

 , Lipeng Jian 3, Lide Jin 2, Shengquan Huang 2
, Lipeng Jian 3, Lide Jin 2, Shengquan Huang 21 Department of Neurosurgery, The Affiliated Hospital of Kunming University of Science and Technology, 650100 Kunming, Yunnan, China
2 Department of Neurosurgery, The First People's Hospital of Yunnan Province, 650100 Kunming, Yunnan, China
3 Department of Neurosurgery, Yunnan Provincial Hospital of Traditional Chinese Medicine, 650032 Kunming, Yunnan, China
Abstract
Intracranial vascular-related diseases are a common occurrence in neurosurgery. They have complex and diverse pathogeneses; further, their diagnosis and treatment remain unclear. Three-dimensional image post-processing technology is an emerging technology that involves converting a brain image scan into a digital model using image post-processing software, thus establishing a 3D view of the region of interest. Three-dimensional visualisation of the brains of patients with cerebrovascular diseases can allow a more intuitive examination of the local anatomy of the lesion as well as the adjacency between the lesion and peripheral nerves, brain tissue, and skull bones. Subsequently, this informs pre-operative planning, allows more accurate diagnosis of cerebrovascular diseases, and improves the safety of surgical treatment. This review summarised the current literature regarding cerebrovascular diseases and the application of 3D image post-processing technology in different cerebrovascular diseases.
Keywords
- image post-processing technology
- cerebrovascular disease
- pituitary tumour
- trigeminal neuralgia
- 3D modelling
Vascular-related diseases are common neurosurgical disorders that mainly include haemorrhagic vascular, ischaemic vascular, and other vascular-related diseases. They are characterised by diverse clinical symptoms, including mild symptoms of headache and dizziness as well as adverse symptoms such as severe neurological deficits, and can be treated through various surgical approaches. However, the utility of conventional brain imaging methods in the auxiliary diagnosis and surgical planning for patients with vascular-related diseases remains unclear. Three-dimensional image post-processing technology is an emerging imaging technology that involves reprocessing of a brain image using image post-processing software to allow 3D visualisation of the lesions, local anatomy, and other adjacent microstructures in the brain of the patient. This information allows the pre-operative formulation of a safe and effective surgical approach. This review summarises the types, diagnosis, and main treatment approaches of cerebrovascular diseases; further, it discusses the pre-operative, intraoperative, and postoperative applications of 3D image post-processing in various cerebrovascular diseases.
Cerebrovascular disease is a general term for a large category of diseases caused by cerebral vascular lesions or cerebral blood circulation disorders or other diseases whose pathogenesis is closely related to cerebrovascular disorders, including trigeminal neuralgia and pituitary tumours. Cerebrovascular diseases are highly prevalent, posing a serious public health concern [1]. Conventionally, cerebrovascular diseases are generally classified into acute and chronic. Acute cerebrovascular diseases include cerebral haemorrhage, cerebral infarction, and transient ischaemic attack, whereas chronic cerebrovascular diseases include vascular dementia [2, 3]. The most common cerebrovascular disease is intracranial aneurysm, which is the formation of a tumour-like bulge in local blood vessels mainly caused by local haemodynamic changes. The rupture of these aneurysms leads to subarachnoid haemorrhage, causing severe headaches and vomiting. Moreover, the bleeding leads to the formation of local haematoma, resulting in the loss of important nerve functions. Lack of prompt treatment of the ruptured aneurysm in time results in re-bleeding and greatly increases the mortality risk. A pituitary tumour is a neoplastic disease whose pathogenesis and involvement of blood vessels remain unclear. However, the incidence of intracranial aneurysms among patients with acromegaly due to a pituitary tumour is as high as 17.3%; additionally, growth hormone (GH) levels at the onset of acromegaly have been positively correlated with the risk of intracranial aneurysms [4]. High levels of GH and growth factor-1 in patients with GH-secreting pituitary tumours increase the risk of aneurysms through arterial dilation and arterial wall degeneration [5, 6]. Trigeminal neuralgia is a cranial nerve disease. In 1932, Dandy [7] proposed that trigeminal neuralgia was caused by neighbouring blood vessels compressing the trigeminal nerve. Specifically, in patients with cerebellopontine angle tumours, the trigeminal nerve root is compressed by abnormal blood vessels leading to demyelination and primary trigeminal neuralgia [8, 9], supporting the close involvement of blood vessels in trigeminal neuralgia.
Medical image post-processing involves the comprehensive use of computer image processing technology to process body images obtained using various digital imaging equipment for specific medical needs. It provides more accurate anatomical and pathophysiological information than the traditional approach of simply obtaining and observing images for the required medical information. Image post-processing allows 3D visualisation, image segmentation, and the application of various methods of image fusion and registration [10]. In clinical practice, medical image post-processing is used for auxiliary observation and diagnosis. Auxiliary observation allows different dimensions and methods for observation, providing more evidence for informed clinical decisions, whereas auxiliary diagnosis expands the range of diagnostic recommendations. 3D Slicer is a global open-source image post-processing software used for medical image analysis (including registration and interactive segmentation) and visualisation (including 3D rendering); further, it is used in image-guided therapy research. It has numerous functions and can be used for multi-organ and whole-body examinations. Further, it supports multimodality imaging, including magnetic resonance imaging (MRI), computed tomography (CT), ultrasonography, positron emission tomography, and nuclear medicine. Of note, 3D Slicer allows lesion modelling, 3D printing, and surgical planning. Additionally, it allows multimodal fusion; for example, in patients with trigeminal neuralgia, image information of nerve fibre bundles, arteries, veins, and brain tissue can be fused into a single image.
Despite the increased interest in the risk factors for the occurrence and development of intracranial aneurysms, including haemodynamic, genetic, and autoimmune factors, however, these remain unclear. Studies have used 3D visualisation to investigate the risk factors for aneurysm formation. Can et al. [11] used 3D Slicer to perform 3D modelling using computed tomography angiography (CTA) images of 56 patients with posterior communication artery aneurysms and 23 healthy controls. Subsequently, they obtained morphological parameters, including the diameter, segmental distance, and intervascular angle of the main blood vessels surrounding the aneurysm. They found that the diameter of the posterior communicating artery was positively correlated with the risk of posterior communicating aneurysms. This indicated that morphological parameters objectively obtained through 3D modelling and measurement can be used to stratify the risk of aneurysm formation. Additionally, these morphological parameters can be used to assess the risk of aneurysm rupture [12, 13]. Jiang [14] divided 14 patients with posterior communication artery aneurysms into rupture and non-ruptured groups. Subsequently, they used 3D modelling of the aneurysm and its surrounding vasculature to obtain nine morphological parameters, including size, height, width, neck width, aspect ratio, bottleneck factor, size ratio, and bubble formation. They found that bubble formation may be associated with the rupture of posterior communicating artery aneurysms [15, 16, 17]. Studies have used 3D models for morphological analysis of aneurysms [14, 18, 19]. Conventionally, the aneurysm volume is calculated using the elliptic volume formula, which is inaccurate and allows for a large margin of error. Chung and Ko [20] proposed an innovative approach for aneurysm volume quantification that uses 3D Slicer and other 3D modelling software platforms to establish an aneurysm model [21, 22]. Using this approach, the aneurysm is removed through model modification, with the volume differences between the models with and without the aneurysm being considered as the aneurysm volume. This quantification method can be used for aneurysms of any shape [23, 24]. Moreover, 3D Slicer can be used to accurately measure the coil bulk density before interventional surgery. Additionally, 3D slicer can reconstruct the aneurysm, brain tissue, surrounding nerves, and blood vessels before surgical microclipping to provide information for pre-operative planning and preparation [25, 26]. Traditionally, digital subtraction and computed tomography angiography are used for pre-operative evaluation of a brain aneurysm. However, they cannot visualise blood clots in large intracranial aneurysms. Spontaneous thrombotic aneurysms account for 60% of all intracranial giant aneurysms. 3D Slicer can be used to reconstruct the thrombus in the giant aneurysm based on time-of-flight angiography, which yields the following three components: blood flow, thrombus, and artifacts. The thrombus and artifacts can be distinguished using a motion-sensitisation-driven equilibrium sequence, thus facilitating pre-operative planning [27].
Elucidating the factors related to changes in the haematoma volume during the onset and development of cerebral haemorrhage is important. Dr. Oge [28] examined the relationship between haematoma enlargement and regularity of the surface of the cerebral haemorrhage by importing CT data of cerebral haemorrhage into the 3D Slicer software [29]. The semi-threshold algorithm was used to establish the haemorrhage tumour profile and the following parameters were collected: haematoma volume, surface area, and surface regularity. No correlation was observed between the expansion of the haematoma volume and surface area. Moreover, the baseline haematoma volume, international normalised ratio, and initial imaging time were significant predictors of haematoma enlargement [30]. Whether the degree of primary brain swelling in patients with subarachnoid haemorrhage is associated with their prognosis given the lack of quantitative measurements, remains unclear. Qin et al. [31] used the semi-automatic threshold algorithm function of the 3D Slicer software to examine the change rate in brain volume (CRBV) in patients with early-onset cerebral oedema [32]. Their findings indicated that the CRBV can be used as a volumetric representation of the degree of brain swelling; interestingly, a large CRBV was associated with a poor prognosis. Taken together, CRBV can be used as a potential neuroimaging biomarker and prognostic indicator for patients with early-stage brain injury following subarachnoid haemorrhage after aneurysm rupture [33]. Hence, 3D Slicer can be used for haematoma projection and surgical planning in cerebral haemorrhage treatment [34, 35]. Accordingly, Qiu et al. [36] used 3D Slicer to inform interventions for patients with cerebral haemorrhage [37, 38]. Further, analysis using 3D Slicer has shown that the average clearance rate of haematoma was 90.75% [36, 39, 40].
Pituitary tumours are relatively common tumours in the sellar region. Patients with pituitary tumours present with decreased vision and abnormal hormone levels. Some primary tumours can have an erosive effect on the sphenoid bone or lead to the expansion of the internal carotid artery [41, 42]. Accordingly, surgical treatment of pituitary tumours is difficult [43], with delayed internal carotid artery rupture being a potentially fatal intraoperative or postoperative complication. Pre-operative CT and MRI data of patients with pituitary tumours can be imported into 3D Slicer to construct 3D models of pituitary tumours, normal pituitary glands, internal carotid arteries, and sphenoid sinuses [44, 45, 46]. The obtained information can then be used to formulate personalised pre-operative plans, that is, appropriate surgical positioning and strategy of opening the sellar septum to contact vital nerve tissue [47, 48, 49, 50].
Trigeminal neuralgia is clinically characterised by temporary, paroxysmal severe pain in the trigeminal nerve region of one side of the face, which significantly interferes with the quality of life of patients. Trigeminal neuralgia usually occurs following neurovascular conflict [51, 52]. Assessment of the involved blood vessels usually requires cranial imaging of the corresponding area. A previous retrospective study analysed the effectiveness of 3D virtual reality reconstruction techniques and traditional MRI scans in planning microvascular decompression surgery in 24 patients with trigeminal neuralgia. Pre-operative 3D reconstruction could yield information regarding the local area of facial and auditory nerves, brain tissue, skull, arteries, and veins [53, 54]. Moreover, it could determine the location of the trigeminal nerve and involved blood vessel [55]. Spatial and anatomical presentation in virtual reality (VR) models can also facilitate surgery [56, 57, 58, 59, 60]. Likewise, CT 3D visualisation during percutaneous balloon compression (PBC) treatment of trigeminal neuralgia allows accurate determination of the optimal position and shape of the contrast agent-filled balloon [61] as well as the relationship between foramen ovale parameters and luminal pressure. Wang et al. [62] performed 3D reconstruction using pre-operative CT images in 20 patients with trigeminal neuralgia. Subsequently, they examined the relationship between the parameters of the foramen ovale and changes in the intraluminal pressure during PBC [55, 63]. Their findings indicated that the parameters of the foramen ovale obtained through 3D reconstruction could inform the control of pressure changes in the target lumen during PBC. Taken together, 3D modelling of the lesion area in patients with trigeminal neuralgia can considerably facilitate informed decision-making by neurosurgeons [64, 65, 66].
Simultaneously combining theory and practice in the traditional teaching approach is difficult. Contrastingly, 3D modelling of specific brain tissue can be combined with conventional teaching methods to increase the interest of students in learning and understanding various basic anatomical knowledge [67, 68, 69, 70]. 3D disease models can be used in the training of neurosurgery residents to explain the characteristics of various diseases, pre-operative surgical approaches, and brain microdissection [71, 72, 73]; furthermore, 3D modelling greatly improves the efficiency of learning and understanding of the surgical treatment of various diseases [74, 75, 76]. Moreover, 3D models can greatly strengthen the communication between doctors and patients [77]. Taken together, neurosurgical diseases, surgical protocols, and rehabilitation approaches can be taught using 3D models established through image post-processing [78, 79, 80].
With the progress of science and technology, our exploration of the human body has become increasingly meticulous. The exploration of the brain as the high-level centre of life is continuous, while our knowledge of cerebrovascular-related diseases has become increasingly extensive through the three-dimensional visualization reconstruction of vascular vessels, brain tissues, and nerves by image post-processing technology [81] (Fig. 1). In this review, we systematically described the application of 3D visualization technology in various cerebrovascular-related diseases. In the diagnosis and treatment of aneurysm, 3D visualization allows the reconstruction of the local morphology of the aneurysm, the relationship between the aneurysm and surrounding tissues, and adequately assesses the risk of rupture, so as to formulate a perfect surgical strategy. For patients with pituitary tumours and trigeminal neuralgia, 3D visualization enables the reconstruction of the local anatomical model of the relevant lesions, so as to have a more in-depth understanding of the disease. The application of 3D visualization technology in intracranial vascular-related diseases not only allows clinicians to have a better understanding of the disease, but also offers great advantages in the development of surgical strategies, determination of the surgical risk, development of individualized surgical strategies, improvement of the accuracy of precision treatment, and reduction in the incidence of postoperative complications, thus conferring important clinical value. The integration of medicine and engineering has been increasing in recent years, offering novel directions in the future development of medicine. For instance, an arterial model can be formulated using a three-dimensional modelling software, while the fluid model in the blood vessel can be calculated using fluid mechanics software. Combining these models enables the assessment of haemodynamic changes in the blood vessel, understanding of the difference in blood flow between lesions and normal tissues, conduct of more in-depth research on lesions, and formulation of a more perfect surgical plan. However, the current development of medical-industrial integration also has certain deficiencies; the time of medical-industrial integration is relatively short, the system is not perfect, while the concept of medical-industrial integration, its goal, and innovative ideas remain unclear. Medical-industrial integration belongs to multidisciplinary cross, the implementation of the more difficult, complex talent is relatively lack of, in the future, with the medical-industrial combination of more and more in-depth, more and more medical composite talents, to meet the current medical development of the increasingly diversified, high-end requirements, to stimulate the development of medical-industrial combination of the new vitality of the comprehensive, to solve more problems in medical, and to make more contributions to the life and health of mankind.
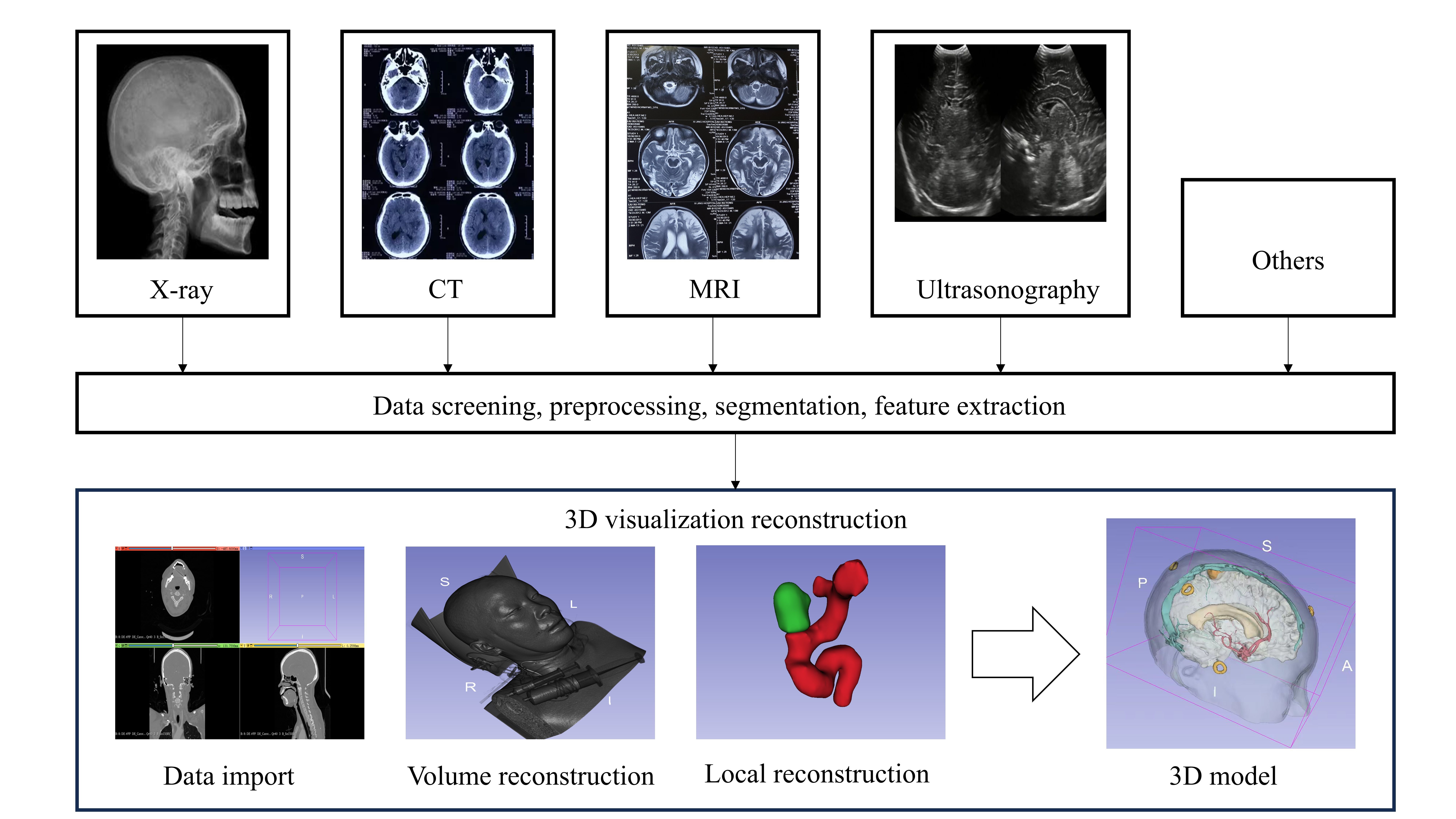 Fig. 1.
Fig. 1.
3D visual reconstruction technique route. Image Description: Make a copy of the patient’s reconstructed data (X-ray, CT, MRI, ultrasound, or other), which must be the original data, usually in DICOM format. Further data screening, pre-processing, segmentation, feature extraction. Imported into the image post-processing system, using the image post-processing software related tools for volumetric reconstruction, local lesion dissection, lesion assessment through the reconstruction of three-dimensional model, the development of preoperative surgical strategy, and explain the condition to the family. CT, computed tomography; MRI, magnetic resonance imaging.
Scientific and technological advances have allowed the increasingly extensive exploration of the human body. Accordingly, the development of 3D visualisation with image post-processing technology has facilitated the elucidation of cerebrovascular diseases. This technology can be used to establish stent models for patients with aneurysms using pre-operative imaging data as well as to pre-operatively formulate personalised and optimal surgery plans. An increasing convergence between medicine and engineering has recently occurred. A typical example of this medicine-engineering integration is the establishment of an arterial model using 3D modelling software and the calculation of the fluid model in the blood vessels using a fluid mechanics software. However, this integration has several limitations, including the relatively short implementation period and its unclear underlying concepts and goals. Moreover, achieving this integration is difficult as it is a multidisciplinary endeavour and compound talents are lacking. Addressing the aforementioned shortcomings can facilitate the efficient medicine-engineering integration, which can in turn greatly contribute in improving human life and health.
GH, growth hormone; MRI, magnetic resonance imaging; CT, computed tomography; CTA, computed tomography angiography; CRBV, change rate of brain volume; PBC, percutaneous balloon compression.
All authors designed the research study. JD and SZ performed the research. JD, LDJ, LPJ, and SH analyzed the data. JD wrote the manuscript. SH and SZ contributed to editorial changes in the manuscript. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research was supported by the Xingdian Talent Support Plan Project (XDYC-QNRC-2022-0320) and Joint Projects of Kunming University of Science and Technology and Medical Science (KUST-KH2023028Y).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.