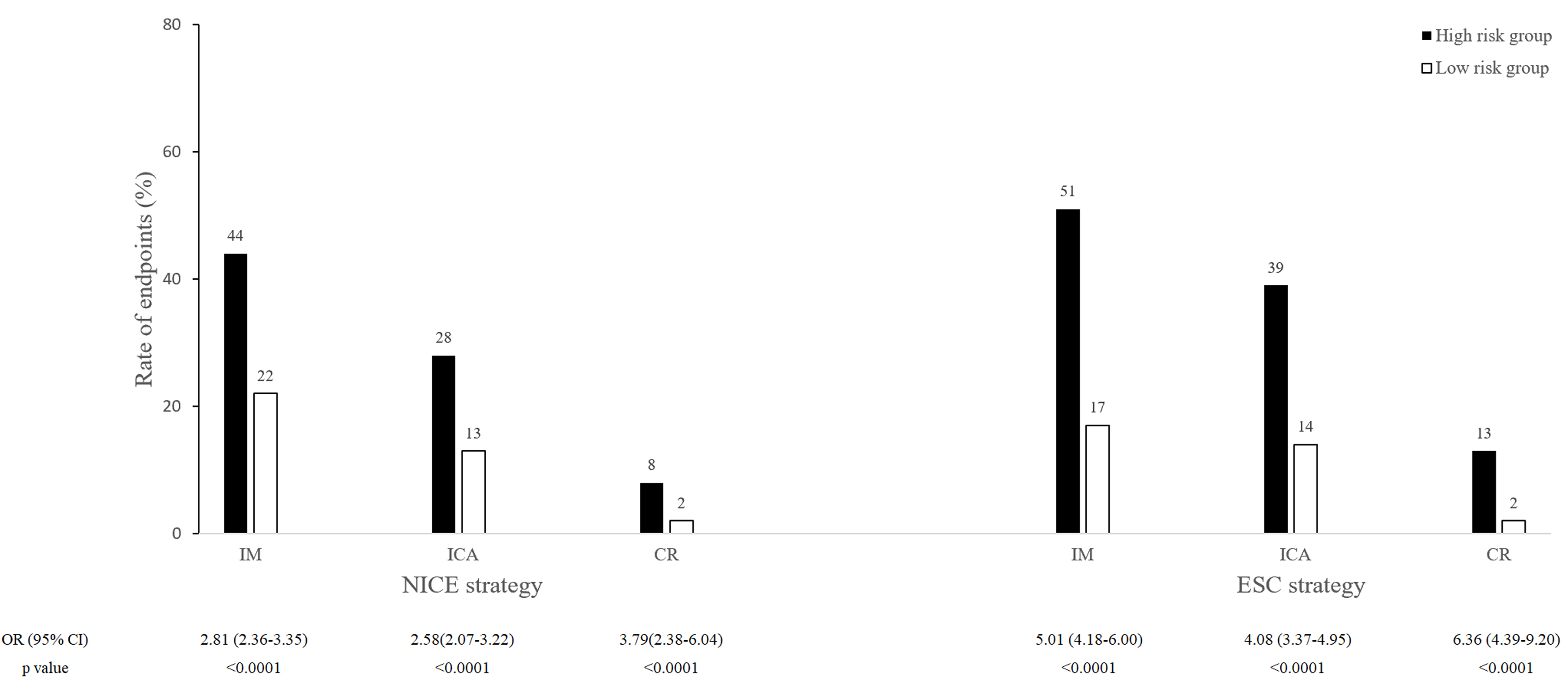 Fig. 3.
Fig. 3.Rates for secondary endpoints in low and high risk groups determined by NICE and ESC strategy. IM, Increase of medication; CR, coronary revascularization; ICA, invasive coronary angiography; OR, odds ratio; CI, confidence interval; Other abbreviations as in Fig. 1.
In Table 2, compared to NICE strategy, ESC strategy correctly divided 843 from
high to low risk, but 56 from low to high in the 2099 negative individuals. Of
the 493 positive individuals, 36 were correctly divided to high risk but 13 to
low. Thus, compared to NICE strategy, the NRI for ESC strategy was 37.49% for
negative, 4.66% for positive, and 42.15% for all (p
When replacing CACS-CL model with RF-CL model in individuals with borderline ESC-PTP and comparing ESC strategy (without CACS) to NICE strategy in Table 3, only 224 negative individuals were correctly reclassified into low risk by ESC strategy (without CACS) and the NRI was attenuated markedly (7.05% in negative and 8.47% in all). Thus, comparing ESC strategy to NICE strategy in Table 2, the correct reclassification of 843 negative individuals should be in large measure (73.43%, 619/843) attributed to the application of CACS in 855 individuals with borderline ESC-PTP. Moreover, only 1 of the 619 individuals suffered from nonfatal myocardial infarction and no individual died in the follow-up.
| Risk groups by ESC strategy | Total | Reclassification |
NRI |
p | ||||
| Low | High | Up | Down | |||||
| Risk groups by NICE strategy | ||||||||
| Negative patients | 2.67% | 40.16% | 42.15% | |||||
| Low | 763 | 56 | 819 | |||||
| High | 843 | 437 | 1280 | |||||
| Total | 1606 | 493 | 2099 | |||||
| Positive patients |
7.30% | 2.64% | ||||||
| Low | 39 | 36 | 75 | |||||
| High | 13 | 405 | 418 | |||||
| Total | 52 | 441 | 493 | |||||
| NICE strategy, 2016 National Institute of Health and Care Excellence
guideline-determined strategy; ESC strategy, 2019 European Society of Cardiology
guideline-determined strategy; CAD, coronary artery disease; NRI, net
reclassification improvement. | ||||||||
| Risk groups by ESC strategy (without CACS) | Total | Reclassification |
NRI |
p | ||||
| Low | High | Up | Down | |||||
| NICE strategy | ||||||||
| Negative patients | 3.62% | 10.67% | 8.47% | |||||
| Low | 743 | 76 | 819 | |||||
| High | 224 | 1056 | 1280 | |||||
| Total | 967 | 1132 | 2099 | |||||
| Positive patients |
3.65% | 2.23% | ||||||
| Low | 57 | 18 | 75 | |||||
| High | 11 | 407 | 418 | |||||
| Total | 68 | 425 | 493 | |||||
| NICE strategy, 2016 National Institute of Health and Care Excellence
guideline-determined strategy; ESC strategy, 2019 European Society of Cardiology
guideline-determined strategy; CACS, coronary artery calcium score; CAD, coronary
artery disease; NRI, net reclassification improvement. | ||||||||
In this CCTA-based cohort comprised of women with SCP, we demonstrated that based on current two risk assessment strategies, low risk groups were associated with fewer obstructive CAD, MACE and changes of downstream management than high risk groups did. Compared to NICE strategy which focused on symptom evaluation, ESC strategy seemed to be associated with greater effectiveness in identifying individuals at low risk. The superiority of ESC strategy could be mainly due to the application of CACS in individuals with borderline ESC-PTP, suggesting that a sequential instrument incorporating CACS with PTP estimation might offer effective deferral for CIT in women presenting with SCP.
In the present study, NICE strategy seemed to be associated with less effectiveness in identifying individuals at low risk compared to ESC strategy. It has been well established that women more often had traditional risk factors, atypical symptoms which might result from the low ability to exercise maximally and high prevalence of nonobstructive and small vessel disease, and lower rates of obstructive CAD than men [3, 7]. In line with these, only 19.02% (493/2592) individuals had obstructive CAD detected on CCTA and nearly half (49.00%, 1270/2592) reported atypical anginal in this study. Thus, although NICE strategy improved clinical outcomes compared to traditional strategies in general SCP individuals [17, 18], the suboptimal performance of NICE strategy may, to a large extent, be attributed to the insufficient power of symptom evaluation alone in women with SCP.
Among the new predictors of obstructive CAD, CACS has been proved to offer the most incremental information of diagnosis and prognosis above traditional cardiovascular risk factors [27, 28, 29]. Moreover, there was a significant increase in clinically useful reclassification when CACS was added to the risk assessment for women [30]. Thus, to permit more accurate risk assessment in women with a borderline ESC-PTP, we used CACS-CL model which incorporated clinical variables plus CACS and revealed the most robust determination of PTP among proposed models [16]. We also replaced CACS-CL model by RF-CL model which had the same clinical variables as CACS-CL model [16] and found that the additional application of CACS made a major contribution to the remarkably risk assessment improvement of ESC strategy. This paradigm incorporating CACS for borderline individuals showed paramount safety according to the extremely low likelihood (3.14%, 52/1658) of obstructive CAD and rate (1.33%, 22/1658) of cardiovascular events in low risk group. In this context, more emphasis should be placed on ESC strategy for the effective identification of women with SCP who may derive minimal benefit from further CIT in clinical practice. It also bears mentioning that ESC strategy would avoid unnecessary CIT at the expense of additional CACS scans. Thus, cost-effectiveness evaluation of this attractive risk assessment strategy for women with SCP is needed in the further.
Although this is the first study to evaluate current risk assessment strategies for women with SCP, several issues merit consideration. First, this study was an observational cohort. Clinical management of individuals before and after CCTA were relied on local physician. Thus, whether ESC strategy will lead to more appropriate decision-making of downstream referral and better clinical outcomes for women with SCP need to be addressed in future studies, such as randomized controlled trials. Second, accumulating evidence support strategies which suggests widespread CACS screening [8, 30], such as the strategy applying CACS-CL to the entire SCP women [31]. Cost-effectiveness of this strategy warrant further evaluation. Third, using data from PROMISE cohort, Fordyce et al. [32] developed a new tool to identify individuals deriving minimal value from CIT. Although the PROMISE minimal risk tool [33] has been externally validated, no recent clinical guideline recommends it as the risk assessment tool for individuals with SCP. Forth, this analysis focused on the presence of obstructive CAD documented by CCTA. Previous studies have demonstrated that CCTA had a high negative predictive value compared with invasive coronary angiogram [34, 35]. So CCTA could offer robust reassurance for both strategies to exclude obstructive CAD. Moreover, we defined unassessable segments as positive ones based on current guideline recommendations in which further testing should be referred for nonconclusive CCTA. Fifth, some female-specific risk factors, such as estrogen status and gestational diabetes mellitus, have shown the potential to improve risk assessment for women [36]. However, additional tests are needed for these attractive biomarkers and cost-effectiveness of them warrant further evaluation. Finally, the long-term follow-up information of secondary outcomes, such as compliance of medication were not collected.
Compared to symptom-focused strategy, ESC strategy which sequentially amalgamated CACS with PTP estimation might have more potential to effectively identify individuals who may derive minimal benefit from further CIT in women presenting with SCP potentially related to obstructive CAD. For more accurate and convenient risk assessment in these individuals, investigations with comprehensive and rigorous design are needed in the future.
HJ, CF and JZ designed the study. HJ and CF wrote the manuscript. YJ, JF, GL, PR and KR collected data. JZ revised the manuscript and provided help and advice on the statistical analysis. YJ, JF, GL, PR and KR analyzed the data. All authors read and approved the final manuscript.
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Tianjin Chest Hospital (approval number: 2017-KY-004).
We would like to express our gratitude to all those who helped us during the writing of this manuscript. Thanks to all the peer reviewers for their opinions and suggestions.
This study was supported by grants from Research Program of Tianjin Chest Hospital (2018XKC10).
The authors declare no conflict of interest.