





 , Zhanhua Liang 3, Zhongrui Yan 2,*
, Zhanhua Liang 3, Zhongrui Yan 2,* , Yiming Liu 1,4,*
, Yiming Liu 1,4,*1 Medical Integration and Practice Center, Cheeloo College of Medicine, Shandong University, 250012 Jinan, Shandong, China
2 Department of Neurology, Jining No. 1 People’s Hospital, Shandong First Medical University, 272000 Jining, Shandong, China
3 Department of Neurology, The First Affiliated Hospital of Dalian Medical University, 116011 Dalian, Liaoning, China
4 Department of Neurology, Qilu Hospital, Cheeloo College of Medicine, Shandong University, 250012 Jinan, Shandong, China
Abstract
Executive function (EF) impairment is a recognized common cognitive deficit in early-onset Parkinson’s disease (EOPD), profoundly impacting patient autonomy and quality of life. While EF-related cognitive decline has been extensively studied in late-onset Parkinson’s disease (LOPD), research on EOPD remains limited. Addressing this gap, this study uniquely employed functional near-infrared spectroscopy (fNIRS), a technique well-adapted for assessing patients with motor challenges, to explore EF-related neural mechanisms in EOPD patients with mild cognitive impairment.
This study included 30 patients with PD, classified into distinct cognitive profiles based on comprehensive assessments of their cognitive function. To assess functional changes in the prefrontal cortex (PFC) we administered a verbal fluency test to evaluate EF during task performance. In the resting state, we recorded neural activity and analyzed the amplitude of low-frequency fluctuations (ALFF) to assess spontaneous brain activity.
During executive tasks, patients with EF-dominant impairment (EOPD-EL) showed increased activation in the dorsolateral prefrontal cortex (DLPFC) and medial prefrontal cortex (mPFC), indicating disrupted balance between the executive and default mode networks. Resting-state analysis revealed reduced spontaneous activity in the ventrolateral prefrontal cortex (VLPFC), suggesting impaired regulatory efficiency in these regions. These findings support the dual syndrome hypothesis in EOPD, with EF dysfunction as a primary deficit that may lead to secondary cognitive challenges.
This study underscores the central role of PFC dysfunction in EOPD-related EF impairment, identifying abnormalities in the DLPFC, mPFC, and VLPFC as key contributors to cognitive decline. These results lay the groundwork for early detection of EF deficits and inform targeted interventions to mitigate cognitive decline in EOPD.
Keywords
- early-onset Parkinson’s disease
- executive function
- prefrontal cortex
- fNIRS
Parkinson’s disease (PD), the second most common neurodegenerative disorder worldwide [1], affects millions. Early-onset Parkinson’s disease (EOPD), though rare, significantly impacts patients’ quality of life and imposes substantial socioeconomic burdens [2]. Occurring during the prime of personal and professional life, EOPD-related cognitive impairments disrupt daily functioning, autonomy, and social roles, often leading to psychological challenges [3, 4]. EOPD has a distinct cognitive impairment profile compared to late-onset Parkinson’s disease (LOPD), with earlier onset, longer duration, and greater clinical heterogeneity [2]. EOPD patients often experience cognitive deficits, particularly in executive function (EF), from early stages, with these deficits persisting longer than in LOPD and deeply impacting daily life and independence [5, 6] and profoundly affecting patients’ daily life and autonomy. Despite previous studies on cognitive aspects of EOPD [3, 5], a significant gap remains in understanding the mild cognitive impairment (MCI) associated with this subtype and its underlying neural mechanisms.
Differentiating EF from other cognitive domains, such as visuospatial skills and memory, is crucial for understanding EOPD’s cognitive profile. EF impairments often appear early in PD, particularly in EOPD, and precede deficits in other cognitive areas [7]. These deficits are strongly linked to functional abnormalities in the prefrontal cortex (PFC), especially the dorsolateral (DLPFC) and medial (mPFC) regions [8, 9]. As the PFC governs EF and integrates working memory, attention, and planning [9], EF impairment frequently affects other cognitive domains. Neuropsychological findings show that EF deficits correlate with impairments in visuospatial and memory functions in PD [10]. Though declines in these areas may sometimes occur independently of EF impairment, they are commonly interconnected [10], suggesting that EF may act as a “coordinator”, with its dysfunction potentially leading to regulatory imbalances and subsequent deterioration in other domains.
EF impairment is an early sign of cognitive decline in PD, persisting throughout disease progression [11]. As the disease progresses, deficits in memory and visuospatial skills tend to worsen alongside ongoing EF decline [12], suggesting that EF dysfunction may be a primary factor leading to impairments in other areas [9]. Neuroimaging study supports this view, with network analyses showing that EF impairment disrupts other cognitive functions by altering brain networks [13]. Therefore, other cognitive impairments, such as those in memory and visuospatial abilities, may be associated with EF dysfunction in EOPD, reflecting the interdependent nature of cognitive processes.
Cognitive impairment in PD is heterogeneous, and the dual syndrome hypothesis categorizes this variation into two types [14, 15, 16, 17]. The first type includes executive and language deficits associated with prefrontal-striatal circuit dysfunction, while the second involves visuospatial, attention, and memory deficits linked to posterior cortical dysfunction. While this framework has been utilized in LOPD [18, 19], its relevance to EOPD remains unexplored. Clinically, these cognitive deficits often overlap, and due to the earlier onset and longer course of EOPD, some studies suggest that executive dysfunction may be more prominent [7, 11]. However, systematic research on the dual syndrome hypothesis in EOPD remains lacking.
Given the pronounced executive dysfunction observed in EOPD and the critical role of the PFC in EF [8, 9, 11], we hypothesize that executive dysfunction might be an early and central feature of EOPD, potentially playing a central role in the development of cognitive impairments, which is consistent with the ‘prefrontal syndrome’ described in the dual syndrome hypothesis [14]. Based on the interconnected nature of cognitive processes, we suggest that difficulties in other domains, such as memory and visuospatial abilities, could be influenced by executive dysfunction, potentially developing as secondary consequences.
To elucidate the neural mechanisms of EF impairment, advanced neuroimaging methods are essential. Functional near-infrared spectroscopy (fNIRS) monitors oxy-hemoglobin ([oxy-Hb]) levels during neural activity, providing reliable brain function data that correlates closely with functional magnetic resonance imaging (fMRI) [20]. fNIRS offers key advantages, including minimal sensitivity to motion artifacts, fewer postural constraints, and high temporal with moderate spatial resolution [21]. Given the common presence of tremors and motor impairments in PD, the minimal restrictions fNIRS imposes on posture, tremors, and movement make it a highly suitable imaging technique for studying PD-related brain function [22, 23].
Although fNIRS is widely used in cognitive neuroscience, its applications in PD research remain limited, primarily focusing on LOPD [22, 24]. fNIRS studies in LOPD patients have explored prefrontal cortical activity during EF tasks, such as the verbal fluency test (VFT), revealing altered activation patterns compared to healthy controls [24, 25]. However, fNIRS research on EOPD, particularly regarding neural mechanisms of EF dysfunction in MCI, is lacking. This gap underscores the need for our study on EF characteristics in EOPD patients with MCI using fNIRS.
Based on this background, this research aims to investigate the characteristics and neural mechanisms of EF impairment in EOPD patients with MCI using fNIRS. Given that EF impairment may represent an early and central symptom in EOPD, other cognitive impairments may be associated with EF dysfunction. We hypothesize that EOPD patients with EF impairment will exhibit significantly different activation patterns in the PFC—particularly in the DLPFC and mPFC—EOPD patients without EF impairment or those who are cognitively normal. We also expect altered spontaneous neural activity in the PFC at rest in EF-impaired EOPD patients. By examining the link between EF deficits and PFC dysfunction, this study seeks to validate and extend the dual syndrome hypothesis in EOPD, providing a foundation for targeted clinical interventions and cognitive rehabilitation.
This study included 30 EOPD patients with disease onset before age 55, an age criterion commonly used to define EOPD in previous studies [26, 27, 28], recruited from the Neurology outpatient and inpatient wards of the First Affiliated Hospital of Dalian Medical University. Although the sample size is modest due to the rarity of EOPD, it reflects substantial recruitment efforts. Participants, aged 42–62 years (disease onset: 37–54 years), were classified based on cognitive assessments. Eligibility criteria followed the 2015 Movement Disorder Society (MDS) guidelines [29], requiring right-handedness, independent task completion, and adequate sensory function. Demographic and clinical details of the participants are summarized in Table 1. Exclusions included PD dementia [30], severe psychiatric disorders (e.g., major depressive disorder, schizophrenia), significant neurological conditions unrelated to PD (e.g., epilepsy, traumatic brain injury) [22], major systemic diseases, substance abuse, and prior deep brain stimulation therapy. Study procedures adhered to the Declaration of Helsinki, with ethical approval from the First Affiliated Hospital of Dalian Medical University (PJ-KS-KY-2021-218) and written informed consent from each participant.
| EOPD-NC | EOPD-EL | EOPD-NEL | p-value | Post hoc test | |||
| n = 12 | n = 12 | n = 6 | |||||
| Demographics | |||||||
| Age (years) | 53.2 |
55.6 |
52.5 |
0.392 | NA | ||
| Gender (Male/Female) | 6 (50.0%)/6 (50.0%) | 6 (50.0%)/6 (50.0%) | 4 (66.7%)/2 (33.3%) | 0.765 | NA | ||
| Years of education (years) | 13.7 |
10.3 |
10.2 |
0.109 | NA | ||
| Clinical data | |||||||
| Onset age (years) | 47.8 |
50.7 |
47.2 |
0.180 | NA | ||
| Hoehn and Yahr stage | 2.0 |
2.1 |
2.0 |
0.973 | NA | ||
| MDS-UPDRS III | 30.5 |
35.5 |
34.2 |
0.813 | NA | ||
| Medication | |||||||
| LEDD (mg/day) | 394.9 |
503.5 |
470.8 |
0.673 | NA | ||
| VFT performance | |||||||
| Total of “river”, “day”, and “home” | 10.8 |
5.3 |
8.5 |
0.003 | EOPD-EL | ||
| Word “river” | 2.4 |
1.8 |
2.5 |
0.355 | NA | ||
| Word “day” | 4.3 |
1.6 |
2.8 |
0.003 | EOPD-EL | ||
| Word “home” | 4.1 |
1.8 |
3.2 |
0.004 | EOPD-EL | ||
| Overall efficiency | |||||||
| MMSE | 28.1 |
25.0 |
27.7 |
0.048 | NA | ||
| Various cognitive domains | |||||||
| Executive functions (Z-score) | |||||||
| Clock Drawing Test | 0.55 |
–0.82 |
0.55 |
EOPD-EL | |||
| EOPD-EL | |||||||
| Category Fluency Test (animals) | 0.48 |
–0.55 |
0.13 |
0.034 | EOPD-EL | ||
| Language (Z-score) | |||||||
| 30–item Boston Naming Test | 0.64 |
–0.67 |
0.06 |
0.003 | EOPD-EL | ||
| Similarities Test | 0.73 |
–0.63 |
–0.20 |
0.001 | EOPD-EL | ||
| Visuospatial functions (Z-score) | |||||||
| Clock copying (Royall’s CLOX) | 0.31 |
–0.22 |
–0.17 |
0.396 | NA | ||
| Block Design Test | 0.71 |
–0.60 |
–0.21 |
0.002 | EOPD-EL | ||
| Episodic memory (Z-score) | |||||||
| Auditory Verbal Learning Test | 0.77 |
–0.48 |
–0.57 |
0.001 | EOPD-NEL | ||
| EOPD-EL | |||||||
| Logical memory | 0.56 |
–0.47 |
–0.16 |
0.031 | EOPD-EL | ||
| Attention/working memory (Z-score) | |||||||
| Symbol Digit Test | 0.54 |
–0.57 |
–0.50 |
0.019 | EOPD-NEL | ||
| Digit Span Test | 0.60 |
–0.45 |
–0.30 |
0.020 | EOPD-NEL | ||
| EOPD-EL | |||||||
EOPD, early-onset Parkinson’s disease; EOPD-NC, EOPD with normal cognition;
EOPD-EL, EOPD with executive function and/or language impairment; EOPD-NEL, EOPD
without executive or language impairments; LEDD, levodopa equivalent daily dose;
MDS-UPDRS-III, part III of the Movement Disorder Society-Sponsored Revision of
the Unified Parkinson Disease Rating Scale; VFT, verbal fluency test; NA, Not
applicable; MMSE, Mini-Mental State Examination. Note: Gender is presented as n
(%). All other continuous variables are presented as mean
We recorded age, gender, education years, and PD onset age, and standardized anti-Parkinsonian medications to levodopa equivalent daily dose (LEDD) [31]. Motor symptom severity was assessed with the Movement Disorder Society Unified Parkinson’s Disease Rating Scale Part III (MDS-UPDRS III) [32], and disease stage with the Hoehn and Yahr scale. Assessments were conducted during the “on” phase for patients with “on-off” phenomena.
Global cognition was assessed using the Mini-Mental State Examination (MMSE),
with additional tests across five cognitive domains, based on the 2012 MDS Level
II guidelines for PD-MCI [33], EF was assessed by the Clock Drawing Test and
Semantic Fluency Test (animals); language function was evaluated using the
Similarities Test and the 30-item Boston Naming Test; visuospatial skills was
measured through the Block Design Test and Clock Copying Test (Royall’s CLOX 2);
memory function was evaluated with the Auditory Verbal Learning Test and Logical
Memory Test; and attention/working memory was evaluated using the Digit Span Test
and Symbol Digit Test. These scales align with prior research [22]. For patients
with “on-off” phenomena, all assessments and examinations were conducted in the
“on” phase. Scores for each cognitive domain were converted into Z-scores, with
any Z-score
Based on clinical observations of considerable deficits in one or more cognitive
domains, EOPD patients were classified as either EOPD-NC (EOPD with normal
cognition) or EOPD-MCI (EOPD with MCI). EOPD-NC was defined as patients with no
failed tests (Z-scores
Given the hypothesis that impairment in EF may be an early and core symptom in EOPD, while deficits in other cognitive domains may arise as complications or secondary effects of executive dysfunction, we further divided EOPD-MCI patients into two subtypes: (a) the executive function-dominant subtype (EOPD-EL, EOPD with executive function and/or language impairment), potentially accompanied by deficits in visuospatial and/or memory and/or attention functions; and (b) the non-executive function subtype (EOPD-NEL, EOPD without executive or language impairments), which includes patients with difficulties in in visuospatial and/or memory and/or attention functions but no impairments in executive or language functions. This classification expands upon the dual syndrome hypothesis, further emphasizing the central role of EF in EOPD.
All PD patients completed the EF task recommended by PD-MCI guidelines [33], specifically the VFT. A 160-second Chinese block-designed VFT was used, following established methods [22]. The experimental paradigm of the VFT task is illustrated in Fig. 1. The test included a 30-second pre-task baseline, a 70-second post-task baseline, and a 60-second task phase, where participants generated phrases starting with “Jiang” (river), “Ri” (day), or “Jia” (home) shown on screen for 20 seconds each. During baseline phases, participants counted from 1 to 5 repeatedly. fNIRS signals were recorded throughout, and participants generated words in each 20-second phase, with only correct words recorded by the experimenter. The VFT score was the total number of correct words across all three phases.
 Fig. 1.
Fig. 1.
Flowchart depicting the procedure of the VFT.
Participants sat in a quiet, dimly lit room to minimize interference and were instructed to close their eyes, stay still, and avoid cognitive activity. Resting-state data were collected for 7 minutes.
We used a 52-channel fNIRS device (ETG-4000, Hitachi Medical, Tokyo, Japan) with
a 0.1-second temporal resolution and 10 Hz sampling rate to measure cerebral
hemodynamics. The system used 695 nm and 830 nm wavelengths, using the modified
Beer-Lambert law, to capture [oxy-Hb] and deoxygenated hemoglobin levels.
Seventeen emitters and sixteen detectors were arranged in a 3
 Fig. 2.
Fig. 2.
52-channel location map across different cortical regions. mPFC, medial prefrontal cortex; OFC, orbitofrontal cortex; VLPFC, ventrolateral prefrontal cortex; TL, temporal lobe; DLPFC, dorsolateral prefrontal cortex.
Demographic and clinical variables were analyzed using SPSS 26.0 (IBM Corp.,
Armonk, NY, USA). Continuous variables are presented as mean
For resting-state analysis, the amplitude of low-frequency fluctuations (ALFF)
was used to assess regional spontaneous neural activity with NIRS-KIT. To ensure
signal stability, the first and last 15 seconds of data were excluded.
Preprocessing steps also included targeted removal of physiological confounds,
such as systemic blood flow and respiratory artifacts, through a combination of
wavelet decomposition and band-pass filtering. The fNIRS time-series data were
transformed to the frequency domain using fast Fourier transform to obtain power
spectra, and the square root of power was calculated for each frequency. ALFF was
defined as the sum of these square roots within the low-frequency range
(0.01–0.08 Hz). ANOVA compared ALFF among the EOPD-NC, EOPD-EL, and EOPD-NEL
groups, followed by two-sample and one-sample t-tests for between- and
within-group comparisons focused on frontal regions. Multiple comparisons were
corrected using FDR (p
Table 1 summarizes the demographics, clinical features, and cognitive
performance of the EOPD-NC, EOPD-EL, and EOPD-NEL groups. Specifically, 12
patients were categorized as EOPD-NC, 12 as EOPD-EL, and 6 as EOPD-NEL. There
were no significant differences among the groups in age, gender, education, age
at onset, Hoehn and Yahr stage, MDS-UPDRS III scores, or LEDD (all
p
The EOPD-EL group scored significantly lower on the VFT total (p = 0.003) compared to the EOPD-NC group. They also produced fewer words for the prompts “day” (p = 0.003) and “home” (p = 0.004) (see Table 1 and Fig. 3).
 Fig. 3.
Fig. 3.
VFT performance across EOPD groups. The EOPD-EL group generated
fewer words overall, particularly for “day” and “home”, compared to the
EOPD-NC group. **p
During the VFT, the EOPD-NC group exhibited significant activation ([oxy-Hb])
changes in 12 Ch (5, 16, 23, 30, 32, 33, 40, 41, 43, 44, 50, and 51; mPFC, VLPFC,
OFC, and TL), with either reductions or increases observed (all p
| Channel | Side | Brain regions | T-value | p-value | |
|---|---|---|---|---|---|
| EOPD-NC | 5 | Right | Medial prefrontal cortex | −3.1104 | 0.0099 |
| 16 | / | Medial prefrontal cortex | −3.5928 | 0.0042 | |
| 50 | Left | Orbitofrontal cortex | 4.3098 | 0.0012 | |
| 23, 30, and 40 | Left and Right | Ventral lateral prefrontal cortex | 4.2901–4.8038 | 0.0006–0.0013 | |
| 32, 33, 41, 43, 44, and 51 | Left and Right | Temporal lobe | 3.1833–6.5232 | 0.0004–0.0087 | |
| EOPD-EL | 3 and 39 | Left and Right | Dorsolateral prefrontal cortex | 2.9100–3.1727 | 0.0089–0.0142 |
| 45 and 50 | Left and Right | Orbitofrontal cortex | 3.3758–3.6996 | 0.0035–0.0062 | |
| 24, 30, 34, and 40 | Left and Right | Ventral lateral prefrontal cortex | 2.9561–3.8452 | 0.0027–0.0131 | |
| 32, 33, 41, 43, 44, and 51 | Left and Right | Temporal lobe | 3.3223–4.6537 | 0.0007–0.0068 | |
| ANOVA: EOPD-NC, EOPD-EL, and EOPD-NEL | 16 | / | Medial prefrontal cortex | 8.7845 | 0.0012 |
| Post hoc: EOPD-EL vs. EOPD-NC | 16 | / | Medial prefrontal cortex | 4.1368 | 0.0004 |
| 6 | Left | Medial prefrontal cortex | 3.1907 | 0.0042 | |
| 4 and 17 | Left and Right | Dorsolateral prefrontal cortex | 3.2275–3.5152 | 0.0020–0.0039 |
 Fig. 4.
Fig. 4.
Changes in [oxy-Hb] levels during VFT and resting-state ALFF
values across EOPD groups. During the VFT task state, (A) EOPD-NC exhibited
decreased mPFC activation alongside increased activation in the VLPFC, OFC, and
TL, while (B) EOPD-EL showed heightened activation in the DLPFC, VLPFC, OFC, and
TL, suggesting higher cognitive effort. (C) In contrast, EOPD-NEL demonstrated no
significant activation changes. (D) ANOVA revealed significant differences in
mPFC activation among the three groups, and (E) post-hoc analysis indicated
significantly higher mPFC and DLPFC activation in EOPD-EL compared to EOPD-NC
(FDR-corrected, p
ANOVA results indicated significant differences among the three groups in
channel 16 (mPFC) (p = 0.0012, FDR corrected) (Table 2 and Fig. 4D).
Post hoc analyses revealed pairwise comparisons among the three groups, showing
that the EOPD-EL group had significantly increased activation in four Ch (4, 6,
16, and 17; mPFC and DLPFC) compared to the EOPD-NC group (all p
The EOPD-NC group exhibited significant ALFF changes in 13 channels (5, 6, 7,
16, 17, 19, 24, 32, 33, 41, 43, 44, 51; mPFC, DLPFC, VLPFC, TL), with either
reductions or increases observed (all p
| Channel | Side | Brain regions | T-value | p-value | |
| EOPD-NC | 5 and 6 | Left and Right | Medial prefrontal cortex | −5.1803 to −3.9110 | 0.0003–0.0024 |
| 16 | / | Medial prefrontal cortex | −8.4431 | 0.000004 | |
| 7 and 17 | Left | Dorsolateral prefrontal cortex | −3.8072 to −3.1308 | 0.0029–0.0096 | |
| 19 and 24 | Left and Right | Ventral lateral prefrontal cortex | −5.0072 to −3.8418 | 0.0004–0.0027 | |
| 32, 33, 41, 43, 44, and 51 | Left | Temporal lobe | 3.3542–3.4845 | 0.0051–0.0064 | |
| EOPD-EL | 13, 19, 29, and 40 | Left and Right | Ventral lateral prefrontal cortex | −8.7441 to −4.1363 | 0.000005–0.002 |
| EOPD-NEL | 6 | Left | Medial prefrontal cortex | −6.9389 | 0.001 |
| 19 and 24 | Left and Right | Ventral lateral prefrontal cortex | −5.3994 to −4.9437 | 0.0029–0.0043 | |
| ANOVA: EOPD-NC, EOPD-EL, and EOPD-NEL | 29 | Left | Ventral lateral prefrontal cortex | 8.3657 | 0.0016 |
| Post hoc: EOPD-EL vs. EOPD-NC | 29 | Left | Ventral lateral prefrontal cortex | −3.8543 | 0.0009 |
ANOVA revealed significant group differences in channel 29 (VLPFC) (p = 0.0016, FDR corrected; Table 3, Fig. 4I). Post hoc tests indicated that the EOPD-EL group had significantly lower activation in channel 29 compared to EOPD-NC (p = 0.0009, FDR corrected; Table 3, Fig. 4J).
Correlation analyses in the entire EOPD cohort revealed that
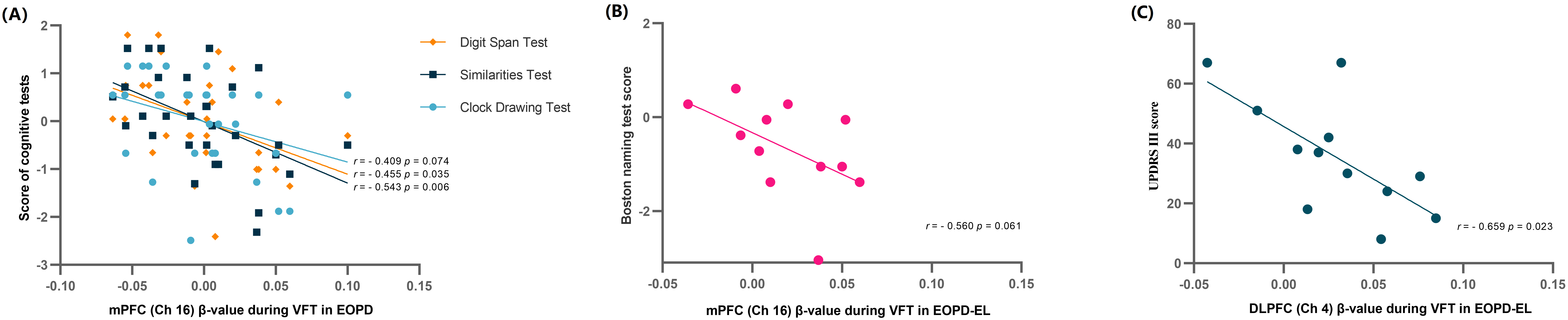 Fig. 5.
Fig. 5.
Correlation between brain activation and cognitive performance in EOPD. (A) In EOPD patients, mPFC activation during VFT negatively correlates with clock drawing, digit span, and similarity test scores. (B) In EOPD-EL, mPFC activation shows a marginal negative correlation with Boston Naming Test scores. (C) In EOPD-EL, DLPFC activation negatively correlates with MDS-UPDRS III scores. Bonferroni-corrected.
To the best of our knowledge, this study is among the first to use task-based and resting-state fNIRS to examine EF impairment and its neural mechanisms in EOPD-MCI. ANOVA and post-hoc comparisons revealed significantly higher activation in the mPFC and DLPFC during executive tasks in the EOPD-EL group compared to EOPD-NC. Additionally, the EOPD-EL group performed worse on behavioral tests, highlighting executive dysfunction as central to cognitive impairment in EOPD. Resting-state ALFF analysis showed markedly reduced spontaneous neural activity in the VLPFC of the EOPD-EL group compared to EOPD-NC. These findings support the dual syndrome hypothesis in EOPD, suggesting that executive dysfunction is a key aspect of cognitive decline and indicating abnormalities in specific brain networks. Unlike studies focused on LOPD, this research provides novel insights into cognitive impairment patterns in EOPD, emphasizing the critical role of the PFC in executive dysfunction.
The increased mPFC activation during the VFT task in EOPD-EL patients likely reflects abnormal default mode network (DMN) function. Typically, key DMN regions, like the mPFC [45], should be suppressed during cognitively demanding tasks to allow the executive network [46], including the DLPFC [47] to function effectively. This reciprocal inhibitory relationship facilitates the dynamic allocation of cognitive resources, ensuring optimal execution of cognitive tasks [46]. Therefore, as our results indicate, DMN activity in cognitively normal EOPD-NC patients is expected to decrease during task performance, allowing the executive network (such as the DLPFC) to become more active. However, in the EOPD-EL group, we observed a relative increase in mPFC activation, which likely reflects an inability to suppress the DMN properly during the task. Thus, the high mPFC activation in EOPD-EL reflects both ineffective DMN suppression and a decline in resource allocation efficiency during cognitively demanding tasks [48].
In addition to mPFC activation, EOPD-EL patients also showed significantly higher DLPFC activation during the VFT task. As a core region of the executive network, the DLPFC supports high-level cognitive processes like working memory, executive control, and response inhibition [8]. In the EOPD-NC group, when the DLPFC is highly active, the DMN (including the mPFC) should be inhibited [46], concentrating cognitive resources to meet task demands. However, in the EOPD-EL group, simultaneous high activation of both the DLPFC and mPFC suggests a disrupted reciprocal inhibition between the DMN and executive networks. The elevated DLPFC activation in EOPD-EL likely reflects a compensatory response [49, 50], where excessive mPFC activation disrupts the DMN-executive network balance, forcing EOPD-EL patients to recruit additional cognitive resources to maintain task performance, thereby increasing DLPFC activation.
In summary, the increased activation of both DLPFC and mPFC in the EOPD-EL group during the VFT suggests a disintegration between the executive network and DMN. The DLPFC activation reflects a compensatory executive response under high cognitive load, while abnormal mPFC activation indicates insufficient DMN suppression. This dual activation pattern points to dysregulated network function in EOPD patients with executive dysfunction, suggesting that DMN dysregulation underlies their EF impairment.
At rest, ALFF reflects regional spontaneous neural activity, a marker of intrinsic brain maintenance [51]. The VLPFC, a core component of the executive network, is crucial for complex tasks like emotion regulation, decision-making, and conflict control [52]. Therefore, VLPFC’s spontaneous neural activity supports the brain’s capacity to maintain EF reserves and regulatory ability in non-task states [53]. The significantly reduced VLPFC ALFF in the EOPD-EL group indicates impaired spontaneity and baseline regulation within the executive network. At rest, spontaneous VLPFC activity coordinates the executive and default mode networks, laying the foundation for effective task-based EF [54]. The lower VLPFC ALFF in the EOPD-EL group may reflect compromised regulatory capacity, reducing the executive network’s ability to build functional reserves and potentially affecting resource allocation during executive tasks.
This study validates and extends the dual syndrome hypothesis in EOPD, showing increased PFC activation (mPFC and DLPFC) during tasks and reduced VLPFC spontaneous activity at rest, suggesting that EF impairment is a key feature of cognitive decline in EOPD. These findings align with prior evidence of early PFC abnormalities associated with PD cognitive deterioration [55, 56]. Additionally, while our neuroimaging findings indicate a close association between EF impairment and PFC dysfunction, the relationship between EF deficits and other cognitive domains, such as memory and visuospatial abilities, requires further investigation. Our results provide empirical support for the dual syndrome hypothesis in EOPD, laying a theoretical foundation for future research on EF and other cognitive domains.
This study has several limitations. First, although EOPD patients are relatively rare, the small sample size may limit the statistical power and generalizability of the findings. A smaller sample size increases the risk of type II errors and may not fully capture the variability within the broader EOPD population. This limits the ability to generalize the results to all EOPD patients. Future studies with larger samples would improve statistical power and strengthen conclusions. Second, while previous study [22] compared PD subtypes without including a healthy control group, the lack of a true healthy control remains a limitation. EOPD-NC may not fully reflect the baseline cognition of non-PD individuals. Future studies should address this by including a healthy control group. Third, while fNIRS combined with ALFF offers a novel approach to assess spontaneous neural activity, it has known limitations, including susceptibility to systemic blood flow artifacts, global signal drift, limited cortical penetration depth, and inability to assess deeper brain regions. These factors may restrict the comprehensiveness of the analysis. Future studies should adopt advanced preprocessing techniques and consider integrating fMRI [57] or other imaging modalities to address these issues and validate findings. Finally, a longitudinal approach would better capture cognitive progression dynamics, providing further validation of the dual syndrome hypothesis.
This study uses task-based and resting-state fNIRS to investigate EF impairments and their neural mechanisms in EOPD. The results show that EOPD patients with EF impairments exhibit distinct activation patterns in the PFC, with increased mPFC and DLPFC activation during tasks and reduced VLPFC activity at rest. These findings support and extend the dual syndrome hypothesis in EOPD, highlighting EF impairment as a core component of cognitive decline. Our study reveals the relationship between EF dysfunction and network dysregulation in EOPD, providing insights into cognitive mechanisms and supporting tailored clinical interventions and cognitive rehabilitation strategies [58].
All data generated or analyzed during this study are included in this published article.
HYW contributed to data acquisition and analysis, funding acquisition, and drafting and revising the manuscript. ZL contributed to data acquisition, funding support, and manuscript review. ZY was responsible for data organization, study design, formal analysis, supervision, project administration, and manuscript review. YL contributed to data interpretation, supervision, and manuscript review. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was approved by the First Affiliated Hospital of Dalian Medical University (PJ-KS-KY-2021-218) and conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from all participants in writing.
We extend our heartfelt thanks to all the participants for their invaluable contributions to this study.
This study was supported by The PhD Research Fund of Jining No. 1 People’s Hospital (No. 2024-BS-003), the Medical and Health Science and Technology Project of Shandong Province (No. 202403090535), the Key R&D Program of Jining (Major Program, No. 2023YXNS004), and the Dalian Medical Science Research Program (No. 1812009).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.