



1 1st Department of Psychiatry, Medical School, National and Kapodistrian University of Athens, 11528 Athens, Greece
Abstract
In this article, we review clinical, theoretical, and empirical grounds for the consideration of a decisive, yet unrecognized, role of emotions in the psychopathology of acute schizophrenia. We describe accordingly the presence of an emotional syndrome named “Psychotic Arousal” and we further explore its clinical characteristics on the grounds of a psychopathological investigation, including its relevance to recent neurobiological advances. Psychotic arousal has been defined as a diffuse affective state, dominated by abnormal experiences that signify disturbed self-processing, as the brain interacts with external or internal objects. This process may eventually result in the experiential alienation of internal and external reality. Evidence supports that the aberrant experiences are of emotional origin and are seen as abnormal experiential feelings. In addition, this article outlines essential characteristics of the abnormal experiences with arguable biological significance. We propose that they are highly eligible to represent a real pathophysiological process, stemming from a hidden physiology related to the formation of core consciousness and reality perception, with severe consequences for cognition. We underline that the recognition of their medical semiology is important and offers us a unique opportunity to unveil aspects of the physiological mechanism behind the development of delusions and the psychopathology of acute schizophrenia. Moreover, we propose a plausible neurobiological path of investigation based on their phenomenological properties. Finally, we call for the field of Psychopathology to recognize and explore the pivotal role of emotions in the emergence of psychosis and the formation of delusions.
Keywords
- delusions
- psychotic arousal
- schizophrenia
- acute psychosis
- abnormal experiential feelings
- emotion
- subcortical connectivity
- amygdala
Delusions are among the main pathognomonic symptoms in schizophrenia and related psychotic disorders. They have been categorized as disorders of the thought content involving mainly higher cognitive functions relevant to belief formation and abnormalities of inferential thinking, information processing, and/or attentional disturbances [1, 2, 3, 4].
However, theories implying a prominent causal role in the formation of delusions to reasoning impairments—of an essentially widespread nature—seem problematic and not fully justified by research evidence. When variables such as IQ and neuropsychological performance were taken into account, differences on syllogistic-deductive reasoning among patients and normal controls have been shown to be insignificant [5, 6, 7, 8, 9].
Likewise, research data on probabilistic reasoning bias suggest that this deficit may not be causally related to either delusions or schizophrenia, but might instead be partly due—and secondary to—impairments in executive functions and memory [10].
On the other hand, studies examining the Jumping to Conclusions (JTC) style of reasoning in psychotic patients and its role in causality of delusions, concluded that JTC is neither a sufficient nor a necessary cause of psychosis or delusions, but may act as a trait representing a liability to delusions [11, 12].
In Psychiatric Phenomenology, scholars addressing the reasoning problem in schizophrenia report that the problem is not the lack of logic, but rather the excessive use of it [13], as the patients “can’t help but grasp on to logic because nothing else is left” [14].
Similarly, an increasing amount of data coming from a cognitive perspective reaches the same conclusion, that the problem with patients becoming deluded is far more complicated than just bad reasoning [7, 8].
We will argue below that, however irrational the delusions are, their origin cannot be attributed to a disorder deducible from cognitive processes explaining common forms of thought, relevant to the irrationality of our common beliefs, such as superstitions and self-deception. Instead, we will try to shed light on an unrecognized emotional syndrome and its potential involvement in the delusion formation and psychotic emergence.
Delusions, beyond their definition as false beliefs, exhibit several distinct qualities that could serve as guiding principles in a clinical approach of investigation:
(1) Delusions arise and evolve during an acute episode of psychosis—either first or recurrent. Though they can persist as ideas in-between the psychotic episodes, their high confidence and behavioral attunement usually dampens as the acute phase of illness ends and they lose their emotional charge [15, 16, 17, 18]. Interestingly though, in cases of illness relapse, patients reiterate original delusions that seem forgotten in the between period [19].
(2) Delusions often present a rather complex elaboration, related mostly to the intellectual abilities and cultural or personal background of the person [20, 21, 22, 23]. It is noteworthy that the more intelligent the person, the more elaborate the delusions tend to be. It is worth observing that such elaborations are typically disconnected from the rest of the person’s world view [5, 24, 25]. A deluded patient very often violates common sense or basic logical laws in regard to the object of delusion. Nevertheless, when not entirely disorganized, the person, apart from the behavior and misconceptions dictated by their delusions, travels rather efficiently in the real world or, furthermore, while holding extraordinary ideas, recognizes the weird claims of other patients [24, 25, 26, 27, 28, 29, 30, 31, 32].
(3) However, the core content and the nuclear themes of the delusions tend to be circumscribed [33, 34].
(4) If we try to subtract the ideational elaboration as we attempt to reach their core content, we are left with several circumscribed themes revolving around specific experiences. Delusions as ideas arise in the base of an experiential frame that is appearing unexpectedly, and most often bewildering to the person. For example, delusional ideas of reference involve ideas built upon a sudden and instant feeling, or experience of personal significance that random events in the external world acquire. Objects or unrelated occurrences become salient and gain an inexplicable significance for the person himself that demand explanation [33]. In some cases, as the person confronts banal environmental instances, the ‘meaning’ may present itself as an immediate, intrusive knowledge in an apocalyptic way [28, 34]. Ideas of passivity, control or thought insertion involve a kind of abolishment of ego boundaries and ownership of private mental acts that form the basic constituents of the normal and self-evident sense of an organism’s uniqueness and subjectivity [35, 36].
For someone who is not suffering from a psychotic episode, these experiences seem unintelligible, almost part of a fantasy or confabulation and hard to envisage as true medical symptoms. Undoubtedly though, for the patients they are very real with devastating consequences.
Currently, these primordial experiences are not forming part of the field of contemporary descriptive psychopathology.
In an ordinary psychiatric examination of psychosis, we tend to value the ideas and their irrational content more than the patient’s experience itself, and we disregard the semiological advantage these symptoms could have in medicine. However, contemporary delusion research, both empirical and conceptual, emphasizes the experiential dimension of delusions and its role in their formation [37, 38, 39].
True delusions or primary delusions as have been distinguished from secondary delusions or “delusion-like” ideas from Jaspers [28], represent an altered ontological framework of patients’ experience. The experiential constituent as a separate dimension relevant to delusion formation, has been also addressed by neurocognitive theorists in previous decades. Several explanations have been offered depending on whether abnormal perceptual contents deriving from neuropsychological or neuropsychiatric deficits, could be accounted for solely or in conjunction with reasoning impairments in the delusion formation (one-factor accounts and two-factor accounts respectively) [40, 41, 42, 43, 44, 45].
Abnormal subjective experiences in psychosis comprise an object of extensive exploration in the domain of psychiatric phenomenology within the realm of existential philosophical tradition [46, 47, 48].
According to phenomenological conceptualization, delusions are forming on the basis of an experiential ontological transformation that generally expresses radical transformations to the most basic structures of experiential life—including time, space, causality, necessity, contingency, and forms of basic self-experience. These transformations are evolving in a delusional atmosphere comprising a qualitative shift in the overall way reality is experienced [49, 50].
According to Feyaerts et al. [34], delusions seem to bypass both rational and irrational inferential processes involved in ordinary belief fixation.
Phenomenological observations and conceptualization broadened our understanding on delusions, shifting the attention from a purely ideational content, based on a reasoned biased formulation, to the consideration of the experiential dimension. It offers a unique perspective on intrapsychic phenomena related to delusion formation, in contrast to the nosologic descriptions of symptoms addressed by the psychiatric classification systems.
Modern phenomenologists further explored the experiential process of the subject that cognitively reacts and meta-experiences primordial experiences, advancing therefore, a first-person consideration and the empathetic understanding of the patient [51, 52].
However, phenomenological analysis being relied heavily in philosophical hermeneutics and tradition, with its own glossary and conventions, turns translation to biological equivalents into a difficult task.
The primary aim of the work we present herein is to explore pathways for the formation of delusions and the emergence of acute psychosis by re-examining essential clinical characteristics with possible biological significance. We favor that for understanding the pathophysiology of the disorder, it is especially important to address the biological nature of the primordial abnormal experiences. However, the first step is to acknowledge their biological validity, their clinical importance and their specific characteristics.
In this paper, we narratively reviewed evidence on the contribution of emotions to the psychopathology of acute schizophrenia, as well as the emotional nature of primordial abnormal experiences. We provided a conceptual framework based on clinical studies exploring these experiences during the acute state of psychosis. In this context, we critically addressed relevant traditional conceptions, attempting to delineate the formal characteristics and properties of the primordial abnormal experiences and to trace possible neurobiological correlates.
A multiyear clinical observation and exploration of acute psychotic patients from their admittance to medical care to symptomatic remission [53, 54], led us to several inferences that, as we will discuss below, are not always aligned with some doctrines in the psychopathology of psychosis [55, 56]. We had to repeatedly face and question several conceptual conventions that implicitly predetermined our way of thinking regarding the process of acute psychosis as follows:
Traditional psychopathology underestimates the role of emotions in the process of acute psychosis. While it recognizes the presence of a discrete emotional state in the predelusional period—the so-called “delusional mood”—and its decisive role in the transition to active psychosis [57, 58], curiously, it appears not to see its intensified, continuous presence during acute psychosis [59, 60].
The significance of delusional mood in the emergence of psychosis was already noted by several Nineteenth-century psychiatrists [28, 61, 62].
The clinical concept of delusional mood or atmosphere (Wahnstimmung) refers to a psychopathological syndrome that involves an increase of basic affective tone, which often manifests with a tonality of guilt, anxiety, potentially fear of death or depression, but also occasionally of anticipatory excitement, euphoria, or manic-like loss of inhibition. Experiences of self-reference, as well as depersonalization or derealization phenomena, and experiences of banishing the individual’s own and shared world, are regularly an inherent part of the clinical picture of delusional mood [55, 62, 63].
The phenomenological exploration of delusional mood in schizophrenia, suggests that the primary delusion only materializes and takes a clearly noematic form, initially on the basis of this global and diffuse state of atmospheric, pathic tension. It is widely asserted that delusions appear either as a relieving answer to the intense emotional discomfort occupying the patient in the predelusional phase, or that they represent a subjective “re-organization of meaning”, preserving the subject’s “vital” relationship with the environment [64].
However, an established doctrine in psychopathology undeniably attests that the emotional or affective counterparts, observed in delusional mood, are strictly predelusional and not present in the phase of acute psychosis, while mainstream psychopathology further asserts that we cannot consider the presence of delusional mood after the appearance of delusions [60].
Delusional mood, as a psychopathological syndrome involving both an affective counterpart with abnormal subjective experiences, has not been addressed by contemporary research. The requirement of in-depth psychopathological interviews, focusing upon the pre-onset features of the patients’ subjective experiences, have been implicated as the main barrier for this shortage [59, 60].
However, there are many studies describing the abnormal subjective experiences in prodromal schizophrenia characteristic to disturbances of the self and world perception, derealization phenomena, attenuated delusional ideas or overvalued ideas, that validate early reports at least as for the primary disturbances in the experiential frame [65, 66, 67, 68, 69, 70].
Furthermore, affective symptoms in the prodromal stages of schizophrenia have been repeatedly attested in contemporary research. Depressive symptoms, dysphoric, anxiety and unspecified symptoms are among the main symptoms characterizing the stage before the onset of psychosis [71]. Therefore, we can safely reason that every one of the constituent parts of the early described delusional mood in the incipient psychosis, has been documented by research, though that doesn’t entail any vital relation to each other.
As we already mentioned, according to contemporary psychopathology of acute schizophrenia, the primacy of delusional mood and the symptoms described above, concern mainly the prepsychotic phase, and conceptually it is not justified to consider them as the delusions appear, and the psychotic episode ensues.
We will assert below that this misconception has biased our clinical judgment for a long time, and induced an intractable conceptual gap in the psychopathology of psychotic emergence: If primary delusions are commencing on a base of an experiential abnormality that already preexists and strictly determines pre-psychotic stages, how do we explain the emergence of psychotic onset and the rise of delusions at a subsequent stage? Why then and not earlier? But above all, what is the nature of these experiential symptoms and how do they influence rational thinking so decisively?
The clinical picture of the acute psychosis, apart from the defining psychotic symptoms such as delusions and hallucinations, displays a plethora of affective symptoms of variable intensity (depressive and anxiety symptoms, fear, perplexity, guilt, sorrow, puzzlement, ecstasy, or even retarded mood) [72].
According to traditional conceptions in the psychopathology of acute schizophrenia, these symptoms, though prominent in the clinical picture, are considered as trivial or of minor significance. They are mainly considered to involve a secondary reaction to positive symptoms [73]. However, an increasing amount of data not only confirms the presence of depressive symptoms in schizophrenia but also speculates a relation with its pathophysiology, decoding the genetic links among schizophrenia and affective illnesses [74, 75, 76, 77, 78, 79, 80].
Nevertheless, these advancements have not yet been integrated into a new coherent conceptual framework in the psychopathology of schizophrenia. Implicitly in clinical practice, we deem that patients are anxious, fearful, excited or agitated because they believe that they are, for example, poisoned or persecuted.
Despite this, what we noticed in our multi-year clinical exploration was that the emotional state of the acute psychotic patient was not secondary to thought disorder. On the contrary, a patient could reconsider morbid thoughts only after the attenuation of the emotional symptoms, as it eventually occurs in response to antipsychotic treatment. This observation was in line with that of other scholars studying the antidopaminergic action of drugs in schizophrenia [81, 82, 83, 84, 85].
Furthermore, deep diving into the experiential emotional state of the patients, our observations revealed that these peculiar experiences as mentioned earlier (instances of feelings of self-relevance, derealization/depersonalization, the abolishment of the ownership of mental acts and the loosening ego boundaries, among others), were an inextricable part of the emotional frame, following its arousal and its subsequent amelioration, taking a syndromic character of a specific emotional arousal. Also of interest are the abnormal experiences recognized by patients and identified as ‘feelings’. Moreover, the more severe the emotional arousal and the intensity of escorted experiences, the more difficult it was for the patient to logically confront the content of the experience, which in this case was taking a form of absolute reality for the patient. Amelioration of the severity of these emotional symptoms was a prerequisite for more logical arguments to prevail. Gradually, the person with schizophrenia, as the emotional arousal retreated and the abnormal ‘feelings’ ceased, declared at first that delusional ideas were no longer valid but, interestingly, very often insisted that at the time of the emotional commotion, they were valid. In a clinical investigation, for unveiling this sequential order and the influential gravity these experiences have in patients’ confidence for the reality of delusions, there is a critical time: approximately in the first two weeks from the initiation of an efficient antipsychotic medication. It is during this time that the initial doubts about the validity of the delusions appear. Challenging questions such as “Why do you now doubt your ideas?” and “What changed from previous days, and what are you not so confident of now?”, reveal answers such as “Because I don’t feel it any more” and lead patients on to descriptions of their abnormal experiential feelings during the previous days of their emotional commotion.
Abnormal primordial experiences in acute psychosis are not fabricated by some imaginative minds. Nor are they pertaining to any specific neuropsychiatric or perceptual abnormality we usually encounter in common neurological disorders. They present consistent and universal characteristics as for:
(a) Their association with a diffuse affective state and their affinity in their experiential mode to be sensed as a kind of instinctive set of feelings;
(b) Their abrupt, spontaneous and momentous mode of appearance, as the person confronts with environmental or internal stimuli, bewildering and surprising the person;
(c) They present case sensitivity and are object-related as for their way to render spontaneously certain occurrences;
(d) They provide an implicit knowledge of ‘the meaning of things’ or ‘of what happens’ that does not include appraisals of “good or bad”—individuals consistently report that they cannot attribute a valence to their experience, but rather they are astonished;
(e) Their relation to reality formation with the ability to bypass selectively rational elaboration;
(f) Their universal appearance, despite patients’ intellectual, social and cultural background.
Regarding the content of these abnormal experiences, they correspond thematically to the experiential basis of primary delusions as already have been presented.
We suggest that these kinds of abnormal experiences are highly eligible for representing a real pathophysiological process, stemming from a hidden physiology related to the formation of core consciousness, and the reality perception with severe consequences to cognition. This paper argues that these aberrant experiences offer us a unique opportunity to unveil aspects of the physiological mechanism behind the above functions, by considering and investigating their essential manifesting features.
Examining the above peculiar experiences under the umbrella of an emotional arousal allowed us to conceptually explore them, translating relevant neuroscientific advances [86, 87] into the emotional nature of the abnormal experiences of psychotic emergence [55].
From a biological perspective, these abnormal experiences may not be considered conjured up, but as a deviant and an unpredictable outcome of an otherwise normal process that takes place continuously and in pulses, as we confront the endless changes in the internal and external environment: that of the emergence of normal experiential feelings that constantly and implicitly arise as the brain interacts with environmental or internal stimuli. Normally, these constantly created feelings go unnoticed, but form the bedrock of basic consciousness, leading to the emergence of subjectivity and ‘self’. Hence, abnormal experiences, as they appear in acute psychosis with their specific content and unique characteristics, might reflect a dysfunctional emergence of an otherwise normal biological process with emotional roots. These feelings as experiences also become aware of, and alienated through, their disturbance.
In a previous publication [55], we concluded accordingly the presence of an emotional state—which we have termed “psychotic arousal” —saturated by distinct abnormal experiences, seen as “abnormal experiential feelings” that correspond to the emergence and acute phase of psychosis. We suggest that contrary to traditional conceptions in the psychopathology of schizophrenia, the clinical characteristics of the so-called “delusional mood” of the previous centuries’ psychopathological descriptions, are not evident only in the predelusional period of illness but, in an escalation of their severity, lead to the onset of psychosis, and also determine the psychopathology of the acute phase (Fig. 1, Ref. [55]).
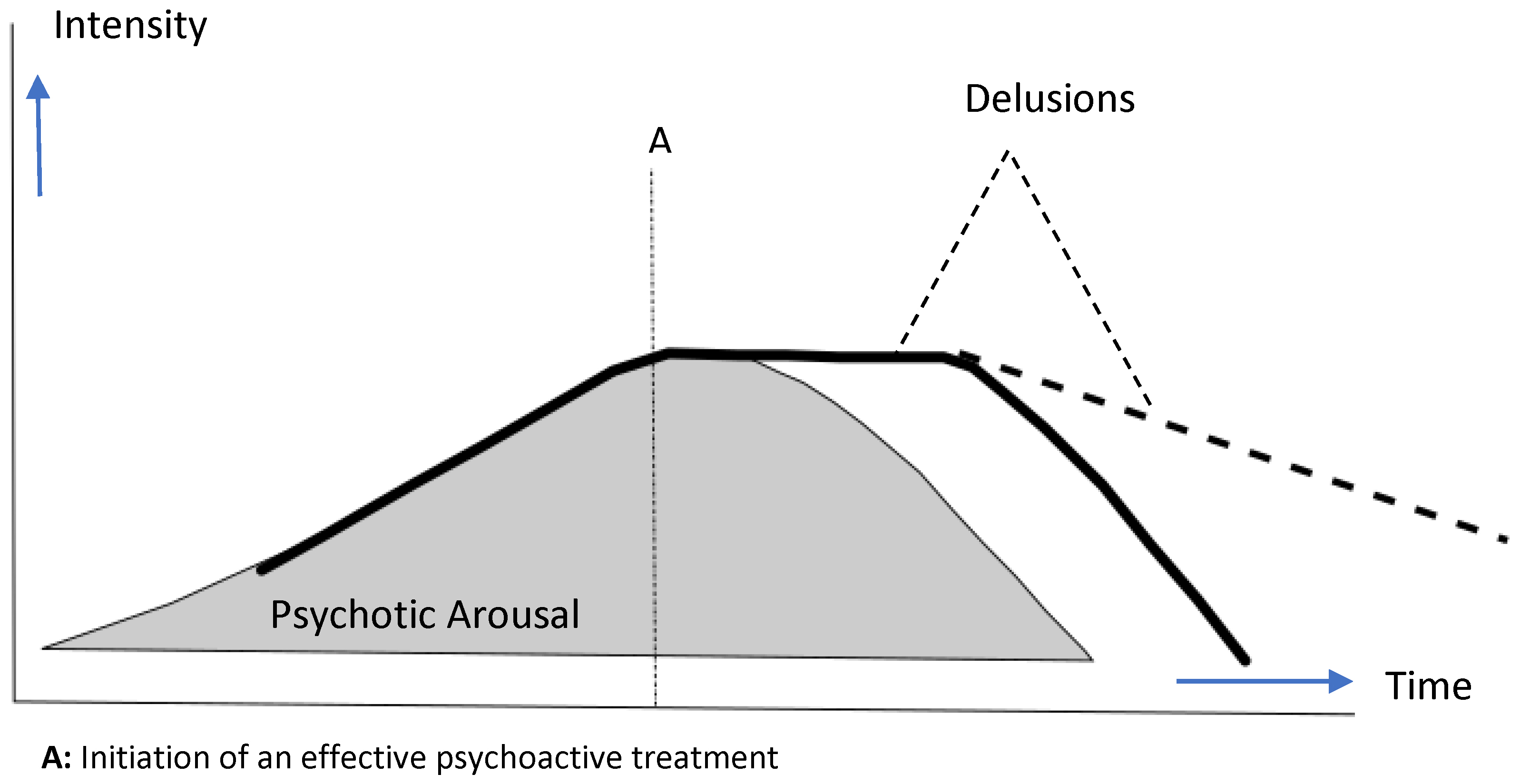 Fig. 1.
Fig. 1.
The diagram describes the emergence of psychotic arousal and delusions in the course of an acute psychotic state. [Reproduced from Margariti MM, Vlachos II (2022). The concept of psychotic arousal and its relevance to abnormal subjective experiences in schizophrenia: A hypothesis for the formation of primary delusions. Medical Hypotheses [55], with permission].
“Psychotic arousal” is a psychopathological construct that can be defined as a diffuse affective state of anxiety, fear, guilt, surprise or ecstasy, saturated by depersonalization and derealization feelings and abnormal experiential feelings, signifying disturbed self-processing as the brain interacts with external or internal objects, resulting eventually in experiential alienation of internal and external reality. As the psychotic arousal evolves, the frequency and the intensity of the abnormal experiential feelings increases. They interrelate with each other, forming absurd connections and morbid representations of the reality that urge for a narrative synthesis in the same way our normative perceived reality is apprehended and accomplished.
Following the above observations and conceptualization, we created an instrument (the psychotic arousal scale—PAS) and we performed a preliminary study [56] to provide empirical verification to our clinical observations in a sample of 55 patients with acute schizophrenia in order to test the following assumptions:
(a) Psychotic arousal is a psychopathological construct distinct from other psychopathological phenomena and eligible for investigation;
(b) Abnormal experiential feelings are an integral part of this entity, and are present during an acute schizophrenia episode;
(c) Psychotic arousal is amenable to antipsychotic treatment during the first period of treatment.
The findings of the study provided encouraging evidence for the consideration of a distinct psychopathological state with these specific emotional characteristics in acute schizophrenia. Results supported:
(a) The presence of an unrecognized psychopathological state, saturated by abnormal experiential feelings in acute psychosis;
(b) Its high affinity to other affective measures (depressive and anxiety);
(c) Its severity was related to the delusions’ conviction; and
(d) It was substantially amenable to antipsychotic intervention early in treatment—more precisely, according to the study’s results, at the first half of the period of the treatment provided for the amelioration of the acute episode.
Recent neuroimaging and neurobiological research highlights schizophrenia as a disorder of disrupted communication within large-scale brain networks, with growing evidence that emotional systems play a key role in the onset and progression of psychosis. Central to this is the corticolimbic circuit, which includes the medial prefrontal cortex, anterior cingulate cortex, nucleus accumbens, hippocampus, and amygdala [88, 89]. This circuitry integrates emotion, cognition, and decision-making, all of which are disturbed in schizophrenia. Studies specifically involve the medial temporal lobe and particularly the amygdala, hippocampus, and related limbic structures. These subcortical regions, highly interconnected with one another, coordinate processes such as memory, emotion, and motor control [90, 91, 92, 93, 94, 95, 96, 97]. Disruptions in their functional connectivity may underlie the core symptoms of schizophrenia and may even serve as biomarkers for diagnosis and treatment monitoring [98, 99, 100]. There is also a growing interest in research on the elucidation of how the complex network and neural dynamics of these subcortical interactions are associated with the manifestation and progression of schizophrenia symptoms [100]. Studies have shown that after treatment, the abnormal subcortical functional gradient in first episode schizophrenia is normalized [100, 101].
The dopamine hypothesis remains today the dominant neurochemical theory of psychosis. Kapur’s aberrant salience theory is an exceptional approach and paradigm on how to link neurobiological advances to the phenomenology of schizophrenia [84].
According to this hypothesis, hippocampal hyperactivity and rhythmicity disturbances are thought to drive excess striatal dopamine signaling. Thus, dopamine dysregulation both disrupts salience detection and contributes to heightened emotional arousal generating ultimately positive symptoms [102, 103, 104, 105, 106, 107, 108].
However, for explaining primary delusions, it is of paramount importance to address self-disturbance in schizophrenia phenomenology. As we described above, psychotic arousal is not only a simple emotional arousal, but it is characterized by the presence of abnormal experiential feelings of circumscribed content, with specific properties. Hyperactivity of the dopaminergic system and rhythmicity alterations may trigger a cascade of events contributing to a chaotic and impaired salience detection. We argue though, that this is only half the story. Based on the semiological analysis of our observations, we propose and anticipate that, dopaminergic dysregulation exerts in parallel a destabilized impact on a system that integrates information—at a primary level—from the internal state of the organism and input from both external sensations and mental images. We speculate that hyperactivation and dopamine dysregulation in rhythmicity could cause, probably in an already vulnerable substrate, a defective integration of stimuli with the image of the internal state, confined to specific and random occurrences with a momentous appearance. We assume that this process of integration provides the emotional character to this course, differentiating it from an ordinary perceptual event. The construction of the basic self as a mental process, presumably, as has already been proposed [86, 87] requires the secure and consistent mental recreation of the organism’s image, as it constantly confronts external and internal images. We propose that this process probably takes place in the vicinity of the subcortical circuitry, though it induces variable and larger-scale adversities to cortico-subcortical brain circuits. We presume the above, based mostly on the spontaneous and momentary character of the experience in conjunction, as an ensemble, to the specific circumscribed content that systematically defies unity of the self in specific occurrences, and to the characteristic absence of attribution of an affective valence to this primary emotional experience. It is difficult to imagine a similar outcome resulting from a higher-order function, though delusion as an integrated narrative represents a higher-order processing.
Subcortical circuits, particularly the amygdala and striatum may mediate this process [102, 106, 109]. The amygdala could be regarded especially central, as it evaluates emotionally salient stimuli and coordinates autonomic, behavioral, and social responses. Its function is modulated by dopamine through specialized intercalated cells, making it a key node in psychosis pathophysiology [110, 111]. Furthermore, intercalated cells receive a wide range of information about sensory experiences and context and are considered to act as barometers of internal state via strong expression of diverse neuromodulators [112, 113, 114]. The amygdala has also been associated with impairments in social functioning [115]. Furthermore, structural and functional alterations of the amygdala have been consistently found in individuals with schizophrenia and, together with other subcortical formations like the hippocampus, have been implicated in the pathogenesis of schizophrenia [116].
In the present article, we highlighted what we called a conceptual fallacy in the psychopathology of acute schizophrenia, providing several clinical, observational, and theoretical evidence, suggesting a principal role for an emotional contribution in the formation of primary delusions and psychotic emergence. Both our clinical observations and the preliminary empirical results are so far suggestive of the presence of an unrecognized emotional syndrome in the psychopathology of acute schizophrenia, saturated by abnormal experiential feelings. We further argued that abnormal subjective experiences in the emergence of psychosis are not a kind of perceptual disturbance or another kind of vague neuropsychological or neuropsychiatric disorder, but are of an emotional origin, and we delineated some of their characteristics.
We strongly support that the concept of psychotic arousal as a psychopathological entity should be evaluated and explored, as it seems very promising for both affective neuroscience, schizophrenia research, and probably psychopharmacological investigations. Specifically for the psychopathology of schizophrenia, it provides plausible answers to long-standing conceptual inconsistencies and smoothly conforms to modern neurobiological evidence with the prospect of promoting a fruitful dialogue.
As for the psychopathology research of schizophrenia, replication and research protocols with the inclusion of larger samples of patients and in different stages of illness, as well as the inclusion of patients with non-schizophrenia psychoses, should be considered.
According to our conceptualization, if primordial experiential feelings, generated in response to environmental and internal stimuli in a disturbed emotional background, can influence so decisively our conscious conceptual processing as to determine the inception and representation of reality, then established doctrines should be reevaluated. It seems to us that acute psychosis presents a vivid paradigm of the deviance of such a process.
One of the main intriguing and unsolved questions in psychiatry concerns the formation of delusions in psychotic illness. Despite the progress in the psychopharmacology and neurobiology of the disease, the absence of a coherent and biologically meaningful psychopathological interpretation hampers scientific progress. Descriptive psychopathology through the dominant implementation of the diagnostic classification systems in the psychiatric educational curricula [117, 118], slowed down several generations of young psychiatrists from addressing the questions that earlier psychiatrists have struggled with. Though we recognize the major importance of the classification systems and we don’t promote their replacement or abandonment, we argue that educational programs in psychiatry should foster the study of psychopathology, not restricted to classification and descriptive domains.
In this article, we also evaluated relevant neurobiological advancements, and based on our psychopathological observations, we suggested a methodological path for the neurobiological elucidation of the provided phenomenological manifestations.
Overall, incorporating psychotic arousal into both clinical assessment and psychopharmacological trials may enhance understanding of schizophrenia’s neurobiology and improve treatment evaluation. This approach bridges emotional, neurochemical, and network-level perspectives, offering a promising framework for future research and clinical practice.
Finally, though these issues are very important for future research, for our patients, it is even more vital.
Schizophrenia, as a mental disorder, is by far the most puzzling disorder in its subjective nature, and the most difficult in the establishment of a mutual ground of understanding between doctors and patients.
However, during our experience in using the psychotic arousal scale for the estimation of psychotic arousal and in the course of communicating its objectives with our patients, we were able to notice the following: for patients, recognition of these absurd feelings comes almost freely. Surprisingly, in the psychiatric interviews that followed, patients very often reported and graded their experiential feelings without even being asked. Signifying these feelings making sense to them as they acknowledge their peculiar and temporally determined presence. Also, we were able to observe that appraising them as important for their condition had a liberating effect on them. For the patients, claiming or insinuating a defective rationality provokes an adverse reaction—probably because they feel that we do not understand them. Therefore, we think that the recognition of the emotional syndrome with the incorporation of the abnormal experiential feelings in the clinical evaluation and therapeutic strategies could serve in advancing doctor-patient communication.
Recognizing the complexity of the emotional disturbance in psychosis could eventually help the patients to better facilitate a conscious conceptual elaboration, promoting collaboration and therapeutic efficacy.
MMM was responsible for the conception of ideas presented, writing, and the entire preparation of this manuscript. MMM read and approved the final manuscript. MMM has participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research received no external funding.
The author declares no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.