

 , Yuli Shuai 1,2, Yiwei Liu 1,2, Sibei Liu 1,2, Xinyu Tang 1,2, Wei Tian 1,2, Yujia Zhang 1,2, Yuhan Kong 1,2,*
, Yuli Shuai 1,2, Yiwei Liu 1,2, Sibei Liu 1,2, Xinyu Tang 1,2, Wei Tian 1,2, Yujia Zhang 1,2, Yuhan Kong 1,2,*
1 Department of Rehabilitation Medicine, The First Affiliated Hospital of Chongqing Medical University, 400016 Chongqing, China
2 Key Laboratory of Physical Medicine and Precision Rehabilitation of Chongqing Municipal Health Commission, The First Affiliated Hospital of Chongqing Medical University, 400016 Chongqing, China
Abstract
Neurological disorders are a leading cause of disability worldwide. Transcranial direct current stimulation (tDCS) is a promising therapeutic tool for neurological disorders. However, a consensus on clinical recommendations for using tDCS in patients with neurological disorders is lacking. In this umbrella review, we aimed to establish evidence-based guidance for using tDCS to treat neurological disorders.
This study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 2020. PubMed/MEDLINE, Embase, the Cochrane Library, the Web of Science, and the Cumulative Index to Nursing and Allied Health Literature (CINAHL) were systematically searched to identify and evaluate existing systematic reviews and meta-analyses on the use of tDCS for neurological disorders. Quality was assessed using the Measurement Tool to Assess Systematic Reviews 2 (AMSTAR 2) and the Grades of Recommendations, Assessment, Development, and Evaluation (GRADE) tool. The Hartung-Knapp-Sidik-Jonkman random effects model was employed for reanalysis.
A total of 17 systematic reviews and meta-analyses encompassing 358 randomized controlled trials and 7160 participants were analyzed. tDCS demonstrated efficacy across seven distinct health conditions, including stroke, Parkinson’s disease, Alzheimer’s disease, cerebellar ataxia, fibromyalgia, disorders of consciousness, and migraine. Adverse effects were rarely reported, with the exception of mood changes associated with fibromyalgia. Our results indicated that tDCS significantly improved 34 distinct health outcomes related to these conditions.
We found that tDCS may be a promising treatment for neurological disorders, with mild and infrequent adverse effects. Further studies are warranted to validate the therapeutic potential of tDCS in the reported neurological conditions, investigate additional neurological health outcomes, and explore the underlying mechanisms of tDCS effects.
CRD42024589432, https://www.crd.york.ac.uk/PROSPERO/view/CRD42024589432.
Keywords
- transcranial direct current stimulation
- tDCS
- neurological disorders
- efficacy
- adverse effect
- umbrella review
Neurological disorders are an important cause of disability and death worldwide, including cerebrovascular and neurodegenerative diseases, neurological-immunological disorders, neuromuscular or peripheral nervous system disorders, traumatic injuries, and a broad range of other neurological disorders [1]. Neurological disorders and the dysfunctions associated with them impose an overwhelming burden on patients. For example, stroke accounts for the largest proportion of disability-adjusted life-years (47.3%) among all nervous system conditions [2]. Approximately 80% of patients develop motor function, 29–81% of individuals in the acute phase experience post-stroke dysphagia [3], 30–50% develop varying degrees of cognitive deficits [4], and 18–33% of individuals experience post-stroke depression [5]. What cannot be disregarded is that the incidence rates of Parkinson’s disease and Alzheimer’s disease are increasing. Based on the Global Burden of Disease (GBD) 2021, over 11.77 million people worldwide have Parkinson’s disease [6]. By 2050, 25.2 million people are projected to be living with Parkinson’s disease worldwide, representing a 112% increase from 2021 [7]. Meanwhile, 7.75 million individuals are thought to experience dementia, and the population is predicted to increase significantly, reaching 152.80 million by 2050 [8, 9]. Disability from these two degenerative diseases increases with time. Motor symptoms, such as bradykinesia, stiffness, postural instability, and tremors, are prominent in Parkinson’s disease, whereas Alzheimer’s disease impacts older adults’ cognitive and memory abilities. Neurorehabilitation is a key component of regaining neurological function. The most crucial aspect is that neurorehabilitation begins following the diagnosis and continues throughout any further treatment procedures [10]. Although neurorehabilitation is actively pursued, treatment effectiveness varies considerably. Effective and safe neurorehabilitation techniques are desperately needed due to the major impact of the dysfunction associated with these conditions on patients’ daily lives and their social reintegration.
Over the past 20 years, transcranial direct current stimulation (tDCS) has emerged as a promising therapeutic tool for neurorehabilitation. As a non-invasive brain stimulation technique, it is characterized by effectiveness, safety, and cost-effectiveness [11]. In tDCS, mild electrical currents (usually 1 to 2 mA) are applied through scalp electrodes. The process enables polarity-dependent cortical excitability control [12], induces neuroplasticity [13], and activates brain network regions and so on [14, 15]. tDCS has prompted extensive research in various neurological conditions, yet a comprehensive review focusing on the effectiveness and safety of tDCS in neurological disorders is lacking. Currently, the use of tDCS in neurological diseases is controversial. First, its therapeutic efficacy and safety have not been consistently reported. Second, previous studies are highly heterogeneous and use relatively few outcome indicators.
We conducted an umbrella review incorporating the latest studies in neurological health-related studies to enhance evidence-based clinical decision-making about tDCS. The main objective was to verify tDCS’s efficacy and safety by a thorough analysis of neurological disorders. Heterogeneity practices and risk of bias were evaluated as secondary objectives.
This umbrella review aimed to systematically analyze systematic reviews and meta-analyses of randomized controlled trials (RCTs) investigating the effect of tDCS on neurological health outcomes. This study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 2020 for overviews of reviews of healthcare interventions [16] and was registered in the Prospective Register of Systematic Reviews (PROSPERO) (CRD42024589432) [17]. The PRISMA 2020 checklist for overviews of reviews of healthcare interventions is shown in Supplementary Material-A. Two authors, Tianfeng Ye and Yuli Shuai, independently and methodically searched PubMed/MEDLINE (https://pubmed.ncbi.nlm.nih.gov/), Embase (https://www.embase.com), the Cochrane Library (https://www.cochranelibrary.com/), the Web of Science (https://www.webofscience.com), and Cumulative Index to Nursing and Allied Health Literature (CINAHL, https://www.ebsco.com/products/research-databases/cinahl-database) from each database’s inception until October 16, 2024, and extracted data into a spreadsheet. The following search terms and their variations were used: “meta-analysis” OR “systematic review” AND “tDCS” OR “transcranial direct current stimulation” OR “HD-tDCS” OR “high-definition transcranial direct current stimulation” (Supplemental Material-B).
Participants: All participants were diagnosed with neurological disorders using standard diagnostic criteria. Interventions: Only tDCS was applied. Control: Any comparator could serve as the control, including sham stimulation, other active interventions, medicines, and treatment as usual. Outcomes: Neurological health outcomes. Study types: Systematic reviews and meta-analyses with adequate data (mean, standard deviation, and sample size) were included, which was essential to the Hartung-Knapp-Sidik-Jonkman (HKSJ) estimation.
The exclusion criteria included (1) patients with no neurological disorders, (2) interventions other than tDCS, and (3) neither safety nor efficacy data to extract.
Two researchers screened the titles, abstracts, and full texts independently. Any disagreements in the selection of papers between the two researchers were resolved by a third researcher (Yiwei Liu). When two or more original papers probed the same effect, only the latest published or more robust evidence-based paper was chosen [18, 19].
The data were extracted from all the studies, including health outcomes, the first author, publication year, type, tDCS parameters (electrode location, intensity, duration, and session), the number of participants, the number of included RCTs, effect measures, the model used for effect estimation (random or fixed effects), effect sizes, and 95% confidence intervals (95% CIs).
Neurological health outcomes were operationally defined as any quantifiable measure of signs, symptoms, functional status, or quality of life that directly results from dysfunction of the nervous system or constitutes a core clinical manifestation of the neurological disorders. Outcome domains were conceptualized based on the World Health Organization’s International Classification of Functioning, Disability and Health (ICF) framework to ensure a systematic approach, encompassing body structures, body functions, activities and participation, and environmental factors [18]. Outcomes, such as pain from fibromyalgia or migraine and depression in post-stroke patients, were included only when they were explicitly recognized as core symptoms of the neurological disorder. A specific list of all searched outcomes is provided in the Supplementary Material-C.
The two authors also independently performed methodological quality and evidence assessments to ensure accuracy.
Methodological quality was assessed in each study using the Measurement Tool to Assess Systematic Reviews 2 (AMSTAR 2) [20]. Seven of the 16 items in AMSTAR 2 were critical. The crucial items were items 2, 4, 7, 9, 11, 13 and 15. Four ratings were assigned to the methodological quality assessments: high, moderate, low, and critically low.
The quality of evidence for each study included in this umbrella review was evaluated using the Grades of Recommendations, Assessment, Development, and Evaluation (GRADE) [21]. The GRADE system encompasses five domains for downgrading and three domains for upgrading the quality of evidence. The downgrading domains comprise (1) risk of bias, (2) inconsistency, (3) indirectness, (4) imprecision, and (5) publication bias. The upgrading domains include (1) large effect, (2) plausible confounding, and (3) a dose-response gradient. Based on these criteria, the quality of evidence was classified into four levels: high, moderate, low, and very low.
Detailed rationales for each AMSTAR 2 and GRADE rating per health outcome are provided in a Supplementary Material-D.
The effect sizes expressed as mean difference (MD) or standardized mean
difference (SMD) with associated 95% CI were recalculated independently using
the DerSimonian and Laird fixed- or random-effects model [22]. This initial step
was taken to maintain consistency with the methods commonly reported in the
original publications, thereby facilitating direct comparisons. Subsequently, we
prespecified the HKSJ random-effects model as the primary reanalysis for all
outcomes to provide more robust estimates, particularly in the context of small
study samples and substantial heterogeneity. The HKSJ method is recognized for
providing more conservative and reliable confidence intervals when the number of
included studies is small (e.g.,
Small sample studies tend to overestimate the effects of tDCS compared to larger
ones. Our primary assessment consisted of the visual inspection of funnel plots
for asymmetry. For meta-analyses that included a sufficient number of studies (at
least 10 RCTs), we additionally employed Egger’s linear regression test to
statistically evaluate funnel plot asymmetry [28]. This threshold was set because
Egger’s test is known to be underpowered and unreliable in syntheses with a
smaller number of studies (k
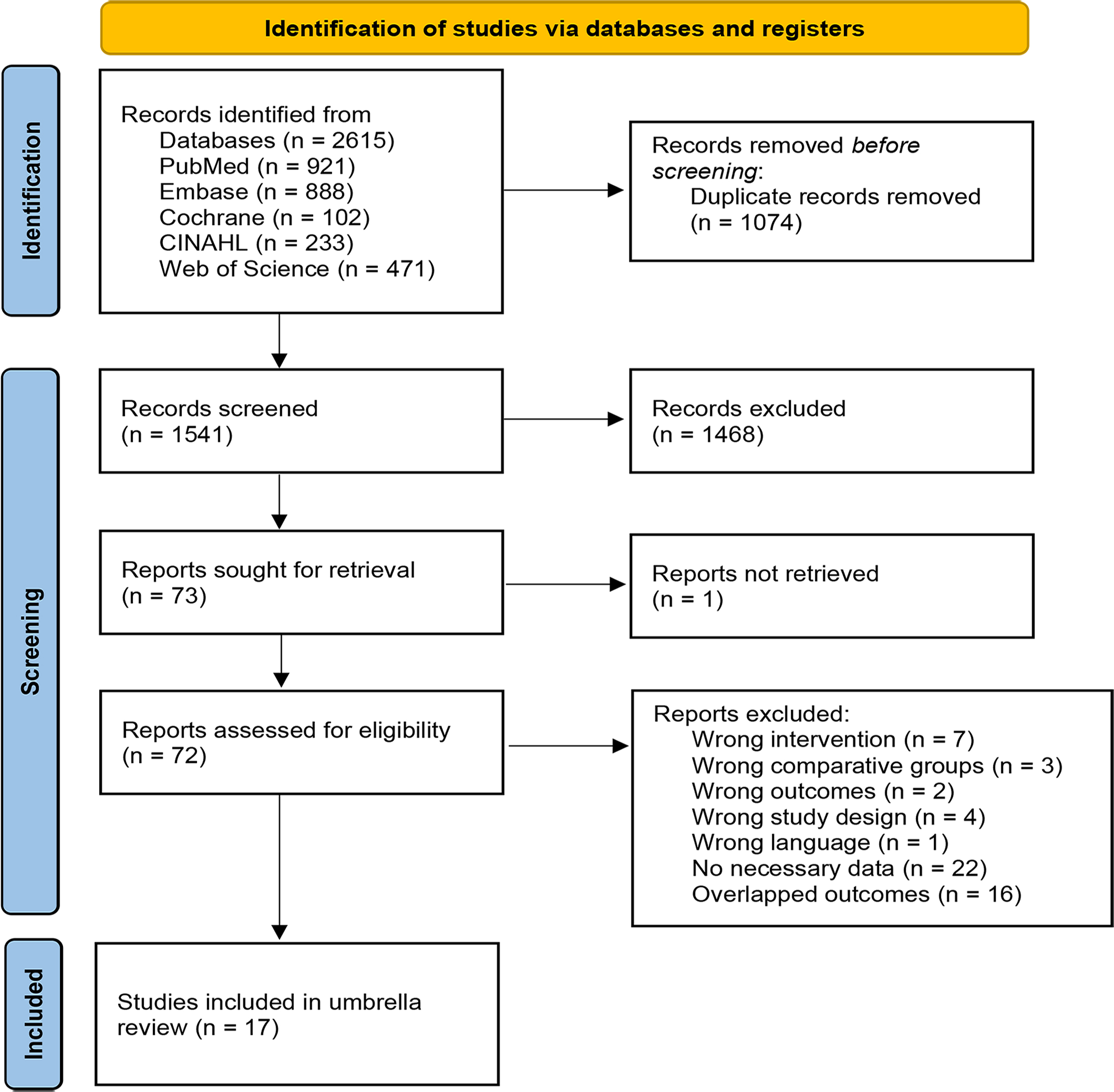
The study selection process is illustrated in Fig. 1. A total of 2615 references were retrieved through the database search. After removing 1074 duplicates, 1468 articles were excluded based on title and abstract screening. Then, full-text reviews excluded 55 articles, and finally, 17 eligible publications were identified [30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46].
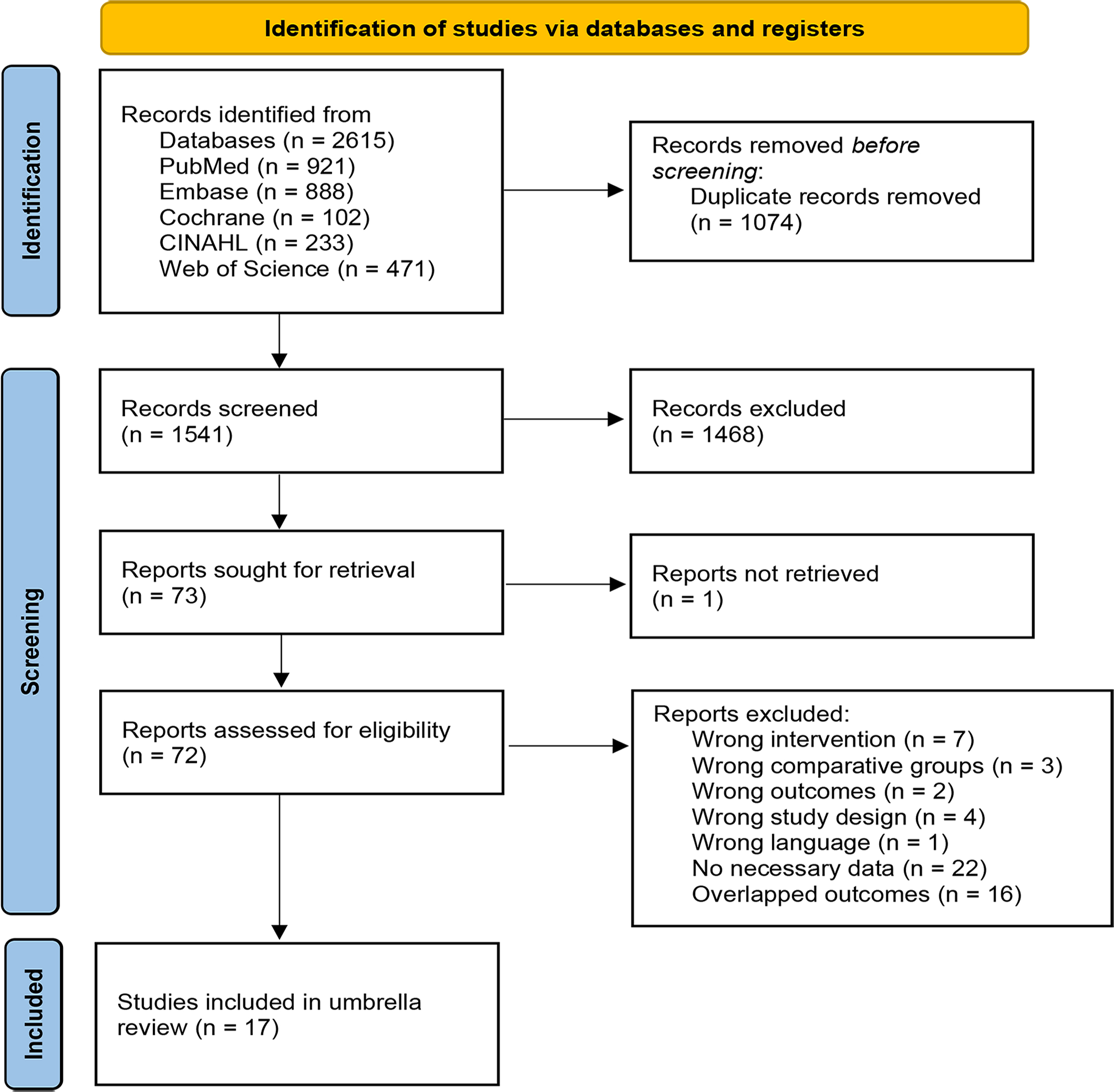 Fig. 1.
Fig. 1.
PRISMA 2020 flow diagram. PRISMA, preferred reporting items for systematic reviews and meta-analyses.
Details regarding patient demographics and tDCS protocols in the included studies are summarized in Table 1 (Ref. [30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46]). Most studies had sample sizes below 800, which were considered small sample studies. The majority of the systematic reviews and meta-analyses included fewer than 10 RCTs, limiting the application of Egger’s test for publication bias. Parameters, such as polarity of the protocol, active electrode placement and the number of sessions, varied according to the disease being studied. However, the intensity and duration of tDCS predominantly ranged from 1–2 mA and 10–20 minutes, respectively. Furthermore, many included studies did not provide information on a stimulation site or a follow-up period, negatively impacting the AMSTAR 2 quality rating.
| Health outcomes | First author/year | Population | Session | Electrode location | Intensity/Duration | Sample | |
| Stroke | |||||||
| Score of MoCA | Lyu 2023 [30] | PSCI | 10–40 | DLPFC, frontal and temporal different brain regions | 1.1–2.0 mA | 403 | |
| 20–30 min | |||||||
| Score of MMSE | Lyu 2023 [30] | PSCI | 15–40 | DLPFC, frontal and temporal different brain regions | 1.1–2.0 mA | 290 | |
| 20–30 min | |||||||
| Score of LOTCA | Lyu 2023 [30] | PSCI | 30 | DLPFC, frontal and temporal different brain regions | 0.5 mA, 1.2 mA | 34 | |
| 20 min | |||||||
| Score of MBI | Lyu 2023 [30] | PSCI | 10–40 | DLPFC,frontal and temporal different brain regions | 1.2–2.0 mA | 264 | |
| 20, 30 min | |||||||
| P300 latency | Lyu 2023 [30] | PSCI | 20, 24 | DLPFC, frontal and temporal different brain regions | 1.2 mA, 2.0 mA | 72 | |
| 20 min | |||||||
| PSD scale score (HAMD/BDI/SADQ-H/SDS) | Li 2022 [31] | PSD | 10–20 | L-DLPFC, M1 of lesioned side | 1.0–2.0 mA | 206 | |
| 20, 30 min | |||||||
| Upper extremity motor function (FMA-UE/ARRT) | Tang 2024 [32] | Stroke | 5–60 | C3, C4, M1, F3, 2.5 cm anterior to M1, right cerebellum | 0.5–3.0 mA | 807 | |
| 9–40 min | |||||||
| Score of BI | Tang 2024 [32] | Stroke | 10–60 | C3, C4, M1, F3 | 1.0–2.0 mA | 283 | |
| 10–30 min | |||||||
| Change of FMA-UE score | Chow 2022 [33] | Stroke | 1–36 | Ipsilesional M1 and supraorbital region, paretic M1, contralesional supraorbital region | 1.2–3.0 mA | 802 | |
| 10–40 min | |||||||
| Lower extremity motor assessment (FMA-LE) | Chow 2022 [33] | Stroke | 10–24 | Ipsilesional M1, precentral gyrus and leg area | 1.5–3.0 mA | 179 | |
| 10–30 min | |||||||
| Spasticity (MAS) | Huang 2022 [34] | Stroke | 6–40 | Anodal: M1, dual stimulation | Anodal: 0.7–2.0 mA | 458 | |
| Cathodal: non-lesioned primary sensorimotor cortex | Cathodal: 0.5–2.0 mA | ||||||
| 13–30 min | |||||||
| Rating about TUGT | Dong 2021 [35] | Stroke | 1, 12 | Ipsilesional motor cortex, SMA | 1.0, 2.0 mA | 45 | |
| 15, 20 min | |||||||
| Rating about FAC | Dong 2021 [35] | Stroke | 10–20 | Ipsilesional leg motor area, ipsilesional leg and hand motor area | 1.0–2.0 mA | 49 | |
| 7–20 min | |||||||
| Dysphagia (DOSS/MMASA/FOIS/FDS/VFSS) | Zhao 2022 [36] | Stroke | 4–48 | Hemisphere about pharyngeal cortex, cerebellar hemisphere | 1.0–2.0 mA | 334 | |
| 20, 30 min | |||||||
| Hemispatial neglect (LBT) | Salazar 2018 [37] | Stroke | 15 | Posterior parietal cortex, left posterior parietal cortex | 1.0 mA, 2.0 mA | 26 | |
| 20, 30 min | |||||||
| Parkinson’s disease | |||||||
| Score of MoCA | Liu 2021 [46] | PD | 20, 56 | L-DLPFC, CZ | 2.0 mA | 63 | |
| 20 min | |||||||
| Score of UPDRS-I | Liu 2021 [46] | PD | 20, 30 | DLPFC, Bi PFC, Fz | 1.0 mA, 1.2 mA | 97 | |
| 20 min | |||||||
| Global cognition (SCOPA/UPDRS/PD-MCI) | De Souza Souto 2024 [38] | PD | 2–10 | L-DLPFC/DLFPC, M1, MFC | 1.0–2.0 mA | 317 | |
| 5–20 min | |||||||
| Memory (DS-F/S-IT/the Go/No-Go Task) | De Souza Souto 2024 [38] | PD | 2–10 | L-DLPFC/DLFPC, M1 | 1.0 mA, 2.0 mA | 124 | |
| 5, 20 min | |||||||
| Reaction time (DS-F/S-IT/the Go/No-Go Task) | De Souza Souto 2024 [38] | PD | 2, 10 | L-DLPFC/DLFPC, MFC | 1.5 mA, 2.0 mA | 66 | |
| 6–20 min | |||||||
| Alzheimer’s disease | |||||||
| Score of MMSE | Hou 2024 [39] | AD/MCI | 10–224 | L-DLPFC, L-FTL, L-TPL | 1.0–5.0 mA | 150 | |
| 20–30 min | |||||||
| Score of MoCA | Hou 2024 [39] | MCI | 5–36 | L-DLPFC/R-DLPFC, L-TL | 1.0–2.0 mA | 159 | |
| 20, 30 min | |||||||
| Score of MODA | Hou 2024 [39] | AD | 14–244 | L-DLPFC, L-FTL | 2.0 mA | 22 | |
| 20 min | |||||||
| P300 latency | Hou 2024 [39] | AD/MCI | 5–56 | L-DLPFC, L-TL contralateral Supraorbital Region | 2.0–5.0 mA | 103 | |
| 20, 25 min | |||||||
| Cerebellar ataxia | |||||||
| Score of SARA | Chen 2021 [40] | CA | 1–10 | Cerebellum, spine, M1 | 2.0 mA | 58 | |
| 20 min, 40 min | |||||||
| Score of ICARS | Chen 2021 [40] | CA | 1, 10 | Cerebellum, spine | 2.0 mA | 51 | |
| 20 min | |||||||
| 8-MWT | Chen 2021 [40] | CA | 1, 10 | Cerebellum, spine | 2.0 mA | 51 | |
| 20 min | |||||||
| Fibromyalgia | |||||||
| Pain intensity (VAS/NRS/FIQ-R/PCP:S) | Yang 2024 [41] | FM | 1–60 | DLPFC, M1, OIC, ON | 1.0 mA, 2.0 mA | 440 | |
| 20, 30 min | |||||||
| Depression (HAM-D/BDI-II) | Yang 2024 [41] | FM | 1–60 | DLPFC, M1, OIC, ON | 1.0 mA, 2.0 mA | 337 | |
| 20, 30 min | |||||||
| Score of FIQ | Yang 2024 [41] | FM | 5–15 | DLPFC, M1, OIC, ON | 1.0 mA, 2.0 mA | 294 | |
| 20 min | |||||||
| Epilepsy | |||||||
| The Frequency of seizures | Lima 2024 [42] | Drug-resistant epilepsy | 1–28 | Cathodal: epilepsy focus | 1.0–2.0 mA | 127 | |
| 20, 30 min | |||||||
| Disorders of consciousness | |||||||
| Score of CRS-R | Fan 2023 [43] | DoC | 1–20 | L-DLPFC/DLFPC, PFC, posterior parietal cortex, bilateral frontoparietal areas, bilateral fronto-temporo-parietal cortices | 2.0 mA, 4.0 mA | 140 | |
| 20 min | |||||||
| Multiple sclerosis | |||||||
| Gait functionality (TUG, 2MWT, 25FWT) | Nombela-Cabrera 2023 [44] | MS | 1–12 | M1, right cerebellar hemi-sphere, cerebellum affected | 1.5–2.5 mA | 84 | |
| 13–30 min | |||||||
| Migraine | |||||||
| Pain intensity | Cai 2021 [45] | Migraine | 4 w, 8 w | Anodal: LDLPFC, L-M1 | 1.0 mA, 2.0 mA | 104 | |
| Cathodal: CZ | 15, 20 min | ||||||
| Adverse effect | |||||||
| Mood change | Yang 2024 [41] | FM | 1–60 | DLPFC, M1, OIC, ON | 1.0 mA, 2.0 mA | 21 | |
| 20, 30 min | |||||||
PSCI, post stroke cognitive impairment; PSD, post stroke depression; PD, Parkinson’s Disease; AD, Alzheimer’s Disease; MCI, mild cognitive impairment; CA, cerebellar ataxia; FM, fibromyalgia; DoC, disorders of consciousness; MS, multiple sclerosis; MoCA, Montreal Cognitive Assessment Test; MMSE, Mini-Mental State Examination; LOTCA, Loewenstein Occupational Therapy Cognitive Assessment; MBI, Modified Barthel Index; HAMD, Hamilton Depression Scale; BDI, Beck Depression Inventory; SADQ-H, Stroke Aphasic Depression Questionnaire Hospital Version; SDS, Self-Rating Depression Scale; FMA-UE, upper extremity Fugl–Meyer Assessment; ARRT, Action Research Arm Test; BI, Barthel Index; FMA-LE, Lower Extremity Fugl–Meyer Assessment; MAS, Modified Ashworth Scale; TUG/TUGT, Timed Up and Go Test; FAC, Functional Ambulation Category; DOSS, Dysphagia Outcome Severity Scale; MMASA, Modified Mann Assessment of Swallowing Ability; FOIS, Functional Oral Intake Scale; FDS, Functional Dysphagia Scale; VFSS, Video Fluoroscopic Swallowing Study; LBT, Line Bisection Test; UPDRS-I, Unified PD Rating Scale I; SCOPA, Scales for Outcomes in PD; PD-MCI, Parkinson’s disease with mild cognitive impairment; DS-F, Digit Span-Forward; S-IT, Stroop Interference Test; MODA, Milan Overall Dementia assessment; SARA, Scale for Assessment and Rating of Ataxia; ICARS, International Cooperative Ataxia Rating Scale; 8-MWT, 8-Meter Walk Time; VAS, Visual Analog Scale; NRS, Numeric Rating Scale; FIQ-R, Modified Fibromyalgia Questionnaire; PCP:S, Profile of Chronic Pain: Screen; HAM-D, Hamilton Depression Rating Scale; BDI-II, Beck Depression Inventory-II; FIQ, Fibromyalgia Questionnaire; CRS-R, Coma Recovery Scale-Revised; 2MWT, 2-Minute Walk Test; 25FWT, 25-Foot Walk Test; L-/R-, left/right; DLPFC, Dorsolateral Prefrontal Cortex; M1, Primary Motor Cortex; C3/C4/F3/CZ/FZ, according to the 10–20 International Electroencephalography System; SMA, Supplementary Motor Area; PFC, Prefrontal Cortex; MFC, Medial Frontal Cortex; FTL, Frontotemporal Lobe; TPL, Temporo-Parietal Lobe; TL, Temporal Cortex; OIC, Opercular-Insular Cortex; ON, Occipital Nerve Regions.
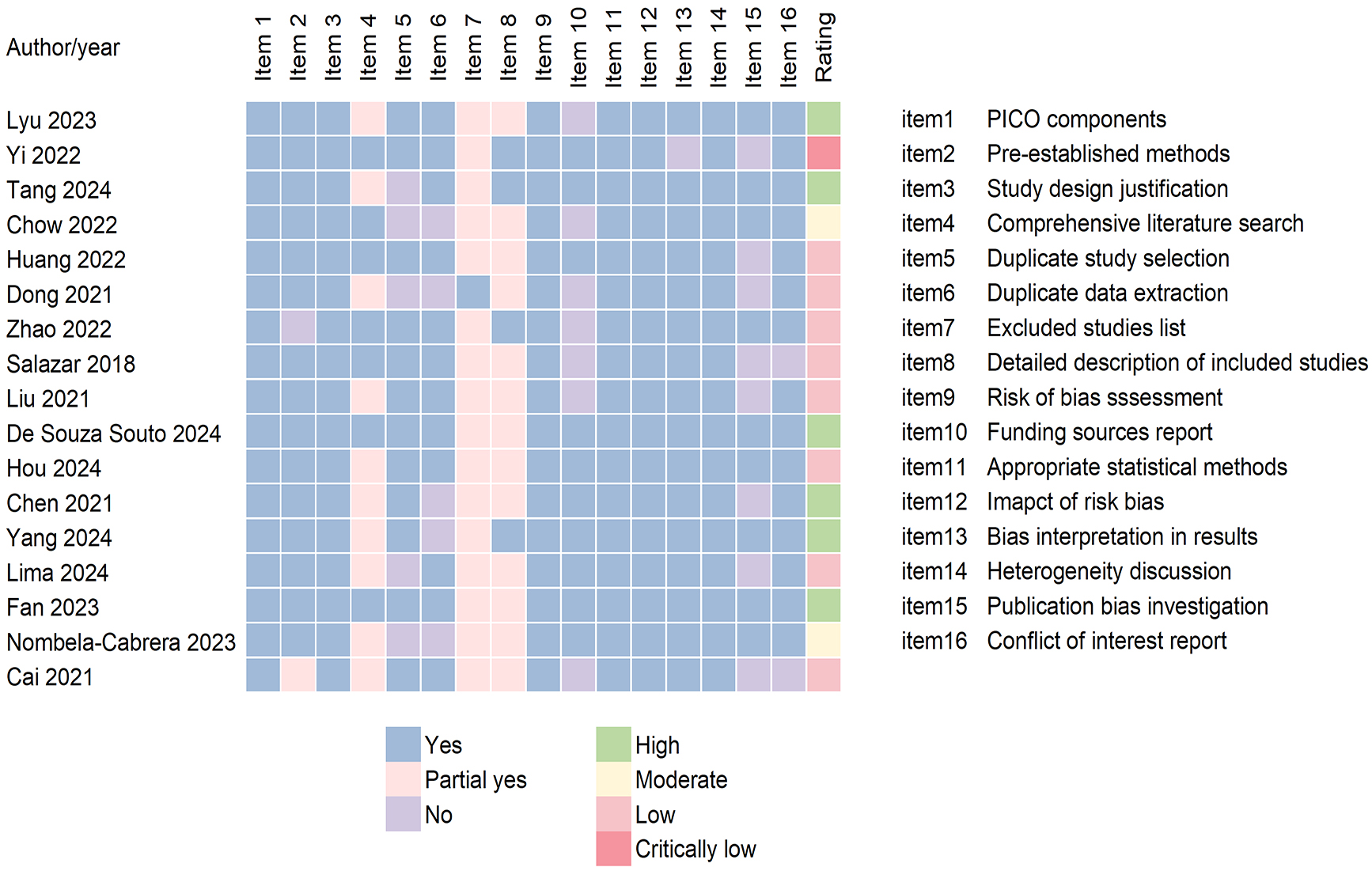
Using AMSTAR 2, the quality of the original study was high in six, moderate in two, low in eight, and critically low in one meta-analysis. Those studies rated high offered an accurate and comprehensive summary of the included health outcomes, containing Montreal Cognitive Assessment Test (MoCA), Mini-Mental State Examination (MMSE), Loewenstein Occupational Therapy Cognitive Assessment (LOTCA), Modified Barthel Index (MBI), Barthel Index (BI), P300 latency, and upper extremity motor function scores in stroke patients; global cognition, memory, and reaction time in Parkinson’s disease; Scale for Assessment and Rating of Ataxia (SARA), International Cooperative Ataxia Rating Scale (ICARS), and 8-Meter Walk Time (8-MWT) scores in cerebellar ataxia; gait functionality in multiple sclerosis; and pain, depression, and Fibromyalgia Questionnaire (FIQ) scores in fibromyalgia.
The detailed classification of the methodological quality is shown in Fig. 2. All studies satisfied the criteria for items 1, 3, 9, 11, 12, and 14, with 9 and 11 identified as key items. However, the majority of the studies received a downgraded rating due to shortcomings in critical items 4, 7, and 15. Regarding item 4, most studies were rated as “Partially Yes” owing to the absence of complete reference lists in the studies found. In the assessment of item 7, a considerable proportion of the studies failed to provide a comprehensive list of potentially relevant research, along with justifications for excluding them. Concerning item 15, six studies were rated as “No” for the insufficient investigation of publication bias.
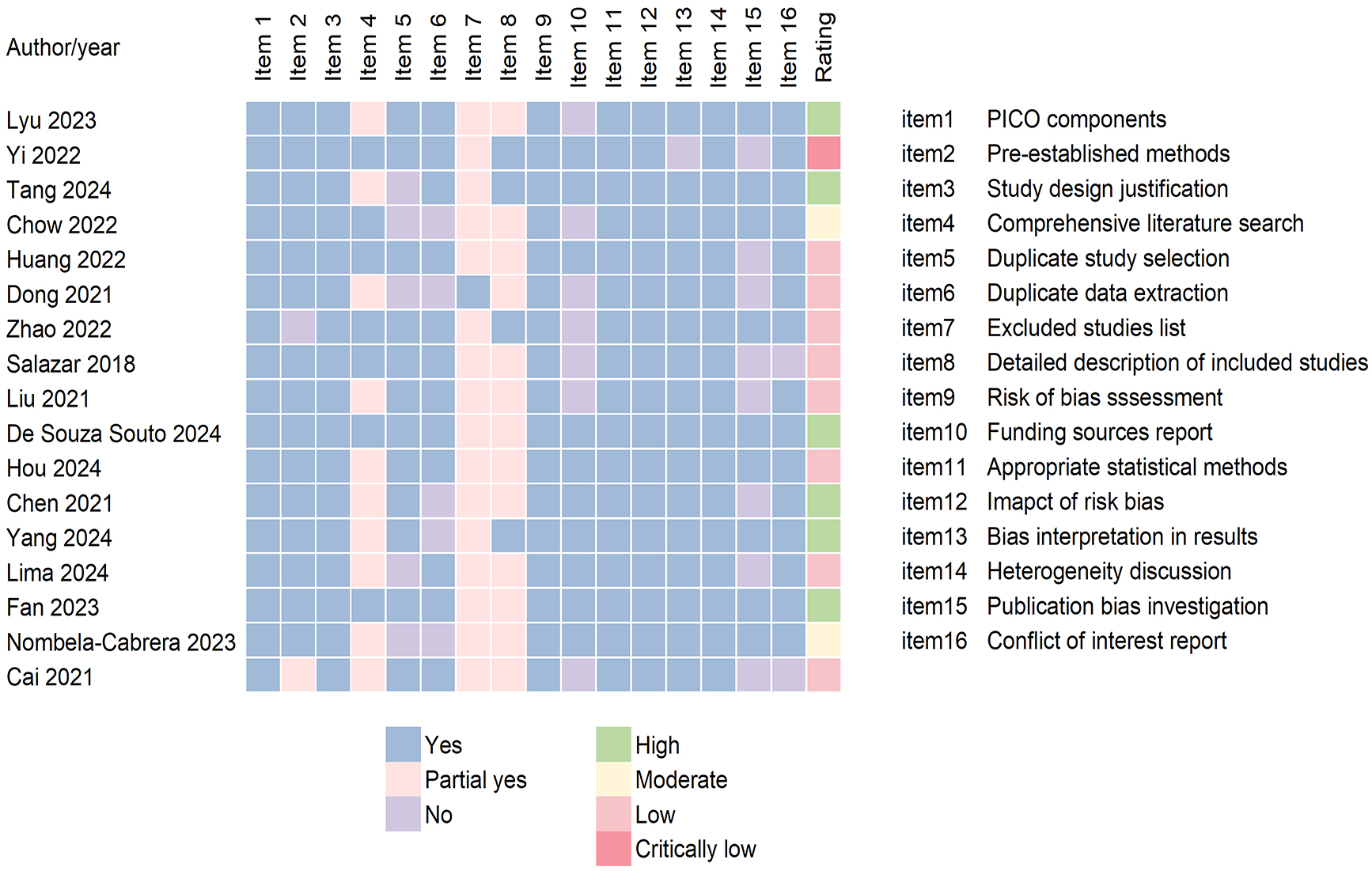 Fig. 2.
Fig. 2.
AMSTAR 2 quality assessment of each study. AMSTAR 2 contains 16 items. Each item has two or three ratings and the final rating is assigned to four assessments: high, moderate, low, critically low. AMSTAR 2, measurement tool to assess systematic reviews 2; PICO, Population, Intervention, Comparison, Outcome.
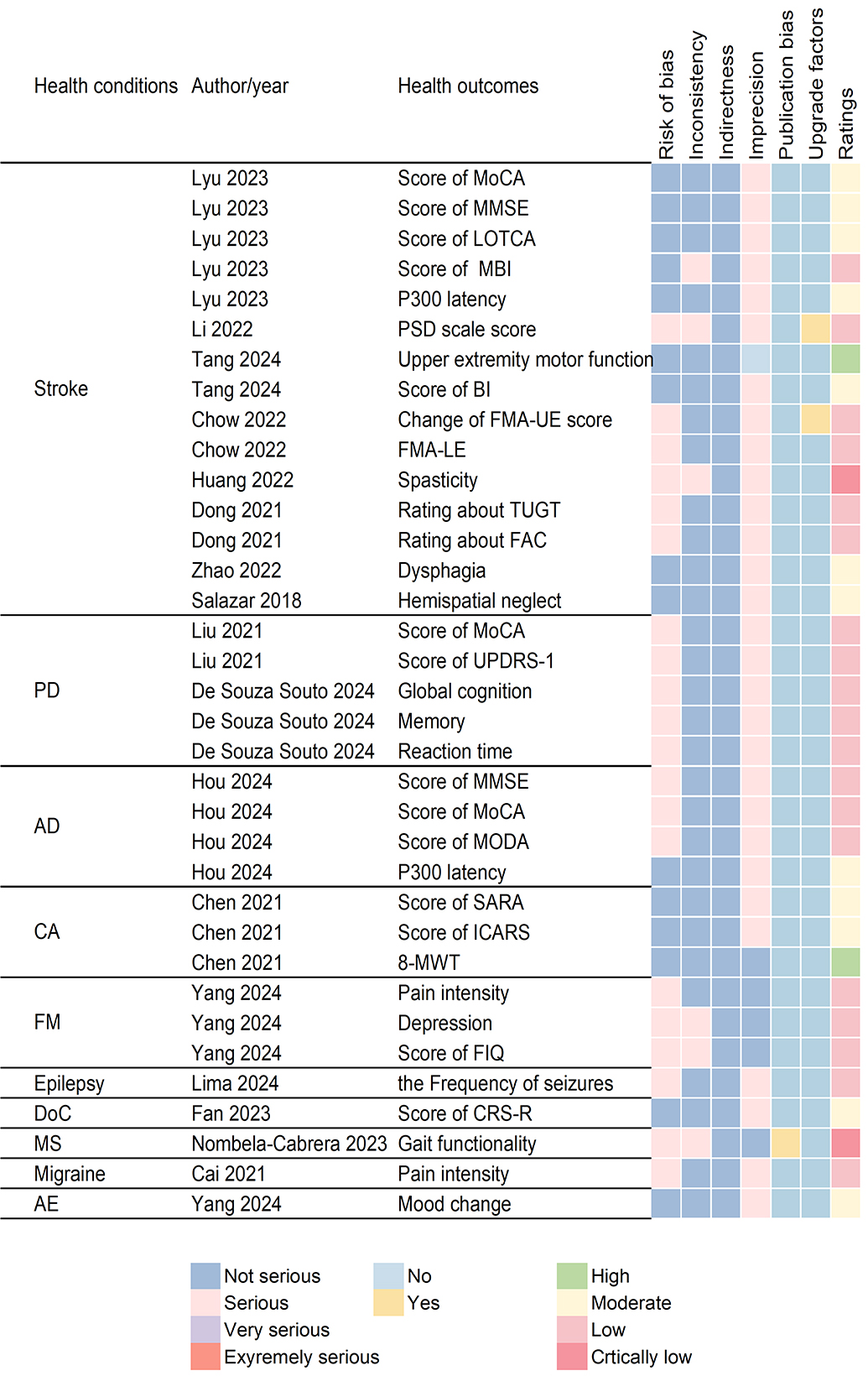
The evidence quality of the original study assessed using GRADE was rated as high in 2, moderate in 12, low in 19, and very low in 2 studies. High-certainty evidence demonstrated that tDCS significantly improved upper extremity motor function in patients with stroke and 8-MWT in cerebellar ataxia. The evidence classification details are comprehensively outlined in Fig. 3. All studies included were RCTs with direct evidence, thereby avoiding rating downgrades. No survey demonstrated plausible confounding or a dose-response gradient, maintaining the current evidence rating.
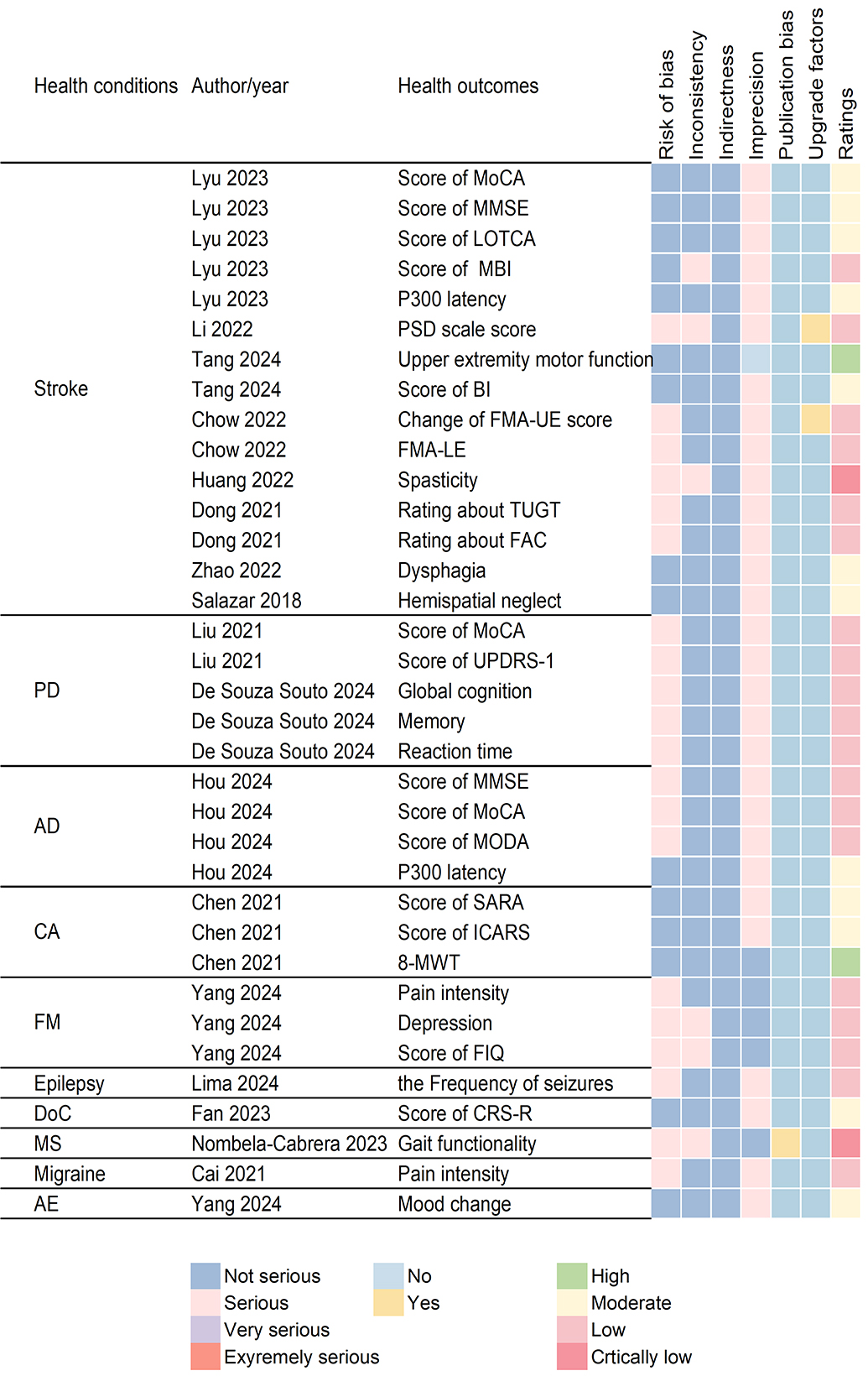 Fig. 3.
Fig. 3.
GRADE evidence assessment of the association between tDCS and each health outcome. The GRADE system encompassed five downgrade domains and three upgrade domains. Each downgrade domain has four ratings and the upgrade domains are totally assessed as “Yes” or “NO”. The final rating is assigned to four assessments: high, moderate, low, and critically low. GRADE, Grades of Recommendations, Assessment, Development, and Evaluation; tDCS, transcranial direct current stimulation; AE, adverse effect.
This umbrella review offered valuable insight regarding whether tDCS could guide clinical practice and patient management. The analysis of evidence from 17 publications indicated that tDCS exerted partial beneficial effects in seven distinct health conditions: stroke, Parkinson’s disease, Alzheimer’s disease, cerebellar ataxia, fibromyalgia, disorders of consciousness, and migraine, with adverse effects related to mood change reported in fibromyalgia. Furthermore, tDCS was found to influence 34 unique health outcomes, with one adverse effect.
The original effect estimates with 95% CI, alongside reanalyzed effect
estimates with 95% CI, I2, Tau2, and 95% PI, and the quality
assessments were all listed (Tables 1,2,3). Effect estimates with original and
new 95% CIs are shown in Table 2. MDs are presented in the most commonly used
original scale units, while SMDs are interpreted using Cohen’s conventions
(small: 0.2–0.5, medium: 0.5–0.8, and large:
| Health outcomes | Included studies | Effect measure | Reported models | Reported 95% CI | Reanalysis | HKSJ | HKSJ p-value | ||
| Fixed | Random | ||||||||
| Stroke | |||||||||
| Score of MoCA | 16 | MD | fixed | 2.53 [2.15 to 2.91] | 2.53 [2.15 to 2.91] | 2.51 [2.05 to 2.98] | 2.46 [1.82 to 3.09] | ||
| Score of MMSE | 10 | MD | fixed | 1.94 [1.48 to 2.40] | 1.94 [1.48 to 2.40] | 2.26 [1.51 to 3.00] | 2.25 [1.52 to 2.98] | ||
| Score of LOTCA | 2 | MD | fixed | 2.27 [1.42 to 3.11] | 2.27 [1.42 to 3.11] | 2.27 [1.42 to 3.11] | 2.27 [1.76 to 2.78] | ||
| Score of MBI | 12 | MD | random | 5.47 [3.76 to 7.18] | 5.47 [3.76 to 7.18] | 5.47 [3.76 to 7.18] | 5.56 [2.87 to 8.25] | ||
| P300 latency | 3 | MD | fixed | –14.53 [–20.41 to 8.66] | –14.53 [–20.41 to 8.66] | –14.54 [–20.69 to 8.38] | –14.57 [–28.60 to –0.54] | ||
| PSD scale score | 8 | SMD | random | 1.61 [1.02 to 2.19] | 1.39 [1.16 to 1.61] | 1.60 [1.02 to 2.19] | 1.64 [0.73 to 2.54] | 0.004** | |
| Upper extremity motor function | 48 | SMD | fixed | 0.22 [0.12 to 0.32] | 0.22 [0.12 to 0.32] | 0.22 [0.07 to 0.37] | 0.22 [0.07 to 0.37] | 0.006** | |
| Score of BI | 15 | MD | fixed | 4.65 [2.82 to 6.49] | 4.65 [2.82 to 6.49] | 4.42 [1.84 to 7.00] | 4.50 [1.63 to 7.37] | 0.005** | |
| Change of FMA-UE score | 28 | MD | fixed | 1.68 [0.25 to 3.11] | 1.68 [0.25 to 3.11] | 1.68 [0.25 to 3.11] | 1.77 [0.70 to 2.86] | 0.003** | |
| Lower extremity motor assessment | 5 | MD | fixed | 2.19 [1.07 to 3.30] | 2.19 [1.07 to 3.30] | 2.19 [1.07 to 3.30] | 2.62 [–0.34 to 5.57] | 0.070 | |
| Spasticity | 12 | SMD | random | –0.83 [–1.25 to 0.40] | –0.77 [–0.92 to –0.62] | –0.83 [–1.25 to –0.40] | –0.83 [–1.33 to –0.33] | 0.004** | |
| Rating about TUGT | 5 | MD | fixed | –2.61 [–4.00 to –1.22] | –1.08 [–1.96 to –0.22] | –2.18 [–4.51 to 0.15] | –4.57 [–15.17 to 6.03] | 0.300 | |
| Rating about FAC | 5 | MD | fixed | 0.35 [0.11 to 0.58] | 0.15 [0.01 to 0.28] | 0.34 [–0.14 to 0.82] | 0.34 [–0.22 to 0.90] | 0.170 | |
| Dysphagia | 18 | SMD | random | 0.80 [0.45 to 1.14] | 0.74 [0.58 to 0.90] | 0.80 [0.45 to 1.15] | 0.81 [0.35 to 1.26] | 0.002** | |
| Hemispatial neglect | 3 | SMD | random | –1.07 [–1.76 to –0.37] | –1.07 [–1.76 to –0.37] | –1.07 [–1.76 to –0.37] | –1.08 [–2.26 to 0.10] | 0.060 | |
| Parkinson’s disease | |||||||||
| Score of MoCA | 2 | SMD | random | 0.87 [0.50 to 1.24] | 0.87 [0.50 to 1.24] | 0.87 [0.50 to 1.24] | 0.87 [–0.61 to 2.35] | 0.080 | |
| Score of UPDRS-I | 2 | SMD | random | –1.29 [–1.60 to –0.98] | –1.29 [–1.61 to –0.98] | –1.29 [–1.60 to –0.98] | –1.30 [–3.17 to 0.58] | 0.070 | |
| Global cognition | 27 | SMD | random | 0.24 [0.09 to 0.40] | 0.24 [0.09 to 0.40] | 0.24 [0.09 to 0.40] | 0.25 [0.10 to 0.40] | 0.002** | |
| Memory | 11 | SMD | random | 0.34 [0.07 to 0.61] | 0.34 [0.08 to 0.59] | 0.34 [0.07 to 0.61] | 0.35 [0.04 to 0.66] | 0.030* | |
| Reaction time | 6 | SMD | random | 0.42 [0.07 to 0.76] | 0.42 [0.07 to 0.76] | 0.42 [0.07 to 0.76] | 0.41 [0.14 to 0.69] | 0.010* | |
| Alzheimer’s disease | |||||||||
| Score of MMSE | 7 | MD | fixed | 1.76 [1.29 to 2.23] | 1.76 [1.29 to 2.23] | 1.97 [1.24 to 2.71] | 2.11 [0.99 to 3.23] | 0.004** | |
| Score of MoCA | 7 | MD | fixed | 0.56 [0.11 to 1.11] | 0.56 [0.11 to 1.01] | 0.56 [0.04 to 1.07] | 0.54 [–0.08 to 1.16] | 0.080 | |
| Score of MODA | 2 | MD | fixed | 6.52 [3.73 to 9.31] | 6.52 [3.73 to 9.31] | 6.52 [3.73 to 9.31] | 6.52 [3.55 to 9.49] | 0.020* | |
| P300 latency | 4 | MD | fixed | –39.73 [–51.78 to 27.68] | –39.73 [–51.78 to 27.68] | –38.35 [–56.19 to 20.50] | –38.15 [–65.51 to 10.79] | 0.020* | |
| Cerebellar ataxia | |||||||||
| Score of SARA | 4 | SMD | random | –0.71 [–1.18 to –0.23] | –0.68 [–1.07 to –0.29] | –0.71 [–1.18 to –0.23] | –0.74 [–1.56 to –0.09] | 0.070 | |
| Score of ICARS | 3 | SMD | random | –0.62 [–1.03 to –0.21] | –0.62 [–1.03 to –0.21] | –0.62 [–1.03 to –0.21] | –0.62 [–1.10 to –0.15] | 0.030* | |
| 8-MWT | 3 | SMD | random | –0.42 [–0.82 to –0.02] | –0.42 [–0.82 to –0.02] | –0.42 [–0.82 to –0.02] | –0.42 [–0.60 to –0.24] | ||
| Fibromyalgia | |||||||||
| Pain intensity | 20 | SMD | random | –1.04 [–1.38 to –0.69] | –0.82 [–0.98 to –0.67] | –1.04 [–1.38 to –0.69] | –1.08 [–1.53 to –0.64] | ||
| Depression | 20 | SMD | random | –0.73 [–1.09 to –0.36] | –0.56 [–0.75 to –0.37] | –0.73 [–1.09 to –0.36] | –0.75 [–1.18 to –0.31] | 0.003** | |
| Score of FIQ | 20 | SMD | fixed | –0.46 [–0.64 to –0.29] | –0.46 [–0.64 to –0.29] | –0.57 [–0.92 to –0.21] | –0.57 [–0.96 to –0.18] | 0.007** | |
| Epilepsy | |||||||||
| The Frequency of seizures | 7 | MD | random | –3.15 [–5.11 to –1.18] | –3.15 [–5.11 to –1.18] | –3.15 [–5.11 to –1.18] | –4.31 [–11.86 to 3.25] | 0.210 | |
| Disorders of consciousness | |||||||||
| Score of CRS-R | 9 | MD | random | 2.07 [1.58 to 2.57] | 0.90 [0.61 to 1.18] | 1.34 [0.57 to 2.10] | 1.39 [0.34 to 2.44] | 0.020* | |
| Multiple sclerosis | |||||||||
| Gait functionality | 11 | SMD | fixed | –0.71 [–1.05 to –0.37] | –0.71 [–1.05 to –0.37] | –0.67 [–1.29 to –0.05] | –0.67 [–1.41 to 0.07] | 0.070 | |
| Migraine | |||||||||
| Pain intensity | 5 | MD | random | –1.44 [–2.13 to –0.76] | –1.47 [–1.95 to –0.99] | –1.46 [–1.99 to –0.92] | –1.46 [–2.29 to –0.62] | 0.008** | |
| Adverse effect | |||||||||
| Mood change | 2 | RD | fixed | –0.06 [–0.11 to –0.01] | –0.06 [–0.11 to –0.01] | –0.06 [–0.11 to –0.01] | –0.06 [–0.07 to –0.05] | 0.006** | |
95% CI, 95% confidence interval; HKSJ, hartung-knapp-sidik-jonkman; SMD,
standardized mean difference. HKSJ p-values: *p
| Health outcomes | I2 | Tau2 | 95% PI | Egger’s p-value | Trim-and-fill method | Association | |
| Stroke | |||||||
| Score of MoCA | 23.30% | 1.05 | [0.15 to 4.77] | 0.33 | 2.73 [2.06 to 3.40] | association | |
| Score of MMSE | 49.40% | 0.53 | [0.41 to 4.09] | 0.15 | 1.39 [0.50 to 2.29] | association | |
| Score of LOTCA | 0.00% | 0.01 | [0.84 to 3.70] | NA | 2.14 [1.70 to 2.57] | association | |
| Score of MBI | 0.00% | 9.47 | [–2.32 to 13.44] | 0.85 | 5.56 [2.87 to 8.25] | association | |
| P300 latency | 8.20% | 15.10 | [–37.88 to 8.74] | NA | –14.57 [–28.60 to –0.54] | association | |
| PSD scale score | 83.90% | 1.05 | [–0.95 to 4.22] | NA | 1.19 [0.15 to 2.23] | association | |
| Upper extremity motor function | 48.80% | 0.19 | [–0.68 to 1.12] | 0.82 | 0.22 [0.07 to 0.37] | association | |
| Score of BI | 37.20% | 16.48 | [–4.82 to 13.81] | 0.92 | 3.71 [0.76 to 6.66] | association | |
| Change of FMA-UE score | 0.00% | 2.45 | [–1.87 to 5.41] | 0.24 | 0.96 [–0.22 to 2.15] | association | |
| Lower extremity motor assessment | 0.00% | 4.23 | [–4.23 to 9.46] | NA | 1.92 [–1.36 to 5.21] | NA | |
| Spasticity | 86.60% | 0.54 | [–2.53 to 0.87] | 0.50 | –0.83 [–1.33 to –0.33] | association | |
| Rating about TUGT | 69.80% | 80.47 | [–32.34 to 23.20] | NA | –0.93 [–11.12 to 9.26] | NA | |
| Rating about FAC | 90.20% | 0.16 | [–0.92 to 1.59] | NA | –0.14 [–0.77 to 0.50] | NA | |
| Dysphagia | 76.70% | 0.73 | [–1.06 to 2.67] | 0.47 | 0.80 [0.35 to 1.26] | association | |
| Hemispatial neglect | 0.00% | 0.07 | [–3.11 to 0.95] | NA | –1.08 [–2.26 to 0.10] | NA | |
| Parkinson’s disease | |||||||
| Score of MoCA | 0.00% | 0.00 | [–1.72 to 3.47] | NA | NA | NA | |
| Score of UPDRS-I | 0.00% | 0.01 | [–3.99 to 1.40] | NA | NA | NA | |
| Global cognition | 0.00% | 0.07 | [–0.31 to 0.81] | 0.02* | 0.09 [–0.08 to 0.26] | association | |
| Memory | 13.20% | 0.10 | [–0.45 to 1.15] | 0.08 | 0.15 [–0.19 to 0.49] | association | |
| Reaction time | 0.00% | 0.01 | [–0.15 to 0.98] | NA | 0.47 [0.21 to 0.72] | association | |
| Alzheimer’s disease | |||||||
| Score of MMSE | 35.00% | 1.01 | [–0.66 to 4.88] | NA | 2.11 [0.99 to 3.23] | association | |
| Score of MoCA | 18.00% | 0.21 | [–0.80 to 1.89] | NA | 0.67 [0.13 to 1.22] | NA | |
| Score of MODA | 0.00% | 0.00 | [–11.57 to 24.61] | NA | NA | association | |
| P300 latency | 42.80% | 159.02 | [–88.37 to 12.08] | NA | –41.67 [–66.33 to –17.02] | association | |
| Cerebellar ataxia | |||||||
| Score of SARA | 27.40% | 0.16 | [–2.32 to 0.85] | NA | –0.39 [–1.22 to 0.43] | NA | |
| Score of ICARS | 0.00% | 0.00 | [–1.59 to 0.34] | NA | –0.62 [–1.10 to –0.15] | association | |
| 8-MWT | 0.00% | 0.00 | [–1.30 to 0.47] | NA | –0.42 [–0.60 to –0.24] | association | |
| Fibromyalgia | |||||||
| Pain intensity | 77.40% | 1.14 | [–3.33 to 1.16] | 0.01 | –0.64 [–1.21 to –0.07] | association | |
| Depression | 69.30% | 0.48 | [–2.30 to 0.80] | 0.01 | –0.39 [–0.92 to 0.15] | association | |
| Score of FIQ | 73.60% | 0.41 | [–1.99 to 0.86] | 0.10 | –0.40 [–0.83 to 0.04] | association | |
| Epilepsy | |||||||
| The Frequency of seizures | 0.00% | 1026.65 | [–91.36 to 82.74] | NA | –2.96 [–15.00 to 9.07] | NA | |
| Disorders of consciousness | |||||||
| Score of CRS-R | 82.80% | 1.33 | [–1.55 to 4.33] | NA | 0.70 [–0.55 to 1.96] | association | |
| Multiple sclerosis | |||||||
| Gait functionality | 69.20% | 0.57 | [–2.61 to 1.27] | NA | –0.67 [–1.40 to 0.07] | NA | |
| Migraine | |||||||
| Pain intensity | 21.90% | 0.03 | [–2.35 to –0.56] | NA | –1.40 [–2.30 to –0.50] | association | |
| Adverse effect | |||||||
| Mood change | 0.00% | [–0.36 to 0.24] | NA | NA | association | ||
NA, not available; 95% PI, 95% prediction interval. Egger’s p-values:
*p
The reanalysis of the 34 outcomes using the HKSJ random-effects model in this
umbrella review showed that 18 out of 34 (38.24%) outcomes exhibited low
heterogeneity (I2
tDCS was significantly associated with 11 health outcomes among post-stroke
patients, including improvements in MoCA scores (MD = 2.46 points, 95% CI:
1.82–3.09), MMSE scores (MD = 2.25 points, 95% CI: 1.52–2.98), LOTCA scores
(MD = 2.27 points, 95% CI: 1.76–2.78), MBI scores (MD = 5.56 points, 95% CI:
2.87–8.25) with large magnitude, BI scores (MD = 4.50 points, 95% CI:
1.63–7.37) with large magnitude, upper extremity motor function (SMD = 0.22,
95% CI: 0.07–0.37), and dysphagia (SMD = 0.81, 95% CI: 0.35–1.26), decreases
in PSD scale scores (SMD = 1.64, 95% CI: 0.73–2.54) with a significant large
effect, P300 latency (SMD = –14.57, 95% CI: –28.60 to –0.54) with a
significant large effect, spasticity (SMD = –0.83, 95% CI: –1.33 to –0.33),
and changes in FMA-UE scores (MD = 1.77 points, 95% CI: 0.70–2.86). Among the
associated health outcomes, 7 out of 11 studies exhibited low heterogeneity
(
Three out of five (60%) analyses supported the association of tDCS with improvements in global cognition (SMD = 0.25, 95% CI: 0.10–0.40), memory (SMD = 0.35, 95% CI: 0.04–0.66), and reaction time (SMD = 0.41, 95% CI: 0.14–0.69), with low heterogeneity. Egger’s test was conducted in two studies, with publication bias detected in one study assessing global cognition in Parkinson’s disease. Furthermore, 60% (3/5) of the health outcomes were rated as having high methodological quality, while all analyses achieved a low-grade rating.
Three out of four (75%) analyses indicated that tDCS was associated with improvements in MMSE scores (SMD = 2.11, 95% CI: 0.99–3.23), MODA scores (SMD = 6.52, 95% CI: 3.55–9.49), and reductions in P300 latency (SMD = –38.15, 95% CI: –65.51 to –10.79). Fifty percent (2/4) of the studies exhibited low heterogeneity. All included studies were separately assessed as low quality according to AMSTAR 2. Only one outcome received a moderate GRADE rating, while the others were low.
Two-thirds (66.67%) of the analyses indicated that tDCS improved ICARS scores (SMD = –0.62, 95% CI: –1.10 to –0.15) and decreased 8-MWT (SMD = –0.42, 95% CI: –0.60 to –0.24), without heterogeneity. Compared with other associated health outcomes, these two outcomes both received high methodological quality and moderate to high evidential ratings.
Our study demonstrated that tDCS was effective for three health outcomes related to fibromyalgia, including pain, depression, and FIQ scores (SMD = –1.08, 95% CI: –1.53 to –0.64; SMD = –0.75, 95% CI: –1.18 to –0.31; SMD = –0.57, 95% CI: –0.96 to –0.18, respectively). The heterogeneity across these outcomes ranged from 69.30% to 77.40%. Although the AMSTAR 2 ratings scored highly, the GRADE ratings were low.
The new estimated 95% CI was insignificant (MD = –4.31 times, 95% CI: –11.86
to 3.25, p
Because only one analysis was included and it had a reanalyzed p-value of less than 0.05, we found that tDCS significantly increased CRS-R scores (MD/RD = 1.39, 95% CI: 0.34 to 2.44), with high heterogeneity. The AMSTAR 2 rating was high, and the GRADE rating was moderate.
One analysis found that tDCS was not helpful for enhancing gait functionality in patients with multiple sclerosis (SMD = –0.67, 95% CI: –1.41 to 0.07). The heterogeneity was 69.20%. Its AMSTAR 2 rating was moderate, but the very low GRADE rating did not support the evidence.
The reanalyzed estimated 95% CI showed that tDCS alleviated pain intensity in migraine patients (MD/RD = –1.46, 95% CI: –2.29 to –0.62). Moreover, the quality assessments of this health condition were both low.
Most studies included reported mild adverse effects, including skin itching, skin tingling, skin burning, headache, dizziness, sleepiness, postural hypotension, and constipation. Mood change was experienced by patients with tDCS (MD/RD = –0.06, 95% CI: –0.07 to –0.05). The AMSTAR 2 rating was high, while the GRADE rating was moderate. No serious adverse events were reported by the authors.
This umbrella review focused on neurological disorders, offering robust evidence on the efficacy and safety of tDCS in a broad range of neurological disorders. A total of 17 systematic reviews and meta-analyses encompassing 358 RCTs and 7160 participants were analyzed. tDCS demonstrated efficacy in seven distinct health conditions, including stroke, Parkinson’s disease, Alzheimer’s disease, cerebellar ataxia, fibromyalgia, disorders of consciousness, and migraine, with adverse effects related to mood changes reported in patients with fibromyalgia. Our results indicated that tDCS significantly influenced 34 neurological health outcomes. Literature on upper extremity motor function in stroke and 8-MWT in cerebellar ataxia showed high methodological and evidential quality based on AMSTAR 2 and GRADE assessments.
tDCS was associated with improvements in cognition, depression, and swallowing in stroke patients, consistent with current research. A previous study showed that tDCS improved global cognitive function in stroke patients more than other non-invasive stimulation methods [47]. Notably, tDCS could also reduce anxiety symptoms [48]. The predominant mechanisms of tDCS treatment in patients with cognitive and psychiatric dysfunction are the modulation of cortical excitability and the plasticity of cortical neurons. Thereby, it can regulate the dynamic imbalance between the default mode network and the frontal-parietal control network, harmonizing cognitive control and emotion regulation [49]. Furthermore, the majority of studies on swallowing function recovery in stroke patients support the positive impact of tDCS in decreasing the rate of complications [50]. Anodal tDCS, specifically targeting the left inferior frontal gyrus, represents a therapeutic way to enhance swallowing function [51]. However, our analysis did not demonstrate that tDCS significantly elevated hemispatial neglect, potentially owing to inadequate evidence. One review reported very low evidence supporting the effect of tDCS on hemispatial neglect [51]. Additionally, tDCS showed efficacy in the management of post-stroke depression, alleviating depressive symptoms by multiple assessment scales in stroke survivors [52]. However, the methodological evidence supporting the association was rated as critically low quality. Therefore, the findings must be interpreted with considerable caution due to the underlying limitations in the primary evidence.
Regarding the effect of tDCS on motor function in stroke patients, our umbrella review, based on the synthesis of existing meta-analyses, demonstrated a significant improvement in upper extremity motor function (as measured by FMA-UE/Action Research Arm Test [ARRT]), with high-quality evidence assessed by AMSTAR 2 and GRADE. This supports the overall efficacy of tDCS for this specific outcome. Maybe because tDCS increases cerebral blood flow or balances the symmetry between the cerebral hemi-spheres [53, 54]. However, the ongoing controversy and heterogeneity in the field must be acknowledged. For instance, some primary studies and systematic reviews have reported limited or inconclusive effects, potentially attributable to variations in study quality, small sample sizes, or differences in outcome measures focusing on muscle strength alone [55, 56]. Notably, a recent large-scale multicenter trial found that adding tDCS to constraint-induced movement therapy did not result in additional benefits in reducing motor impairment in a specific subacute stroke cohort [57]. This apparent inconsistency underscores that the therapeutic efficacy of tDCS is likely significantly modulated by key parameters, such as intensity, target, duration, sessions and patient characteristics (e.g., time since stroke). Therefore, while the aggregated high-quality evidence from meta-analyses supports its potential, the optimal application of tDCS for post-stroke motor recovery requires further refinement. Future research should focus on defining precise stimulation protocols and identifying the patient subgroups most likely to benefit, which is crucial for translating this promising intervention into consistent and effective clinical practice. Although certain effects remain to be clarified, improvements in various functional impairments by tDCS treatment were confirmed and can be broadly applied in the field of stroke rehabilitation.
The study suggested tDCS significantly increased cognition in patients with Parkinson’s disease, with low heterogeneity. Likewise, insight from related fields aligns with what we found. tDCS combined with cognitive training was suggested to enhance attention and working memory in Parkinson’s disease [58, 59, 60]. tDCS over the dorsolateral prefrontal cortex (DLPFC) improved several cognitive performances with large effect sizes [61]. Both of the included studies [38, 46] mentioned that tDCS-induced cognitive gains may stem from enhanced neural connectivity between cortical and subcortical networks, neuroplasticity [51, 62], and increased dopamine release [63] due to cortical stimulation. However, we did not investigate the impact of motor function in Parkinson’s disease patients owing to a lack of substantial evidence. Thus, the effect of tDCS on this condition is unclear. Some insight from this field suggests a slight benefit on the motor ability of patients with Parkinson’s disease [64, 65]. However, the latest secondary study argued that tDCS combined with motor training improves motor function, particularly in gait-related parameters [66]. tDCS that was designed to simultaneously target motor and cognitive regions effectively improved motor and cognitive performance during tasks [67, 68]. Therefore, research efforts are proposed to further confirm the effect of tDCS on motor areas.
Regarding patients with Alzheimer’s disease, we reported the effects of tDCS on
distinct cognitive domains, including MMSE, MODA, and p300 latency scores. Many
studies have been conducted recently on tDCS as a potentially beneficial
intervention for Alzheimer’s disease patients. Our findings are consistent with
these investigations [69, 70]. Despite the significant efficacy, meta-analytic
evidence on specific cognitive functions is inconsistent. An up-to-date umbrella
review indicated that tDCS could significantly boost cognitive abilities like
global cognition, language, executive functions, and memory in patients with
Alzheimer’s disease and mild cognitive impairment [71]. Another meta-analysis
provided insight that tDCS effectively enhanced global cognition in older adults
with mild cognitive impairment but no specific memory or executive functions
[72]. However, the etiology and pathogenesis of AD remain inadequately explored.
The potential mechanisms are as follows. On the one hand, tDCS could facilitate
alterations in synaptic efficacy to enhance cortical function [73]. On the other
hand, tDCS could increase the permeability of the blood-brain barrier, promote
cerebral perfusion, and elevate blood flow velocity [74]. tDCS probably impacts
amyloid-beta (A
Our research provides evidence that tDCS mitigates ataxia symptoms in patients with cerebellar ataxia with lasting results. The involved meta-analysis [40] reported that tDCS modulates cortical excitability to promote neuroplasticity in the cerebellar cortex [51]. Given that cerebellar ataxia can lead to slow and irregular patterns in Purkinje cells [76], the predominant neuronal type in this region, the application of tDCS could enhance Purkinje cell functionality and restore the normal functions of the cerebellar network. tDCS proved to be better than other non-invasive stimuli in treating cerebellar ataxia [77]. A previous study showed that tDCS reduced disease severity and enhanced finger dexterity and quality of life in patients with cerebellar ataxia [78]. A meta-analysis and systematic review further substantiated the superior efficacy of tDCS in improving gait ataxia compared to finger dexterity [40]. While there is some evidence regarding the effects of tDCS on cerebellar ataxia, the scarcity of literature underscores the necessity for further research to gain a comprehensive understanding of the subject.
Our study found that tDCS was useful for three key health outcomes of fibromyalgia: pain, depression, and FIQ scores. Regarding pain alleviation, prior systematic reviews and meta-analyses have consolidated existing evidence for the clinical effectiveness of tDCS in managing fibromyalgia-related pain [79, 80]. They confirmed that applying tDCS at 2 mA to the left primary motor cortex was the most effective approach. It is presently unclear whether depression can be alleviated by tDCS. While one systematic review questioned the effects on anxiety and depression, another study argued that tDCS is a safe approach to reducing depression [41]. The potential mechanism underlying fibromyalgia is believed to be linked to central sensitization [81, 82]. The primary meta-analysis [41] indicated that tDCS mitigated abnormal central nervous system function by promoting structural plasticity and neuronal reorganization [83]. As the debate regarding this concern is ongoing, further evidence is necessary.
Our study demonstrated that tDCS did not significantly reduce the frequency of seizures. The newly estimated 95% CI calculated using the HKSJ method differed from the original 95% CI. In contrast, some previous evidence has indicated the potential effect of tDCS on epilepsy patients. Several studies suggested that tDCS reduces seizure frequency in patients with epilepsy and refractory epilepsy [84, 85, 86]. Nevertheless, a meta-analysis found that tDCS did not appear to affect epileptiform discharges, although it could lower seizure frequency [87]. The fundamental mechanism of tDCS in epilepsy remains unclear, but it is probably due to the decreased excitability of the cerebral cortex resulting from cathodal hyperpolarization or modulation of N-methyl-D-aspartate (NMDA) receptors and the Gamma-aminobutyric acid (GABA) system [88, 89]. Considering the differences and vagueness, we hypothesize that the inconsistency might be attributed to remarkable heterogeneity. Whether tDCS produces adverse effects in patients with epilepsy has been controversial for many years. Consequently, we recommend that future studies prioritize minimizing heterogeneity and providing more credible evidence to substantiate the effectiveness and safety of tDCS in treating epilepsy.
This umbrella review proposed that tDCS was efficient for disorders of consciousness, consistent with the results of other studies. Professor Aurore Thibaut, whose research focuses on the efficacy of tDCS in disorders of consciousness, has consistently demonstrated [90, 91, 92, 93] that tDCS can enhance consciousness levels in patients with disorders of consciousness. Meanwhile, a guideline provided class II evidence supporting the efficacy of tDCS for disorders of consciousness [94]. Earlier meta-analyses reported that multiple tDCS sessions on the left-dorsolateral prefrontal cortex (L-DLPFC) were the most effective [95, 96] in patients with disorders of consciousness. Moreover, several studies reported that tDCS demonstrated notable efficacy for patients diagnosed with a minimally conscious state [97, 98]. The following are some potential explanations mentioned for why tDCS may enhance consciousness. One reason is that tDCS may alter the cortex’s excitability in response to anodal stimulation [99]. According to the mesocircuit model [16, 100], tDCS stimulation targeting the L-DLPFC induces increased cortical activity, which subsequently robustly stimulates the striatum. This increased striatal output inhibits the internal globus pallidus (GPi), thereby reducing GPi-mediated suppression of the thalamus. Consequently, the disinhibited thalamus effectively excites cortical regions, particularly the prefrontal cortex, establishing a self-reinforcing positive feedback loop. This sustained neurocircuitry activity maintains high-level, organized cortical processing, potentially promoting the recovery of wakeful consciousness. Another reason is that it can enhance synaptic plasticity by altering the NMDA acid receptor’s mediation [12]. Patients with disorders of consciousness have a long and difficult recovery process. Thus, it is essential to identify the therapeutic mechanism of tDCS for this patient population.
We discovered the potential of tDCS to improve gait functionality for patients with multiple sclerosis, along with very low-quality evidence. Despite low certainty, some findings support the effect of tDCS in patients with multiple sclerosis [101, 102]. tDCS had favorable effects on cognitive processing speed, mood, pain, and fatigue in multiple sclerosis [103]. Fatigue, recognized as the most common disabling symptom in multiple sclerosis, was effectively treated with tDCS and benefited the most [104], while motor performance benefited the least [105]. The mechanism of tDCS in treating multiple sclerosis remains unclear. Uncertain mechanisms and considerable heterogeneity across studies persist, underscoring the need for further large-scale, long-term investigations.
This study demonstrated the efficacy of tDCS in reducing pain intensity among migraine patients, corroborating earlier findings [106]. tDCS exhibited a superior effect on pain relief compared to other non-invasive stimulation techniques [107]. One significant pathophysiological mechanism of migraine is central sensitization [108]. The original study [45] explained that multiple tDCS sessions may induce cumulative and long-term neuroplastic changes within the cerebral cortex of individuals experiencing migraine [109].
Our reanalysis reported that tDCS led to mood changes in patients with fibromyalgia. Future studies should use large sample sizes to confirm this negative effect. Considering other studies, we can conclude that the mild and transient adverse effects support tDCS as a low-risk treatment for neurological disorders. This idea is in accordance with the preliminary evidence [110, 111, 112]. Effects were categorized into three groups: mostly skin harms, effects on neurological or psychological problems and other potential effects. No serious adverse events were reported from our reanalysis, suggesting it is a safe therapeutic tool for short-term use. However, the long-term safety profile remains inadequately characterized because of the lack of systematic long-term monitoring. Therefore, the safety of long-term tDCS application is unknown.
This umbrella review synthesized evidence regarding the clinical efficacy and
safety of using tDCS in patients with neurological disorders, while also
providing a framework for mechanistic investigations. tDCS delivers a
subthreshold direct current, typically between 1 and 2 mA, through electrodes
placed on the scalp. First, this technique induces polarity-dependent modulation
of cortical excitability. Specifically, anodal stimulation normally enhances
neuronal firing, while cathodal stimulation generally decreases it. Then, these
transient excitability shifts can subsequently facilitate synaptic plasticity.
During the transformation, tDCS is thought to modulate NMDA receptor-dependent
processes, inducing long-term potentiation-like or long-term depression. Synaptic
plasticity is integral to the reconstruction of neural networks. This process
applies to the majority of neurological disorders, typically stroke. tDCS may
affect neurotransmitter systems for therapeutic purposes, including modulating
dopamine levels in Parkinson’s disease and GABA levels in epilepsy. Additionally,
emerging evidence suggests that tDCS could potentially modulate cerebral blood
flow, particularly affecting motor function in stroke and treating Alzheimer’s
disease. Also, there are certain mechanisms based on the pathogenesis. For
example, tDCS may impact the production and degradation of A
We identified significant heterogeneity (I2
Thus, we recommend that future studies conduct subgroup analyses based on predefined factors (e.g., etiology or tDCS protocol) or meta-regressions to examine the influence of continuous variables (e.g., mean age and baseline scores) on effect size to explore the sources of heterogeneity. We urge the field to develop and adopt consensus-based tDCS protocols for specific neurological disorders. Concurrently, primary studies must rigorously adhere to reporting guidelines, such as the template for intervention description and replication (TIDieR) checklist [113] to ensure the complete and transparent documentation of all intervention details. In conclusion, the high heterogeneity observed in this study does not necessarily challenge the potential efficacy of tDCS but rather highlights that its effects are significantly modulated by protocol choices and patient factors. Acknowledging and systematically investigating these sources of variation are critical next steps toward refining tDCS into a reliable and precise therapeutic tool.
The quality of the methodology and supporting evidence was crucial for our conclusion. Compared to other health endpoints, literature on upper extremity motor function in stroke and on the 8-MWT in cerebellar ataxia demonstrated high methodological and evidential quality according to AMSTAR 2 and GRADE assessments. In contrast, certain studies focusing on stroke, Alzheimer’s disease, Parkinson’s disease, epilepsy, and migraine had notable methodological shortcomings. These findings underscore the need for cautious interpretation and highlight areas where future research should aim to reduce variability and strengthen evidence quality.
The volume of literature and the availability of sufficient demographic and clinical data were critical. The health endpoints for Alzheimer’s disease, cerebellar ataxia, fibromyalgia, epilepsy, disorders of consciousness, multiple sclerosis, and migraine each included just one systematic review and meta-analysis, which could reduce the credibility of the results. Additionally, reanalysis showed no association between tDCS and epilepsy or multiple sclerosis. Due to insufficient data (mean, standard deviation, and sample size) for reanalysis by HKSJ, some health endpoints, such as spinal cord injury, traumatic brain injury, headache, and central neuralgia, were excluded.
In the reanalysis, the new estimated 95% CI was generally narrower than the 95% PI, likely because the 95% PI accounts for variability in individual observations. Moreover, the 95% PI range included zero, indicating that tDCS efficacy was highly variable. This meant that the effectiveness of tDCS was unpredictable and could be negative in certain medical circumstances. Most included studies involved small sample sizes below 800, leading to potential publication bias, except for two meta-analyses [32, 33]. Thus, we conducted Egger’s test to address this limitation. Nevertheless, most meta-analyses incorporated fewer than 10 RCTs, preventing their application. Although some studies were not eligible for review using Egger’s test, publication bias could be tested by funnel plot with contours and correction using the trim-and-fill method. This indicated that while selective reporting or unpublished small-sample studies may exist, they did not significantly impact the overall conclusions.
This umbrella review suggests that future research should focus on the efficacy of tDCS on motor function in stroke, Parkinson’s disease, epilepsy, and multiple sclerosis patients. It also calls for more RCTs testing the efficacy of tDCS in patients with Alzheimer’s disease, cerebellar ataxia, fibromyalgia, epilepsy, disorders of consciousness, multiple sclerosis, and migraine. We encourage studies to offer more detailed information for performing secondary research. For example, future primary meta-analyses on tDCS should prioritize sensitivity analyses to identify the sources of the observed heterogeneity. Investigating moderators, such as stimulation parameters (intensity, target, duration, and sessions) and patient demographics, will be essential for developing personalized and optimized tDCS protocols. Secondary research is also recommended to analyze multiple effect sizes, assess heterogeneity, and thoroughly report publication bias.
In conclusion, this umbrella review systematically summarized a vast amount of existing evidence from published systematic reviews and meta-analyses. We found that tDCS was associated with improvements in a majority of the health outcomes evaluated in multiple neurological disorders, and it exhibited a favorable safety profile. However, the strength of this evidence was often limited, necessitating further high-quality research to confirm the efficacy of tDCS for specific conditions. Further studies should validate the therapeutic potential of tDCS in the reported neurological conditions, investigate additional neurological health outcomes, and explore the underlying mechanisms of tDCS effects.
GBD, global burden of disease; tDCS, transcranial direct current stimulation; PRISMA, preferred reporting items for systematic reviews and meta-analyses; PROSPERO, prospective register of systematic reviews; CINAHL, cumulative index to nursing and allied health literature; HD-tDCS, high-definition transcranial direct current stimulation; HKSJ, hartung-knapp-sidik-jonkman; AMSTAR 2, measurement tool to assess systematic reviews 2; GRADE, grades of recommendations, assessment, development, and evaluation; MD, mean difference; SMD, standardized mean difference; 95% CI, 95% confidence interval; 95% PI, 95% prediction interval; MoCA, montreal cognitive assessment test; MMSE, mini-mental state examination; LOTCA, loewenstein occupational therapy cognitive assessment; MBI, modified barthel index; HAMD, hamilton depression Scale; BDI, beck depression inventory; SADQ-H, stroke aphasic depression questionnaire hospital Version; SDS, self-Rating depression scale; FMA-UE, upper extremity fugl–meyer assessment; ARRT, action research arm test; BI, barthel index; FMA-LE, lower extremity fugl–meyer assessment; MAS, modified ashworth scale; TUG/TUGT, timed up and go test; FAC, functional ambulation category; DOSS, dysphagia outcome severity scale; MMASA, modified mann assessment of swallowing ability; FOIS, functional oral intake scale; FDS, functional dysphagia scale; VFSS, video fluoroscopic swallowing study; LBT, line bisection test; UPDRS-I, unified PD rating scale I; SCOPA, scales for outcomes in Parkinson’s Disease; PD-MCI, Parkinson’s disease with mild cognitive impairment; DS-F, Digit Span-Forward; S-IT, stroop interference test; MODA, milan overall dementia assessment; SARA, Scale for Assessment and Rating of Ataxia; FIQ-R, modified fibromyalgia questionnaire; PCP:S, profile of chronic pain:screen; HAM-D, Hamilton Depression Rating Scale; BDI-II, Beck Depression Inventory-II; FIQ, fibromyalgia questionnaire; CRS-R, coma recovery scale–revised; 2MWT, 2-minute walk Test; 25FWT, 25-foot walk test.
The original contributions presented in this study are included in the article and supplementary material. Further inquiries can be directed to the corresponding author.
TY, YS, YL, SL, XT, WT, YZ and YK were involved in the original conceptualization. TY, YS, YL and SL were responsible for developing the study methodology. TY, YS and YL did the literature search. SL, XT, WT and YZ were responsible for data curation. TY and YS did the formal statistical analysis. TY wrote the original draft. YS and YK edited and reviewed the manuscript. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
We would like to thank MogoEdit for its English editing during the preparation of this manuscript.
This research received no external funding.
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/JIN47145.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.