


 , Zhong Zuo 1,*
, Zhong Zuo 1,*1 Department of Cardiology, The First Affiliated Hospital of Chongqing Medical University, 400016 Chongqing, China
2 Department of Cardiology, The First Affiliated Hospital of Chongqing Medical and Pharmaceutical College, 400060 Chongqing, China
3 Department of Cardiology, Chongqing Red Cross Hospital, 400020 Chongqing, China
† These authors contributed equally.
Academic Editor: Brian Tomlinson
Abstract
Heart failure (HF) is a complex clinical syndrome with symptoms and signs due to
cardiac dysfunction, leading to high hospitalization and morbidity. HF treatment
has rapidly developed in recent decades, and breakthroughs have been made.
Although conventional neurohormonal blockade therapies, including
Keywords
- Heart failure
- Diamond approach
- New therapies
- Individualized treatment
Heart failure (HF) is the biggest challenge to cardiovascular disease treatment
in the 21st century, with substantial morbidity, rehospitalization, and
mortality, which affected estimated 23 million people worldwide [1]. The
incidence of HF in American adults increased from 5.7 million to 6.2 million in
the past few years [2]. The data from
GWTG®-HF (Get With The
Guidelines–Heart Failure, Dallas, Texas, USA) showed that the rates for 5-year
mortality and readmission in patients hospitalized for HF exceeded 80% and 75%,
respectively [3]. According to the 2021 ESC
(European society of cardiology, Brussels,
Belgium) heart failure guideline, HF is now subdivided as either reduced ejection
fraction (rEF) (HFrEF: left ventricular ejection fraction (LVEF)
Although conventional neurohormonal blockade therapies significantly improve the prognosis of patients with HFrEF, mortality and rehospitalization remain high. A study enrolled 11,064 HFrEF patients showed that under neurohormonal blockade therapies, the 2-year mortality for patients with worsening HF events was as high as 22.5%, and the hospitalization for recurring malignant HF within 30 days was 56% [5].
A large amount of data showed that conventional therapies cannot meet the current needs, and HF treatment urgently needs to be updated. New therapy for HFrEF has been rapidly developing in recent years. Therapies such as ivabradine, angiotensin receptor-neprilysin inhibitor (ARNI), sodium-glucose cotransporter 2 (SGLT2) inhibitor, vericiguat, and omecamtiv mecarbil, etc., which have been proved to improve the prognosis of HFrEF patients. This article mainly clarified the timing, scope of application, contraindications for the clinical use of each agent, and optimal therapies under various clinical conditions.
Multiple factors are involved in the occurrence of HF and progressive treatment,
and therefore, it is necessary to combine drugs with different mechanisms for the
most successful treatment of HFrEF. The effective combination of
angiotensin-converting enzyme (ACE) inhibitors (ACEI)/angiotensin receptor
blockers (ARBs), mineralocorticoid receptor antagonists (MRAs), and
We proposed the diamond approach and it included new drugs and provided possible combinations based on the mechanism and clinical trials so that the most suitable drug regimen was used for an individual patient, and most importantly, to propose the necessity of the conjunction of medicines (Fig. 1). Different from the current guidelines, we proposed to use the diamond approach in an early and comprehensive manner at the beginning of ventricular remodeling in HFrEF to prevent further deterioration of HF and maximize the prognosis of patients (Fig. 2).
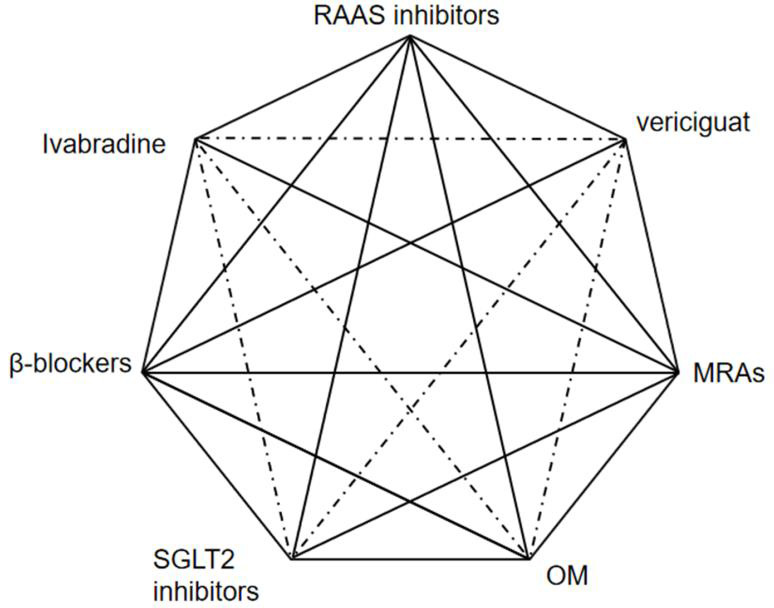 Fig. 1.
Fig. 1.Possible combinations of different heart failure drugs based on latest clinical research. The diagram shows useful combinations (thick lines), possible combinations (dotted lines). RAAS inhibitors, renin-angiotensin-aldosterone inhibitors; MRAs, mineralocorticoid receptor antagonists; SGLT2 inhibitors, sodium-glucose cotransporter 2 inhibitors; OM, omecamtiv mecarbil.
Dysregulation of cardiac
Bronchospasm was one of the adverse reactions caused by
ACEIs and ARBs reversed ventricular remodeling by blocking the
renin-angiotensin-aldosterone system (RAAS). ACEIs competitively inhibited ACE
and reduce angiotensin II (A-II), and they were important mediators of cardiac
remodeling because A-II caused myocardial hypertrophy [22] and promoted cardiac
fibrosis [23]. Same as
Contraindications to ACEIs also applied to ARBs [14, 15, 16, 17]. Several trials found
that greater cardiovascular benefits were obtained by the combination of ACEIs
and ARBs [27, 29]. However, there was no recommendation for this combination
because of the increased possibility of adverse reactions such as hypotension,
hyperkalemia, and worsening of renal function [14, 30]. There should be concern
for patients on ACEIs or ARBs if any of the following occurs: symptomatic
hypotension (systolic blood pressure (SBP)
Aldosterone was the terminal hormone of the RAAS and played a role in myocardial
remodeling. In addition to diuresis and potassium preservation, aldosterone
caused myocardial interstitial fibrosis [6]. MRAs blocked the action of
aldosterone on mineralocorticoid receptors and reversed cardiac remodeling.
Spironolactone [31] and eplerenone [32] significantly reduced the mortality and
hospitalization of HFrEF (LVEF
The correlation between adverse cardiovascular events and rapid heart rhythm has
been confirmed in patients with cardiovascular disease, and lowering the heart
rate reduced cardiovascular risk [33, 34, 35]. A retrospective cohort study found that
high resting heart rates often occured in HFrEF and were always associated with
adverse outcomes [36]. Ivabradine slowed down the heart rate by selectively
inhibiting the funny ion current (I
In the SHIFT trial, ivabradine significantly reduced HF hospitalization but not
cardiovascular or all-cause mortality compared with placebo [34]. A prospective
study showed that ivabradine is beneficial for HFrEF by effectively improving the
symptoms and quality of life [39]. Ivabradine was added to therapy when patients
have received the maximum dose of
Ivabradine should be avoided in patients with sinus bradycardia, sinoatrial
block, or second degree or above atrioventricular block [14, 16, 17]. Due to its
mechanism of action, it had no effect on cardiac inotropy or systemic vascular
resistance [33]. However, cornerstone research did not include patients with
hypotension (blood pressure (BP)
As a multi-compound drug composed of the ARB valsartan and the neprilysin inhibitor sacubitril, ARNI showed an extraordinary effect on the reversal of cardiac remodeling. The PARADIGM-HF trial demonstrated that ARNI exceeded enalapril in reducing cardiovascular mortality (hazard ratio (HR), 0.80 [95% CI, 0.71–0.89]) and hospitalization for HFrEF (HR, 0.79 [95% CI, 0.71–0.89]) patients [45]. The superiority of ARNI compared with enalapril in improving the quality of life has also been proven [46].
In the EVALUATE-HF trial, a significant reversal in cardiac remodeling was observed after 3 months of ARNI treatment for HFrEF patients [47]. The PROVE-HF study further explored the association between improvement of ventricular remodeling and the reduced level of N-terminal-pro-brain natriuretic peptide (NT-ProBNP) [48]. For patients hospitalized with acute HF, the TRANSITION study demonstrated the safety and efficacy of early in-hospital initiation of ARNI after hemodynamic stability [49], and the PIONEER-HF trial confirmed the superiority of initial treatment with ARNI compared to enalapril through the 8 weeks of follow-up [50]. Similar conclusions were made in several studies where ARNI exceeded ACE inhibitors/ARBs in reducing hospitalization [51] and improving the quality of life for HFrEF patients during the 12 months of follow-up in real world practice [52]. The cardio-renal benefit provided by natriuretic peptides indicates that ARNI was superior to other traditional RAAS inhibitors for the treatment of HF and CKD.
Despite causing a modest increase in the urine albumin-to-creatinine ratio (UACR), ARNI was found to slow the rate of decrease in the eGFR more effectively compared to enalapril [53]. Prospective researches have proved that patients with HFrEF and CKD can benefit from ARNI [54, 55]. ARNI has become a new cornerstone and first-line therapy for HFrEF in guidelines [14, 16, 30]. Common side effects of ARNI were related to hypotension, renal insufficiency, and rare angioedema. It should be further noted that the contraindications to ACE inhibitors/ARBs also apply to ARNI.
By inhibiting sodium-glucose cotransporter 2 (SGLT2) which presented at the early proximal tubule, SGLT2 inhibitors prevented the reabsorption of the majority of filtered urinary glucose, and lowered blood glucose levels. Except as glucose-lowering agents [56], SGLT2 inhibitors showed beneficial effects on hospitalization for HF, and cardiovascular and total mortality in patients with diabetes [57, 58, 59, 60, 61]. The specific mechanisms of SGLT2 inhibitors that confer cardiac benefits remained unknown, and might be related to lowering of blood pressure, diuresis, weight loss, amelioration of myocardial metabolism and fibrosis, and reduction of the excessive activation of the sympathetic nervous system (SNS) and RAAS [62, 63, 64].
In the DAPA-HF trial, dapagliflozin reduced the primary endpoint for
cardiovascular death or worsening of HF (HR, 0.74 [95% CI, 0.65–0.85];
P
The EMPEROR-Reduced trial enrolled HFrEF patients with more severe HF (73% of
patients with LVEF
A subgroup analysis of the DAPA-HF trial [71] showed that the combination of SGLT2 inhibitors and ARNI was efficacious and safe. Caution was advised in patients with genital and urinary tract infections [72, 73], ketoacidosis [74], hypovolemia (e.g., hypotension, dehydration, and cerebral infarction), or hypoglycemia (when combined with insulin or an insulin secretagogue) [75]. Ketoacidosis was a serious but extremely rare clinical condition in patients on SGLT2 inhibitors. The rate reportedly was less than 0.76/1000 patient-years in patients receiving canagliflozin [76] and 1/1000 for empagliflozin [57]. How SGLT2 inhibitors might be contributing to ketoacidosis has not been fully understood, but major illness, prolonged starvation, heavy alcohol use, and lower insulin doses were potential ketoacidosis triggers.
The nitric oxide-soluble guanylate cyclase-cyclic guanosine monophosphate (NO-sGC-cGMP) pathway was the main regulator in myocardial metabolism and endothelial function, and it was a potential target for the treatment of chronic HF [77]. As a new oral sGC stimulator, vericiguat was cardioprotective by increasing the activity of cyclic guanosine monophosphate (cGMP) [78, 79].
In the SOCRATES-REDUCED trial [80], vericiguat was proven to be well-tolerated
and safe in HFrEF during the 12 weeks of follow-up. The VICTORIA trial [81]
enrolled HFrEF patients with more severe heart failre than those in other
contemporary clinical trials, and found that even under guideline-directed
medical therapy (GDMT), vericiguat still reduced the composite primary outcome of
cardiovascular death or first HF hospitalization (P = 0.02) over a
median follow-up of 10.8 months. This result was mostly driven by reduced HF
hospitalization, with a statistically nonsignificant reduction in cardiovascular
death. A secondary analysis of the vericiguat trial showed that there were
time-dependent risks of events according to index hospitalization subgroups, in
which the worsening outpatient subgroup had the lowest risk compared to those at
HFrEF was characterized by decreased ejection fraction and cardiac contractility. Current available inotropic agents, including adrenergic receptor agonists (i.e., dobutamine), phosphodiesterase inhibitors (i.e., milrinone), and calcium sensitizer (i.e., levosimendan), effectively increased cardiac contractility. However, due to their specific mechanisms of action, these agents were associated with increased myocardial oxygen consumption, intracellular calcium, increased heart rate, hypotension, arrhythmias, and mortality [83, 84, 85].
OM was a selective, small-molecule cardiac myosin activator (also referred to as a cardiac myotrope) that binded to the catalytic domain of myosin and increased cardiac contractility without affecting cardiac myocyte intracellular calcium concentrations or myocardial oxygen consumption [86, 87]. Different from conventional inotropic agents, OM was a potential treatment for HFrEF patients due to its properties [88].
The recent large randomized controlled trial GALACTIC-HF was conducted to
demonstrate this hypothesis [89]. This trial enrolled HFrEF patients with EF
Many patients with heart failure have not received the optimal treatment due to clinicians’ insufficient awareness of the importance of drug combinations and excessive caution of adverse reactions it brings. Therefore, we proposed the diamond approach in this review to express the necessity of conjunction of therapies and exhibit possible combinations based on the latest clinical researches.
HF frequently have comorbidities such as hypotension, arrhythmias, and kidney disfunction. Considering that it may take months to prescribe all therapies recommended in the diamond approach, we believe the choice of optimal agents should vary along with different conditions and is worthy of attention. The following summarize the related studies and give some suggestions about personalized treatment in this regard.
Unless contraindicated or not tolerated, usage of the diamond approach in an early and comprehensive manner is crucial. In clinical practice, commonly step-up therapy of HF may reduce the benefit in patients with heart failure. Therefore, we combined the diamond approach and proposed a more aggressive treatment for HF (Fig. 2).
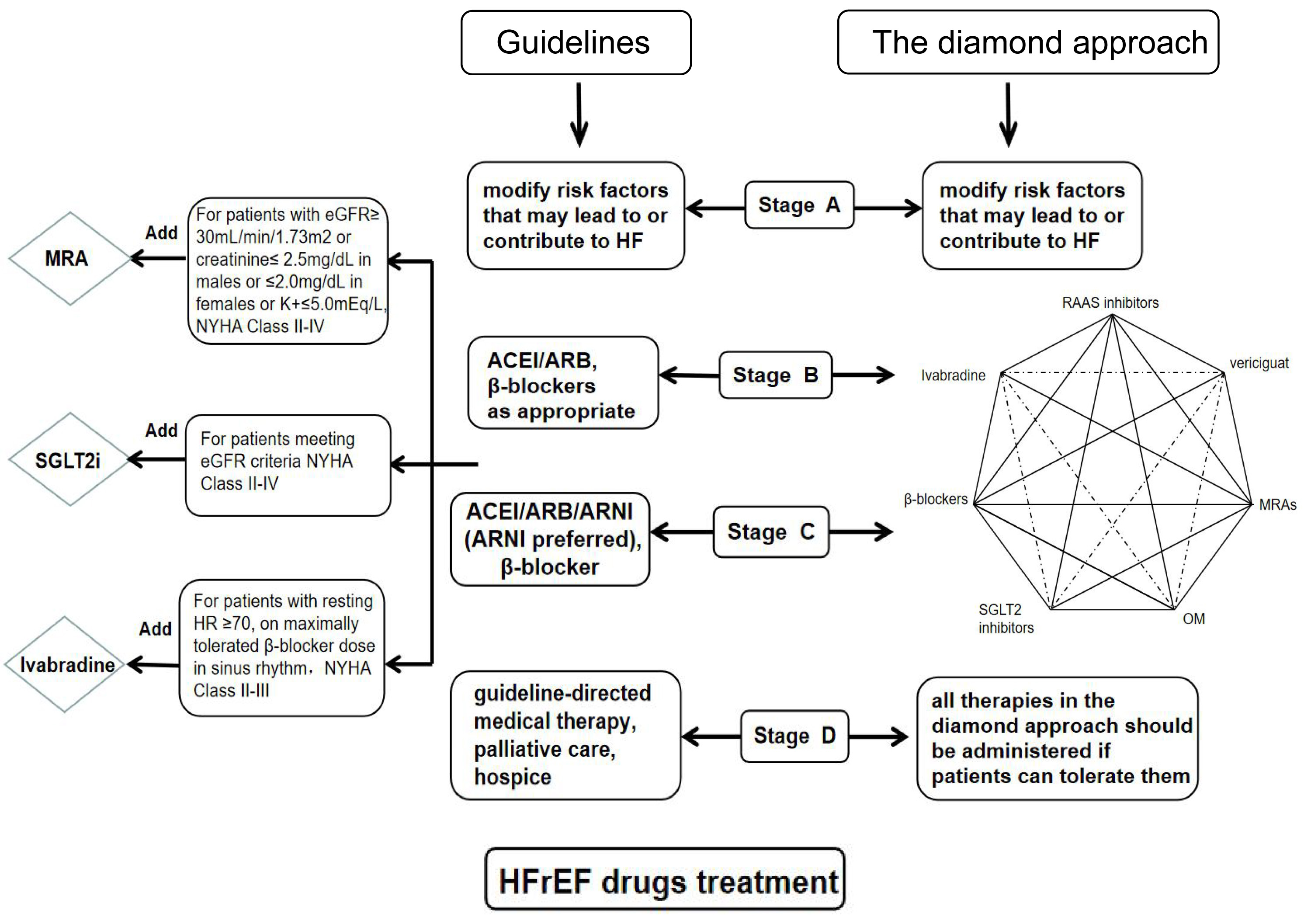 Fig. 2.
Fig. 2.Drug treatment algorithm for heart failure according to guidelines and diamond approach. Comparison of drug treatments between guidelines and the diamond approach in the four stages of heart failure. MRA, mineralocorticoid receptor antagonist; eGFR, estimated glomerular filtration rate; NYHA, New York Heart Association; SGLT2i, sodium-glucose cotransporter 2 inhibitor; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; ARNI, angiotensin receptor-neprilysin inhibitor; HFrEF, heart failure with reduced ejection fraction; HF, heart failure.
Patients with HF often had low BP. HF therapies such as ACEIs/ARBs, MRAs, and
The VICTORIA trial found that patients receiving vericiguat therapy had a higher
incidence of hypotension and syncope, which was related to the drug’s mechanism
[81]. The GALACTIC-HF trial excluded patients with low blood pressure (SBP
For patients with hypotension but lack of evidence of low perfusion, usage of these disease-modifying drugs should be considered. For these patients, it is necessary to titrate from a small dose and strictly monitor BP and heart rate. There are often improvements in heart function and hypotension for HFrEF patients after a period of treatment. When hypotension occurs, the most important action to be taken is reducing unnecessary vasodilators and diuretics and then adjusting the above medications.
Myocardial ischemia, infarction, and scar formation caused by coronary heart
disease were the most common causes of HF. A randomized controlled retrospective
(PARADISE-SWEDEHEART) study performed in Sweden found that the incidence of HF in
patients after MI was as high as 13–32%, and these HF patients were associated
with higher morbidity and rehospitalization. Early, comprehensive, and
standardized drug treatment largely determined the prognosis for these patients.
ACEIs [95, 96]/ARBs [28], MRAs [97], and
In the recent PARADISE-MI trial, it was found that when compared with an ACEI, ARNI reduced the primary endpoints (cardiovascular death, HF hospitalization, or outpatient development of HF) by 10% in patients with AMI, although statistical difference was not reached (P = 0.17). This study also observed that ARNI improved heart function more effectively because of its gradual action. Whether OM is benefical for AMI was not clear, since the GALACTIC-HF trial did not include relevant patients [89]. Because OM effectively increased cardiac contractility without increasing myocardial oxygen consumption and arrhythmia, it benefited patients after AMI. The specific effects of early use of ivabradine, SGLT2 inhibitors, and vericiguat on AMI remained unknown due to a lack of data.
CKD and HF often coexist, with CKD being present in 40–50% of chronic HF patients [101]. In addition to hemodynamic disturbances, the continuous activation of the SNS and RAAS also played a crucial role in CKD [102, 103]. The key to treatment lied in breaking the vicious cycle between the neuroendocrine system and hemodynamic disorder. ACEIs/ARBs [26, 104, 105, 106, 107]/ARNI [53, 108] and MRAs [32, 109] improved the prognosis of HFrEF with CKD. ARNI was a more optimal choice than ACEIs/ARBs for CKD because its superior cardiorenal effect has been proven. In the Kidney Disease Improving Global Outcomes (KDIGO) Controversies Conference, it was suggested that ARNI is an essential medicine for patients with HFrEF and CKD [110].
A meta-analysis including several randomized trials [111] found that
Out of consideration for renal insufficiency, disease-modifying drugs including ACE inhibitors, ARBs, ARNI, and MRAs are usually underused. Stopping these drugs or administering a low-dose of these drugs always leads to poor outcomes. Unless contraindicated or not tolerated, all patients with HFrEF and CKD should be routinely and comprehensively receiving these therapies, and drugs need to be titrated to the maximum dosage under strict monitoring.
Due to most clinical trials excluding patients with advanced CKD (eGFR
A study showed that ARNI increased the LVEF and was well tolerated in HFrEF with
ESRD on dialysis [119]. It was found that in the DAPA-CKD [120] trial,
dapagliflozin can delay the deterioration of renal function and reduce
cardiovascular death in patients with CKD (eGFR: 25–75 mL/min/1.73 m
Known as reversible non-ischemic dilated cardiomyopathy, AiCM was caused by tachycardias, atrial fibrillation (AF), and premature ventricular contractions. The elimination of arrhythmia was the optimal treatment for AiCM, and it reversed cardiomyopathy. Because AiCM often occured with HF, therapies for HF should also be considered for AiCM [121]. Thus far, guidelines only recommend HF treatments for tachycardia-induced cardiomyopathy (T-CM). We suggested that the same therapy should be used for atrial fibrillation-induced cardiomyopathy (AF-CM) and premature ventricular contraction-induced cardiomyopathy (PVC-CM), because these patients were very likely to benefit from these disease-modifying drugs.
There were double benefits from the use of
The two HF classification schemes that are widely used are the American College of Cardiology Foundation/American Heart Association (ACCF, West End, Washington, D.C., USA/AHA, Dallas, Texas, USA) staging system and the New York Heart Association (NYHA, Dallas, Texas, USA) functional classification. The stage system mentioned by ACCF/AHA considers the development and progression of HF, whereas the NYHA classes focused on exercise capacity and the severity of symptoms of HF. According to the different classifications, the treatments for HF were also dynamic and subject to change. Different from the current guidelines [16, 125, 126], we proposed a much more aggressive treatment for HF.
Stage A HF exhibited no structural heart disease or HF symptoms. However, due to combined risk factors, these patients are vulnerable to heart failure. Thus, we held the same point of view as the guidelines in terms of stage A treatment, that was, risk factors that may lead to or contribute to HF should be modified [15].
Stage B HF was characterized by asymptomatic cardiac dysfunction, and the
neuroendocrine system was activated at this stage [127]. It was previously
demonstrated that ACEIs [128] and
Patients in stage C have symptoms of heart failure based on structural heart
disease. In this stage, recommended therapies include ACEIs/ARBs/ARNI,
Stage D patients were associated with worsening heart function and often required inotrope or device therapy. However, therapies that improve prognosis should be considered if patients can tolerate them, or even tolerate only a small dose. Drugs should be initiated at very low doses, and patients should be closely monitored for signs or symptoms of intolerance. Vericiguat and OM may exert a satisfactory effect on these patients due to their mechanisms of action.
The continuous update of HF drugs enables the use of numerous effective targeted therapies for patients with HFrEF, and brings hopes to further improve the outcome of these patients. How to use these drugs to maximize the benefits in these patients is what clinicians must consider. Based on evidence-based clinical data, the diamond approach tries to give the suggestions on most appropriate drugs for individual HF patient. Furthermore, we believe the key of HF treatment is to effectively prevent deterioration of HF. The ‘diamond’ approach proposed in this review did not focus only on the derivation of individualized and optimized treatments, but also conveyed the perspective of aggressive treatment for HFrEF.
DAPA-CKD, Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney
Disease; DAPA-HF, Dapagliflozin and Prevention of Adverse Outcomes in Heart
Failure; DECLARE-TIMI 58, Dapagliflozin Effect on the Incidence of Cardiovascular
Events-Thrombolysis in Myocardial Infarction 58; EMPA-REG OUTCOME, Empagliflozin
Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients;
EMPEROR-REDUCED, Empagliflozin Outcome Trial in Patients With Chronic Heart
Failure with Reduced Ejection Fraction; EVALUATE-HF, Effects of
Sacubitril/Valsartan vs. Enalapril on Aortic Stiffness in Patients with Mild to
Moderate Heart Failure and Reduced Ejection Fraction; GALACTIC-HF, Global
Approach to Lowering Adverse Cardiac Outcomes Through Improving Contractility in
Heart Failure; PARADIGM-HF, Prospective Comparison of LCZ696 Compared to
Enalapril to Determine the Impact on Global Morbidity and Mortality in Heart
Failure; PARADISE-MI, Prospective ARNI vs ACE Inhibitor Trial to DetermIne
Superiority in Reducing Heart Failure Events After Myocardial Infarction;
PARADISE-SWEDEHEART, Trial with the use of a nationwide myocardial infarction
registry from Sweden (SWEDEHEART); PIONEER-HF, Comparison of Sacubitril/Valsartan
Versus Enalapril on Effect on NT-proBNP in Patients Stabilized From an Acute
Heart Failure Episode; PROVE-HF, Effects of Sacubitril/Valsartan Therapy on
Biomarkers, Symptom Improvement, and Ventricular Remodeling for Heart Failure;
SHIFT, Systolic Heart Failure Treatment with the I
HBG and HT wrote the manuscript with support from PP and ZZ. HBG, HT, YJH and DW revised the manuscript under PP and ZZ guidance. All authors read and approved the final manuscript.
Not applicable.
Not applicable.
Supported by the Science and Health Joint Medical Research Project of Chongqing (2018ZDXM010) (2020FYYX101) and the Fundamental Science and Advanced Technology Research of Chongqing (cstc2019jcyj-msxmX0433).
The authors declare no conflict of interest.