

 , Anke Zhang 5,*, Yongzhi Deng 1,6,*
, Anke Zhang 5,*, Yongzhi Deng 1,6,*1 College of Acupuncture and Massage, Changchun University of Chinese Medicine, 130117 Changchun, Jilin, China
2 Department of Dermatology, Tongji Hospital, School of Medicine, Tongji University, 200092 Shanghai, China
3 Department of Chinese Medicine Internal Medicine, The Affiliated Hospital to Changchun University of Chinese Medicine, 130021 Changchun, Jilin, China
4 State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, The First Affiliated Hospital, College of Medicine, Zhejiang University, 310027 Hangzhou, Zhejiang, China
5 Department of Neurosurgery, The Second Affiliated Hospital, School of Medicine, Zhejiang University, 310009 Hangzhou, Zhejiang, China
6 Department of Acupuncture, The Third Affiliated Hospital to Changchun University of Chinese Medicine, 130117 Changchun, Jilin, China
†These authors contributed equally.
Abstract
Stroke is the most common cerebrovascular disease and one of the leading causes of death and disability worldwide. The current conventional treatment for stroke involves increasing cerebral blood flow and reducing neuronal damage; however, there are no particularly effective therapeutic strategies for rehabilitation after neuronal damage. Therefore, there is an urgent need to identify a novel alternative therapy for stroke. Acupuncture has been applied in China for 3000 years and has been widely utilized in the treatment of cerebrovascular diseases. Accumulating evidence has revealed that acupuncture holds promise as a potential therapeutic strategy for stroke. In our present review, we focused on elucidating the possible mechanisms of acupuncture in the treatment of ischemic stroke, including nerve regeneration after brain injury, inhibition of inflammation, increased cerebral blood flow, and subsequent rehabilitation.
Keywords
- ischemic stroke
- electroacupuncture
- inflammation
- nervous system
- rehabilitation
According to previous studies, approximately 13.7 million people are affected and afflicted by stroke each year [1, 2]. Stroke is currently the second leading cause of death worldwide [3], accounting for 10% of all deaths [4, 5]. Its high mortality, disability, and recurrence rates impose a heavy economic burden on global health care systems. Stroke is broadly categorized as ischemic or hemorrhagic; this review focuses on the mechanisms associated with ischemic stroke. This is the most common type of stroke and is caused by occlusion of cerebral blood vessels or cerebral thrombosis, which results in blockage of cerebral blood flow (CBF) and thereby causes ischemia, hypoxia, and softening or even necrosis of brain tissue.
After ischemic stroke onset, restoring cerebrovascular function to reinitiate the blood supply to the brain is the first priority. Current conventional treatment strategies include angioplasty, stenting, intravenous thrombolytic therapy, and thrombectomy. However, there are obvious limitations to these therapies, including stringent treatment time windows, strict indications for administration, and many contraindications [6, 7]. The safety and efficacy of these treatment strategies are also controversial according to previous clinical research [8]. Therefore, there is an urgent need to identify novel effective therapeutic strategies for clinical use.
Acupuncture originated in China, has a history of more than 3000 years, and is an important component of Chinese medicine [9]. It involves the stimulation of specific acupuncture points on the body surface with specially designed metal needles within the theoretical framework of traditional Chinese medicine and utilizes twisting and lifting techniques or electrical impulses to treat diseases [10, 11, 12]. Acupuncture is rapidly developing; its use has spread to many countries and its efficacy is widely recognized. Scientists have studied the efficacy and underlying mechanisms of acupuncture, and the effectiveness of acupuncture as an alternative therapy for stroke has been described in the literature [13]. However, the potential mechanisms through which acupuncture may aid the treatment of stroke are not yet fully understood. Therefore, the purpose of this study is to investigate the possible mechanisms of acupuncture in the treatment of stroke. Various studies have demonstrated that acupuncture pretreatment can treat ischemic stroke by inducing cerebral ischemic tolerance, regulating oxidative stress, increasing CBF, inhibiting apoptosis, and promoting neural regeneration; thus, it is a promising prevention strategy and alternative therapy for stroke [14].
Ischemic stroke is caused by a reduction in or interruption of blood flow in the cerebral arteries due to various causes, including atherosclerosis, cardiogenic embolism, vasculitis, hereditary diseases, and hematologic disorders [15, 16]. Ischemic stroke directly impairs neurological function in three main ways. First, ischemia and infarction during ischemic stroke cause direct damage to brain tissue. Second, ischemia induces the production of excess reactive oxygen species (ROS), causing oxidative stress, which exacerbates neuronal dysfunction. Finally, the inflammatory cascade caused by ischemic stroke is thought to result in further neuronal damage.
Acupuncture, which originated in China, has been developed as a unique treatment modality during its long history and is an important part of Chinese medicine [17, 18]. Several clinical studies have shown that acupuncture improves postural balance, reduces muscle spasms, and increases muscle strength [19, 20, 21]. In electroacupuncture (EA) therapy, a fine needle is inserted into the selected acupoint. After tactile confirmation that the needle is correctly placed, an EA machine is connected to the acupuncture needle, and a low-frequency pulse current similar to that of human bioelectric currents is delivered with different stimulation parameters to treat different diseases [22]. A systematic review and meta-analysis published in 2015 evaluated the clinical efficacy and safety of EA in the treatment of ischemic stroke [23]. The mechanism of EA in the treatment of ischemic stroke has also received much attention recently; scientists conducted a systematic review and analysis of recent clinical studies and found that EA can play a role in the treatment of ischemic stroke through the following five mechanisms: (1) EA can promote neuronal proliferation and differentiation and induce poststroke neurogenesis and neuroprotection, (2) EA can effectively ameliorate the damage caused by cerebral ischemia‒reperfusion, (3) EA can increase CBF and alleviate blood–brain barrier dysfunction after stroke, (4) EA can inhibit apoptosis, and (5) EA pretreatment can induce cerebral ischemic tolerance [24, 25, 26, 27, 28]. Herein, we review the main potential mechanisms of acupuncture in the treatment of stroke.
Studies on the mechanism of acupuncture in treating ischemic stroke models were obtained by a PubMed literature search, which was limited to full-text studies published in English between January 1, 2000, and December 31, 2022. The following search string was used for the literature search: (“electroacupuncture” OR “acupoint”) AND (“ischemic stroke” OR “neurogenesis” OR “cerebral ischemia” OR “cerebral reperfusion” OR “cerebral blood flow” OR “apoptosis autophagy” OR “preconditioning” OR “rehabilitation”). We identified a total of 120 published articles. Papers that did not describe the specific mechanisms by which EA treated ischemic stroke injury, papers that had information on stroke and EA but were unrelated, and papers that used EA as a secondary treatment were excluded. Of these, a total of 40 published articles met the inclusion criteria. All searches were limited to animal studies, most of which used a similar animal model of ischemic stroke, the unilateral transient middle cerebral artery occlusion (MCAO) model.
The beneficial effect of EA on neurogenesis after brain injury may be related to
neurotrophic factors. Neurogenesis in adult mammals is accomplished primarily
through the division of stem and progenitor cells [29]. Adult neurogenesis, i.e.,
neuronal growth and development, mainly occurs in two brain regions: the
subventricular zone (SVZ) of the lateral ventricle and the subgranular zone (SGZ)
of the dentate gyrus (DG) of the hippocampus [30, 31]. Reports indicate the
presence of neural stem cells (NSCs) in the neocortex, amygdala, striatum, and
substantial nigra [32]. These NSCs have the ability to differentiate into
different types of neurons, astrocytes, and oligodendrocytes at the time of brain
injury [33, 34]. Neural progenitor cells (NPCs) are present in the SVZ and
migrate to the site of the injury, where they form new functional synapses with
the remaining neurons and connect new neural circuits [35, 36]. Brain injury
activates endogenous neural repair systems, and the proliferation and survival of
these neural cells are thought to play a role in neural repair in the brain,
which is a potential therapeutic target [37, 38, 39]. Neurotrophic factors can
prevent ischemic injury and exert neuroprotective effects. Glial cell-derived
neurotrophic factor (GDNF) belongs to the transforming growth factor beta
(TGF-
Notch receptors are highly conserved, single-channel transmembrane proteins that are involved in various cytogenesis-related processes, including cell differentiation, apoptosis, and proliferation, and play an important role in the regulation of self-renewal and differentiation of NSCs after ischemic injury. In the MCAO animal model, EA at LI11 and Zusanli ST36 was found to activate the Notch signaling pathway, significantly decreasing cerebral infarct size, improving cerebral nerve function, and promoting the proliferation of NSCs in rats [56, 57, 58, 59]. Basic fibroblast growth factor (bFGF) promotes the regeneration and repair of mesodermal ectodermal cells, which is essential for the development and differentiation of the central nervous system (CNS). In both cerebral ischemia/reperfusion (CI/R) and MCAO models, EA treatment was found to significantly increase the expression level of bFGF in the striatum and cortex and thus exert neurogenic and protective effects [60, 61, 62]. One of the most abundant neuropeptides in the nervous system, neuropeptide Y (NPY), is a key regulator of homeostasis inside and outside the CNS, while NPY can also promote neurogenesis in the SVZ and DG regions. Furthermore, acupuncture can upregulate the expression of NPY in the CNS [63, 64, 65, 66]. In addition to affecting neurogenesis and proliferation, ischemic stroke also severely impairs brain function due to cerebral ischemia/reperfusion.
CI/R leads to the generation of large amounts of ROS, resulting in an imbalance between oxidative and antioxidative status in the body and thus oxidative stress, which in turn causes cellular damage and necrosis, which is a key factor in ischemic brain injury [67, 68]. Mitochondria are the main site of aerobic cellular respiration, supplying energy to cells and participating in cell differentiation, apoptosis, and information transfer [69]. Under normal physiological conditions, the respiratory chain of mitochondria is the main source of ROS, but CI/R increases the leakage of electrons generated in the respiratory chain, resulting in the production of large amounts of ROS [70]. Furthermore, CI/R causes a large decrease in the level of superoxide dismutase (SOD), a key factor in maintaining oxidative and antioxidative balance, impairing its function as a free radical scavenger and the redox balance of mitochondria, and causing the excessive production of ROS and free radicals with impaired antioxidant capacity, ultimately leading to mitochondrial dysfunction [71, 72]. Experiments have shown that EA of Fengchi GB 20 can activate the antioxidant enzyme system and increase the ability of SOD and glutathione peroxidase (GSH-Px) to scavenge excessive ROS; this increase in SOD activity involves the nuclear factor erythroid-2 related factor 2 (Nrf2)/heme oxygenase (HO-1) signaling pathway, and the increase in GSH-Px activity may be associated with increased antioxidant activity by glutathione (GSH) [73, 74]. CI/R causes lipid peroxidation to produce malondialdehyde (MDA) and 4-hydroxynonenoic acid (4-HNE), and EA at GB20 and ST36 can reduce the degree of lipid peroxidation and MDA production during MCAO [75]. A systematic review and meta-analysis published in 2014 showed that EA reduced the infarct size and improved neural function in animal models of cerebral ischemia [76]. The respiratory chain function of mitochondria was found to be significantly improved after EA at Shuigou GV26 and GV20, and the activities of succinate dehydrogenase (SDH), cytochrome C oxidoreductase, and NADH dehydrogenase (NADH-Q) reductase were found to be increased, resulting in an elevated antioxidant capacity and inhibition of ROS production [77]. It was also found that CI/R impaired the phosphoinositide 3-kinase (PI3K)-protein kinase B (AKT)-mammalian target of rapamycin (mTOR)-mediated autophagy–lysosome pathway (ALP) to increase the percentage of dysfunctional mitochondria while impairing mitochondrial autophagy, an important change associated with CI/R, and EA restored mitochondrial autophagy through the Pink1/Parkin signaling pathway to ameliorate the impairment of the ALP [78, 79].
The inflammatory cascade after ischemic stroke results in the activation of a series of inflammatory cells and the release of inflammatory signals. Acupuncture exerts anti-inflammatory effects by regulating multiple immune cell populations and inflammatory transmission, which involves glial cells, vagal cholinergic anti-inflammatory pathways, and leukocytes (Fig. 1).
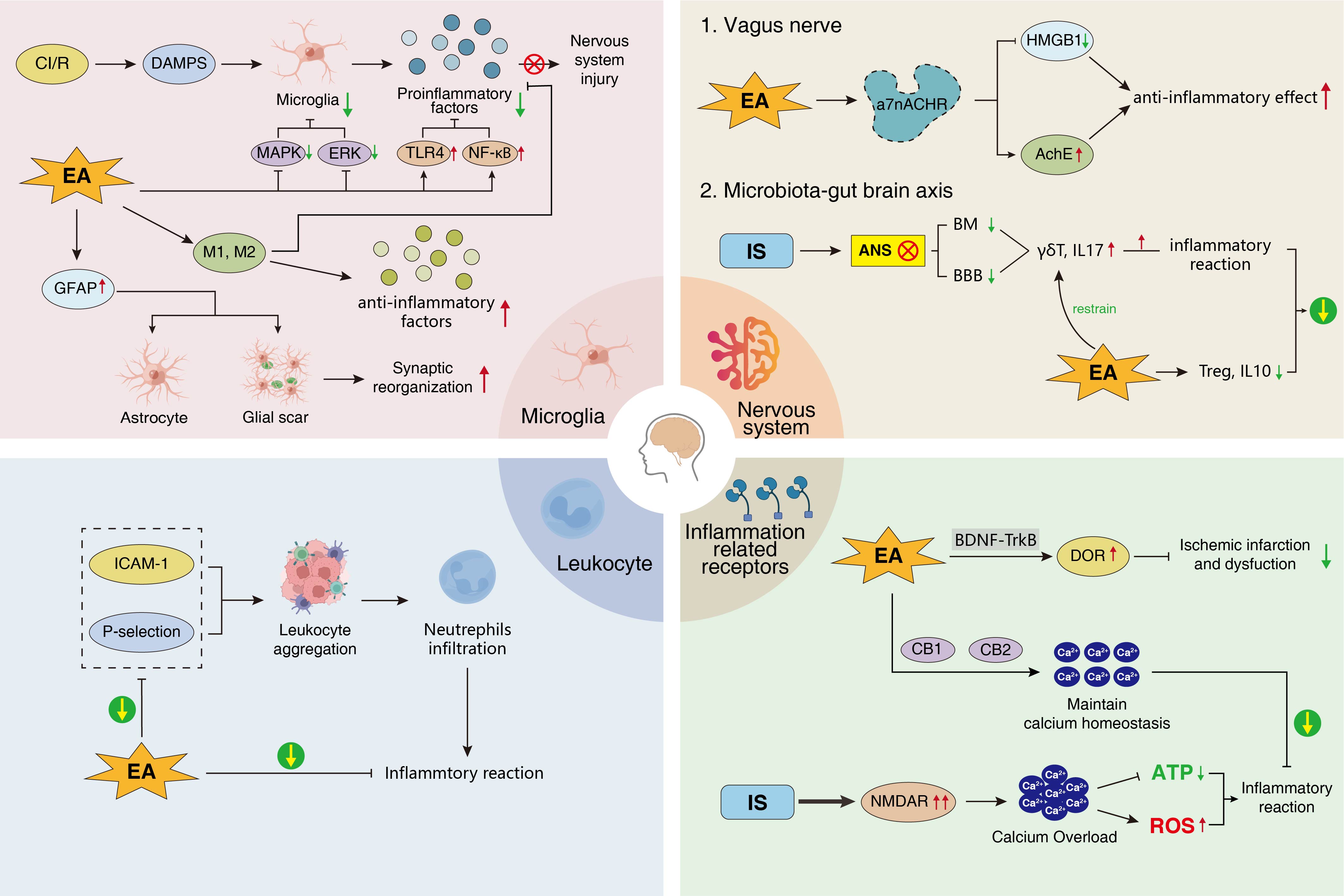 Fig. 1.
Fig. 1.Anti-inflammatory effects of EA. EA, Electroacupuncture; GFAP,
glial fibrillary acidic protein; M1, M1 microglia; M2, M2 microglia; CI/R,
cerebral infarction/reperfusion; DAMPs, damage-related molecular patterns; MAPK,
mitogen-activated protein kinase; ERK, extracellular regulatory protein kinase;
TLR4, Toll-like receptor 4; NF-
Microglia are the most numerous immune cells in the brain, accounting for
5–10% of all cells in the brain [80]. Damaged neurons release damage-related
molecular patterns (DAMPs) after CI/R, and DAMPs rapidly activate microglia [56].
On the one hand, the anti-inflammatory factors (interleukin, IL-4, IL-10, IL-13,
TGF-
Stimulation of the vagus nerve may be a potential therapeutic strategy to
effectively reduce the inflammatory response and promote neurological recovery
[94]. The vagal cholinergic anti-inflammatory pathway can inhibit the release of
TNF-
After ischemic injury, the production of adhesion molecules and chemotactic mediators of leukocytes increases, resulting in the recruitment of large numbers of leukocytes to the injured area and their adhesion to endothelial cells, as well as an increase in neutrophil infiltration, which exacerbates the release of proinflammatory factors and the inflammatory response [102, 103]. Intercellular cell adhesion molecule-1 (ICAM-1) is an important receptor that mediates the leukocyte adhesion response, and its expression level is increased in response to inflammatory stimuli in ischemic injury, thereby exacerbating leukocyte adhesion and infiltration [104, 105]. The expression of platelet p-selectin (P-selectin), an adhesion molecule, is upregulated after ischemic injury, causing leukocytes to roll on stimulated endothelial cells, resulting in leukocyte extravasation and aggravating the inflammatory response while causing platelets to adhere and aggregate and lose their stability, thus forming a thrombus [106]. EA was found to inhibit the expression of ICAM-1 and P-selectin, reduce the adhesion and infiltration of leukocytes, and exert an anti-inflammatory effect [107].
In addition to its analgesic and sedative effects, activation of the
delta-opioid receptor (DOR) has been shown to effectively protect against
ischemic-hypoxic injury during CI/R by reducing excitatory neurotransmitter
expression through ion homeostasis and reducing impaired neurotransmission, which
may be related to the BDNF-tyrosine kinase
receptor B (TrkB) signaling pathway. EA at GV26 and PC6 was shown to upregulate
DOR expression by mediating the BDNF-TrkB signaling pathway and significantly
reduce ischemic infarction and functional impairment [108, 109]. Glutamate is an
important excitatory neurotransmitter in the CNS. Ischemic transporter
dysfunction in the brain after stroke leads to excessive release of glutamate and
overactivation of N-methyl-D-aspartate (NMDA) glutamate
receptor (NMDAR), which induces excitotoxicity leading to neuronal cell injury
and death [110]. In an animal model of ischemia induced by vascular occlusion,
glutamate levels were found to be significantly higher in the control group
(135.19
The gut is the most important immune organ of the human body, accounting for
approximately 70% of the immune function of the whole body. The
microbiota–gut–brain axis (MGBA) is a bidirectional regulatory network between
the brain and the gut [123]. After stroke, homeostasis of the intestinal
microbiota is disrupted, dysregulation of the autonomic nervous system (ANS)
leads to the weakening of intestinal movement and barrier function, and
proinflammatory factors in the intestine enter the brain through the damaged
blood‒brain barrier to aggravate injury [124]. Studies have shown that T cells
play a key role in tissue damage secondary to ischemic stroke [125]. The initial
inflammatory cascade causes T cells to migrate to, and T cell subpopulation
(
The blood‒brain barrier (BBB) consists of the brain capillary wall and glial cells and is a barrier between the blood circulation and brain tissue. Due to its poor permeability, the BBB can limit the exchange of free substances between blood and brain tissue, and it has a role in maintaining the homeostasis of the brain’s internal environment and protecting neural tissue from damage by toxins and pathogens [130, 131, 132]. After ischemic injury, the integrity of the BBB is disrupted and its permeability increases, resulting in vasogenic edema and hemorrhagic transformation [133]. In a CI/R rat model, EA at GV20 and GV14 can reduce ischemic damage to brain cortical neurons and the BBB [134]. In addition, EA downregulates the expression of Nogo-A, an inhibitory neuroregenerative factor, to alleviate BBB damage [135]. EA at GV20, GV26, and ST36 improved the vascular ultrastructure of brain tissue in CI/R rats, promoting capillary generation and restoration of vascular function, which was closely related to the upregulation of VEGF mRNA expression [136]. The expression of metalloproteinase inhibitor-1 (TIMP-1) mRNA and protein tissue inhibitor was found to be dysregulated after EA at GV20, Hegu LI4, and Taichong LR3 in an MCAO animal model [137]. The protein and mRNA expression levels of matrix metalloproteinase 9 (MMP-9) were shown to significantly reduced in the BBB of CI/R rats after EA at GV20 and GV26 [138]. Reduced inflammatory cell infiltration and upregulation of matrix metalloproteinase 2/water channel protein (MMP2/AQP) expression occurred after EA at GV20 and ST36 [139]. The above experimental results all indicate that acupuncture can ameliorate BBB injury and exert neuroprotective effects on ischemic brain tissue.
VEGF promotes the proliferation and division of endothelial cells, increases
vascular permeability, and promotes neoangiogenesis [132, 140]. EA was shown to
activate the HIF-1
A
Apoptosis is a genetically controlled, programmed process of autonomous cell
death, and can be induced by excess free radicals generated in acute cerebral
ischemia, by a Ca
Autophagy is a process by which cells degrade their own components using lysosomes; autophagy and apoptosis jointly maintain cellular homeostasis under normal physiological conditions [155, 156]. Cellular autophagy is regulated by Unc-51-like autophagy-activated kinase 1 (UIK1) and FUN14-containing structural domain protein 1 (FUNDC1) [157]. Pretreatment by EA at GV20 and GV26 was shown to suppress p-ULK1 and FUNDC1 expression and upregulate p-mTORC1 and microtubule-associated protein light chain 3 (LC3-I) expression, thereby improving neurological function and reducing the infarct volume [158]. The silent information regulator 1 (SIRT1)-forkhead box proteins O1 (FOXO1) signaling pathway is an important factor in autophagy regulation. After EA pretreatment, the ratio of IC3-II/LC3-I is decreased; the complex effect of acetylated (AC)-FOXO1 and Atg7 is reduced; the levels of p62, SIRT1, and FOXO1 are elevated; and the number of autophagosomes in CI/R rats is significantly reduced. The neuroprotective effect of EA pretreatment may be related to the activation of the SIRT1-FOXO1 signaling pathway [159].
As early as the pre-Qin period in ancient China, the concept of prevention
before disease has been followed in Chinese medicine [28]. Preventive acupuncture
can open the meridians, regulate the organs, balance yin and yang, support the
positive, and eliminate the evil [160]. Acupuncture is widely used in the
prevention and treatment of ischemic stroke because of its few side effects and
high safety and efficacy [28]. EA pretreatment was found to confer tolerance to
cerebral ischemic injury in rats; Furthermore, neurological impairment was shown
to be significantly increased and the infarct volume (38.3
The main sequelae of ischemic stroke sequelae are numbness, hemiparesis, motor dysfunction, cognitive dysfunction, and memory loss, which are often responsible for the high disability rate and poor outcomes. Zhan et al. [167] reported in a meta-analysis of 14 randomized controlled trials {896 patients with poststroke cognitive impairment (PSCI)} that EA improved cognitive function and motor function in patients with PSCI. In a stroke rehabilitation experiment, the control group was given standard physiotherapy, and the intervention group received acupuncture. Analysis of the experimental data showed that the immediate and long-term outcomes of the intervention group were better than those of the control group, with EA significantly ameliorating spasticity and motor dysfunction of the limbs caused by stroke and restoring the ability of the patients to perform daily life activities [168]. Another study on stroke hemiplegia found that acupuncture significantly improved muscle spasms and mobility in hemiplegic limbs [169]. Ischemic stroke induces vascular cognitive impairment (VCI), and the learning and memory abilities of VCI model rats are improved after EA at GV20 and Shenting GV24, which may be related to the fact that EA increases the postsynaptic current frequency in neurons in the hippocampal CA3-CA1 regions, promoting connectivity and plasticity [170]. Furthermore, acupuncture at ST36 was shown to alleviate cognitive dysfunction and normalize cAMP concentrations, Protein kinase A (PKA) activity, and phosphorylation of cAMP response element binding protein (pCREB) and pERK expression in patients with vascular dementia, while blocking the PKA signaling pathway was found to reverse the beneficial effect of acupuncture, indicating that acupuncture improves hippocampal function through the regulation of the cAMP/PKA/CREB signaling pathway [171]. Long-term potentiation (LTP) in the hippocampus is responsible for memory formation and learning, and induction of LTP is dependent on NMDAR activation [172]. EA is able to reverse LTP impairment in a rat depression model, possibly by upregulating the expression of the NMDAR subunit NMDARs with NR2B subunits (GluN2B) in the hippocampus [173]. EA at ST36 and SP6 was shown to reduce local circuit inhibition and enhance LTP, possibly by promoting synaptic transmission via inhibition of gamma-aminobutyric acid (GABA) release from interneurons to increase the excitability of granule cells [174]. Acupuncture can activate language-related brain areas and rebuild the neural network responsible for language to relieve language impairment [175] (Table 1, Ref. [52, 75, 77, 87, 101, 111, 137, 152, 153, 170, 174, 176]).
| Acupoint | Acupuncture Parameters | Outcome | Model | Year | Reference |
| Fengchi GB20 | 2 Hz, 30 min | Affected the degree of lipid peroxidation and MDA production after MCAO | MCAO | 2004 | Siu et al. [75] |
| Shuigou GV26 | 5/20 Hz, 2–4 mA, 30 min, 1 mm | Significantly increased respiratory enzyme activity and reduced ROS production | MCAO | 2009 | Zhong et al. [77] |
| Yanglingquan GB34 Xuanzhong GB39 | 2 Hz, 10 min, 5 mm | Decreased glutamate levels | MCAO | 2010 | Lee et al. [111] |
| Quchi LI11 | 1/20 Hz, 30 min, 2–3 mm | Promoted the activation of the PI3K/Akt pathway and inhibited apoptosis in the brain | MCAO | 2012 | Chen et al. [152] |
| Sanyinjiao SP6 | 2 Hz, 20 min | Increased LTP | AD | 2012 | He et al. [174] |
| Baihui GV20 | 2 Hz, 20 min, 10 days, 2 mm | Significantly increased the mRNA expression of BDNF and VEGF | MCAO | 2014 | Kim et al. [52] |
| Neiguan PC6 | 2/15 Hz, 1 mA, 30 min, 5 days | Decreased IL-1 |
MCAO | 2015 | Han et al. [87] |
| Zusanli ST36 | 1–20 Hz, 0.2 mA, 30 min, 3 days | Decreased NF- |
MCAO | 2016 | Liu et al. [176] |
| Hegu LI4 Taichong LR3 | 2 Hz, 1 mA, 7 days | Increased Bcl-2 protein and TIMP-1 levels and decreased Bax protein and MMP-9 levels | MCAO | 2016 | Ma et al. [137] |
| Dazhui GV14 | 2/15 Hz, 1 mA, 30 min, 5 mm | Significantly reduced the mRNA levels of choline acetyltransferase, five subtypes of muscarinic receptors, and a7NACHR | MCAO/R | 2018 | Chi et al. [101] |
| Shenshu BL23 | 2/100 Hz, 1 mA, 40 min | Decreased the Bax/Bcl 2 ratio and cleaved cystatin-3 levels | MCAO | 2022 | Long et al. [153] |
| Shenting GV24 | 2/20 Hz, 1–3 mA, 30 min, 3 mm, 20 days | Increased synaptic transmission efficiency and plasticity in the CA3-CA1 region of the hippocampus | VCI | 2022 | Dai et al. [170] |
MDA, malondialdehyde; MCAO, middle cerebral artery occlusion; VCI, vascular
cognitive impairment; LTP, long-term potentiation; AD, Alzheimer’s disease; VEGF,
vascular endothelial growth factor; MMP-9, matrix metalloproteinase 9; MCAO/R,
Middle cerebral artery occlusion/reperfusion; TNF-
Acupuncture is a promising alternative treatment option for ischemic stroke with high efficacy, safety, and convenience. However, the efficacy of acupuncture has been challenged and questioned, the fundamental reason being that some of the mechanisms of action are still unclear. At present, there have been few international reports or studies on acupuncture treatment; high-quality acupuncture research studies are lacking and the theoretical basis for the benefits of acupuncture has not yet been adequately described. Furthermore, most of the research on acupuncture has been performed in China; clinical research results from China are not accepted by international mainstream medicine, and the acupuncture methods used in this research are not in line with international standards. Research methods for studying acupuncture are not consistent with modern scientific methods, and no method has yet been established to evaluate the clinical efficacy of acupuncture. It is difficult to perform a randomized controlled trial (RCT) study on acupuncture; furthermore, the use of blinding and placebos in acupuncture research is also controversial and it can be difficult to determine the criteria for a meta-analysis of acupuncture studies. The qualifications of the physician are also an important consideration related to acupuncture, as the teaching modes of major universities and training institutions vary greatly; thus, the theoretical knowledge and operational skills of acupuncturists worldwide are not necessarily consistent, meaning that treatment effects vary from person to person. In addition, due to interindividual variability, the location of acupuncture points differs among individuals, which in turn leads to biased clinical conclusions, and the optimal frequency, timing, and methods of acupuncture have also yet to be determined.
This study reviewed the evidence for the beneficial effects of EA on ischemic stroke in animal studies. EA can promote nerve cell regeneration after ischemic stroke and alleviate CI/R injury by reducing oxidative stress and inhibiting the inflammatory response. EA can also improve cerebrovascular function, affect angiogenesis, and reduce apoptosis and autophagy. Furthermore, EA preconditioning can increase ischemic tolerance and contribute substantially to subsequent rehabilitation.
QX and MG designed the review and wrote the manuscript. AS, CF and ST designed and drew pictures and tables. YD and AZ collected and organized reference materials. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.