
 , Hai-Jian Sun 1,2,*
, Hai-Jian Sun 1,2,*1 Department of Pharmacognosy, State Key Laboratory of Natural Medicines, China Pharmaceutical University, 210009 Nanjing, Jiangsu, China
2 Department of Pharmacognosy, School of Traditional Chinese Pharmacy, China Pharmaceutical University, 211198 Nanjing, Jiangsu, China
3 Department of Physiology, Xuzhou Medical University, 221004 Xuzhou, Jiangsu, China
† These authors contributed equally.
Academic Editors: Brian Tomlinson and Takatoshi Kasai
Abstract
Due to their high prevalence and incidence, diabetes and atherosclerosis are increasingly becoming global public health concerns. Atherosclerosis is one of the leading causes of morbidity and disability in type 1 and/or type 2 diabetes patients. Atherosclerosis risk in diabetic patients is obviously higher than that of non-diabetic individuals. Diabetes-related glycolipid metabolism disorder has been shown to play a central role in atherosclerosis development and progression. Hyperglycemia and dyslipidemia increase the risks for atherosclerosis and plaque necrosis through multiple signaling pathways, such as a prolonged increase in reactive oxygen species (ROS) and inflammatory factors in cardiovascular cells. Notwithstanding the great advances in the understanding of the pathologies of diabetes-accelerated atherosclerosis, the current medical treatments for diabetic atherosclerosis hold undesirable side effects. Therefore, there is an urgent demand to identify novel therapeutic targets or alternative strategies to prevent or treat diabetic atherosclerosis. Burgeoning evidence suggests that plant and herbal medicines are closely linked with healthy benefits for diabetic complications, including diabetic atherosclerosis. In this review, we will overview the utilization of plant and herbal medicines for the treatment of diabetes-accelerated atherosclerosis. Furthermore, the underlying mechanisms of the ethnopharmacological therapeutic potentials against diabetic atherosclerosis are gathered and reviewed. It is foreseeable that the natural constituents from medicinal plants might be a new hope for the treatment of diabetes-accelerated atherosclerosis.
Keywords
- Diabetes
- Atherosclerosis
- Natural medicine
- Phytochemicals
- Therapeutic target
Due to metabolic abnormalities, diabetes is a risk factor for cardiovascular diseases, affecting over 350 million people globally [1]. Long-term hyperglycemia is associated with various micro- and macro-vascular complications, including endothelial cell dysfunction, neuropathy, retinopathy, nephropathy, myocardial infarction, heart failure, and atherosclerosis [2]. Atherosclerosis, a chronic inflammatory disease, is characterized by arterial wall thickening and lipid-enriched plaque formation [3, 4]. Diabetes accelerates atherosclerosis progression and worsens the clinical outcomes. Independently, diabetes mellitus increases the risk of atherosclerosis [5] and the risk of atherothrombotic coronary artery disease is higher in diabetic patients [6]. In the presence of diabetes, atherosclerosis progression, inflammatory cell infiltrations into the vascular wall, and plaque necrosis are markedly accelerated [7]. The effects of diabetes on the occurrence and development of atherosclerosis have been shown in murine models with mutations of key molecules involved in the control of lipid metabolism, such as low density lipoprotein receptor (LDLR) and apolipoprotein E (ApoE) [8]. Various molecular mediators and signaling pathways including excessive reactive oxygen species (ROS) production, increased production of oxidized low density lipoprotein (ox-LDL), insulin resistance, mitochondrial dysfunction, inflammatory microenvironment, increased intracellular formation of advanced glycation end-products (AGEs), transcription factors, non-coding transcripts, and gut microbiota dysfunction are necessary for diabetes to aggravate atherosclerosis progression [9]. Recently, accumulative evidence indicates that epigenetic regulation also plays a key role in the onset and development of diabetes and atherosclerosis, such as DNA methylation, histone modification or non-coding RNAs [10, 11, 12]. It is being accepted that epigenetic mechanisms might serve as an efficient tool to better understand the pathogenesis of diabetes-accelerated atherosclerosis [13]. Despite advances in elucidation of the mechanisms responsible for diabetes-associated atherosclerosis, the molecular events resulting in accelerated atherosclerosis in diabetes mellitus patients have yet to be fully established. Due to the complicated etiologies and individual heterogeneity in diabetic atherosclerosis, an appropriate strategy for the prevention and treatment of diabetic atherosclerosis is necessary [14, 15, 16, 17]. Therefore, it is important to identify novel targets or pharmaceutical agents to inhibit diabetes-accelerated atherosclerotic diseases.
Phytochemicals and traditional Chinese medicine (TCM) have various biologically
active substances that can be used for human disease therapy, including diabetes
and atherosclerosis [18, 19]. For example, as an antimalarial botanical drug,
artemisinin exhibits antidiabetic effects because of its ability to convert
pancreatic cells into functional
Diabetes, a group of metabolic disorders that are characterized by
hyperglycemia, is becoming a serious challenge on global health and economic
development [27, 28]. In 2019, globally, a total of 463 million people were
diagnosed with diabetes. This number is expected to reach 700.2 million by 2045
[29]. Therefore, diabetes is a global chronic disorder that will impose a huge
burden on social, financial, and health systems around the world [30]. Type 1
diabetes is caused by autoimmune destruction of pancreatic beta cells, whereas
type 2 diabetes is characterized by
Atherosclerosis is one of the most dangerous vascular complications of diabetes.
It is characterized by arterial wall thickening, lipid-enriched plaque formation,
and weakening elasticity (Fig. 1) [36]. Interactions among various cell types
promote fatty streak formation, which progresses to atheromatous plaques, plaque
destabilization, and rupture [8]. Since atheroprone endothelial layer is
frequently exposed to low shear stress, blood flow frictional forces prime
endothelial cells for atherogenesis [37]. Endothelial cell injury is an early
event in initiation of vascular homeostasis disturbance, which is reflected by
the release of proinflammatory cytokines and adhesion molecules, including tumor
necrosis factor
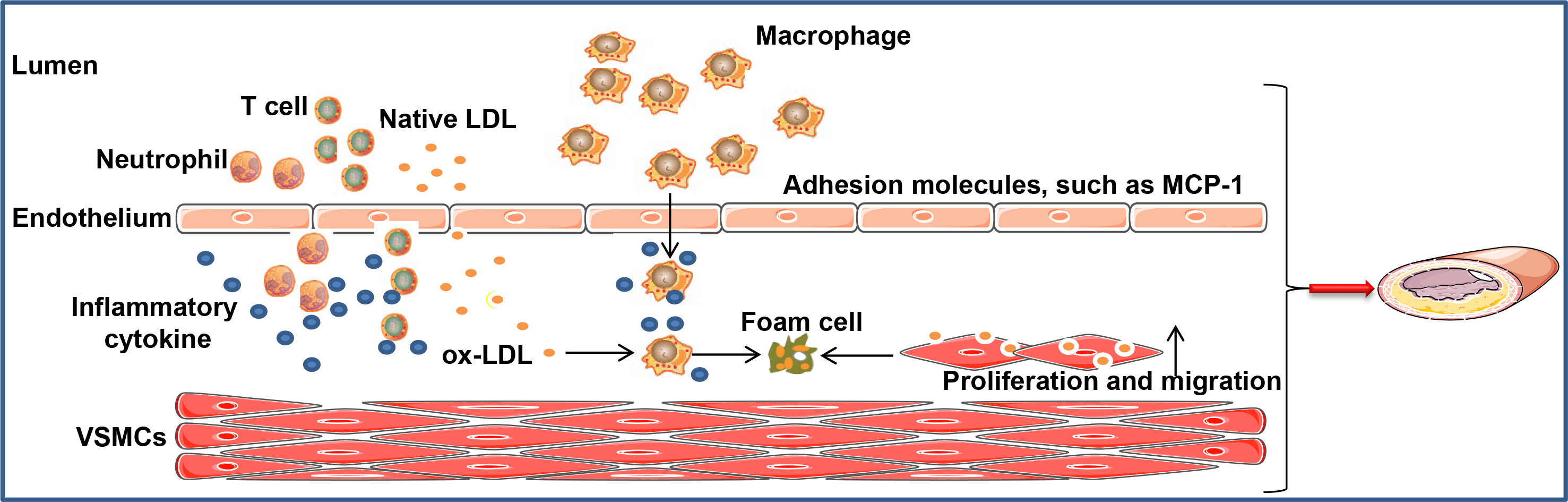 Fig. 1.
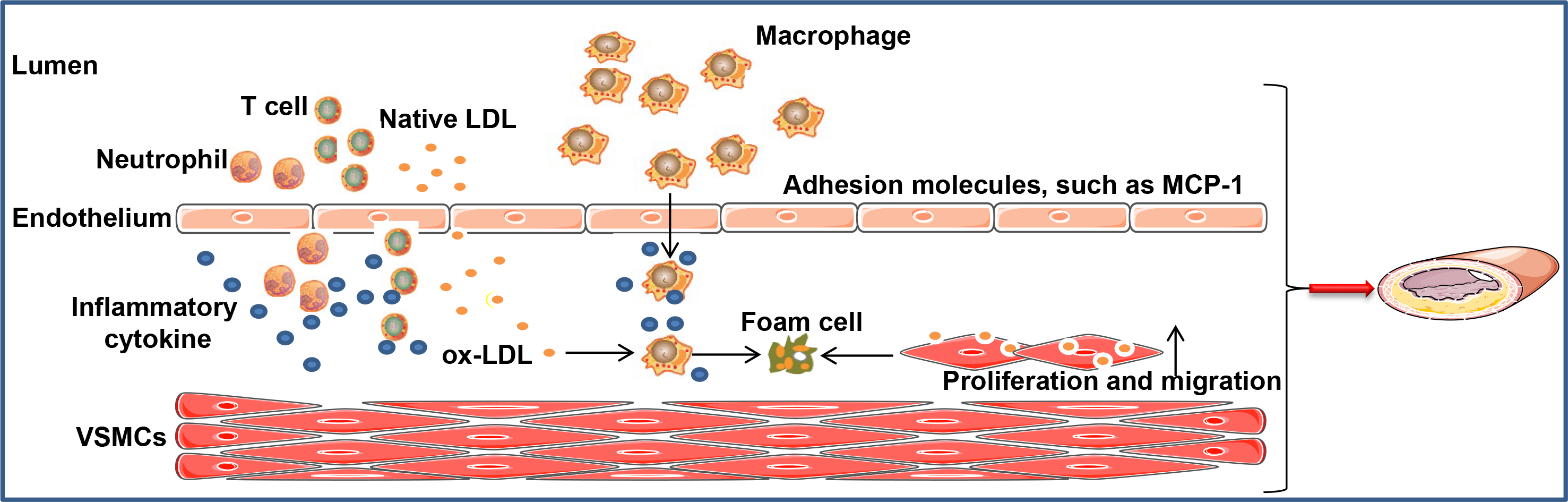
Fig. 1.Formation of atherosclerotic lesions. Vascular endothelial cell injury by pathological wall shear stress, oxidative stress, or other factors induce cholesterol disposition, adhesion molecule expression, and cytokine/chemokine release, resulting in attachment of more monocytes and leukocytes from blood circulation to the endothelium. Immune regulatory factors released by T cells promote atherosclerosis progression. ox-LDL uptake by macrophages is necessary for foam cell generation, facilitating lipid core development. In addition, VSMCs migrate into the intima, where they are proliferative, resulting in overproduction of extracellular matrix. Transformed VSMCs also take up ox-LDL cholesterol, contributing to foam cell formation and atherogenesis. Besides, VSMCs proliferation and migration is an important factor for intimal thickening and sclerosis. ox-LDL, oxidized low density lipoprotein; VSMCs, vascular smooth muscle cells; MCP1, macrophage chemoattractant protein-1.
There is a direct relationship between diabetes and atherosclerosis [40], that is, atherosclerosis development is accelerated in diabetic patients [41]. A systematic review and meta-regression analysis reported that diabetes is a risk factor for carotid atherosclerosis in Chinese adults [42]. Moreover, a systematic review has reported that diabetes is a risk factor for increased carotid intima-media thickness and carotid plaques [43]. A cross-sectional baseline study was performed to evaluate the prevalence of complications and associated clinical characteristics in 6958 newly diagnosed type 2 diabetic patients. It was found that one-third of type 2 diabetic patients had microvascular and macrovascular complications at the time of diagnosis [44]. Through multidetector computed tomography angiography, the incidence of single and multiple vascular diseases in diabetic patients was found to be higher than in non-diabetic patients [45], suggesting a high burden of atherosclerotic plaque in diabetic patients. Increasing global burden of atherosclerosis necessitates the development of effective preventive health strategies and early-detection of cardiovascular complications, especially in diabetic patients. High-quality epidemiological studies on carotid atherosclerosis should aim at elucidating the prognostic value of differences in plaque characteristics observed among diabetic patients. Effective strategies for primary prevention and management of carotid atherosclerosis will improve the quality of life for patients with diabetic atherosclerosis.
Globally, diabetes and atherosclerosis are highly prevalent, with the number of
new morbidities increasing annually. Therefore, studies have aimed at elucidating
the molecular mechanisms through which diabetes accelerates atherosclerosis.
These studies have used murine models with mutations in key molecules involved in
regulation of lipid metabolism, such as ApoE and LDLR under high-fat
high-cholesterol diets [46]. Recent studies have documented the molecular
mechanisms underlying diabetes-associated atherosclerosis. They include
hyperglycemia, glycosylation, AGEs overproduction, insulin dysfunction,
endoplasmic reticulum stress, mitochondrial dysfunction, increased production of
ox-LDL, decreased adiponectin, decreased nitric oxide (NO) production, gut
microbiota, non-coding RNA, vascular calcification, oxidative stress,
inflammatory response, and endothelial dysfunction [9, 34, 46, 47, 48, 49, 50]. The
cross-talk between atherosclerosis and diabetes has been established using novel
therapeutics in diabetic atherosclerosis (Fig. 2). High glucose (HG) promotes the
expression levels of proinflammatory factors, AGEs formation, ROS generation,
fatty acid oxidation, and free fatty acid production in endothelial cells, which
are important signs of atherosclerotic endothelial damage [8]. In addition, AGEs
interact with their receptors to induce the proliferation and migration of VSMCs,
core events in initiation and progression of atheroma [51]. Furthermore, diabetes
enhances atherosclerosis progression by regulating various molecules, such as
protein kinase-
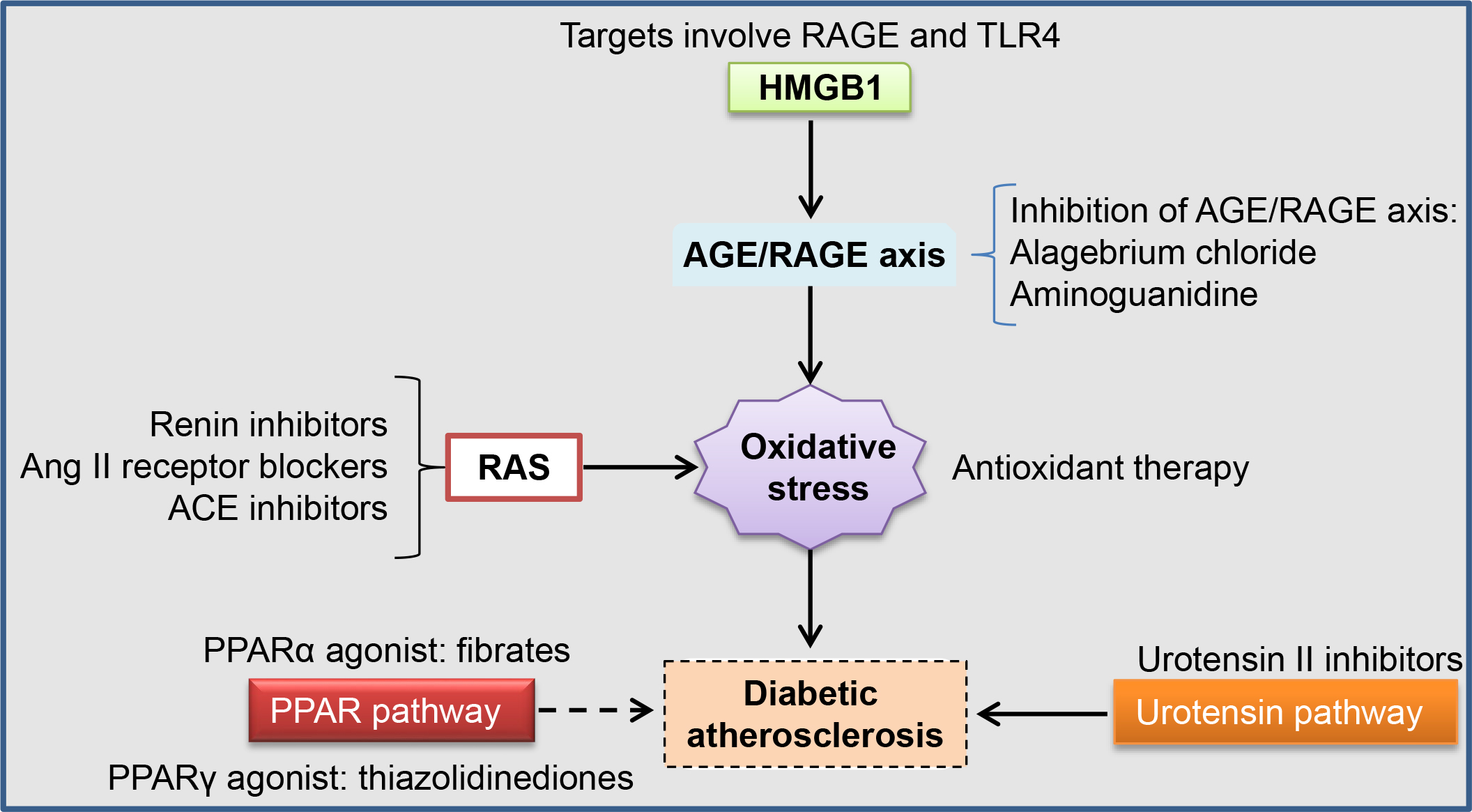 Fig. 2.
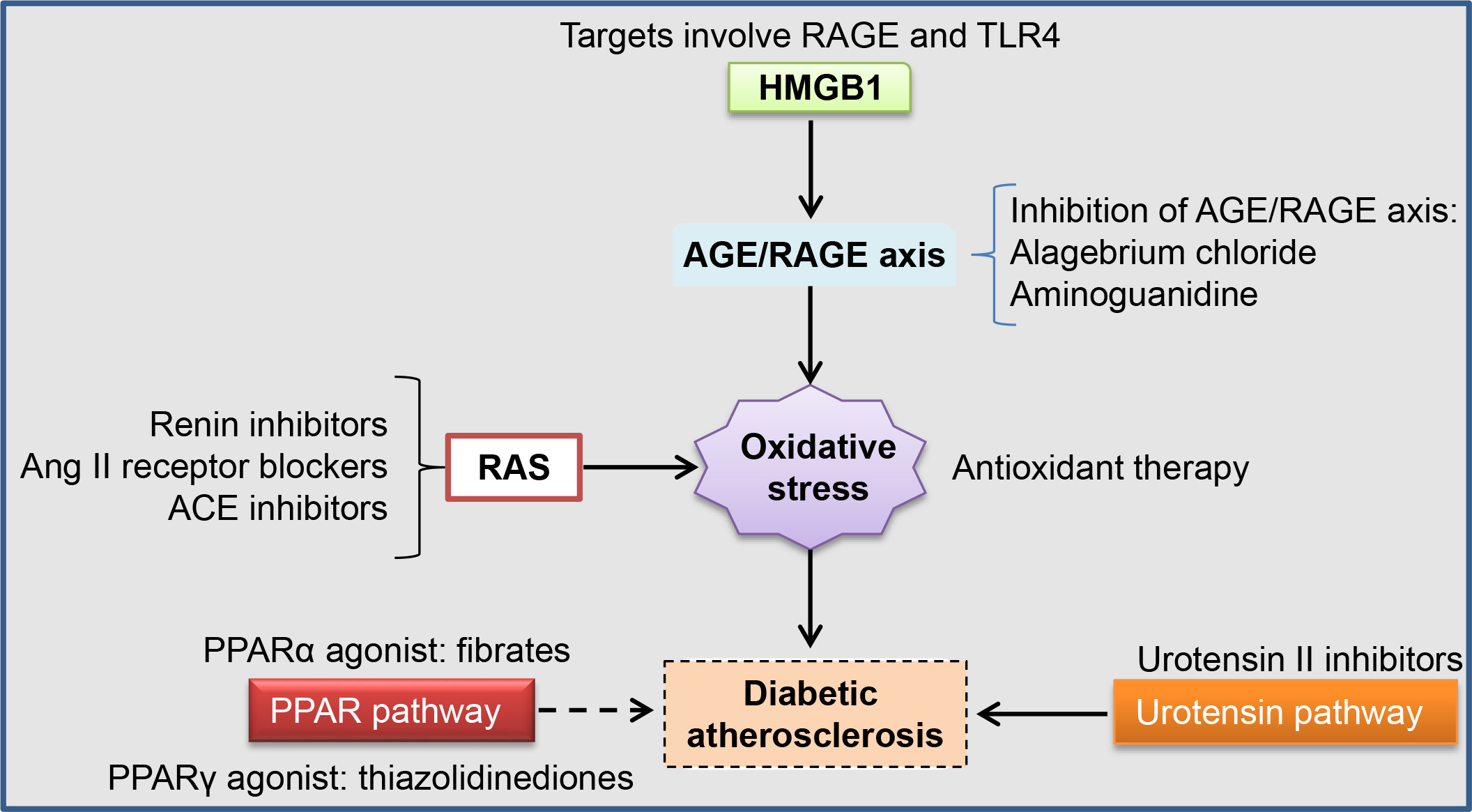
Fig. 2.Current therapeutics in diabetes-associated atherosclerosis. Interplay of several pathways, such as the AGE/RAGE axis, urotensin II, RAS, and PPAR, is involved in diabetes-associated atherosclerosis pathogenesis. The current therapeutic approaches specifically target these pathways, thus, providing promising treatment options for diabetic atherosclerosis. ACE, angiotensin-converting enzyme; AGE/RAGE, advanced glycation end product/receptor for advanced glycation end product; RAS, renin–angiotensin system; TLR4, Toll-like receptor 4.
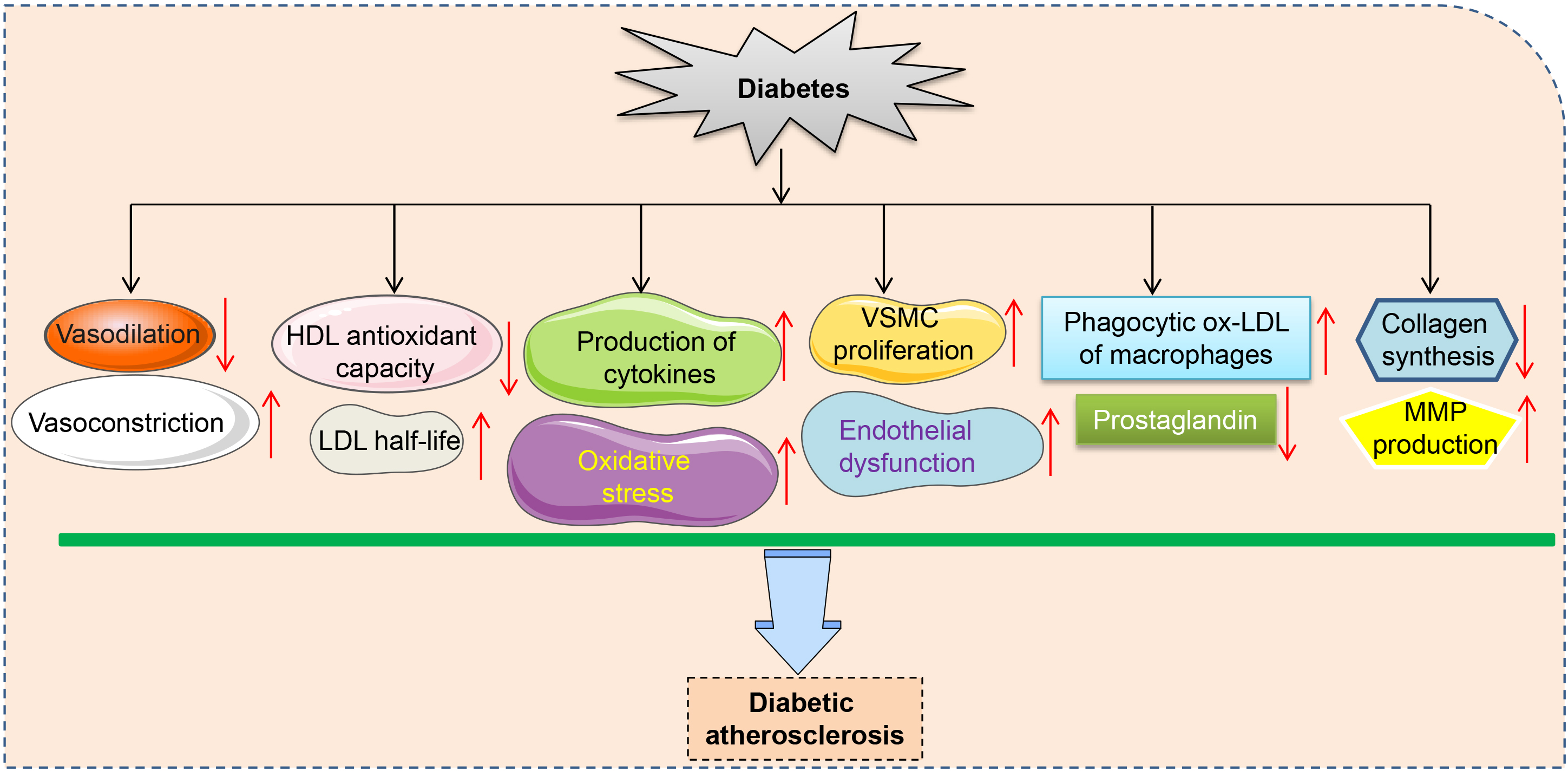 Fig. 3.
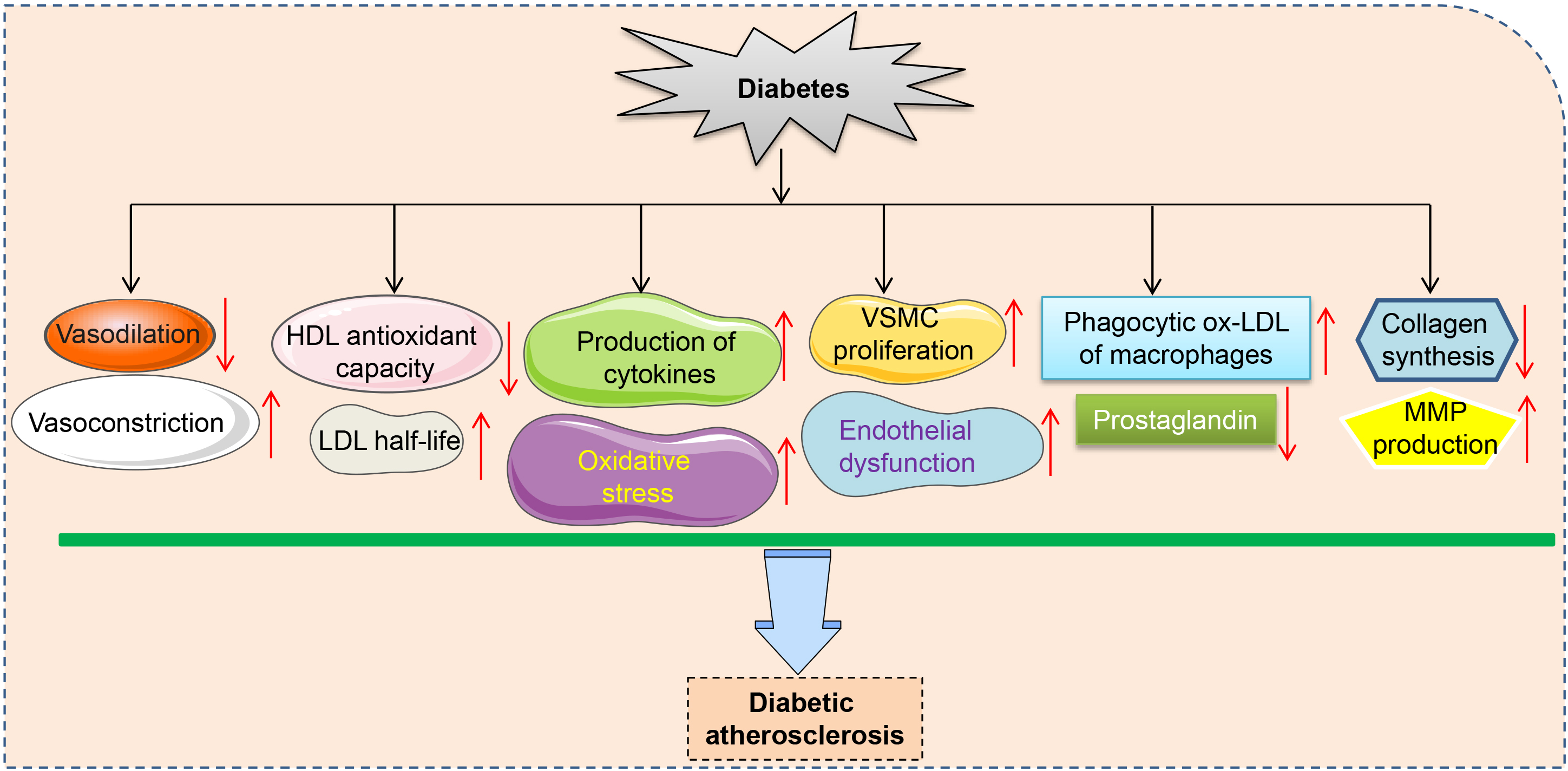
Fig. 3.Schematic presentation of the role of diabetes in atherosclerosis. A chronic hyperglycemia state promotes endothelial-independent vasoconstriction, the half of LDL, cytokine secretion, oxidative stress, VSMC proliferation, endothelial dysfunction, foam cell formation, MMP production, and inhibits endothelial–dependent vasodilation, HDL antioxidant capacity, and collagen synthesis, leading to atherosclerosis development. LDL, low density lipoprotein; VSMCs, vascular smooth muscle cells; MMP, matrix metalloprotein; HDL, high density lipoprotein.
Curcumin, a yellow bioactive constituent isolated from Turmeric (Curcuma longa), is used as a diet supplement to prevent or treat diabetes-associated complications [64]. Due to its antioxidant and anti-inflammatory properties, curcumin inhibits the development of atherosclerosis and hyperlipidemia [65, 66, 67]. Moreover, curcumin reduces diabetes-associated cardiovascular risk [67]. A limited number of clinical trials have determined the therapeutic effects of curcumin in diabetes and atherosclerosis patients. A randomized placebo-controlled trial revealed that curcumin treatment for 12 weeks reduces the risk of cardiovascular events in type 2 diabetes and dyslipidemia patients [68]. In healthy people, daily oral administration of curcumin significantly suppressed low-density lipoprotein and apolipoprotein B levels, but increased high-density lipoprotein and apolipoprotein A levels, indicating its anti-atherosclerosis efficacy [69]. Curcumin treatment for 6 months lowers atherogenic risks in type 2 diabetes patients, as evidenced by reduced pulse wave velocity, leptin levels and increased serum adiponectin levels [70]. Therefore, this extract might be helpful for improving metabolic profiles in diabetes patients with atherosclerosis. Large-scale clinical trials should be performed to characterize the actual potential and molecular mechanisms of curcumin for treating diabetic atherosclerosis.
Although curcumin has various pharmacological effects in cardiovascular and
metabolic disorders, its clinical applications are limited by its poor water
solubility, rapid metabolism, and low bioavailability [71]. Curcumin derivatives
and/or analogs, such as L3 (1, 7-bis (3, 5-di-tert-butyl-4-hydroxyphenyl)-1,
6-heptadiene-3, 5-dione) have been developed to improve the biological activities
of curcumin [72]. L3 treatment ameliorated dyslipidemia as well as hyperglycemia
and reduced oxidative stress in aortic arch, thereby mitigating atherosclerotic
degeneration in diabetic mice [73]. These findings imply that L3 can alleviate
diabetic atherosclerosis progression, which provides a scientific basis for
clinical applications of L3. Moreover, by suppressing plasma lipopolysaccharide
(LPS) levels, improving intestinal barrier functions, and inhibiting macrophage
activation, oral curcumin attenuated high fat diet (HFD)-induced glucose
intolerance and atherosclerosis in LDL receptor knockout (LDLR
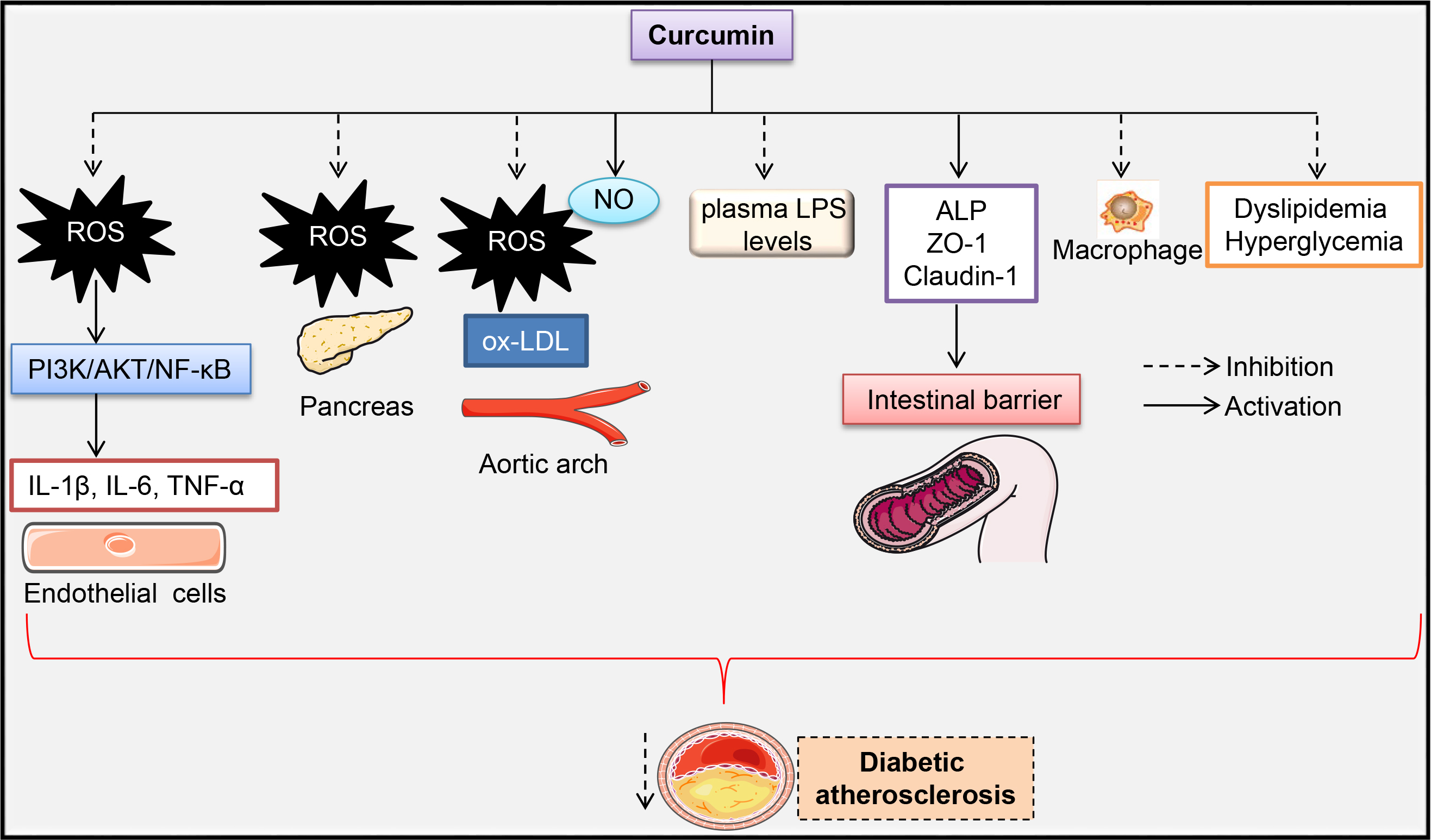 Fig. 4.
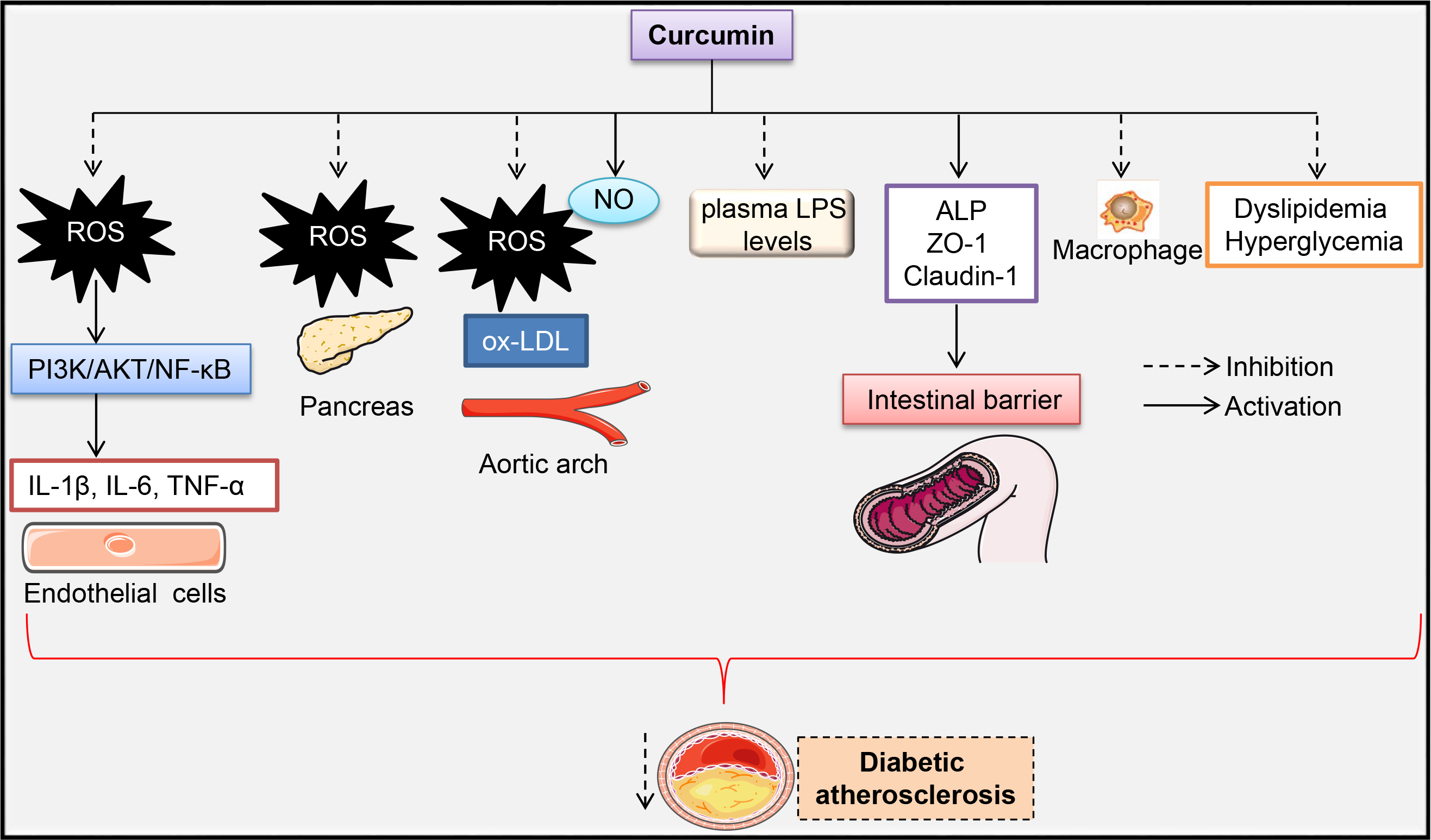
Fig. 4.Signaling pathway by which curcumin alleviates
atherosclerosis progression in diabetes. Anti-inflammatory effects of curcumin
in rat thoracic aorta endothelial cells were associated with inhibition of the
ROS/PI3K/AKT/NF-
As a protoberberine alkaloid, berberine is abundantly present in several medicinal plants that have a wide spectrum of pharmacological activities, including anti-diabetic and anti-atherosclerotic effects [76, 77]. Glucose- and cholesterol-lowering effects of berberine have been reported. Berberine has been reported to reduce fasting blood glucose levels, glucose intolerance, and hyperlipidemia in type 1 and type 2 diabetes [78, 79]. Berberine enhancement of glucose utilization in adipocytes and myocytes, and suppression of glucose absorption in intestinal cells results in a net hypoglycemic effect [80]. Activation of AMPK is also involved in beneficial metabolic effects of berberine, which reduces lipid accumulation in the adipocytes and increases glucose uptake in the myotubes [81]. Thus, berberine has antidiabetic properties.
In addition, cholesterol-lowering activities, anti-inflammatory as well as
anti-oxidant properties, inhibition of VSMC proliferation, and improvement of
endothelial dysfunction by berberine synergistically contribute to its
atheroprotective effects [79]. Treatment with berberine for 30 days induced a
slightly greater reduction in low-density lipoprotein cholesterol and
inflammatory factors in patients with acute coronary syndrome (ACS), following
percutaneous coronary intervention when compared to standard therapy alone [82].
In a recent study, berberine treatment reduced aortic ROS production and
suppressed serum malondialdehyde (MDA) levels in an ApoE
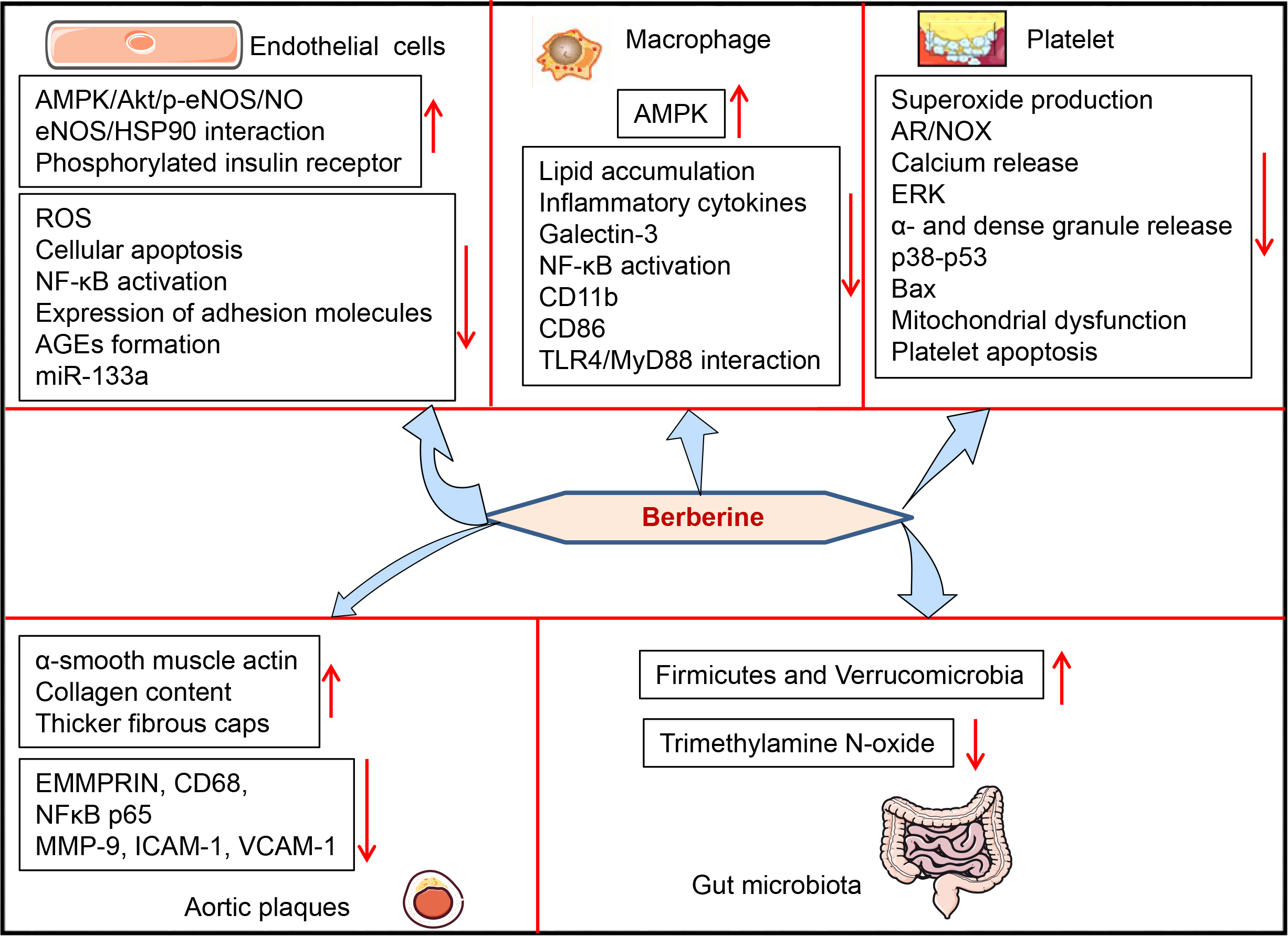 Fig. 5.
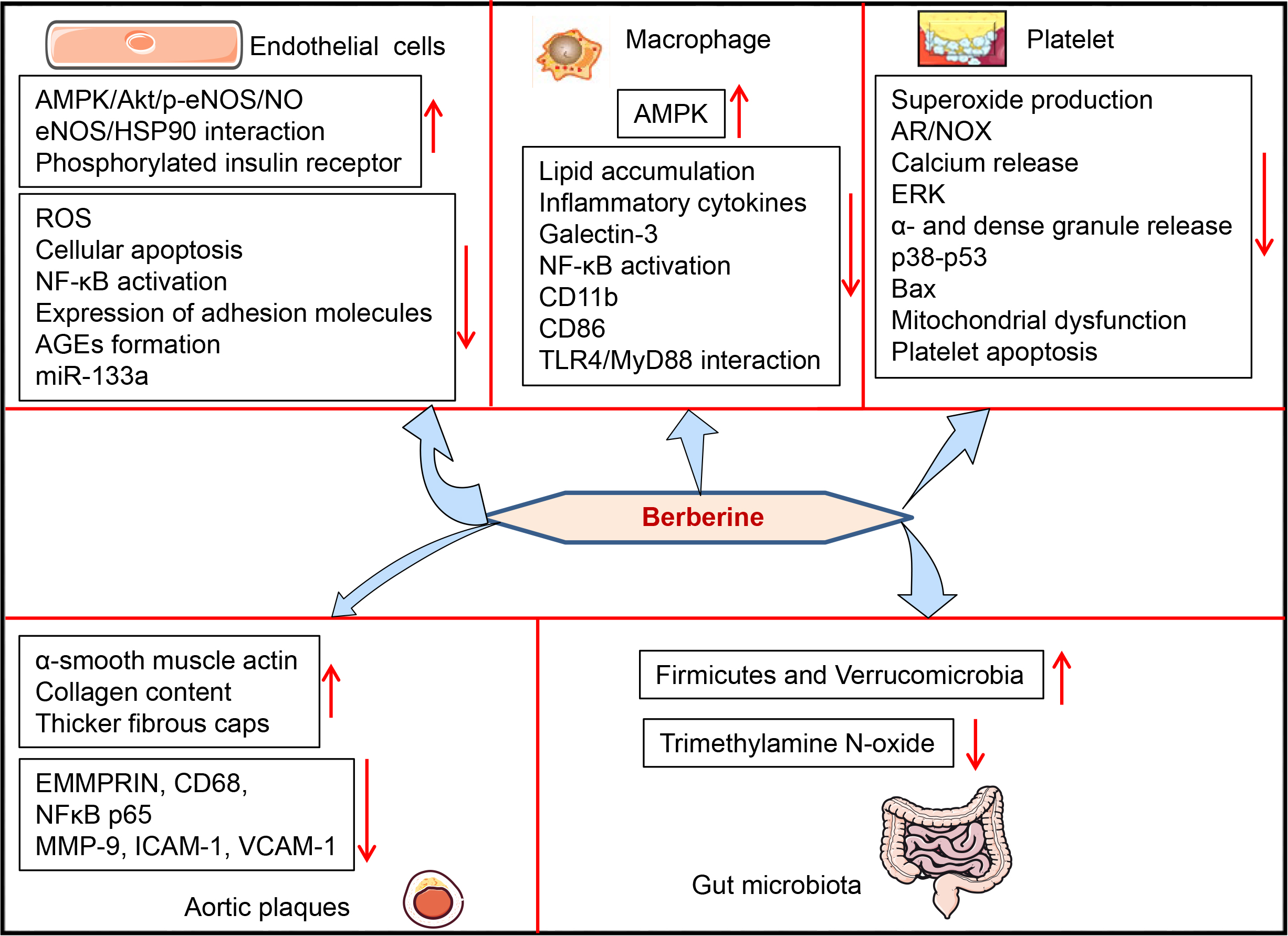
Fig. 5.Atheroprotective effects and mechanisms of berberine in
diabetes. Berberine attenuates diabetic atherosclerosis by regulating the
functions of vascular endothelial cells, VSMCs, macrophages, platelets, and gut
microbiota. Berberine protects against HG-induced apoptosis, ROS production, and
inflammation in endothelial cells by upregulating phosphorylation of the insulin
receptor and downstream AMPK/Akt/eNOS/NO signaling, promoting the association
between eNOS with HSP90, inhibiting AGEs formation, miR-133a and NF-
Resveratrol, a natural phytoalexin in enriched plants, foods and beverages, exerts a broad spectrum of biological and pharmacological actions by regulating various targets and signaling pathways [87]. Resveratrol has anti-atherosclerosis, anti-diabetic, anti-aging, anti-obesity, and anti-cancer effects [88]. Cardiovascular protective effects of resveratrol may be attributed to its anti-inflammatory, anti-oxidative, anti-platelet, insulin-sensitizing, and lipid-lowering effects [89]. Moreover, activation of silent information regulator 1 (SIRT1), AMPK, and endogenous anti-oxidant enzymes contributes to its beneficial cardiovascular effects [89].
Resveratrol treatment counteracts pro-atherosclerotic effects of HG on
endothelial cells by inhibiting the mRNA expressions of endothelin-1 and
E-selectin, and stimulating endothelial nitric oxide synthase (eNOS)/NO
signaling. These effects occur in a SIRT1-dependent manner since gene deletion of
SIRT1 ameliorates the effects of resveratrol [90]. Endothelial hyperpermeability
is the initial step in diabetic atherosclerosis development, therefore,
amelioration of endothelial hyperpermeability might exert protective effects
against diabetic atherosclerotic complications [18, 91]. Increased permeability
and caveolin-1 expression in monolayer endothelial cells exposed to HG can be
prevented by resveratrol [92]. Blockade of vascular endothelial growth factor
(VEGF) and kinase insert domain receptor (KDR) signaling pathway is involved in
resveratrol-mediated alleviation of HG-induced hyperpermeability and caveolin-1
overexpression [92]. Resveratrol inhibits the proliferation and migration of
VSMCs exposed to HG by inactivating NF-
Salidroside is an important phenylpropane glycoside in medicinal plants of the
genus Rhodiola. It is associated with remarkable curative effects and few side
effects on metabolic, cardiovascular, and neurological diseases [99]. Salidroside
has favorable biological as well as pharmacological activities, including
amelioration of glucose intolerance, insulin insensitivity,
Atherosclerosis initiation and pathogenesis are closely associated with
ox-LDL-induced endothelial damage. Exposure of human umbilical vein endothelial
cells (HUVECs) to ox-LDL dose dependently reduced cell viability and SOD
activity, increased lactate dehydrogenase (LDH) release and cellular oxidative
stress. These effects were antagonized by pretreatment with salidroside [107].
Under ox-LDL stimulation, salidroside stimulates the SIRT1-FOXO1 pathway to
inhibit oxidative stress and to enhance autophagy in HUVECs [107]. Activation of
AMPK/SIRT1 signaling by salidroside is also involved in amelioration of ox-LDL-induced oxidative stress and mitochondrial dysfunction in HUVECs [107]. ox-LDL promotes macrophage-derived foam cell formation and apoptosis, while
salidroside co-treatment inhibits it, partly by regulating MAPK and Akt signaling
pathways [108]. Upregulation of peroxisome proliferator-activated receptor
gamma-coactivator-1
Ginkgo biloba is known as the Maidenhair tree, and its leaf extracts are used to
treat various pathologies [111]. Extracts from this plant have various
cardiovascular protection functions, which are largely attributed to their free
radical scavenging abilities, anti-inflammatory properties, and anti-platelet
activation abilities [112]. Ginkgo biloba extracts are promising therapeutic
agents for cardiovascular and metabolic diseases [113]. Ginkgo biloba leaf
extracts are mainly composed of terpenoids, flavonoids, alkylphenols, polyprenols
and organic acids, which have been shown to have the potential for treatment of
metabolic syndromes associated with increased risks of cardiovascular disease
events [114]. Terpenoids (bilobalide and ginkgolides A, B, and C) and flavone
glycosides (isorhamnetin, quercetin, and kaempferol) are the two major compounds
in Ginkgo biloba leaves. The special Ginkgo biloba leaf extract, EGB761, has been
reported to maintain glucose homeostasis by protecting pancreatic
In addition, Ginkgo biloba extracts increased resistance of endothelial progenitor cells to oxidative stress in diabetic patients by dose dependently improving SOD activities and reducing the apoptotic rate of endothelial progenitor cells within the peripheral blood of diabetic patients [122]. Zhao et al. [123] confirmed that EGB761 pretreatment reduces HG-induced monocyte adhesion and ROS production in human aortic endothelial cells by inducing HO-1 expressions through Akt/eNOS and p38/MAPK pathways. Cui et al. [124] showed that pretreatment with Ginkgolide A significantly inhibited the overproduction of IL-4, IL-6, and IL-13 in HG-incubated endothelial cells, this may be attributed to regulation of signal transducer and activator of transcription 3 (STAT3) phosphorylation. Ginkgo biloba extract-derived rutin dose-dependently reduced ROS generation and NLRP3 inflammasome activation in human umbilical vein endothelial cells under HG conditions [125]. Rutin administration restored acetylcholine-induced endothelial diastolic dysfunction in thoracic aortic tissues of high glucose diet-fed rats [125]. Given that hyperglycemia-induced low-grade inflammation and oxidative burst in endothelial cells are key events in the onset and progression of diabetic atherosclerosis, Ginkgo biloba extracts might be promising candidates for attenuating diabetes-associated atherosclerosis by targeting endothelial dysfunction. Despite favorable effects of Ginkgo biloba extracts on diabetic atherosclerosis, studies, especially clinical trials, should aim at evaluating the safety and efficacy of Ginkgo biloba extracts.
Salvia miltiorrhiza (Danshen), a traditional Chinese herbal medicine, modulates multiple targets to treat cardiometabolic diseases, including diabetes and atherosclerosis [126]. In the last several decades, studies have aimed at delineating the putative cardiovascular protective effects of this phytochemical through modern scientific research [127]. Salvianolic acid and tanshinones are the predominant bioactive compounds in Salvia miltiorrhiza, and both of them were shown to treat atherosclerosis-related cardiovascular and metabolic diseases by targeting multiple signaling pathways [126], such as inhibition of oxidative damage and inflammatory responses, suppression of leukocyte adhesion as well as modulation of endothelial NO production [128, 129].
As the most abundant water-soluble compound in the root of Salvia miltiorrhiza,
Salvianolic acid B treatment increased NO production, decreased ROS formation,
and suppressed endothelial cell apoptosis in isolated mouse aortas, thereby
improving endothelial function in diabetic rats with fluctuating blood glucose
levels [128, 130]. Salvianolic acid B prevented platelet-derived growth factor
(PDGF)-induced proliferation of VSMCs and neointimal hyperplasia in arteries,
effects that were Nrf2-dependent [131]. Antiatherogenic effects of Salvianolic
acid B are associated with NF-
Celastrol is a triterpenoid derived from various traditional Chinese medicinal plants, such as Tripterygium wilfordii (Thunder God Vine), Celastrus orbiculatus, Celastrus aculeatus Celastrus reglii, and Celastrus scandens [135]. As an active ingredient in plants, celastrol has great potential for treatment of various chronic inflammatory disorders, including rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), and allergies [136]. Studies have reported on the medicinal value of celastrol in diabetes, obesity, and atherosclerosis [137]. By modulating intricate cellular pathways and networks associated with disease pathology, celastrol is effective in treating various metabolic diseases and complications [19].
Celastrol administration for 2 months significantly lowered fasting plasma glucose, glycated haemoglobin (HbA1C) and homeostasis model assessment index (HOMA-IR) levels in type 2 diabetic animal models. Moreover, it improved abnormal lipid metabolism, oxidative stress and proinflammatory cytokine activities in the kidney, liver as well as adipose tissues [138]. In mitochondrial dysfunction and insulin resistance models of human skeletal muscle cells, celastrol augments insulin-stimulated glucose uptake activities by activating the PI3K/Akt pathway and enhancing mitochondrial activities [139]. Chronic low-grade inflammation is involved in the development of insulin resistance in adipose tissues, a noticeable feature in diabetes. Inhibition of pro-inflammatory cytokines in adipose tissues is an effective strategy for ameliorating insulin resistance in diabetes. In mitochondrial dysfunction-induced insulin resistance in 3T3-L1 adipocytes, celastrol improved metabolic functions with reductions in ROS production and inflammatory factors [140]. These findings imply that by targeting multiple organs or tissues, celastrol may be a therapeutic option for diabetes.
Ji et al. [141] reported that celastrol reduced atherosclerotic plaque
sizes in ApoE
Catalpol, one of the active components in the roots of Rehmannia glutinosa, has
been found to protect against osteoporosis, neurodegenerative diseases, and
diabetic complications [143]. Catalpol decreased plasma glucose levels in
streptozocin (STZ)-induced diabetic rats, which was attributed to increased
glucose utilization in the liver and skeletal muscles [144]. Inhibitory effects
of catalpol on blood glucose levels were reversed by blockade of opioid
Paeonol is the main active compound isolated from Cortex Moutan (Paeonia
suffruticosa Andrews, Ranunculaceae). It has various beneficial effects, such as
anti-atherosclerotic and anti-apoptosis effects [146]. Chen et al. [147]
evaluated the effects of paeonol on vascular smooth muscle cell (VSMC)
proliferation or vascular endothelial cell injury under HG conditions. They found
that paeonol inhibited the secretion of VEGF and platelet derivative growth
factor B (PDGF-B) from endothelial cells, a critical event for suppression of
VSMC proliferation in the co-culture model. Moreover, conditioned medium from
paeonol-treated endothelial cells inhibited protein overexpression of Ras, P-Raf,
and P-ERK in VSMCs, suggesting that paeonol exerts anti-atherosclerosis
activities by regulating the communication between VSMCs and endothelial cells.
Paeonol exerted inhibitory effects on apoptosis, oxidative stress, and
inflammatory responses in HUVECs exposed to HG and palmitic acid, and these
effects were dependent on SIRT1/FOXO3a/NF-
Fisetin (3,3
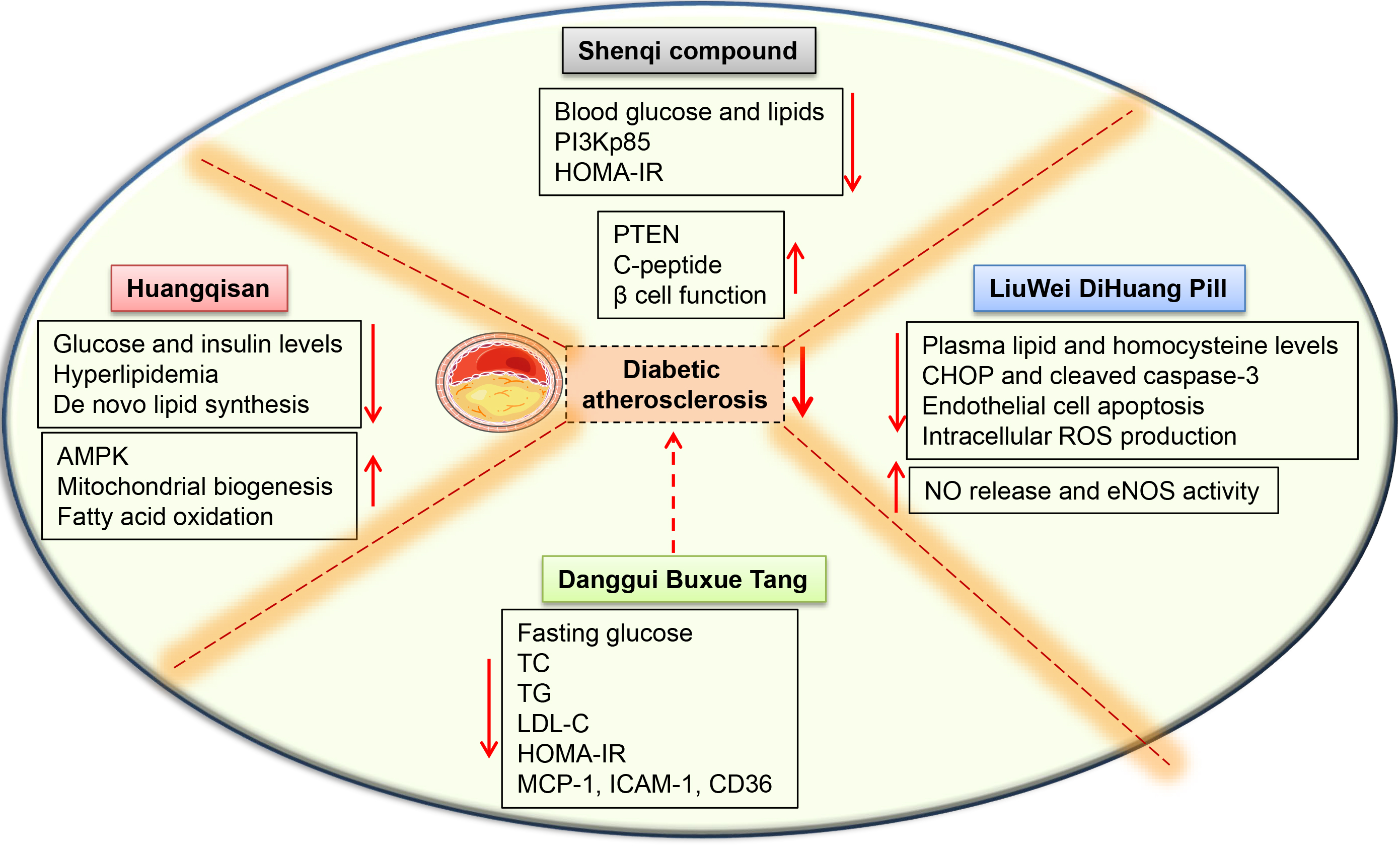
Generally, TCM is used as a water decoction with a specific combination of different herbs (also known as formulas), which are prepared in a unique way [152]. Treatment of human diseases requires a comprehensive strategy involving appropriate TCM formulas [23]. Particularly, three classical TCM formulas (Qingfeipaidu Decoction, Huashibaidu Decoction and Xuanfeibaidu Decoction) have been shown to be effective in treatment of coronavirus disease 2019 (COVID-19) [153]. Accordingly, several TCM formulas are associated with remission of cardiovascular disease-related complications [154]. We reviewed various TCM formulas with potential beneficial effects in diabetic atherosclerosis therapy (Fig. 6).
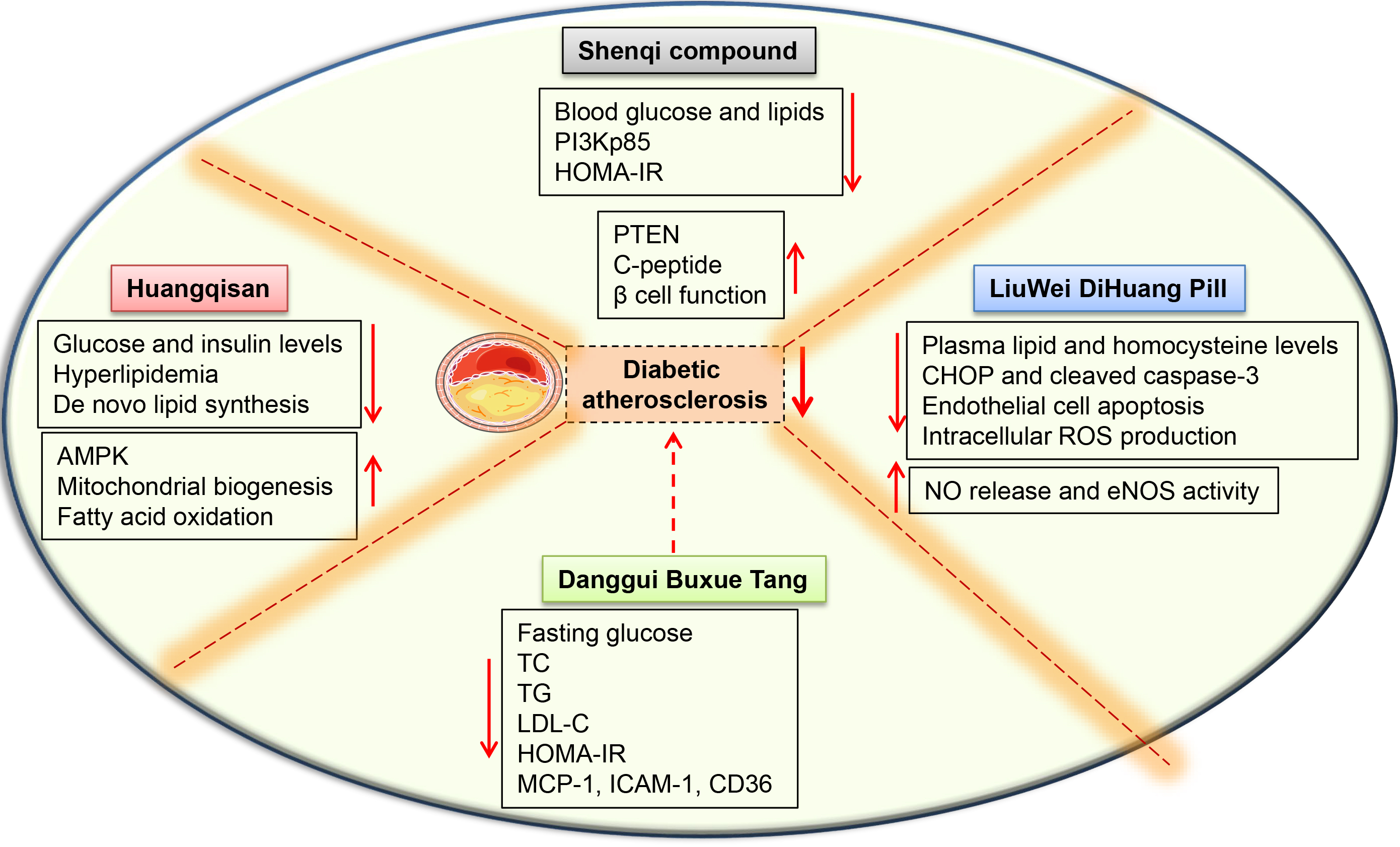 Fig. 6.
Fig. 6.Schematic presentation of the mechanisms of TCM
formulas in diabetes-associated atherosclerosis. LiuWei DiHuang Pill decreased
plasma lipid and homocysteine levels in mice models of diabetic atherosclerosis,
inhibited homocysteine-induced ROS production, CHOP and cleaved caspase-3
expressions in endothelial cells, and upregulated NO release as well as eNOS
activities in HUVECs. Huangqisan normalized glucose and insulin levels,
de novo lipid synthesis, and improved glucose tolerance in obese rats.
Huangqisan is also effective in reversing metabolic disorders by promoting AMPK
signaling, mitochondrial biogenesis, and fatty acid oxidation. Danggui Buxue Tang
significantly suppressed serum levels of TG, LDL-C and diminished the expressions
of lipogenic genes in the aorta of diabetic mice. Shenqi compound ameliorates
HOMA-IR, gluco-lipid metabolism, and aortic morphology by elevating PTEN mRNA
expressions while suppressing PI3Kp85 mRNA expression in aorta. In addition,
Shenqi compound protects islet
Shenqi compound is composed of eight Chinese herbs, including yam, salvia,
trichosanthin, dogwood, ginseng, astragalus, wine rhubarb, and Raw radix
rehmanniae [155, 156]. Shenqi compound ameliorated gluco-lipid metabolism and
aortic morphology in diabetic Goto-Kakizaki (GK) rats, which was attributed to
increased PTEN mRNA expressions and suppressed PI3Kp85 mRNA expressions in the
aorta [157]. Compared to rosiglitazone, shenqi compound was shown to exert better
curative effects in the treatment of diabetic vasculopathy [158]. Liu et
al. [155] reported that Shenqi compound treatment improved polydipsia,
polyphagia, weight loss, and vascular injury in a spontaneous diabetic rat model.
Gene microarray experiments have shown that the Shenqi compound is an effective
therapeutic option for diabetes. It regulates the biological functions involved
in sensory perceptions of smell, G-protein coupled receptor signaling pathway,
and cytoplasmic translation [155]. A systematic review and meta-analysis reported
that Shenqi compound regulates intestinal flora metabolites in type 2 diabetes
[159], a critical event involved in diabetic atherosclerosis pathogenesis [160].
A randomized controlled multicenter trial has proven that the Shenqi compound
improves lower extremity atherosclerosis of type 2 diabetic patients by
protecting islet
Among the complex TCM formulations, Danggui Buxue Tang (DBT) is the simplest one, and it has been clinically used in China for over 800 years [162]. The herbal formula contains two herbs: 10 qian Astragali Radix (AR; roots of Astragalus membranaceus (Fisch.) Bunge or Astragalus membranaceus (Fisch.) Bunge var. mongholicus (Bunge) P.K. Hsiao, Huangqi in Chinese) and 2 qian Angelicae Sinensis Radix (ASR; roots of Angelica sinensis (Oliv.) Diels, Danggui in Chinese) (qian is a weight unit in ancient China, where 1 qian is equivalent to ~3 g) [162]. The TCM Danggui Buxue decotion inhibits inflammatory damage in renal tissues by regulating nuclear factor (NF)-kappaB signaling pathway [163]. This decoction is a commonly used prescription for the treatment of migraines, menopausal symptoms, cardiac injury, iron-deficient anemia, and diabetic nephropathy [162, 164, 165, 166, 167, 168]. Evidence for the protective effects of Danggui Buxue decotion against diabetic atherosclerosis have been documented by Huang et al. [169], who found that administration of the Danggui buxue decoction reduced homeostasis assessment of insulin resistance (HOMA-IR) and serum levels of triglyceride (TG), cholesterol (CHOL), as well as low-density lipoprotein-cholesterol (LDL-C) in Goto-Kakizaki (GK) rats. Danggui buxue decoction-associated lipid metabolism regulation is beneficial for delaying atherosclerosis development in diabetic GK rats, with the mechanism likely to be involving lipid metabolic gene regulation in aorta vessels [169]. Furthermore, oral administration of Danggui buxue decoction decreased blood levels of total cholesterol (TC), triglyceride (TG), low-density lipoprotein cholesterol (LDL-C), and inhibited mRNA expressions of monocyte chemoattractant protein (MCP)-1, intercellular adhesion molecule (ICAM)-1 and CD36 in aorta tissues from diabetic GK rats, suggesting that the Danggui buxue decoction is a potential therapeutic option for the early stages of diabetes-associated atherosclerosis [170]. Ferulic acid, formononetin, calycosin, astragaloside, caffeic acid, ligustilide, and butyphthalide, which are bioactive metabolites in Danggui buxue decoction, contribute to the protective effects of Danggui buxue decoction against diabetes-associated atherosclerosis [169]. These results show the value of this formula in the treatment of diabetic atherosclerosis. However, clinical trials for Danggui buxue decoction have not been performed. Therefore, well-designed clinical trials, in-depth mechanistic studies, investigations on side effects of Danggui buxue decoction and drug interactions should be the focus of future studies.
Huangqisan is a traditional herbal formula that is derived from Sheng Ji Zong Lu (written in the Song Dynasty of China). This representative formula is composed of Astragali Radix, Pueraria Radix, and Cortex Mori Radicis. These three individual herbs have been traditionally used for the treatment of various diseases for thousands of years [171]. Astragali Radix, Pueraria Radix, and Cortex Mori Radicis have anti-diabetic activities [172, 173, 174, 175]. Moreover, Astragali Radix has anti-oxidant, and immunological activities [176]. Astragali Radix was shown to decrease fasting blood glucose levels in diabetic animal models [177]. Puerarin, one of the major constituents of Astragali Radix, may be beneficial in controlling blood glucose levels in type 2 diabetes patients [178]. In addition, other ingredients of Huangqisan, such as Astragaloside IV, Sanggenon D, and 1-de-oxynojirimycin, have glucose-lowering effects [179, 180], indicating that Huangqisan might be a potential formula for treatment of diabetes and its complications.
Huangqisan treatment decreased plasma TC, TG, FFA and FABP4 levels, normalized
glucose and insulin levels, and improved glucose tolerance in HFD-fed rats [181].
RNA-Seq analysis combined with qPCR revealed that this formula triggers
beneficial effects on glucose-lipid metabolism by regulating mRNA expressions of
some important glucose and lipid metabolism-associated genes, such as Acat2,
Apoc4, Bhmt, Cyp3a62, Cyp51, Egln3 (Phd3), Fads1, Fads2, Gnmt, Hmgcs1 and Pemt
[181]. Huangqisan ameliorates metabolic disorders and maintains glucose
homeostasis in hyperlipidemia rats by augmenting mitochondrial biogenesis and
fatty acid oxidation to increase thermogenesis and energy expenditure. Therefore,
Huangqisan is a stimulator for converting white adipocytes into brown-like
adipocytes [182]. Huangqisan administration lowered body weight, fasting blood
glucose, and serum lipid levels while improving glucose tolerance and insulin
sensitivity in HFD-induced obese mice and db/db mice. Moreover, this prescription
blocked the formation of atherosclerotic plaques in LDLR
LiuWei DiHuang Pill was first mentioned by Qian Yi in the Song Dynasty (AD
1119). It was described as a traditional prescription for the treatment of
various diseases, including invigoration of yin, particularly kidney yin [184].
Liuwei Dihuang Pills are comprised of Rehmanniae radix praeparata, Corni fructus,
Dioscoreae rhizoma, Alismatis rhizoma, Moutan cortex, and Poria at a ratio of
8:4:4:3:3:3. These herbs play dominant roles in suppression of inflammation and
oxidative stress in various cardiovascular disorders [185, 186, 187, 188]. Liuwei Dihuang
Pills are a safe and effective formula for the prevention and treatment of
diabetes and its complications, such as diabetic encephalopathy, diabetic muscle
atrophy, and diabetic nephropathy [189, 190, 191, 192]. Treatment with Liuwei Dihuang Pills
decreased fasting blood glucose levels and attenuated neural apoptosis,
overexpression of caspase-3 as well as A
A combination of Ginkgo Leaf Tablets with Liuwei Dihuang Pills downregulated plasma levels of carboxymethyl lysine (CML) and 8-isoprostane(8-IsoP) in type 2 diabetes, although macrovascular event occurrence and carotid intima-media thickness were not altered [195]. Zhao et al. [194] reported that co-treatment with Ginkgo Leaf Tablets and Liuwei Dihuang Pills remarkably downregulated urinary microalbumin to urinary creatinine ratio (Umalb/cr) levels and diabetic nephropathy prevalence in 140 outpatients with type 2 diabetes. However, the co-treatment had no effect on carotid intima-media thickness levels and incidence of cardiovascular as well as cerebrovascular events, suggesting that these two proprietary herbal medicines are beneficial in diabetic microvascular complications. The efficacy of Liuwei Dihuang Pills as a therapeutic option for diabetic macrovascular complications, such as atherosclerosis, should be evaluated further. Jing et al. [196] evaluated the direct effects of Liuwei Dihuang Pills on atherosclerotic lesion development in the aortic root of ovariectomized ApoE-deficient mice. They found that by reducing plasma lipid and homocysteine levels, as well as inhibiting endothelial cell apoptosis and inflammatory responses, Liuwei Dihuang Pills prevented plaque formation in animal models of menopausal atherosclerosis. Therefore, Liuwei Dihuang Pills can potentially be used to halt atherosclerosis-associated vascular diseases in menopausal women. Although Liuwei Dihuang Pills are promising as therapeutic options for diabetes and atherosclerosis, they are associated with several limitations. First, in vitro and in vivo studies should aim at confirming the preventive and therapeutic values of Liuwei Dihuang Pills in diabetic atherosclerosis. Second, scientific and technologic approaches should be used to elucidate on the efficacy of this formula and its combinations with other prescriptions in treating diabetes. Finally, mechanistic studies and long-term clinical trials, as well as studies evaluating the safety of this selected formula are required to inform its future applications in the treatment of diabetes-associated atherosclerosis.
Nutrition therapy is an important supplementary strategy to treat diabetes and atherosclerosis, and dietary berries have received increasing attention because of its roles in the management of diabetes and its associated complications [197]. Dietary berries contain plentiful fiber and polyphenols, a small amount of carbohydrates and fats, certain essential micronutrients, including vitamin C, E potassium, manganese, and folic acid, contributing its health benefits in people with diabetes [198]. Several epidemiological studies have revealed that the bioactive compounds from berries could effectively reduce inflammation, oxidative stress, diabetes, and cardiovascular diseases [199, 200, 201]. It has been reviewed that supplementation of blueberries, cranberries, strawberries and raspberries might hold beneficial effects in diabetes through augmenting antioxidant abilities, decreasing biomarkers of atherosclerosis, and ameliorating glycemic and lipid profiles [201]. For example, administration of black raspberry extracts for 12 weeks decreased postprandial glucose and surrogate markers of atherosclerosis in adults with pre-diabetes [202]. Strawberries have been reported to improve atherosclerotic risk factors in subjects with metabolic syndrome, such as dyslipidemia and circulating adhesion molecules [203]. A randomized double-blind controlled trial has shown that consumption of freeze-dried strawberry significantly decreases C-reactive protein levels and lipid peroxidation in patients with type 2 diabetes, but does not affect serum glucose concentrations and anthropometric indices [204]. AMPK, a serine/threonine protein kinase, plays a central role in the regulation of cellular metabolism in cells, and this kinase is becoming a potential therapeutic target for the treatment of several chronic diseases, including obesity, diabetes, and cardiovascular diseases [205, 206]. Naturally occurring compounds are beneficial to the human body by acting on the AMPK signaling pathway. Coincidentally, Battino’s group has disclosed that a methanolic strawberry extract attenuates lipid accumulation in HepG2 cells by AMPK activation [207]. Later, the same group further found that strawberry supplementation increased antioxidant enzyme activities, mitochondrial biomass, and decreased intracellular oxidative stress in in old rats, an effect that is AMPK dependent [208]. These exciting results collectively confirm the involvement of AMPK in the beneficial effects exerted by strawberry against lipid deposition and aging progression. Likewise, it is possible that AMPK activation by strawberry might be used to prevent or delay diabetic atherosclerosis, which needs to be ascertained in the future studies.
As a natural dietary source of (poly)phenols, Red raspberry (Rubus idaeus) consumption ameliorates the impaired vasoconstriction and vasorelaxation response in the obese Zucker rat, a model of metabolic syndrome, suggesting that dietary intervention of Red raspberry prevents and/or reverses diabetes-induced vascular complications [209]. In consistence with this, Song et al. [210] have found that Red raspberry treatment decreases body weight gain, steatosis grade scores and insulin resistance in HFD-induced obese mice. The protection of Red raspberry against diet-induced obesity and related metabolic disorders may be mediated by a set of genes involved in lipid metabolism and fibroblast growth factor 21 signaling pathway [210]. Physico-chemical characterization and metabolomic analysis showed that cyanidin 3-O-glucoside and cyanidin 3-O-sambubioside are the main anthocyanins of Andean elderberry, and these bioactive compounds exhibit antioxidant, antihypertensive, antiobesity and antidiabetic properties [211]. Consumption of a tropical highland blackberry beverage is found to mitigate plasma levels of triglycerides, total cholesterol, and glucose levels in healthy individuals on a high-fat, high-carbohydrate diet challenge, indicating that drinking this beverage from a blackberry micro-filtered juice is beneficial for lipid and glucose metabolism in people [212]. Overall, scientific evidence has highlighted the beneficial effects of berries as a dietary supplement in the treatment of human diseases, including diabetes and atherosclerosis [213]. More in vitro, in vivo and clinical studies are necessary to reaffirm the preventive and therapeutic activities of dietary berries in human disorders. Dietary berries could be highly developed in the nutraceutical and functional food industries. Although the favorable effects of dietary berries on the prevention and management of human illness, they should be recommended as part of a healthy diet.
The daily diet contains a wide range of secondary metabolites, with polyphenols
and flavonoids being highest in abundance, which may prevent the onset of various
chronic diseases, including diabetes and atherosclerosis [214, 215]. As the
highest components of plant secondary metabolites, polyphenols contain a benzene
ring with hydroxyl (OH) moieties, ranging from simple flavonoids and phenolic
acids to complex procyanidins [214, 215]. A number of scientists tested the
therapeutic potential of polyphenols and flavonoids, and found that both
phytochemicals possess anti-diabetic, anti-oxidative, cardioprotective,
neuroprotective, anticarcinogenic, anti-inflammatory effects, to name a few
[216, 217, 218, 219]. Actually, polyphenols and flavonoids in colorful fruits and
vegetables confer anti-diabetic actions in experimental animal models and human
studies [220]. Molecular studies have shown that polyphenols and flavonoids
contribute to human health by regulating metabolic and signaling pathways at
various levels [214]. The potential effects of polyphenolic compounds on glucose
and lipid homeostasis have been studied from in vitro, in vivo,
and clinical studies. A systemic review and meta-analysis has demonstrated that
intake of polyphenols is capable of preventing or treating diabetic complications
[221]. A clinical study has revealed that supplementation of polyphenols,
flavonoids, and stilbenes could reduce the risk of diabetic patients at high risk
of cardiovascular disorders [222]. Consistent with clinical studies, cellular and
animal studies support the benefits of various individual polyphenols in diabetes
and its complications, including flavan-3-ols (EGCG), flavonols (quercetin),
isoflavones (genistein), flavanones (naringenin), anthocyanidins, phenolic acids
(caffeic acid and gallic acid), stilbenes (resveratrol) and curcumin [214]. For
instance, polyphenols, including resveratrol (a major polyphenol in red wine),
apigenin, and S17834 (a synthetic polyphenol), are documented to inhibit the
acceleration of aortic lesion development in diabetic LDL receptor-deficient mice
[223]. Further studies have shown that the beneficial abilities of such
polyphenols are abrogated by overexpression of dominant-negative AMPK mutants,
suggesting the involvement of AMPK signaling in polyphenols effects [223].
Numerous studies have indicated that flavonoids might be beneficial for diabetes
and its complications through reducing insulin resistance, inflammation, and
oxidative stress in skeletal muscle and fat, reducing apoptosis and promoting
proliferation of pancreatic
Natural constituents from medicinal plants have the potential for the prevention and treatment of diabetic atherosclerosis. We reviewed the current therapeutic potential and mechanisms of plant and herbal medicines in diabetic atherosclerosis. However, the clinical evidence associating various herbs and their benefits in diabetes-associated atherosclerosis is not extensive. First, most of the clinical trials on herbal medicines used small sample sizes, presented incomplete data, and did not use random designs. Moreover, exclusion and inclusion criteria are unspecific in several clinical studies, thereby limiting clinical applications of herbal medicines in patients with diabetic atherosclerosis. In this regard, rigorous clinical trials with large sample sizes and randomized, controlled designs are warranted to confirm the therapeutic efficacies of these medicines in diabetic atherosclerosis. Second, unlike patent drugs, most of the formulas prescribed by doctors might contain different amounts of ingredients and treatment cycles may vary from patient to patient. Therefore, there is a need to systematically and accurately evaluate the efficacy of TCM formulas in the management of diabetic atherosclerosis. Third, it is more likely that Chinese herbal medicines are used to treat human diseases together with other drugs in modern medical practice. Therefore, interactions between herbs and other drugs should be carefully assessed. Fourth, some herbs have toxic side effects. However, Chinese herbal medicine combinations have reduced toxicities and improved efficacies. Unfortunately, adverse effects of Chinese herbal medicines have seldom been mentioned in published in vivo studies. Organ-specific toxic effects and pharmacological doses of most herbal medicines should be probed in both animal studies and clinical studies. Fifth, diabetic atherosclerosis is a multi-stage disease caused by multiple factors. However, most of the published documents evaluated the effects of Chinese herbs by assessing one or several aspects of diabetic atherosclerosis. The underlying mechanisms of Chinese medicines in diabetic atherosclerosis should be systematically evaluated. Last, active components in distinct compounds have not been defined, and their molecular targets are inconclusive. Therefore, emergence of systems biology and network pharmacology provides great possibilities for comprehensively analyzing and predicting large-scale drug target interactions. Despite these challenges, well-designed clinical trials and experimental studies should be performed to establish the mechanisms of Chinese medicines in order to promote their modernization for the prevention and treatment of diabetes-associated atherosclerosis. In addition, identification of novel molecules and signaling cascades in diabetes and atherosclerosis will enhance our understanding of multifaceted characteristics of diabetes-associated atherosclerosis. Systems biology, such as proteomics, genomics, transcriptomics, and metabolomics, single cell transcriptomics, and spatial transcriptomics may serve as tools for exploring interventions of herbal medicine in diabetes-associated atherosclerosis. Evaluation of multi-target mechanisms of herbal medicine will inform the development of drugs for treatment of diabetic atherosclerosis.
Although studies have shown that herb medicines, dietary berries, plant polyphenols and flavonoids can potentially be used in diabetic atherosclerosis, clinical translation of these findings should be done carefully. Additionally, unfavorable pharmacokinetics, pharmacodynamics, poor water solubility, rapid metabolism, and low bioavailability might limit extensive clinical applications of some herbs. Therefore, a number of their derivatives and analogs or novel delivery methods have been developed. Comprehensive investigations of herbal medicines in diabetic and atherosclerosis will improve our understanding of their pharmacological actions and inform on novel therapeutic targets for human diseases. Overall, plant and herbal medicines present a promising direction for the treatment of diabetes-associated atherosclerotic disease. In future, the combination of herbal and western medicines might facilitate the treatment of diabetic atherosclerosis. Therefore, exploration of drug interactions and adverse effects are mandatory.
All authors contributed significantly to this review. ZCW and HJS proposed the concept and wrote the manuscript. MZL helped to draw schematic diagrams. JOM, KXL, and HJS were responsible for reviewing and editing the original draft.
Not applicable.
We thank JOM for his intelligent discussion in revision.
This research was funded by the National Natural Science Foundation of China (8217021262 and 81700364), high-level introduction of talents and scientific research start-up funds of CPU (3150020068), Jiangsu Natural Science Foundation (BK20170179).
The authors declare no conflict of interest.