


 , Mladjan D. Golubović 1,2, Milan V. Lazarević 1,2, Tomislav L. Kostić 2,3, Dragana S. Stokanović 2, Miodrag N. Đorđević 2,4, Vesna G. Marjanović 2,5, Marija D. Stošić 5, Dragan J. Milić 1,2
, Mladjan D. Golubović 1,2, Milan V. Lazarević 1,2, Tomislav L. Kostić 2,3, Dragana S. Stokanović 2, Miodrag N. Đorđević 2,4, Vesna G. Marjanović 2,5, Marija D. Stošić 5, Dragan J. Milić 1,21 Clinic of Cardiovascular Surgery, Clinical Center Nis, 18000 Nis, Serbia
2 Medical School of Nis, University of Nis, 18000 Nis, Serbia
3 Clinic for Cardiology, Clinical Center Nis, 18000 Nis, Serbia
4 Clinic for Endocrine Surgery, Clinical Center Nis, 18000 Nis, Serbia
5 Clinic for Anesthesiology and Intensive Therapy, Clinical Center Nis, 18000 Nis, Serbia
Academic Editor: Carmela Rita Balistreri
Abstract
Elderly patients scheduled for major elective vascular surgery are at high risk
for a major adverse cardiac events (MACE). The objectives of the study were: (1)
To determine the individual discriminatory ability of four risk prediction models
and four biomarkers in predicting MACEs in elderly patients undergoing major
elective vascular surgery; (2) to find a prognostic model with the best
characteristics; (3) to examine the significance of all preoperative parameters;
and (4) to determine optimal cut-off values for biomarkers with best predictor
capabilities. We enrolled 144 geriatric patients, aged 69.97
Keywords
- Biomarker
- Risk score
- Elderly
- Vascular surgery
- MACE
The World Health Organization defines persons as old/elderly if they
Patients older than 40 years of age who have had vascular surgery belong to the high-risk subset [9] with rates of myocardial infarction (MI) and cardiac arrest (CA) greater than 5% [10]. The Revised Cardiac Risk Index (RCRI) or by the author known as Lee index, and Gupta Myocardial Infarction or Cardiac Arrest (MICA) score are two non-specific models for predicting peri/postoperative cardiac risk recommended by the European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA) guidelines with a class I recommendation and level of evidence B [10]. None of the above models have an adequate predictive ability in patients undergoing non-cardiac vascular surgery [11, 12]. Developed in 2017, the Geriatric-Sensitive Cardiac Risk Index (GSCRI) is a significantly better model in preoperative prediction of MI and CA than the RCRI or Gupta MICA score in a subset of geriatric patients according to c-statistics. Containing seven significant predictors, the GSCRI was developed and validated using the 2013 and 2012 geriatric cohorts, respectively, of the National Surgical Quality Improvement Program (NSQIP) [13].
Cardiac biomarkers are hallmarks of various pathophysiological mechanisms, such as inflammation, ischemia, neurohormonal activation, plaque instability or rupture, platelet activation, and myocardial wall stretch and stress [14, 15]. The latter can be established with preoperative assessment of B-type natriuretic peptide (BNP) or N-terminal fragment of pro-BNP (NT-proBNP), which is recommended according to the Canadian Cardiovascular Society (CCS) in patients 65 years or older [16]. Cardiac troponins and natriuretic peptides are biomarkers recommended by ESC with a class IIb recommendation [10]. On the basis of the data of the beneficial impact of preoperative levels of different cardiac biomarkers on increasing the predictive power of the RCRI [17, 18, 19], both in non-cardiac as well in vascular surgery, we hypothesized that there would be a similar effect on the Gupta MICA score and GSCRI. We focused the research on: (1) Biomarkers and risk scores recommended by leading professional associations, which have been shown to be useful in assessing the cardiac risk of non-cardiac and/or geriatric patients in previous studies; (2) biomarkers covering all potential pathophysiological mechanisms involved in the development of major adverse cardiac events (MACEs); and (3) biomarkers and risk scores that are widely used in clinical practice.
The objectives of this 180-day follow-up study were: (1) to determine the individual discriminatory ability of four risk-prediction models (RCRI, Gupta MICA, GSCRI, and American Society of Anesthesiologist (ASA) score) and four biomarkers (NT-proBNP, high-sensitivity troponin I (hs-TnI), high-sensitivity C-reactive protein (hs-CRP), and creatine kinase (CK)-MB for MACEs); (2) to find a prognostic model with the best characteristics in predicting MACEs on the basis of different combinations of predictors; (3) to examine the relationship of all preoperative anamnestic, clinical, and laboratory parameters with the occurrence of MACEs; and (4) to determine the optimal cut-off values for biomarkers with the best predictive abilities.
Over a period of two years (from July 2017 to July 2019), we enrolled 144
geriatric patients, aged 69.97
Blood was sampled 48 h preoperatively from the median cubital vein and stored in
vacutainer serum tubes without additives. NT-proBNP (pg/mL) and hs-TnI (ng/mL)
were measured in whole blood specimens using chemiluminescence enzyme immunoassay
(CLEIA) technology and Magtration Technology on a PATHFAST Immunoanalyser
(Mitsubishi Chemical Europe GmbH, Düsseldorf, Germany). The serum was
separated using centrifugation and frozen at -80
Online software was utilized for estimation of the RCRI [20] as well as the Gupta MICA [21] and GSCRI [22] risk scores. The ASA score [23] and the New York Heart Association (NYHA) classification [24] were determined in all patients preoperatively by the attending anesthesiologist.
The outcome of interest was the appearance of a MACE within six months from the date of surgery. We defined MACEs as an extended spectrum of five cardiovascular complications: myocardial infarction, cardiac arrest, decompensated heart failure, new-onset atrial fibrillation, and stroke.
We used the Statistical Package for Social Sciences (SPSS 21.0; IBM Corp., Chicago, IL, USA) for data analysis. Baseline characteristics are presented as frequencies (qualitative variables) or, in cases of quantitative variables, as means with standard deviations or medians with interquartile ranges (for data deviating heavily from normal distribution on the basis of a contingent of distributional characteristics (i.e., skewness, presence of extreme values, and Shapiro–Wilk test). A parametric method, Student’s t-test, and a non-parametric method, Mann–Whitney U-test, were used for quantitative variables. Fisher’s exact test was performed to determine the association between qualitative variables. Significant predictors of MACE occurrence were identified using univariate and multivariate binary logistic regression modeling and Cox regression modeling. In addition, receiver operating characteristic (ROC) curve analyses were performed to evaluate the discriminatory power of various risk scores and biomarkers, as well as to determine the optimal cut-off values. ROC curves for multiple variables were constructed on the basis of probabilities obtained by binary logistic regression modeling. ROC curves were compared with the DeLong test using MedCalc software (v. 19.0; MedCalc Software Ltd, Ostend, Belgium). A p-value less than 0.05 was considered to be a measure of statistical significance.
During the first six months after the surgical intervention, MACE was noted in 33 (22.9%) patients. Almost two thirds (21 patients) of these patients had a MACE in the first month. About half of them (16 patients) had only one event, while 10 patients (6.9%) had two events. One patient experienced five, the maximum number of events recorded. Three patients (2.1%) died during follow-up. The most frequent MACE was decompensated heart failure, which occurred in 22 patients (15.3%). New onset atrial fibrillation was registered in 13 patients (9%), and myocardial infarction and ventricular arrhythmia occurred in eight patients each (5.5%). Two patients (1.39%) had a stroke during follow-up.
MACEs in the first six months after the intervention were associated with female
gender (p
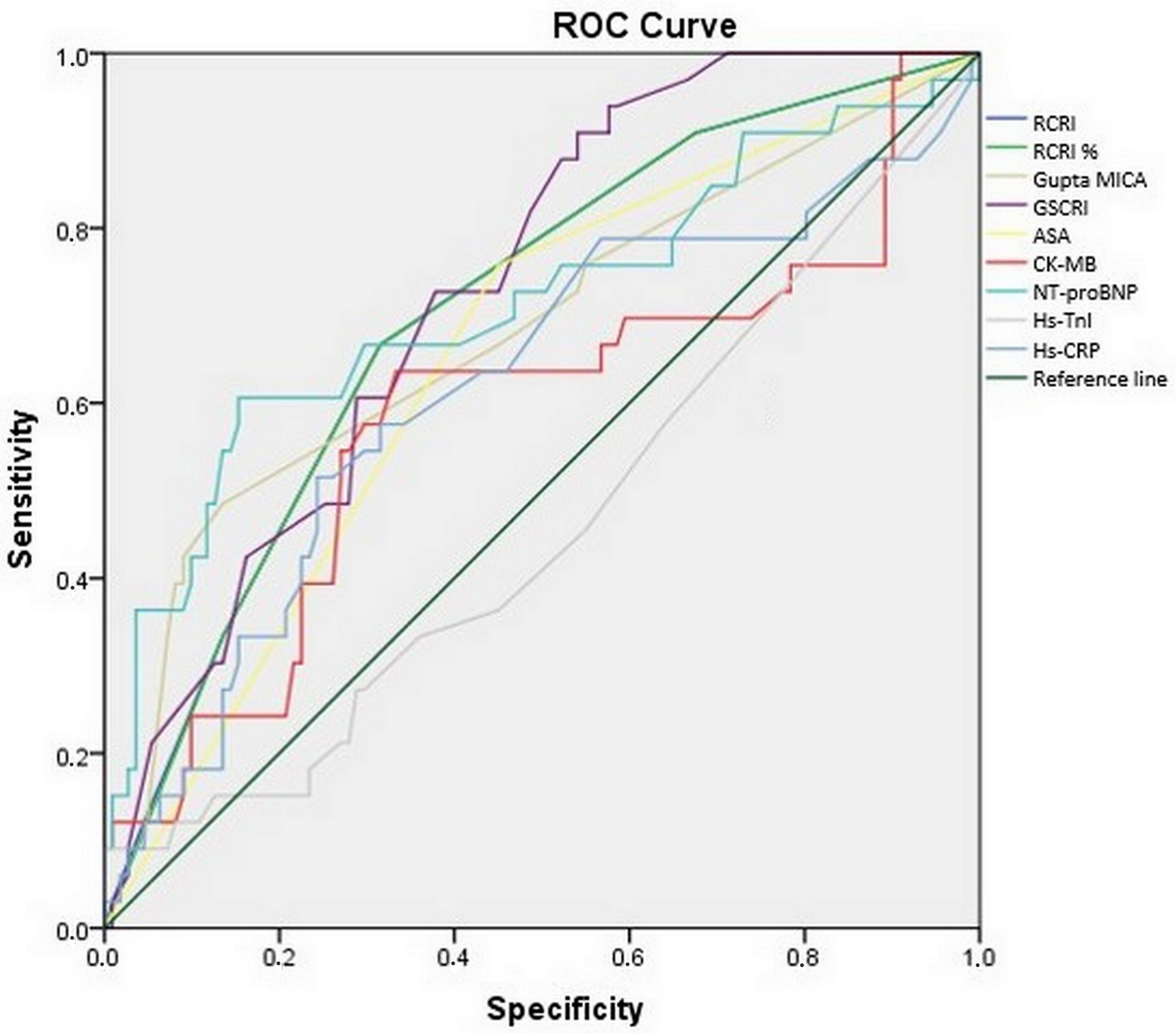 Fig. 1.
Fig. 1.Individual discriminative ability of risk scores and biomarkers. The receiver operating characteristic (ROC) curve illustrates the discriminative ability of four biomarkers and four risk scores. Abbreviations: ROC, receiver operating characteristic; RCRI, Revised Cardiac Risk Index; MICA, myocardial infarction and cardiac arrest; GSCRI, Geriatric-Sensitive Cardiac Risk Index; ASA, American Society of Anesthesiologist; CK, creatine kinase - MB isoenzyme; NT-proBNP, N-terminal fragment of pro-B-type natriuretic peptide; Hs-TnI, High-sensitivity troponin I; Hs-CRP, high-sensitivity C-reactive protein.
| Variable | With MACE | Without MACE | p-value |
| Age (years) | 69.76 |
69.65 |
0.109* |
| aGender (male) | 5 (15.2%) | 45 (40.5%) | 0.007 |
| Dyspnea (NYHA class) | 2.58 |
2.04 |
|
| Atrial fibrillation | 3 (9.1%) | 4 (3.6%) | 0.197 |
| Previous CVI | 5 (15.2%) | 37 (32.5%) | 0.051 |
| Previous CAD | 14 (42.4%) | 17 (15.3%) | 0.002 |
| Previous cardiomyopathy | 6 (18.2%) | 12 (10.8%) | 0.367 |
| Prior PCI | 2 (6.1%) | 3 (2.7%) | 0.323 |
| Previous MI | 9 (27.3%) | 16 (14.4%) | 0.115 |
| Prior CABG | 1 (3.0%) | 1 (0.9%) | 0.407 |
| Previous hypertension | 30 (90.9%) | 92 (82.9%) | 0.408 |
| Previous DM | 14 (42.4%) | 39 (35.1%) | 0.538 |
| Insulin-dependent DM | 11 (33.3%) | 22 (19.8%) | 0.155 |
| Insulin-independent DM | 3 (9.1%) | 17 (15.3%) | 0.567 |
| Previous hyperlipidaemia | 10 (30.3%) | 23 (20.7%) | 0.361 |
| Smoking | 16 (48.5%) | 41 (36.9%) | 0.311 |
| Family history | 18 (54.5%) | 38 (34.2%) | 0.043 |
| Beta-blocker | 27 (81.8%) | 77 (69.4%) | 0.189 |
| ACE inhibitor | 28 (84.8%) | 78 (70.3%) | 0.117 |
| Calcium channel antagonist | 16 (48.5%) | 23 (20.7%) | 0.003 |
| Antiplatelet therapy | 27 (81.8%) | 55 (49.5%) | 0.001 |
| Statins | 17 (51.5%) | 51 (45.9%) | 0.692 |
| Diuretics | 3 (9.1%) | 21 (18.9%) | 0.286 |
| Nitrates | 3 (9.1%) | 7 (6.3%) | 0.696 |
| Intervention type | 0.006 | ||
| AAAR | 13 (39.4%) | 18 (16.2%) | |
| CE | 14 (42.4%) | 66 (59.5%) | |
| AFBP | 2 (6.1%) | 1 (0.9%) | |
| FPBP | 4 (12.1%) | 26 (23.4%) | |
| ASA score | 3.0 (2.5–3.0) | 2.0 (2.0–3.0) | 0.002 |
| Haemoglobin (g/dL) | 13.4 (12.0–14.3) | 13.6 (12.5–14.4) | 0.479 |
| Creatinine ( |
92.0 (80.2–125.6) | 88.4 (79.0–106.6) | 0.166 |
| WBC count (10 |
7.3 (6.4–8.6) | 7.0 (5.8–8.1) | 0.161 |
| Platelet count (10 |
213.0 (148.0–251.0) | 228.0 (191.0–274.0) | 0.073 |
| Urea (mmol/L) | 6.0 (5.2–8.6) | 5.6 (5.0–6.9) | 0.176 |
| CRP (mg/L) | 2.8 (2.0–4.9) | 3.4 (2.1–6.5) | 0.403 |
| LDL (mmol/L) | 2.84 |
2.79 |
0.783* |
| HDL (mmol/L) | 1.2 (0.9–1.3) | 1.2 (1.0–1.4) | 0.263 |
| CK-MB (U/L) | 104.0 (47.5–132.0) | 74.0 (56.0–108.0) | 0.130 |
| EF (%) | 50.06 |
55.76 |
|
| BMI (kg/m |
25.76 |
25.65 |
0.844* |
| ICU (days) | 3.0 (2.0–4.0) | 1.0 (1.0–1.0) | |
| RCRI | 2.06 |
1.18 |
|
| RCRI (%) | 10.18 |
7.27 |
|
| Gupta MICA | 0.7 (0.2–1.5) | 0.4 (0.2–0.7) | 0.001 |
| GSCRI | 4.5 (1.9–11.1) | 1.7 (0.3–7.2) | |
| NT-proBNP (pg/mL) | 234.0 (89.2–429.5) | 95.0 (74.0–114.0) | |
| Hs-TnI (ng/mL) | 0.003 (0.001–0.008) | 0.004 (0.002–0.010) | 0.559 |
| Hs-CRP (mg/L) | 0.9 (0.4–3.2) | 0.4 (0.3–0.9) | 0.040 |
| Legend: *, t-test; NYHA, New York Heart Association; CVI, cerebrovascular insult; CAD, coronary artery disease; PCI, percutaneous coronary intervention; MI, myocardial infarction; CABG, coronary artery bypass graft; DM, diabetes mellitus; ACE, angiotensin converting enzyme; AAAR, repair of abdominal aortic aneurysm; CE, carotid endarterectomy; AFBP, aortobifemoral bypass; FPBP, femoropopliteal bypass; ASA, American Society of Anesthesiologist; WBC, white blood cells; CRP, C-reactive protein; LDL, low-density lipoprotein; HDL, high-density lipoprotein; CK-MB, MB isoenzyme of creatine kinase; EF, ejection fraction; BMI, body mass index; ICU, intensive care unit; RCRI, Revised Cardiac Risk Index; MICA, myocardial infarction and cardiac arrest; GSCRI, Geriatric-Sensitive Cardiac Risk Index; NT-proBNP, N-terminal fragment of pro-B-type natriuretic peptide; Hs-TnI, High-sensitivity troponin I; Hs-CRP, high-sensitivity C-reactive protein. | |||
| Variable | Area (95% CI) | p-value | Cut-off | Sensitivity (%) | Specificity (%) |
| RCRI | 0.707 (0.609–0.805) | 2 | 66.7 | 68.5 | |
| RCRI (%) | 0.706 (0.608–0.804) | 10.1 | 66.7 | 68.5 | |
| Gupta MICA | 0.682 (0.570–0.795) | 0.001 | 0.8 | 48.5 | 86.5 |
| GSCRI | 0.731 (0.644–0.818) | 1.5 | 90.9 | 45.9 | |
| ASA score | 0.654 (0.551–0.757) | 0.008 | 3 | 75.8 | 55 |
| NT-proBNP (pg/mL) | 0.713 (0.600–0.826) | 208 | 60.6 | 84.7 | |
| Hs-TnI (ng/mL) | 0.462 (0.347–0.578) | 0.512 | 0.035 | 9.1 | 100 |
| Hs-CRP (mg/L) | 0.618 (0.501–0.735) | 0.04 | 0.92 | 51.5 | 75.7 |
| CK-MB (U/L) | 0.587 (0.465–0.709) | 0.13 | 94 | 63.6 | 66.7 |
| Legend: RCRI, Revised Cardiac Risk Index; MICA, myocardial infarction and cardiac arrest; GSCRI, Geriatric-Sensitive Cardiac Risk Index; ASA, American Society of Anesthesiologist; NT-proBNP, N-terminal fragment of pro-B-type natriuretic peptide; Hs-TnI, High-sensitivity troponin I; Hs-CRP, high-sensitivity C-reactive protein; CK-MB, MB isoenzyme of creatine kinase. | |||||
Further, we have tested various combinations of risk scores and markers to
determine the best combination. Out of the total of eight risk scores and
biomarkers tested, three (ASA risk score, hs-TnI, and hs-CRP) did not add to the
discriminatory ability of the combinations. Excellent discriminatory ability (AUC
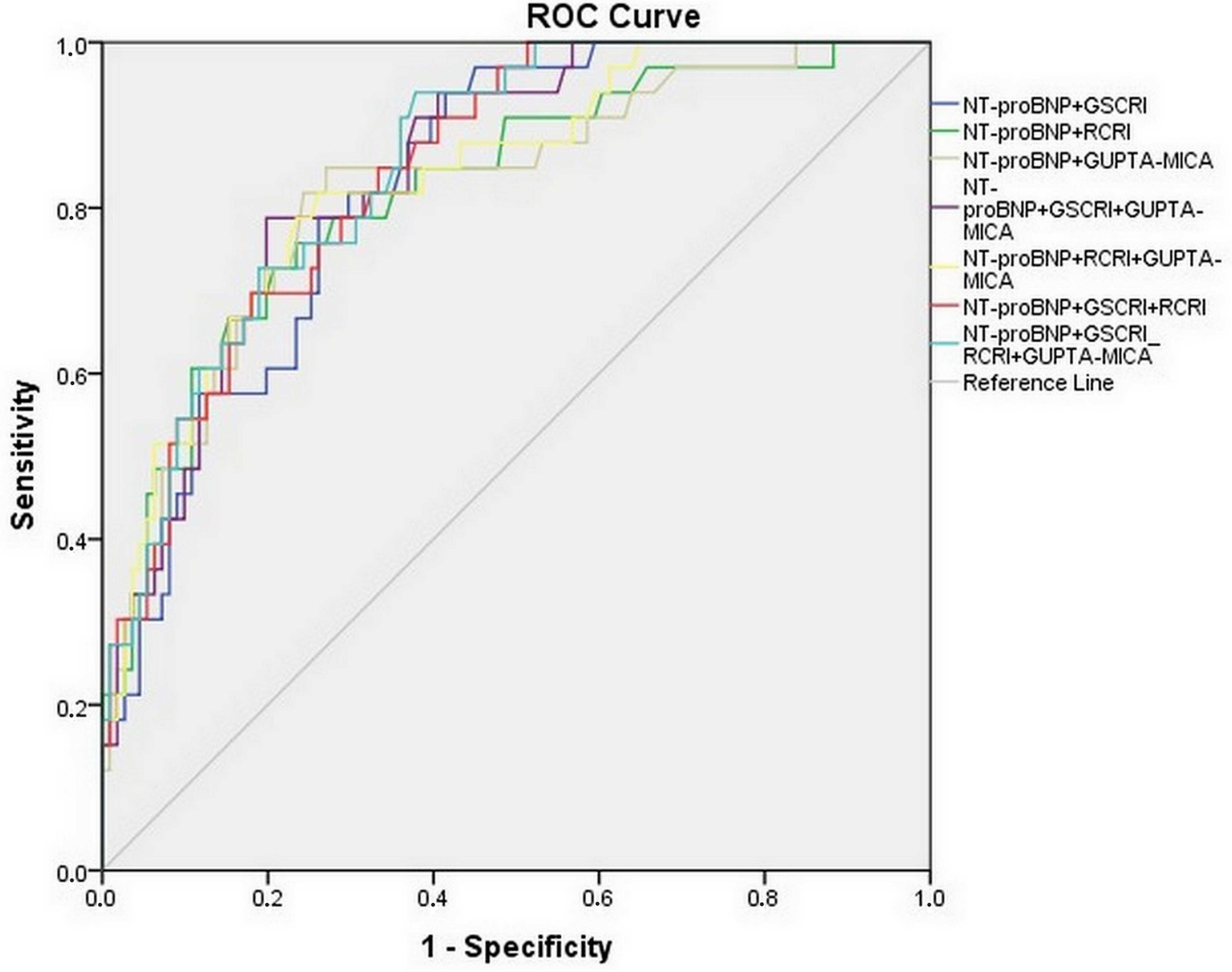 Fig. 2.
Fig. 2.Discriminative ability of NT-proBNP and different risk-score combinations. The receiver operating characteristic (ROC) curve illustrates the discriminative ability seven different NT-proBNP combinations of biomarkers and/or risk scores. Abbreviations: ROC, receiver operating characteristic; NT-proBNP, N-terminal fragment of pro-B-type natriuretic peptide; GSCRI, Geriatric-Sensitive Cardiac Risk Index; RCRI, Revised Cardiac Risk Index; MICA, myocardial infarction and cardiac arrest.
Using the binary logistic regression method, univariable analysis identified a
number of possible predictors of MACE occurrence within six months after the
surgical intervention. Previously determined cut-offs for Gupta MICA, GSCRI,
NT-proBNP, and hs-CRP had greater predictive values than any risk
scores/biomarkers by themselves. Nevertheless, we found only three independent
predictors in the multivariable model explaining 44.5%–67.5% of the MACE
occurrence variance (
| Variable | Univariable analysis - OR (95% CI) | p-value | Multivariable analysis - OR (95% CI) | p-value |
| Gender (female) | 3.818 (1.371–10.633) | 0.01 | 7.303 (1.084–49.208) | 0.041 |
| Previous CAD | 4.074 (1.720–9.650) | 0.001 | 10.380 (1.320–81.599) | 0.026 |
| Positive family history | 2.305 (1.047–5.077) | 0.038 | 0.436 (0.091–1.950) | 0.277 |
| Calcium channel antagonists | 3.601 (1.582–8.198) | 0.002 | 1.377 (0.266–7.131) | 0.703 |
| Antiplatelet drugs | 4.582 (1.755–11.962) | 0.002 | 2.911 (0.455–18.620) | 0.259 |
| Dyspnea (NYHA class) | 4.443 (2.128–9.274) | 1.444 (0.317–6.582) | 0.635 | |
| ASA score | 3.812 (1.582–9.188) | 0.003 | 1.059 (0.089–12.577) | 0.964 |
| EF (%) | 0.881 (0.823–0.942) | 0.928 (0.834–1.033) | 0.174 | |
| CK-MB (U/L) | 1.006 (1.001–1.011) | 0.017 | 1.010 (1.000–1.020) | 0.058 |
| CE vs. AAAR | 0.294 (0.117–0.735) | 0.009 | 0.491 (0.050–4.861) | 0.543 |
| AFBP vs. AAAR | 2.769 (0.226–33.879) | 0.425 | 31.339 (0.570–1722.649) | 0.092 |
| FPBP vs. AAAR | 0.213 (0.060–0.760) | 0.017 | 2.299 (0.133–37.361) | 0.577 |
| RCRI | 1.788 (1.285–2.486) | 0.001 | ||
| RCRI (%) | 1.194 (1.082–1.317) | 0.935 (0.686–1.275) | 0.673 | |
| RCRI ( |
4.343 (1.899–9.931) | 0.001 | ||
| Gupta MICA | 2.720 (1.465–5.049) | 0.002 | ||
| Gupta MICA ( |
6.024 (2.516–14.421) | 2.486 (0.403–15.339) | 0.327 | |
| GSCRI | 1.135 (1.051–1.227) | 0.001 | ||
| GSCRI ( |
8.500 (2.450–29.495) | 0.001 | 6.775 (0.830–55.268) | 0.074 |
| NT-proBNP (pg/mL) | 1.006 (1.003–1.009) | |||
| NT-proBNP ( |
8.507 (3.569–20.276) | 25.599 (4.869–134.574) | 0 | |
| Hs-CRP ( |
3.306 (1.472–7.421) | 0.004 | 3.751 (0.761–18.487) | 0.104 |
| Legend: OR, odds ratio; CI, confidence interval; CAD, coronary artery disease; NYHA, New York Heart Association; ASA, American Society of Anesthesiologist; EF, ejection fraction; CK-MB, MB isoenzyme of creatine kinase; AAAR, repair of abdominal aortic aneurysm; CE, carotid endarterectomy; AFBP, aortobifemoral bypass; FPBP, femoropopliteal bypass; RCRI, Revised Cardiac Risk Index; MICA, myocardial infarction and cardiac arrest; GSCRI, Geriatric-Sensitive Cardiac Risk Index; NT-proBNP, N-terminal fragment of pro-B-type natriuretic peptide; Hs-CRP, high-sensitivity C-reactive protein. | ||||
Similar predictors were identified for 6-month survival without a MACE. In the
multivariable Cox regression model (
| Variable | Univariable analysis - HR (95% CI) | p-value | Multivariable analysis - HR (95% CI) | p-value |
| Gender (female) | 3.177 (1.226–8.231) | 0.017 | 1.713 (0.543–5.407) | 0.358 |
| Previous CAD | 2.998 (1.502–5.983) | 0.002 | 1.818 (0.566–5.840) | 0.315 |
| Positive family history | 2.003 (1.009–3.977) | 0.047 | 1.491 (0.533–4.169) | 0.447 |
| Calcium channel antagonists | 2.767 (1.396–5.482) | 0.004 | 0.715 (0.212–2.415) | 0.589 |
| Antiplatelet drugs | 3.811 (1.572–9.235) | 0.003 | 2.566 (0.762–8.639) | 0.128 |
| Dyspnea (NYHA class) | 3.600 (1.925–6.735) | 1.752 (0.584–5.256) | 0.317 | |
| ASA score | 3.170 (1.429.7.033) | 0.005 | 2.163 (0.388–12.056) | 0.379 |
| EF (%) | 0.905 (0.860–0.953) | 1.001 (0.934–1.073) | 0.974 | |
| CK-MB (U/L) | 1.004 (1.002–1.006) | 0.001 | 1.002 (0.999–1.005) | 0.115 |
| CE vs. AAAR | 0.386 (0.181–0.823) | 0.014 | 0.261 (0.056–1.213) | 0.087 |
| AFBP vs. AAAR | 2.069 (0.466–9.197) | 0.339 | 6.537 (0.794–53.662) | 0.08 |
| FPBP vs. AAAR | 0.290 (0.095–0.891) | 0.031 | 0.789 (0.145–4.303) | 0.784 |
| RCRI | 1.504 (1.185–1.908) | 0.001 | ||
| RCRI (%) | 1.145 (1.059–1.239) | 0.001 | 0.849 (0.690–1.094) | 0.231 |
| RCRI ( |
3.495 (1.696–7.215) | 0.001 | ||
| Gupta MICA | 1.907 (1.304–2.790) | 0.001 | ||
| Gupta MICA ( |
4.182 (2.105–8.312) | 1.407 (0.451–4.391) | 0.556 | |
| GSCRI | 1.097 (1.038–1.160) | 0.001 | 1.071 (0.987–1.161) | 0.098 |
| GSCRI ( |
7.050 (2.150–23.121) | 0.001 | ||
| NT-proBNP (pg/mL) | 1.004 (1.003–1.006) | 1.004 (1.001–1.006) | 0.002 | |
| NT-proBNP ( |
5.928 (2.939–11.955) | |||
| Hs-TnI (ng/mL) | 1889.529 (2.136–1671404.819) | 0.029 | 1460.863 (0.216–9895313.278) | 0.105 |
| Hs-CRP ( |
2.822 (1.424–5.590) | 0.003 | 2.716 (1.107–6.665) | 0.029 |
| Legend: HR, hazard ratio; CI, confidence interval; CAD, coronary artery disease; NYHA, New York Heart Association; ASA, American Society of Anesthesiologist; EF, ejection fraction; CK-MB, MB isoenzyme of creatine kinase; AAAR, repair of abdominal aortic aneurysm; CE, carotid endarterectomy; AFBP, aortobifemoral bypass; FPBP, femoropopliteal bypass; RCRI, Revised Cardiac Risk Index; MICA, myocardial infarction and cardiac arrest; GSCRI, Geriatric-Sensitive Cardiac Risk Index; NT-proBNP, N-terminal fragment of pro-B-type natriuretic peptide; Hs-TnI, High-sensitivity troponin I; Hs-CRP, high-sensitivity C-reactive protein. | ||||
The goal of preoperative risk assessment is to reduce not only perioperative but also long-term postoperative mortality and morbidity through the development of a strategy for optimization of a patient’s clinical condition. Adverse cardiac events are responsible for nearly half of perioperative deaths [25]. The lack of a generally accepted definition of MACE [14], differences in high-sensitivity biomarker assays [26], and consequent changes in the definitions of individual cardiac events [27] are several problems in analyzing and comparing study results. The term MACE was established to assess the safety and effectiveness of various cardiac therapeutic methods [28] and has long referred to the manifestations of the atherosclerotic process in the coronary and cerebral vasculature [29]. In our study, MACEs represent a composite of a wide range of postoperative complications, and our aim was to undertake a more comprehensive evaluation of cardiovascular risk prediction. In this regard, decompensated heart failure and new-onset atrial fibrillation were the two most common adverse events, although they may not be directly related to atherosclerosis.
Because of systemic atherosclerosis, over 90% of patients scheduled for major vascular surgery have pathological substrate on coronary arteries [30]. Various intraoperative conditions that are not easy to incorporate into predictive models, such as tachycardia, hypotension, bleeding, and duration of surgery are independently associated with MACEs. Mentioned factors and others, like bradycardia and hypertension, are part of the overall cardiac risk of vascular surgery [31]. If the frequency of pathoanatomical changes, loss of functional organic reserve, and homeostatic imbalances associated with aging are added to this, a subgroup of elderly vascular surgical patients with an exceptional risk of postoperative cardiac complications is obtained [32, 33]. A group from the University of Pittsburgh performed a retrospective cohort study involving over four million patients over the age of 65, recognized age as a risk factor for postoperative mortality, and proposed expanding the list of surgical procedures to be designated as high risk [7].
Although widely used, RCRI did not achieve an adequate level of prediction of
MACEs in patients expecting abdominal aneurysm repair, relying on data from the
original study [34], which was also shown in subsequent research [35]. The
results of the study from which it was derived showed a better predictive ability
of GSCRI compared with RCRI and Gupta MICA for myocardial injury and cardiac
arrest after 30 days, both in geriatric (0.76) and in the overall population
(0.83) [13]. The same study found that the Gupta MICA was the risk score with the
highest degree of underestimation of cardiovascular complications in the
geriatric subgroup. Our results indicated that the highest AUC occurred using the
GSCRI risk score (0.731). A good level of discrimination, with an AUC above 0.7,
was shown by adopting NT-proBNP (0.713) and RCRI (0.707). We interpret the better
characteristics of RCRI in relation to the Gupta MICA score in the following
ways: (1) The most common complication was decompensated heart failure, and it
was found in two thirds of patients who have had a MACE. Unlike the Gupta MICA
score, both RCRI and GSCRI include evidence of a history of heart failure in
their design. We found a significant association (p
Both in the above-mentioned and in our study, the value of AUC obtained by applying GSCRI in geriatric patients was not higher than 0.8, which is a generally accepted value for the excellent discriminatory ability of a biomarker and/or score [37]. This indicates difficulty in stratifying cardiovascular risk in subgroups of patients with highly variable health conditions, such as geriatric and vascular disease.
A multivariable model of binary logistic and Cox regression analysis confirmed
earlier evidence of a connection between NT-proBNP and MACEs after vascular
surgery [19]. This natriuretic peptide has been singled out as a biomarker with
the greatest discriminatory potential. Its advantage over other biomarkers is
that it can be a recognizable sign of a wider range of heart conditions such as
asymptomatic ischemia, left ventricular hypertrophy and/or systolic dysfunction,
and left atrial dilatation and/or fibrillation [38]. In a study that included
over 300 patients who underwent major vascular surgery, it was reported that
using a cut-off value of 319 ng/L for preoperative NT-proBNP was an excellent
predictor of postoperative MACEs after 6 months [39]. We have identified that a
NT-proBNP cut-off value of 208 ng/L had a hazard ratio for postoperative MACEs of
almost 26 (95% CI:
Female gender and preexisting coronary artery disease are two possible predictors of MACE that were obtained by application of the multivariable model of binary logistic regression. Systemic stress response associated with vascular surgery is a trigger for the development of acute coronary syndrome in patients with preexisting coronary artery disease [43]. Because of a sharp drop in estrogen, 50-year-old women are thought to be at higher risk for developing cardiovascular disease than 70-year-old men [44]. Older females have the highest incidence of heart failure with preserved ejection fraction, and this form of heart failure accounts for about 90% of all new episodes [45]. This may also explain the association of antiplatelet agents and calcium channel blockers with the occurrence of MACEs. Antiplatelet drugs are routinely used preoperatively in patients with previous coronary artery disease and calcium antagonists, as safe drugs for this form of heart failure [46] are often the first choice in controlling systolic and diastolic hypertension, ischemia, and improving diastolic relaxation [47].
Our results confirmed the poor predictive ability of preoperative troponin
measurement for MACEs after vascular surgery [17]. In contrast, we established
that preoperative hs-CRP was a useful biomarker for predicting 6-month
postoperative cardiovascular events. We do not consider this result surprising as
earlier studies examining cardiac events at longer time intervals after vascular
surgery have confirmed the usefulness of hs-CRP [48, 49]. The reason for the good
predictive ability of hs-CRP for a wide group of cardiovascular events may be its
correlation with the increase in proinflammatory cytokines, which is
characteristic not only for the process of atherosclerosis but also occurs in
congestive heart failure [45]. The Cox regression multivariable model singled out
hs-CRP and NT-proBNP as the only two independent predictors among the biomarkers,
risk scores, and preoperative anamnestic data. Hs-CRP levels
Elderly patients scheduled for major elective vascular surgery are at high risk for a MACE during the 6-month postoperative period, the most common of which is decompensated heart failure. Researching new approaches in MACE prediction is a complex and challenging process both because of the inability of an individual score or biomarker to give a satisfactory level of prediction and because of the constant aspiration of clinicians to make these procedures simple and applicable. NT-proBNP as a biomarker and GSCRI as a risk score showed the greatest predictive potential in our study. GSCRI + NT-proBNP is a two-variable model with excellent predictive ability. More complicated models with three or more variables did not provide a significant increase in discriminatory power. We believe that the combination of GSCRI + NT-proBNP enables the identification of patients at particular risk for a cardiovascular event who could benefit from aggressive preoperative reduction of risk factors, more careful perioperative monitoring, and stricter control of hemodynamic parameters. This can serve as a guide in future studies for creating a categorical classification system on the basis of value intervals of NT-proBNP and calculated risk for the same.
MI, myocardial infarction; CA, cardiac arrest; RCRI, Revised Cardiac Risk Index; ESC, European Society of Cardiology; ESA, European Society of Anaesthesiology; GSCRI, Geriatric-Sensitive Cardiac Risk Index; NSQIP, National Surgical Quality Improvement Program; BNP, B-type natriuretic peptide; NT-proBNP, N-terminal fragment of pro-B-type natriuretic peptide; CCS, Canadian Cardiovascular Society; Hs-TnI, high-sensitivity troponin I; Hs-CRP, high-sensitivity C-reactive protein; CLEIA, chemiluminescence enzyme immunoassay technology; CK-MB, MB isoenzyme of creatine kinase; ASA, American Society of Anesthesiologist; MACE, major adverse cardiac event; SPSS, Statistical Package for Social Sciences; ROC, receiver operating characteristic; NYHA, New York Heart Association; CAD, coronary artery disease; ICU, intensive care unit; AUC, area under the curve.
All authors contributed significantly to this study and revised the manuscript. VP, MG, ML and DM are responsible for conceptualization of the research and data collection. VP, MG, TK and DS analyzed the data. VP, MĐ, MS and VM interpreted the data. VP wrote the paper.
The research was performed at Clinic for Cardiovascular Surgery, Clinical Center Nis in accordance with the Helsinki Declaration principles. The Study was approved by Ethics Committee of the Faculty of Medicine, University of Nis, Nis, Serbia (chairperson - professor Vladmila Bojanic; protocol number - 12-5342/2; date of approval 31.05.2017.). All participants gave informed written consent for participation in this study, prior to enrollment.
Thanks to all the anonymous peer reviewers for their opinions and suggestions.
This research received no external funding.
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://rcm.imrpress.com/EN/10.31083/j.rcm2203115.