



 , Barbora Kolářová 3,†, Petr Kolář 3, David Krahulík 4,5, Ahmed Naser Mohamed Afifi 1, Pavel Otruba 1,*
, Barbora Kolářová 3,†, Petr Kolář 3, David Krahulík 4,5, Ahmed Naser Mohamed Afifi 1, Pavel Otruba 1,* , Martin Nevrlý 1,*
, Martin Nevrlý 1,*1 Department of Neurology, University Hospital Olomouc, 779 00 Olomouc, Czech Republic
2 Department of Neurology, Faculty of Medicine and Dentistry of Palacký University Olomouc, 779 00 Olomouc, Czech Republic
3 Department of Rehabilitation, University Hospital Olomouc, 779 00 Olomouc, Czech Republic
4 Department of Neurosurgery, University Hospital Olomouc, 779 00 Olomouc, Czech Republic
5 Department of Neurosurgery, Faculty of Medicine and Dentistry of Palacký University Olomouc, 779 00 Olomouc, Czech Republic
†These authors contributed equally.
Abstract
Parkinson’s disease (PD) is a progressive neurodegenerative disorder characterized by motor and non-motor symptoms. Deep brain stimulation (DBS) of the subthalamic nucleus (STN) is a recognized treatment for advanced PD, yet its impact on gait parameters remains variable. The aim of this prospective study was to evaluate changes in spatiotemporal gait parameters following DBS-STN in patients with advanced PD.
Thirty patients with advanced PD underwent bilateral DBS-STN. Gait assessments were performed preoperatively and three months postoperatively using a pressure-sensitive treadmill under three walking speed conditions (slow, optimal and fast). Spatiotemporal gait parameters (as walking speed, double-stance phase, cadence, step length, stance phase duration) and derived values, such as asymmetry of both step length and stance phase, were analyzed with respect to the clinically better and worse limbs defined in accordance with Movement Disorder Society Unified Parkinson’s Disease Rating Scale (MDS-UPDRS).
No significant changes in walking speed, cadence, or double stance phase duration comparing gait characteristics pre- and postoperatively were found. Significant improvements were found in step length for the clinically worse limb at slow and optimal walking speeds and in stance phase duration for the clinically better limb at fast walking speed. Additionally, asymmetry in both step length and stance phase duration decreased at the fast walking speed after stimulation. For all other parameters evaluated in other walking speeds, the differences were not statistically significant.
DBS-STN combined with medication had limited overall effects on spatiotemporal gait parameters in patients with advanced PD. However, when the clinically worse and better lower limbs were analyzed separately, selective improvements in step length and stance phase duration, along with reduced gait asymmetry at higher walking speeds were observed. These findings suggest that DBS may modulate specific components of gait control rather than global gait performance, highlighting the importance of individualized assessment in postoperative gait evaluation.
Keywords
- Parkinson’s disease
- deep brain stimulation
- gait disorder
Parkinson’s disease (PD) is the second most common neurodegenerative, progressive disorder. Currently, more than 6 million people live with PD, and given the globally increasing average life expectancy, this number is likely to rise [1]. Gait disturbances are highly prevalent in PD and significantly affect mobility, increase fall risk, and reduce functional independence and quality of life [2].
PD is characterized by both motor and non-motor symptoms [1], and although both can influence gait, motor symptoms remain the predominant contributors to gait abnormalities. In the early stage, patients present with motor impairments including tremor, bradykinesia, hypokinesia, rigidity, dystonia, reduced associated movements (synkineses), and postural abnormalities such as forward trunk flexion and impaired trunk counter-rotation. These symptoms are related to impaired spatiotemporal gait characteristics including reduced gait speed, decreased step length, prolonged stance phase duration and double support time, and decreased cadence, compared to healthy individuals [3, 4, 5]. In the late stage, additional features that impair gait may occur, including Pisa syndrome, camptocormia, abduction of the upper limbs with elbow flexion, difficulties rising from a seated position, postural instability, progressive loss of gait fluency, freezing of gait (FOG) and falls, which further contribute to the worsen gait patterns and progressive deterioration of walking ability [1, 6]. Motor symptoms typically present asymmetrically, with one side of the body being more affected. The limb with greater impairment is clinically designated as the worse limb, whereas the contralateral side is considered the better limb [7]. This asymmetry also affects gait characteristics; however, asymmetry is still insufficiently accounted for in many gait studies focusing on patients with PD. Also, identifying the degree of asymmetry is essential for individualized rehabilitation strategies and disease monitoring. The assessments of spatiotemporal gait parameters are critical for monitoring disease progression and evaluating therapeutic interventions such as deep brain stimulation (DBS). A recent scoping review highlighted the importance of integrating kinematic and kinetic data in PD gait analysis [4], which can be reliably captured using pressure-sensitive treadmill systems [4].
The pathophysiology of gait impairment in PD involves dysfunction across multiple neural substrates, including the basal ganglia, cerebellum, brainstem structures such as the pedunculopontine nucleus (PPN), and peripheral nervous system involvement [3]. The main pharmacological treatments influencing PD symptoms are levodopa and dopamine agonists, which alleviate symptoms by supplementing or mimicking dopamine, the deficiency of which is the primary cause of PD motor features. These medications improve tremor, bradykinesia, and hypokinesia, thereby positively influencing gait. However, after several years of treatment, motor fluctuations typically develop, including ‘ON–OFF’ states, wearing-off, and dyskinesias [8], FOG occurring primarily in the ‘OFF’ state, when dopaminergic medication is ineffective, or in response to specific triggers such as turning, passing through narrow spaces, cognitive load, or emotional factors [1, 6]. In selected cases meeting indication criteria, these complications can be addressed by continuous infusion therapies (levodopa or apomorphine pump systems) or by DBS, usually targeting the subthalamic nucleus (STN) or, alternatively, the internal globus pallidus [8, 9]. Bilateral DBS of the STN is a widely recognized therapy for advanced PD, often providing long-term reduction in rigidity, bradykinesia, tremor, and dyskinesia, and allowing for a reduction of levodopa equivalent daily dose [10].
Nevertheless, improvements in other symptoms, such as gait and postural stability, are often only temporary or absent [11, 12]. Several studies demonstrate that DBS can improve specific biomechanical gait parameters—such as increasing step length, reducing cadence, and shortening the double-stance phase, resulting in enhanced gait stability [13]—its overall impact on gait remains inconsistent, as some patients exhibit measurable improvement while others show little change or even deterioration in gait function due to variability in neural responses and stimulation settings [14].
During levodopa treatment cycles, performance differences between limbs are observable, with the clinically worse limb showing more severe symptoms during ‘OFF’ periods [15]. This limb-specific vulnerability highlights the importance of considering asymmetry when evaluating therapeutic interventions. Therefore, in this study, we examined the effects of DBS-STN (deep brain stimulation of the subthalamic nucleus) in patients with advanced PD. We hypothesised that DBS-STN would significantly improve key spatiotemporal gait parameters—specifically increased gait speed and step length, and reduced stance and double-stance phase durations—with greater improvements expected for the clinically worse limb.
All patients met the UK Brain Bank criteria for diagnosis of idiopathic PD. All patients met the indication criteria for DBS-STN treatment and underwent bilateral implantation of DBS-STN. All patients were fully informed about the procedure and the procedure was performed by a single surgeon and the same team of neurologists. The indication, inclusion criteria for DBS and the surgical procedure were described in our previously published papers [16, 17, 18]. In all cases DBS treatment was indicated as standard therapy.
After signing informed consent, 30 patients with advanced PD in the stage of late motor complications indicated for DBS-STN were enrolled in the study between March 2015 and May 2024. The study was approved by the local ethics committee in accordance with the principles and recommendations of the Declaration of Helsinki, 1975 and later revisions.
The participants were required to walk independently overground for at least 10 meters without assistance and to sustain treadmill walking for at least 2 minutes, with or without handrail support. Additionally, they had no neurological, orthopedic, or severe visual impairments that could affect gait for reasons other than PD.
All patients were evaluated using the Movement Disorder Society Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) [19] to quantify motor symptoms (MDS-UPDRS III) and motor complications (MDS-UPDRS IV), always in the ‘ON’-medication state (baseline) and three months after implantation of DBS-STN in the ‘ON’-medication/‘ON’-stimulation state. Demographic and clinical data regarding the MDS-UPDRS are summarized in Table 1.
| Number of participants (female/male) | 30 (10/20) |
| Age [years] (SD) | 61.40 (5.77) |
| Duration of disease (years) | 9.07 |
| More affected side (Right/Left) | 15/15 |
| Levodopa equivalent dosage preoperatively (mg) | 1241.03 |
| Levodopa equivalent dosage 3 months postoperatively (mg) | 636.40 |
| MDS-UPDRS III preoperatively in ‘ON’ state | 19.33 |
| MDS-UPDRS III 3 months postoperatively in ‘ON’ state | 9.57 |
| MDS-UPDRS IV preoperatively | 4.13 |
| MDS-UPDRS IV 3 months postoperatively | 1.67 |
SD, standard deviation; MDS-UPDRS, Movement Disorder Society Unified Parkinson’s Disease Rating Scale.
All patients underwent assessment on the Zebris FDM-T treadmill system (Isny) (SN: 0002-1146, Zebris Medical GmbH, Isny im Allgäu, Germany), which was performed before DBS implantation (1–5 days prior). This assessment was designated V1 in the study, and at 3 months after DBS activation, i.e., 4 months post-surgery, it was designated V2 in the study.
The patients were examined in the ‘ON’-medication state after administration of their standard medication doses, without using a suprathreshold dose. Additionally, the second assessment was additionally performed with the DBS system activated and optimally adjusted (pulse width 60 µs, pulse frequency 130 Hz, voltage individualized according to clinical effect, typically around 3.0 V) [16]. The medication regimen was adjusted concurrently with DBS.
Gait evaluation was performed under three distinct self-selected walking speed conditions. The participants were instructed to walk at a subjectively slow pace, followed by their comfortable self-selected walking speed, and finally at their maximal tolerated walking speed. Each condition was assessed separately to capture variations in spatiotemporal gait parameters across different speed profiles.
Gait analysis was conducted using the Zebris FDM-THL pressure-sensitive treadmill (Zebris Medical GmbH, Isny, Germany), which provides a standardized and controlled testing environment suitable for clinical and research applications. The system captures detailed plantar pressure distribution during walking, expressed in Newtons per square centimeter (N/cm2), allowing for precise quantification of spatiotemporal gait parameters, such as step length, stance and swing phases, cadence, and double-stance duration. Because the treadmill allows controlled walking speeds and highly repeatable test conditions, it supports reliable comparisons across multiple assessment points and offers a high-resolution method for detecting subtle changes in gait biomechanics. The Zebris FDM-THL system combines pressure-mapping technology with standardized treadmill-based locomotion, providing an objective and reproducible framework for evaluating DBS-related gait modifications in Parkinson’s disease patients [13]. This particular Zebris model provides fixed, pre-set belt speeds and does not adapt its speed during walking.
All assessments were performed with the participants walking barefoot to ensure consistent sensor contact and data accuracy. All participants were capable of initiating, maintaining, and terminating gait on the treadmill without assistance. All patients were secured in an overhead safety harness during treadmill walking, and gait was not externally paced, ensuring that step timing and rhythm were self-selected and not influenced by external cues [13].
The participants walked on the Zebris FDM-THL in self-paced mode; once they reached their subjectively slow, comfortable, or fast speed, the treadmill belt speed was fixed. At each of the three speeds, the participants completed at least 1 minute of familiarization followed by 1 minute of recording. Steady state was determined by experienced assessors after the predefined familiarization interval. There was a 2-minute break between the changes to rest.
For each condition, the mean and standard deviation (SD) of all recorded spatiotemporal gait parameters across the 1-minute measurement interval were included in the final analysis. For the purpose of final analysis, relevant gait parameters were evaluated with respect to the clinically better and worse limb, as determined by motor scores from the MDS-UPDRS III (items 3.3–3.8 and 3.15–3.17) [19].
Evaluated spatiotemporal gait parameters included:
Walking speed—self-selected walking speed subjectively in slow mode, comfortable mode and maximal tolerated.
Double-stance phase—the percentage of the gait cycle during which both feet are simultaneously in contact with the treadmill belt.
Cadence—the number of steps per minute, derived from stride time—the interval between successive heel contacts of the same foot, measured in seconds.
Step length—for each limb defined as the linear distance between the heel contact of one foot and the subsequent heel contact of the contralateral foot on the treadmill belt. Clinically better and worse limbs were considered in the analysis for this parameter.
Asymmetry of step length—relative percentage difference between the step lengths of the two limbs. Values closer to zero, indicate greater symmetry in the lengths of the stance phase.
Stance phase duration—for each limb expressed as a percentage of the total gait cycle, representing the time during which the contralateral limb is not in contact with the treadmill surface. Clinically better and worse limbs were considered in the analysis for this parameter.
Asymmetry of stance phase—the relative percentage difference between the duration of the stance phase of the two limbs. Values closer to zero, indicate greater symmetry in the gait pattern, reflecting more equivalent stance phase durations.
All calculations were performed in R software-version 4.4.1 (2024-06-14,
Foundation for Statistical Computing, Vienna, Austria) [20]. The normality of data
distribution was assessed using the Shapiro–Wilk test. When the assumption of
normality was violated, the paired Wilcoxon signed-rank test was applied; in
other cases, the paired t-test was applied. Statistical analyses were
performed separately for each variable using either the t-test or the
Wilcoxon test, without conducting comparisons between variables (e.g., slow vs.
optimal). For normally distributed data, the paired t-test was used. The
data contained missing values, which were imputed using the K-nearest neighbors
(KNN) algorithm [21], employing functions available in the R package caret. The
data set of step length contained altogether 2.78% of missing values (10
values), the data set of the stance phase contained 2.22% of missing values (8
values). Test evaluation was performed at the significance level of p
No differences were found between V1 and V2 for walking speed, double stance phase duration or cadence. Statistics revealed no significant differences in any of these parameters between V1 and V2 in minimum, optimal, or maximum walking speeds. For the results, see Table 2.
| SGS | Time point of the assessment | Mean (SD) | Median (IQR) | Statistical test | |
| Walking speed [m/s] | Slow | V1 | 0.37 (0.08) | 0.42 (0.31–0.42) | W = 7.00 (p = 0.136) |
| V2 | 0.38 (0.07) | 0.42 (0.35–0.42) | |||
| Optim | V1 | 0.69 (0.21) | 0.83 (0.56–0.83) | W = 10.00 (p = 0.542) | |
| V2 | 0.70 (0.20) | 0.83 (0.44–0.83) | |||
| Fast | V1 | 1.00 (0.37) | 1.25 (0.69–1.25) | W = 14.00 (p = 0.264) | |
| V2 | 1.02 (0.34) | 1.25 (0.69–1.25) | |||
| Double stance phase duration [% of gait cycle] | Slow | V1 | 37.60 (7.47) | 37.30 (35.05–40.45) | t = –1.23 (p = 0.885) |
| V2 | 39.60 (5.95) | 38.65 (36.68–41.00) | |||
| Optim | V1 | 29.73 (5.49) | 29.70 (27.80–32.67) | W = 205.00 (p = 0.611) | |
| V2 | 30.31 (5.13) | 29.90 (26.77–33.38) | |||
| Fast | V1 | 26.41 (5.30) | 25.95 (22.97–28.59) | W = 216.50 (p = 0.513) | |
| V2 | 25.99 (6.32) | 26.17 (21.64–29.62) | |||
| Cadence [steps/minute] | Slow | V1 | 84.30 (22.20) | 81.50 (69.00–98.50) | t = 1.51 (p = 0.071) |
| V2 | 75.07 (19.67) | 73.50 (60.75–88.00) | |||
| Optim | V1 | 100.70 (21.08) | 103.50 (94.00–112.75) | t = –0.13 (p = 0.552) | |
| V2 | 101.13 (18.31) | 101.50 (86.25–113.25) | |||
| Fast | V1 | 113.92 (19.02) | 114.00 (103.00–128.50) | t = –0.08 (p = 0.533) | |
| V2 | 114.20 (22.27) | 114.50 (103.25–126.00) |
Legend: SGS, self-selected gait speed; V1, gait assessment before DBS
implantation; V2, gait assessment 3 months after DBS activation; Slow,
subjectively slow self-selected walking speed [m/s]; Optim, comfortable
self-selected walking speed [m/s]; Fast, subjectively maximal tolerated walking
speed [m/s]; W, Wilcoxon; t, T-test; p, significant
difference at the significance level of p
Significant improvements in step length for the clinically worse limb were observed for slow and optimal walking speeds; for the fast walking speed, the level of significance reached slightly above 0.05. A significant difference was found in the clinically better limb for stance phase duration between V1 and V2 at fast walking speed. Additionally, asymmetry in both step length and stance phase duration decreased at the maximal tolerated walking speed within the tested patient group. For all other evaluated parameters—including step length, stance phase duration, and gait asymmetry—during minimal and comfort self-selected walking speeds, differences between V1 and V2 were not statistically significant. Detailed results are presented in Table 3. Data distributions with indicated statistical significance are presented in Figs. 1,2.
| Clinically worse limb | |||||
| SGS | Time point of the assessment | Mean (SD) | Median (IQR) | Statistical test | |
| Step length [cm] | Slow | V1 | 27.38 (8.18) | 26.00 (22.25–32.50) | t = –1.75 (p = 0.046) |
| V2 | 31.37 (9.94) | 31.00 (23.75–37.75) | |||
| Optim | V1 | 40.03 (9.92) | 40.00 (34.50–47.00) | t = –2.01 (p = 0.027) | |
| V2 | 43.63 (10.97) | 45.00 (35.25–51.00) | |||
| Fast | V1 | 49.99 (15.21) | 54.50 (40.25–62.80) | t = –1.68 (p = 0.052) | |
| V2 | 53.39 (14.41) | 58.00 (42.00–63.00) | |||
| Stance phase duration [% of gait cycle] | Slow | V1 | 68.11 (3.93) | 67.55 (66.50–69.95) | t = –1.75 (p = 0.955) |
| V2 | 69.69 (3.79) | 69.50 (67.20–71.90) | |||
| Optim | V1 | 63.76 (4.67) | 64.35 (62.05–66.45) | W = 165.50 (p = 0.917) | |
| V2 | 65.11 (3.70) | 64.60 (62.92–67.27) | |||
| Fast | V1 | 62.83 (3.00) | 62.30 (60.85–64.47) | W = 184.00 (p = 0.769) | |
| V2 | 62.94 (4.10) | 62.85 (60.75–64.38) | |||
| Clinically better limb | |||||
| Mean (SD) | Median (IQR) | ||||
| Step length [cm] | Slow | V1 | 27.55 (7.78) | 28.00 (22.25–31.00) | t = –1.61 (p = 0.059) |
| V2 | 31.64 (10.10) | 33.00 (24.75–38.50) | |||
| Optim | V1 | 41.07 (10.19) | 43.50 (40.00–46.00) | t = –1.62 (p = 0.058) | |
| V2 | 43.70 (9.97) | 45.00 (36.25–51.25) | |||
| Fast | V1 | 50.83 (14.84) | 56.00 (43.75–61.00) | t = –0.61 (p = 0.275) | |
| V2 | 52.11 (14.39) | 57.40 (39.50–62.00) | |||
| Stance phase duration [% of gait cycle] | Slow | V1 | 69.41 (4.89) | 69.75 (66.95–72.55) | W = 213.00 (p = 0.660) |
| V2 | 70.07 (3.78) | 69.90 (67.38–72.38) | |||
| Optim | V1 | 64.45 (5.56) | 65.45 (63.62–66.88) | W = 205.00 (p = 0.611) | |
| V2 | 65.26 (2.63) | 64.70 (63.28–67.25) | |||
| Fast | V1 | 63.78 (3.02) | 63.65 (61.68–65.95) | t = 1.91 (p = 0.033) | |
| V2 | 62.87 (3.08) | 62.35 (60.82–64.85) | |||
| Asymmetry | |||||
| Mean (SD) | Median (IQR) | ||||
| Step length [cm] | Slow | V1 | –0.70 (17.94) | 3.40 (–9.64–11.21) | t = 0.25 (p = 0.400) |
| V2 | –1.84 (21.02) | –1.16 (–11.92–7.49) | |||
| Optim | V1 | 0.80 (15.59) | 2.39 (–4.64–8.46) | W = 255 (p = 0.212) | |
| V2 | –0.52 (15.83) | 0.83 (–6.16–6.52) | |||
| Fast | V1 | 1.91 (5.19) | 2.44 (–2.91–5.03) | t = 2.08 (p = 0.023) | |
| V2 | –3.36 (12.20) | –1.66 (–7.51–2.68) | |||
| Stance phase duration [% of gait cycle] | Slow | V1 | 1.55 (6.94) | 1.52 (–1.55–5.64) | t = 0.74 (p = 0.232) |
| V2 | 0.32 (6.72) | 0.15 (–2.42–2.90) | |||
| Optim | V1 | 0.78 (5.70) | 0.94 (–2.03–3.22) | W = 279 (p = 0.175) | |
| V2 | 0.13 (5.93) | 0.15 (–2.66–3.09) | |||
| Fast | V1 | 1.42 (3.94) | 1.04 (–0.21–3.01) | t = 1.75 (p = 0.045) | |
| V2 | –0.14 (4.91) | 0.17 (–1.90–2.11) | |||
Legend: p, significant difference at the significance level of
p
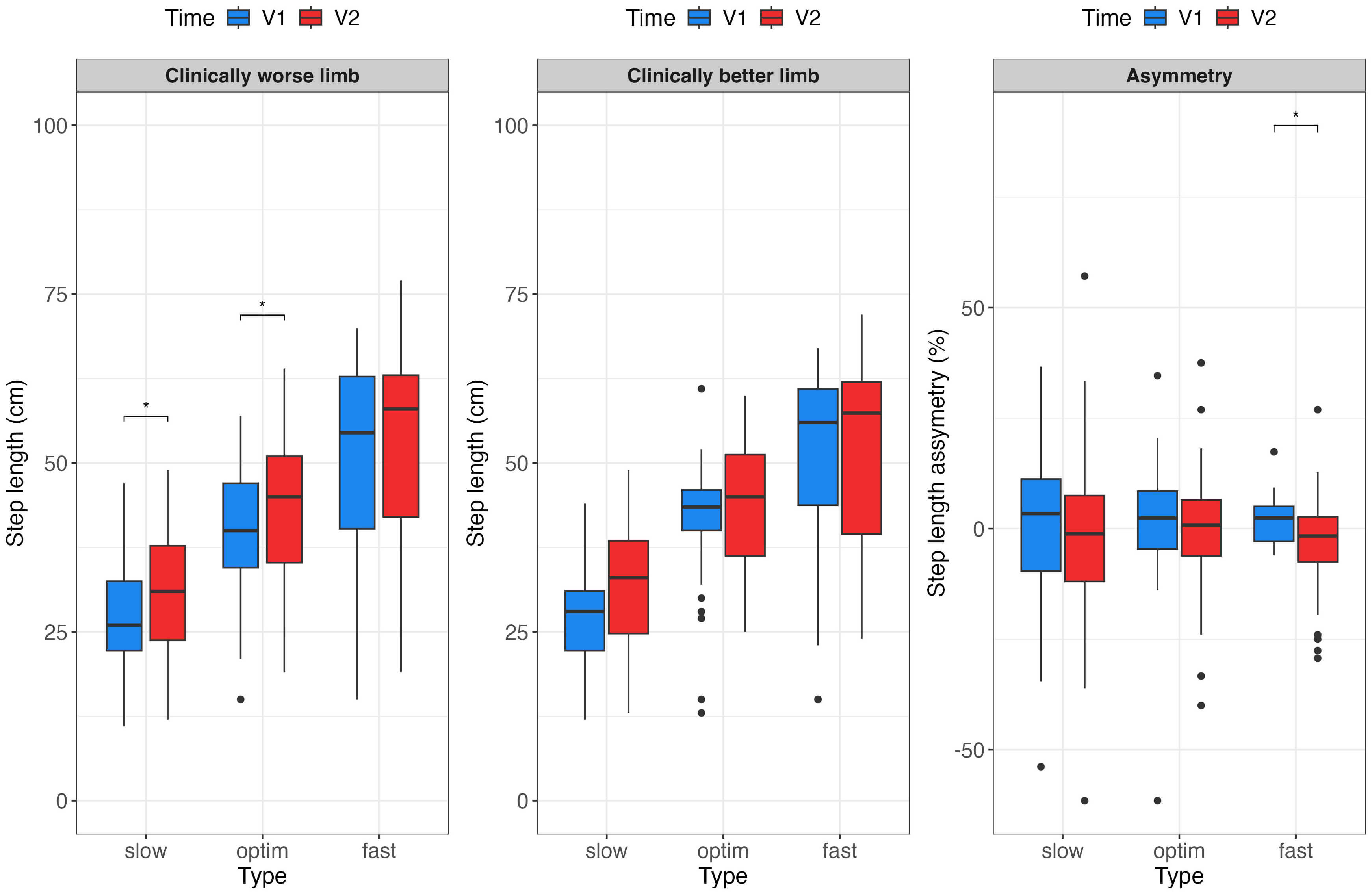 Fig. 1.
Fig. 1.
Boxplots showing medians, the first and third quantiles and
outliers for comparison of step length (cm) of clinically worse and better limbs,
together with asymmetry of step length for both limbs (%). * significance
level of p
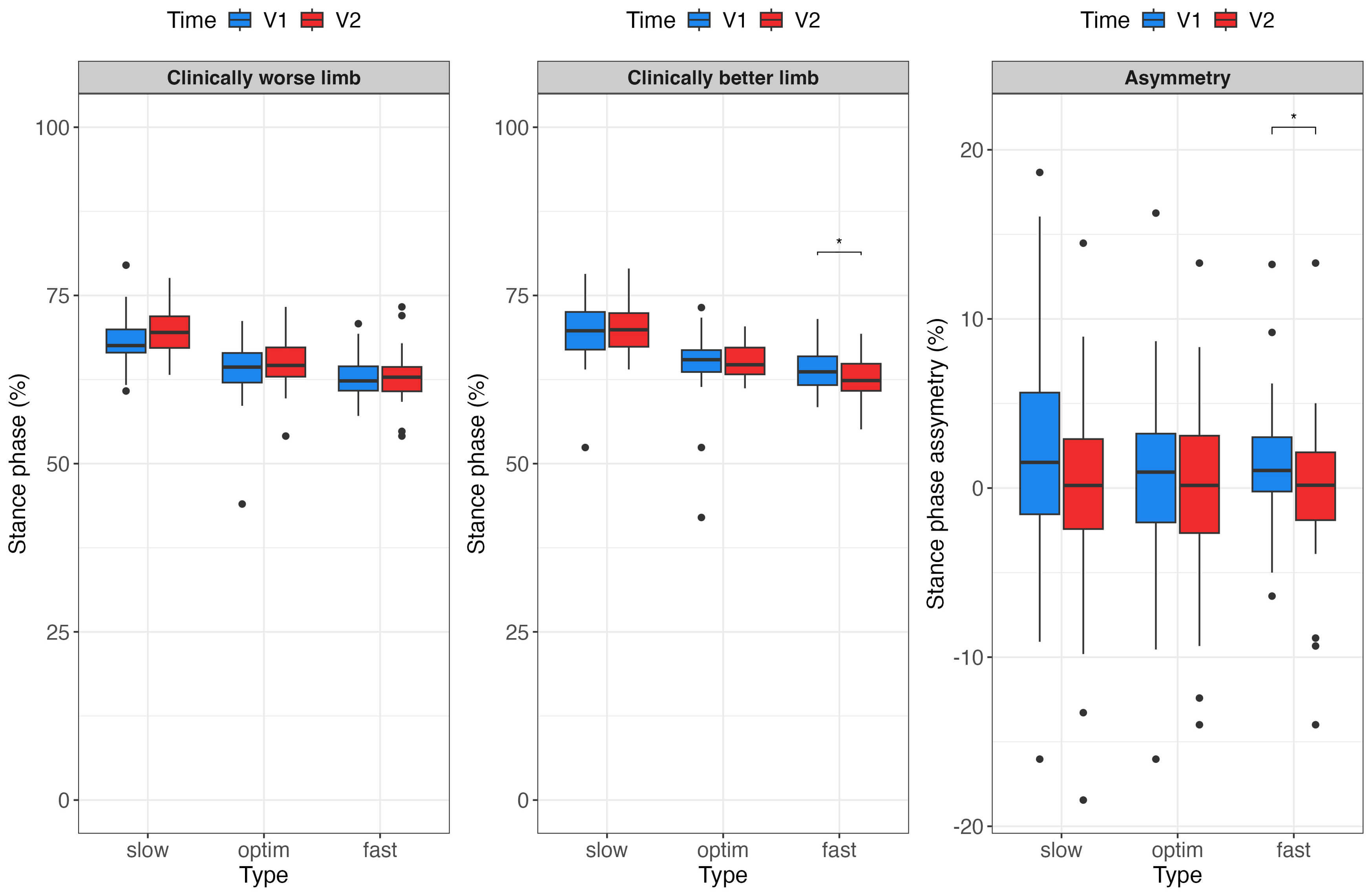 Fig. 2.
Fig. 2.
Comparison of stance phase duration of the clinically worse and
better limbs, together with asymmetry of stance phase duration for both limbs
(%), measured at minimal, optimal and maximal walking speed and at times V1
(blue) and V2 (red). * significance level of p
Significant improvements were found for parts (III and IV) of the MDS-UPDRS score (for details see Table 4).
| MDS-UPDRS score | ||||
| Time point of the assessment | Mean | Med | Statistical test | |
| III | V1 | 19.33 (9.30) | 18.00 (13.25–22.75) | W = 434.00 (p |
| V2 | 9.57 (5.65) | 8.00 (5.25–14.00) | ||
| IV | V1 | 4.13 (1.74) | 4.00 (3.00–5.00) | W = 384.50 (p |
| V2 | 1.67 (1.52) | 1.50 (0.00–3.00) | ||
In accordance with the study results, the DBS-STN combined with medication had limited overall effects on spatiotemporal gait parameters in patients with advanced PD. No significant changes were found in walking speed, cadence, or double-stance phase duration comparing gait characteristics preoperatively and postoperatively.
On the contrary, our study demonstrates that in patients receiving established therapy combining DBS-STN targeted to the more affected limb and medication, step length significantly increases in the clinically worse limb at slow and optimal gait velocities. Additionally, asymmetry in both step length and stance phase duration decreased at the fast walking speed after stimulation.
Although our study did not directly assess postural stability, reduced gait asymmetry may reflect components of more efficient postural control, as the asymmetry and postural-control domains are closely linked. Free-living gait studies demonstrate that abnormalities in asymmetry and postural control co-occur and contribute to gait impairment in PD [22, 23]. In our study, however, these mechanisms can only be hypothesized, as postural control itself was not measured.
A similar effect was reported by Cani et al. [24], who used an 18-meter free walk and the Timed Up and Go test, observing mild to moderate improvements in step length and gait symmetry with combined therapy. Unlike our study, however, they also noted improvements in gait speed and cadence. This difference may be partially explained by methodological variations, specifically regarding the self-selected speed of treadmill walking in our study vs. hallway walking in theirs.
Also, Johnsen et al. [25] reported a reduction in asymmetry, although they defined the clinically better and worse limb based on a combination of the MDS-UPDRS scores and quantitative gait analysis. Cadence, as in our results, did not improve, but they observed an increase in gait speed. These findings cannot be fully compared with ours, as their patients were always assessed without medication, with DBS-STN in either the ‘ON’ or ‘OFF’ state. Further limitations of their study include the small sample size (n = 8) and the fact that DBS settings could be adjusted only a few hours prior to the assessment.
In contrast, a study by Ravi et al. [26] reported different findings, describing an increase in step time asymmetry following the implementation of DBS-STN compared to the preoperative state, indicating a potential negative impact on gait. Differences in all other gait characteristics between pre- and postoperative conditions were negligible. Notably, that study [26] included patients who already exhibited postural instability prior to surgery. Another distinction from our study lies in the gait assessment methodology: gait was evaluated using body-worn sensors while participants walked in a figure-eight pattern, requiring them to navigate around two positioned objects. Moreover, the study involved relatively small patient cohorts, and baseline gait impairments may not have been present to a comparable extent across participants. Postoperatively, optimization of stimulation parameters and adjustment of dopaminergic therapy—undertaken to achieve the best possible overall clinical condition rather than targeting gait specifically—could have contributed to the variability in outcomes.
The study by Barbieri et al. [27] describes asymmetry, deterioration in kinematic parameters (joint angles), and step length of the more affected limb in individuals with PD, both in ‘ON’ and ‘OFF’ medication states. Although levodopa improves certain motor symptoms, it appears insufficient to correct kinematic asymmetry. In healthy older adults, no significant joint kinematic asymmetries were found, indicating that such asymmetry is not a typical feature of physiological aging. The authors also hypothesize that the asymmetry observed in individuals with PD represents a pathological characteristic that may negatively impact the efficiency and stability of locomotion during gait.
A likely explanation for the absence of DBS-related differences in walking speed is the “treadmill effect”. Treadmill walking provides continuous external rhythmic cueing through belt motion and visually predictable forward flow, which can stabilize gait patterns and reduce natural stride-to-stride variability, thereby masking potential DBS-related improvements. External cueing is known to enhance gait performance in PD patients and can attenuate differences between stimulation conditions [28]. This may explain why our findings diverge from studies such as Roper et al. [29], who reported significant DBS-related improvements in overground gait velocity.
Roper et al. [29] noted that DBS-STN can improve gait speed both independently and in combination with medication. Cani et al. [24] further demonstrated that stimulation even surpassed the effect of levodopa in enhancing gait speed, step length, and turning ability. Conversely, levodopa showed greater efficacy in reducing step length variability and asymmetry, whereas stimulation alone had a limited effect in this regard.
The clinical relevance of gait speed is highlighted by studies on comfortable gait speed (CGS), also referred to as self-selected walking speed, which is widely recognized as a reliable indicator of functional mobility and fall risk in patients with PD [30, 31]. Typical gait speed in PD patients is often below 1.1 meters per second (m/s), with values below this threshold associated with a twofold increase in fall risk [31]. Weiss et al. [32] demonstrated that quantitative gait measures, including gait speed, predict fall risk even in early-stage PD, supporting their integration into multimodal clinical assessments. Parkinsonian gait is typically characterized by reduced step length, increased variability, and impaired rhythmicity, with these deficits exacerbated at slower walking speeds, reflecting impaired automaticity and rhythm [33].
Finally, differences between studies may also be attributed to electrode placement, selection of optimal contacts, and adjustment of stimulation parameters (pulse width, frequency, amplitude), as emphasized by Wodarg et al. [34]. Additionally, while treadmill walking imposes higher demands than floor walking, it enables immediate and detailed evaluation of spatiotemporal gait parameters, which represents an important methodological advantage. The length of follow-up also account for differences in study results. In the presented study, the 3-month follow-up was chosen as sufficient, as the DBS stimulation parameters were no longer significantly adjusted and the antiparkinsonian therapy was not changed in any of the subjects. Over the 3-month interval, no significant progression of the disease can be expected that would significantly affect the clinical condition of the patients.
Although STN or GPi DBS improves global motor symptoms, as verified by the MDS-UPDRS III questionnaire, its effects on gait and postural control are limited. DBS primarily modulates the basal ganglia–thalamo–cortical nerve pathways, suppressing pathological beta-band synchronization and thereby improving bradykinesia, rigidity and tremor—symptoms strongly associated with dopaminergic dysfunction [35, 36]. In contrast, gait, balance and FOG arise from dysfunction in predominantly non-dopaminergic networks, which include the pedunculopontine nucleus (PPN), the wider mesencephalic locomotor area (MLR), cerebellar circuits and spinal pattern generators [37, 38, 39]. As a result, significant improvements in MDS-UPDRS III after DBS-STN can coexist with minimal or inconsistent benefits for walking [40].
Several methodological limitations should be considered when interpreting the results of this study: a relatively small number of subjects; a short follow-up period; the absence of more precise assessments of postural stability; and the evaluation of treadmill gait, which differs in some respects from regular floor gait. The sample size was moderate and derived from a single tertiary center, which may limit the generalizability of the findings to the broader PD population. We could also discuss the follow-up interval. A longer follow-up period of 6 months or 1 year might be more reasonable. However, a longer follow-up could present additional limitations due to the possible natural progression of the disease, which could alter gait. The use of posturography or a clinical test of sensory interaction on balance should provide a more accurate for postural stability evaluation. Gait assessment was conducted exclusively in a treadmill environment. Although the Zebris FDM-THL system provides highly controlled and reproducible measurement conditions, treadmill walking does not fully replicate overground gait and caution is warranted when extrapolating these findings to realworld walking conditions.
In accordance with our study results, DBS-STN combined with medication had limited overall effects on spatiotemporal gait parameters in patients with advanced PD. No significant changes were found in walking speed, cadence, or double-stance phase duration when comparing preoperative and postoperative gait performance. These findings indicate that global gait characteristics remained largely unchanged following DBS.
Nevertheless, when gait was analyzed with respect to the clinically better and worse limb, selective improvements emerged. Specifically, step length for the clinically worse limb and stance phase duration for the clinically better limb improved under certain walking conditions, and gait asymmetry decreased at higher walking speeds. These results suggest that DBS-STN may modulate specific components of gait control, even if it does not substantially influence overall gait performance.
The gait asymmetry, shortened step length, and reduced gait speed represent key manifestations of movement impairment in PD, which can be ameliorated by a combination of pharmacotherapy and DBS. Treatment success depends on the individual patient’s response to medication, precise surgical electrode placement, and optimal adjustment of stimulation parameters.
The originality of our study lies in the comprehensive assessment of spatiotemporal gait parameters and the evaluation of DBS-STN in combination with medication under real-life clinical conditions. Unlike our previous study [13], which was conducted on a smaller patient cohort and focused primarily on the relationship between spatiotemporal parameters and the MDS-UPDRS questionnaire scale, the present study included a larger patient sample and additionally analyzed gait asymmetry, providing insights into differences between the clinically better and worse limbs. By examining differences between the clinically better and worse limbs, we provide a more detailed understanding of how DBS influences gait components that may not be evident through global parameters alone. Our findings even highlight the importance of individualized postoperative assessment in evaluating treatment outcomes in advanced PD.
The datasets generated for this study are available on request to the corresponding author.
DS and BK both authors contributed equally to this work. DS, BK and MN wrote the main manuscript. DS, BK, PK, DK, ANMA, PO and MN made clinical evaluations of subjects. BK, DS and PK made investigation on treadmill and evaluation of gait. DK made all surgical procedures. PO and PK made critical review of manuscript. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was approved by the Ethics Committee of the University Hospital Olomouc, file number 159/19, in accordance with the principles and recommendations of the Declaration of Helsinki, 1975 and later revisions. All participants signed informed consent.
The authors would like to thank to Veronika Glogarová, M.A., Department of foreign languages, Faculty of Medicine and Dentistry, Palacký University Olomouc, for proofreading this text. Thanks to Viktoria Nesrstová, MSc, Ph.D., Department of Rehabilitation, University Hospital Olomouc and Department of Informatics and Quantitative Methods, Faculty of Informatics and Management, University of Hradec Králové, for the statistic processing.
Research was supported by Ministry of Health, Czech Republic–conceptual development of research organization (FNOl, 00098892).
The authors declare no conflicts of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.