

1 Department of Pharmacy, the First Hospital of China Medical University, Shenyang 110001, P.R. China
2 School of Pharmacy, China Medical University, Shenyang 110001, P.R. China
3 Safety Evaluation Center, Shenyang Research Institute of Chemical Industry, Shenyang 110021, P.R. China
Abstract
A meta-analysis was performed to compare the antihypertensive efficacy of morning and evening dosing. Database of Pubmed, Embase, Cochrane, Web of Science CNKI, VIP, and Wanfang were searched up to December 2018. A total of 19 randomized control trials and 1215 participants were included in this meta-analysis. Administration time of amlodipine did not affect the office blood pressure (RR = -0.03, 95% CI -0.93-0.88, P = 0.96), daytime blood pressure (RR = -0.30, 95% CI -1.05-0.46, P = 0.44), 24 h mean blood pressure (RR = 1.15, 95% CI -0.39-2.70, P = 0.14), or heart rate (RR = 0.11, 95% CI -1.22-1.45, P = 0.87). Administration of amlodipine in the evening could significantly reduce the nighttime blood pressure (RR = 2.04, 95% CI 1.27-2.81, P < 0.00001), increased non-dipper alteration (RR = 0.51, 95% CI 0.41-0.63, P < 0.00001), and contained better anti-hypertension efficacy (RR = 0.64, 95% CI 0.550.74, P < 0.00001). For patients with hypertension, especially for non-dipper hypertension, taking amlodipine in the evening will be more beneficial. Better quality trials conducted in different regions and with larger sample size are necessary to verify the conclusion of this study.
Keywords
- Amlodipine
- blood pressure
- chronopharmacodynamics
- hypertension
- meta-analysis
With the development of social economy and aging population, chronic diseases have become a major public health issue affecting the health of residents in China and the World (Forouzanfar et al., 2017; Liu et al., 2014). Hypertension is one of the most common chronic diseases with high prevalence, and it is the most important risk factor for cardiovascular and cerebrovascular diseases (Laurent and Boutouyrie, 2007; Verwoer et al., 2014). According to hypertension guidelines, five classes of antihypertensive drugs that include angiotens in converting enzyme inhibitors (ACEI), angiotensin II receptor blockers (ARB), calcium-channel blockers (CCB), diuretics, and beta blockers are suggested for hypertensive therapy (Gabb et al., 2016).
Amlodipine, a third-generation dihydropyridine (DHP) calcium-channel blocker (CCB), is widely used for antihypertension. The mechanism of action for CCB is demonstrated by blocking the extracellular calcium influx through the voltage-dependent L-type calcium channels, which result in the decrease in the intracellular concentration of calcium in vascular smooth muscles cells (VSMCs). This calcium exchange directly causes vasodilation and anti-hypertensive effects (Mason et al., 2003).
Normal blood pressure fluctuates regularly within 24 hours with peaks from 6 am to 9 am and from 4 pm to 6 pm, and then gradually dropping to the lowest point from 2 am to 3 am. The purpose of hypertension treatment is to control the blood pressure and avoid excessive fluctuations to reduce cardiovascular and cerebrovascular accidents.
Amlodipine is a long-acting CCB that controls blood pressure. Administration of the drug once-a-day can better control blood pressure within 24 hours. However, when is the most appropriate time to take the medication? What are the differences in efficacy at different times? In this study, a meta-analysis was performed to compare the anti-hypertensive efficacy of morning and evening dosing in order to better understand this issue.
The following databases were used from inception to December 2018: Pubmed, Embase, Web of Science and Chinese Academic Journal from CNKI, VIP, and Wanfang. The following search terms (“amlodipine” or “Norvasc”) and (“blood pressure” or “Hypertension”) and (“morning” or “evening” or “chronopharmacology” or “chronotherapy”) were used in the search strategy. No language restrictions were excluded during the search process.
Studies were included if they were randomized control trials (RCTs), participants met the diagnostic criteria for hypertension, or when sufficient data and outcome indicators could be extracted. Subjects complicated with cardiac failure or cerebral infarctions were excluded from our studies.
Two authors extracted data and assessed the study quality independently. In this study, the modified Jadad scale was used to evaluate the RCTs, which awards four to seven stars as high quality. The literature information such as author, publication year, study design, sample size, treatment of amlodipine, and outcome indicator of office blood pressure (office BP), daytime blood pressure, nighttime blood pressure, 24 h mean blood pressure, heart rate (HR) and non-dipper alteration were all collected.
Review Manager (RevMan 5.3, Cochrane Center) was used for statistical analysis. Heterogeneity analysis across trials was initially assessed by Chi-square test: when P > 0.05 or I2 < 50% fixed-effects model was selected; when P < 0.05 or I2 > 50% random-effects model was selected. Relative risk (RR) and 95% confidence interval (95% CI) were chosen as the analysis statistic for dichotomous data, and the mean differences (MD) and 95% CI were chosen as the analysis statistic for continuous data.
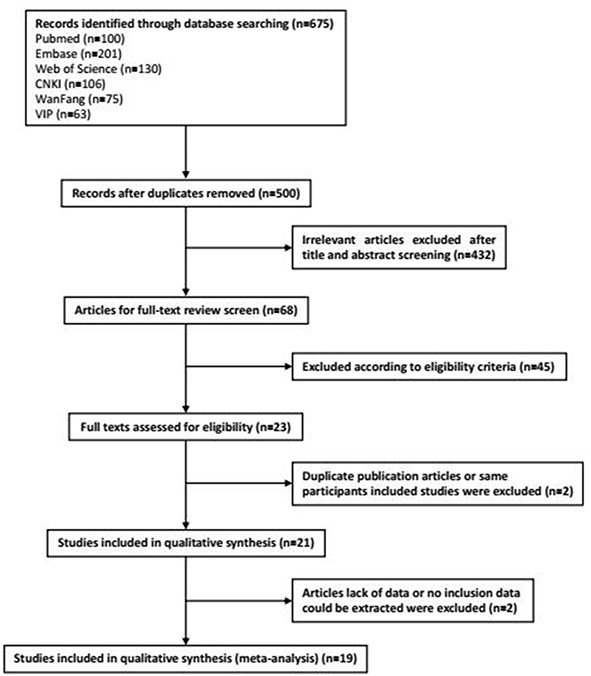
The study flow diagram was shown in Fig. 1, totally of 25 RCT studies (India (1), Switzerland (1), Germany (1), and China (19)) and 1481 participants were included in the meta-analysis. The characteristics of these studies were listed in Table 1.
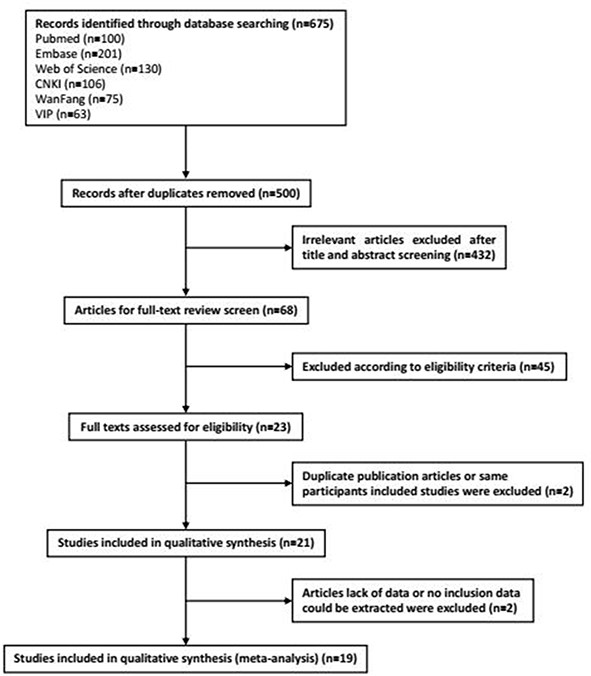 Figure 1.
Figure 1.Flow diagram of the study.
| Study | Region | Study design | Participants | Sample size | Outcomes |
|---|---|---|---|---|---|
| Chen and Huang (2012) | China | RCT | Class I essential hypertension | 61 | 3-8 |
| Chen (2013) | China | RCT | Class I and II essential hypertension | 80 | 7-8 |
| Feng (2013) | China | RCT | non-dipper essential hypertension (elder) | 68 | 1-2, 7-8, 10-11 |
| Hou (2016) | China | RCT | non-dipper hypertension (elder) | 100 | 7-8, 11 |
| Khodadoustan et al. (2017) | India | RCT | primary hypertension | 6 | 7-9, |
| Li et al. (2011) | China | RCT | non-dipper hypertension | 38 | 3-6, |
| Lin and Wu (2016) | China | RCT | non-dipper hypertension (elder) | 94 | 7-8, 11 |
| Mengden et al. (1993) | Switzerland | RCT | mild-to-moderate essential hypertension | 20 | 1-6, 9 |
| Nold et al. (1998) | Germany | RCT | mild-to-moderate essential hypertension | 12 | 3-9 |
| Qiu et al. (2000) | China | RCT | mild-to-moderate hypertension | 32 | 1-9 |
| Qiu et al. (2003) | China | RCT | mild-to-moderate essential hypertension | 62 | 1-9 |
| Ren (2013) | China | RCT | non-dipper Class II essential hypertension | 48 | 3-8, 10 |
| Sun et al. (2007) | China | RCT | non-dipper essential hypertension (elder) | 54 | 1, 5, 10-11 |
| Tang et al. (2014) | China | RCT | essential systolic hypertension | 160 | 1, 3, 5, 7, 11 |
| Wang (2013) | China | RCT | non-dipper essential hypertension (elder) | 90 | 3-8, 10 |
| Xiao et al. (2009) | China | RCT | essential systolic hypertension | 86 | 1, 7, 11 |
| Yan (2014) | China | RCT | non-dipper essential hypertension (elder) | 62 | 1-2, 5-8 |
| Zhang et al. (2012) | China | RCT | non-dipper essential hypertension (elder) | 58 | 1-2, 5-8, 10 |
| Zhou and Li (2012) | China | RCT | non-dipper essential hypertension (elder) | 84 | 3-8, 10 |
Outcomes: 1- office SBP; 2- office DBP; 3- dSBP; 4- dDBP; 5-nSBP; 6-nDBP; 7-24 hSBP; 8-24 hDBP; 9-heart rate; 10-non-dipper alteration; 11-anti-hypertension efficacy
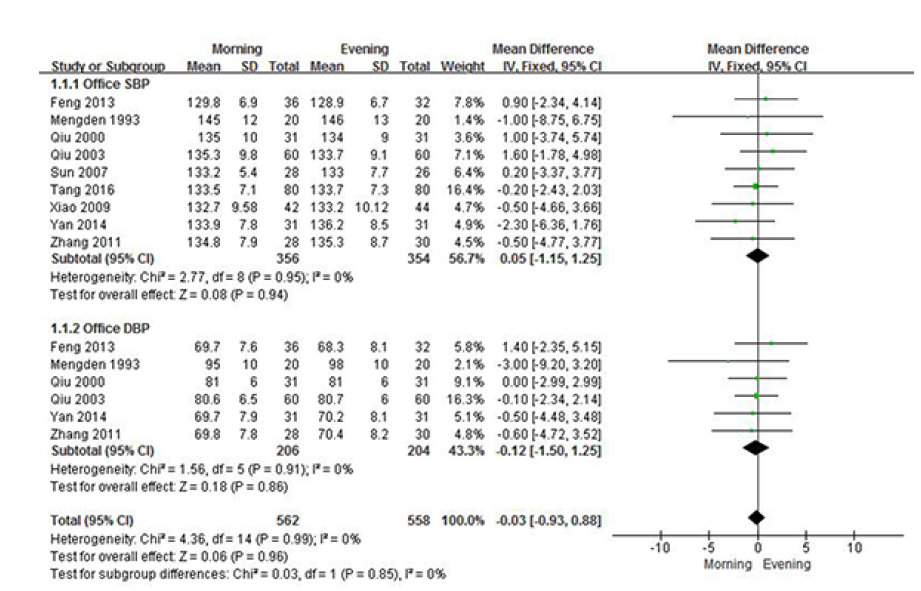
3.2.1 Office BP
As shown in Fig. 2, the changes of office SBP (RR = 0.05, 95% CI -1.15-1.25, P = 0.94) and DBP (RR = -0.12, 95% CI -1.501.25, P = 0.86) were similar between the two groups of that taking amlodipine in the morning or in the evening.
 Figure 2.
Figure 2.Comparison changes of office BP after taking amlodipine in the morning or in the evening.
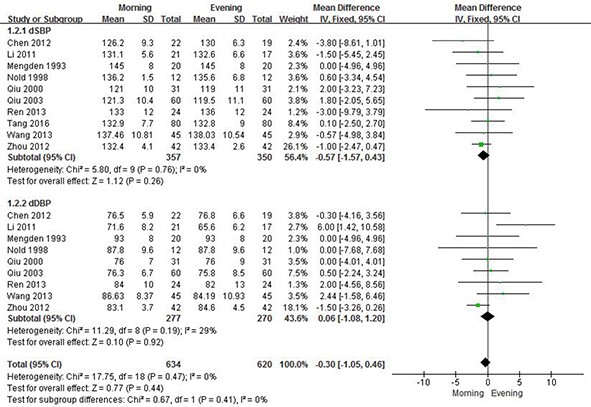
3.2.2 Daytime BP
Fig. 3 shows the changes of daytime BP after taking amlodipine in the morning or evening. There were no significant differences found to dSBP (RR = -0.57, 95% CI -1.57-0.43, P = 0.26) and dDBP (RR = 0.06, 95% CI -1.08-1.20, P = 0.92).
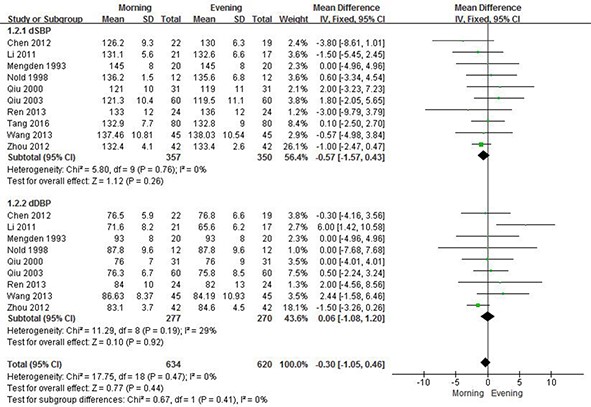 Figure 3.
Figure 3.Comparison changes of daytime-BP after taking amlodipine in the morning or in the evening.
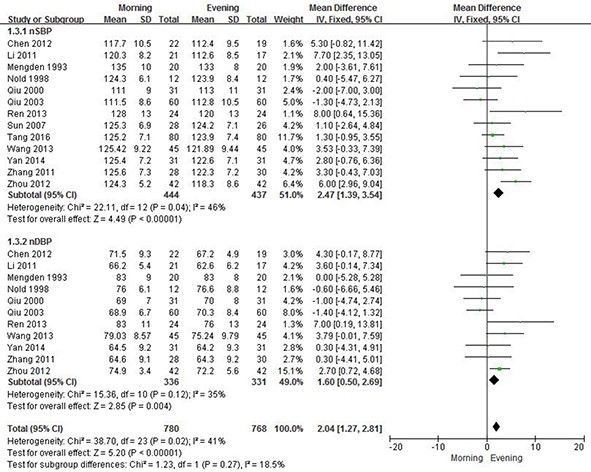
3.2.3 Nighttime BP
Compared to the group of dosage in the morning, amlodipine administration in the evening could significantly reduce the nSBP (RR = 2.47, 95% CI 1.39-3.54, P < 0.00001) and nDBP (RR = 1.60, 95% CI 0.50-2.69, P = 0.004) (see Fig. 4).
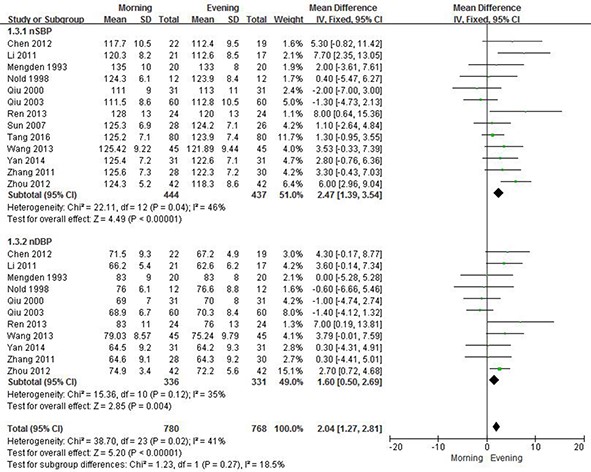 Figure 4.
Figure 4.Comparison changes of nighttime BP after taking amlodipine in the morning or in the evening.
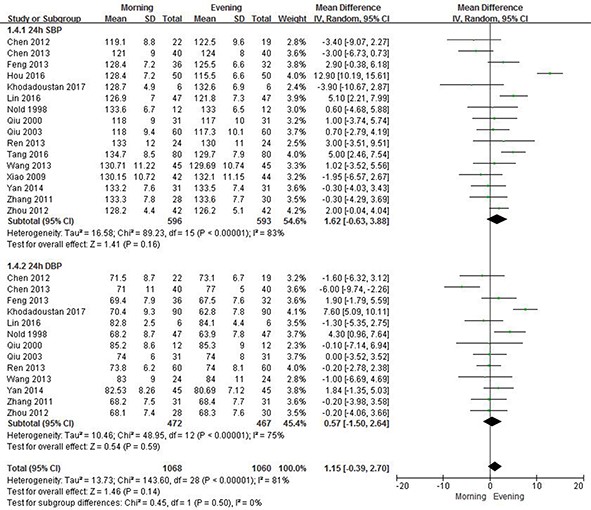
3.2.4 24 hBP
As shown in Fig. 5, the 24 h SBP (RR = 1.62, 95% CI -0.63-3.88, P = 0.16) and 24 h DBP (RR = 0.57, 95% CI -1.50-2.64, P = 0.59) of the evening group were both lower compared to the morning group, but not statistically different between the two groups.
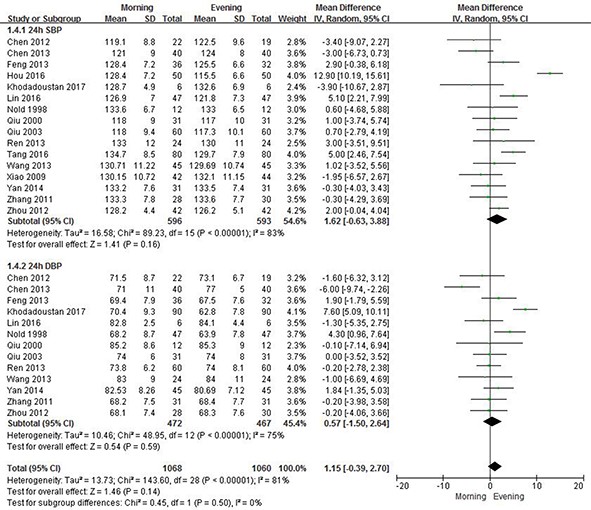 Figure 5.
Figure 5.Comparison changes of 24 h BP after taking amlodipine in the morning or in the evening.
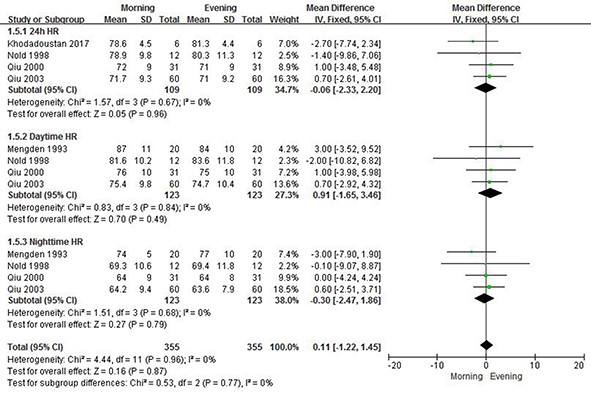
3.2.5 Heart rate
Fig.6 shows the changes of heart rate after taking amlodipine in the morning or in the evening. There were no statistical differences of 24 h HR (RR = -0.06, 95% CI -2.33-2.20, P = 0.96), daytime HR (RR = 0.91, 95% CI -1.65-3.46, P = 0.49) and nighttime HR (RR = -0.30, 95% CI -2.47-1.86, P = 0.79) between the two groups.
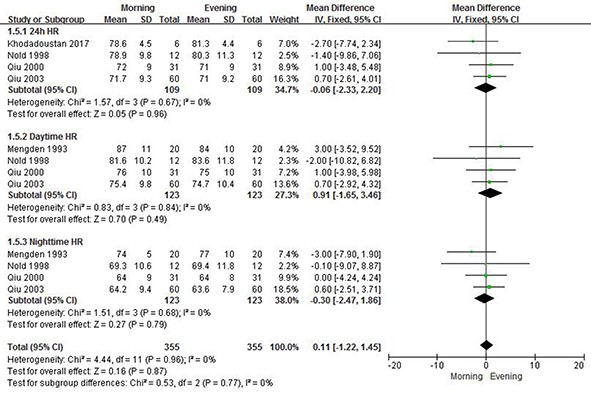 Figure 6.
Figure 6.Comparison changes of heart rate after taking amlodipine in the morning or in the evening.
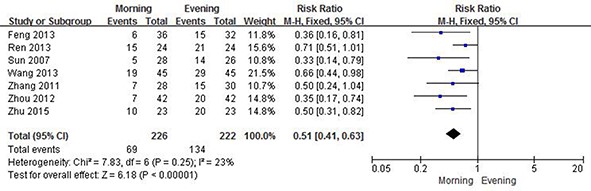
3.2.6 Non-dipper alteration
Several studies reported the non-dipper alteration (Feng, 2013; Ren, 2013; Sun et al., 2007; Wang, 2013; Zhang et al., 2012; Zhou and Li, 2012; Zhu, 2015). As shown in Fig. 7, the non-dipper hypertension was significantly improved and transformed to dipper hypertension after taking amlodipine in evening compared to the morning (RR = 0.51, 95% CI 0.41-0.63, P < 0.00001).
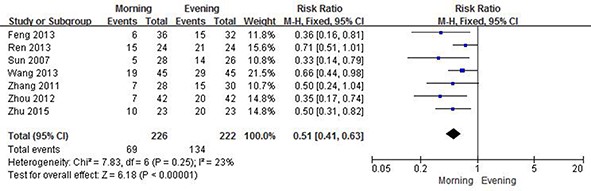 Figure 7.
Figure 7.Comparison non-dipper alteration after taking amlodipine in the morning or in the evening.
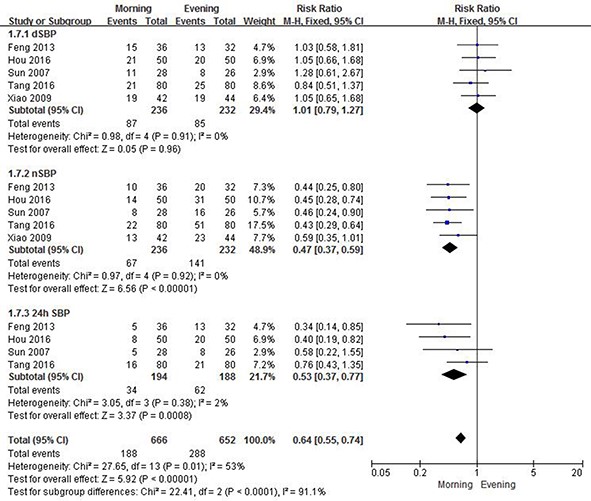
3.2.7 Anti-hypertension efficacy
As shown in Fig. 8, no difference for dSBP was observed between the morning and evening groups (RR = 1.01, 95% CI 0.791.27, P = 0.96), but the evening dosage group had better efficacy of nSBP (RR = 0.47, 95% CI 0.37-0.59, P < 0.00001) and 24 h SBP (RR = 0.53, 95% CI 0.37-0.77, P = 0.0008).
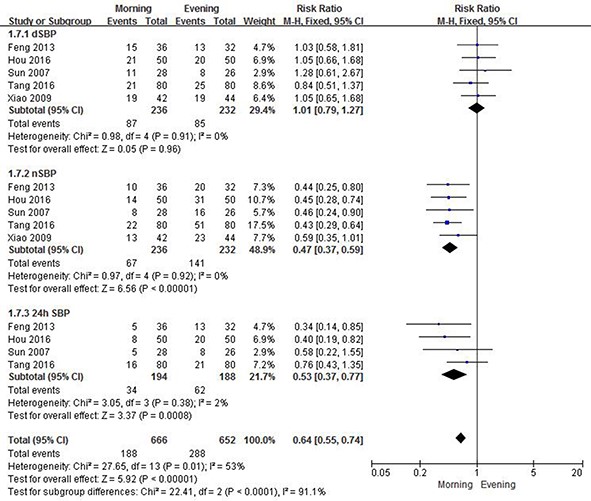 Figure 8.
Figure 8.Comparison anti-hypertensive efficient after taking amlodipine in the morning or in the evening.
Amlodipine, as a long-acting third-generation dihydropyridine calcium antagonist, selectively inhibits the trans-membrane influx of calcium ions into the cardiac muscle and vascular smooth muscle (Mason et al., 2003). Amlodipine is a peripheral arterial vasodilator that acts directly on vascular smooth muscle to reduce the resistance of the peripheral vascular system (Bol et al., 2012). Amlodipine is mainly used for the treatment of hypertension and found to further reduce the risk of fatal and nonfatal cardiovascular events, primarily strokes and myocardial infarctions. It is an irreplaceable drug used worldwide in elder hypertension, hypertension with diabetes, coronary heart disease, and angina (Ruzyllo et al., 2007; Sahney, 2006).
This study systematically evaluated and compared the antihypertensive effects of amlodipine administered at various times by meta-analysis. We demonstrated that administration time did not affect the office blood pressure, daytime blood pressure, 24h mean blood pressure, or heart rate. Amlodipine could significantly reduce the nighttime blood pressure, recover the rhythm of blood pressure at night, and have better antihypertensive efficacy, especially for nighttime systolic and 24 h mean systolic blood pressures.
Due to BP fluctuation, dipper hypertension is defined as nocturnal BP decline with a normal fall > 10%, and non-dipper hypertension is defined as a circadian rhythm over 24 h with abnormal fall < 10% at night with organ damage (heart, brain and kidney), high risk of cardiovascular and cerebrovascular diseases, and adverse outcomes (Chen et al., 2018; Kario et al., 2001; Kurpesa et al., 2002; Zhu, 2015). Staessen et al. reported both the blood pressure decrease and ratio that showed a curvilinear correlation with age and the smallest decrease and largest ratio were observed in older (≥ 70 years) subjects (Staessen et al., 1997). According to this study, administration of amlodipine in the evening could significantly increase the conversion from non-dipper to dipper hypertension (P < 0.00001) that are more beneficial for elder patients.
Studies done by Hu et al. and Ji et al. compared the left ventricular diastolic function of administration time to hypertension complicated with heart failure (Hu et al., 2012; Ji et al., 2017). Results showed that taking amlodipine in the evening could significantly increase the left ventricle diastolic early peak, diastolic velocity, and reduce early diastolic filling period achieving better antihypertensive effect. Both studies found that administration of amlodipine in the evening could better control nighttime blood pressure, transform non-dipper hypertension to normal pressure rhythm, and contain remarkable clinical effects with minimal damage to the left ventricle. Amlodipine could effectively protect the target organs and reduce the incidence of cardiovascular events, especially in the treatment of hypertension complicated with cardiac failure. Other studies have also reported that long-term treatment with amlodipine could effectively reduce left ventricular mass and improve left ventricular diastolic function in patients with hypertension (Bălan, 2009; Motoki et al., 2014).
The aim of this study was to compare the anti-hypertensive efficacy of amlodipine dosing during morning versus evening. In order to investigate the anti-hypertensive efficacy of monotherapy, the combination of amlodipine and other anti-hypertensive drugs were not included. The aim of this study to investigate the antihypertensive efficacy of mono-therapy of amlodipine, the combination of amlodipine and other anti-hypertensive drugs were not included in our study. Thus there are a couple of limitations that should be considered from this study. First, there were certain regional limitations in the results since most trials were conducted in China (16 of 19 studies). Second, the sample sizes of the included RCT trials were relatively small. Better quality trials conducted in different regions and with larger sample size are necessary to verify the conclusion of this study.
Administration of amlodipine in the evening could effectively reduce nighttime blood pressure, offer more non-dipper alteration, and better address antihypertensive efficacy. This meta-analysis indicates beneficial effects of amlodipine dosage in the evening for patients with hypertension, especially for non-dipper hypertensives. Considering the limitations of this study, more high quality trials should be conducted in different regions of the world and with larger sample sizes to verify the conclusion of this study.
This project was supported by the China Medical Hand in Hand Engineering Committee and Beijing Medical Award Foundation (Grant No.: YXJL-2018-0616-0060). I would like to express my gratitude to all those who helped me during the writing of this manuscript. Thanks to all the peer reviewers and editors for their opinions and suggestions.
The authors report no declarations of interest.