


1 Clinical Laboratory, Quanzhou First Hospital Affiliated to Fujian Medical University, 362000 Quanzhou, Fujian, China
Abstract
Background: To analyze the polymorphism distribution of low density
lipoprotein receptor rs688, AvaII, NcoI gene in
ischemic stroke, and explore the linkage disequilibrium among them. The
correlation between the linkage disequilibrium and ischemic stroke was further
analyzed. Methods: The levels of serum lipid (triglyceride, cholesterol,
high density lipoprotein cholesterol, low density lipoprotein cholesterol,
apolipoprotein A1, apolipoprotein B) and rs688, AvaII,
NcoI polymorphism of low density lipoprotein receptor gene were tested
in patients with ischemic stroke (n = 140), healthy control (n = 129) and
patients with other cerebrovascular diseases (n = 122). Chi-square test was used
to compare the gene frequency and allele frequency of each group. Both the
linkage disequilibrium of the three genes and the alleles correlated with
ischemic stroke were analyzed. The correlation of linkage disequilibrium gene and
ischemic stroke was analyzed with logistic binary regression. Results:
In the ischemic stroke group, significant difference was observed in frequencies
and allelic frequencies of low density lipoprotein receptor (LDLR) rs688
and AvaII. No difference of NcoI was found. Linkage
disequilibrium was found for rs688 and AvaII (D’ = 0.927,
R
Keywords
- rs688
- AvaII
- NcoI
- genetic polymorphism
- ischemic stroke
Stroke is a disease with high incidence, disability rate, mortality and recurrence rate, which has been the leading cause of death and disability for adults in China. In the data from Global Burden of Disease (GBD) 2016, stroke had been the leading cause of life loss in China for many years [1, 2, 3]. The main types of stroke include ischemic stroke and hemorrhage stroke, and in 2016, the prevalence rates of ischemic and hemorrhage stroke were 1762.77 and 406.16 cases per 100,000 people, respectively [4]. The prevention and management of stroke, especially ischemic stroke has been a great public health concern in China.
There are ten manageable risk factors of ischemic stroke including hypertension, diabetes, dyslipidemia, heart disease, smoking, alcohol intake, unhealthy diet, abdominal obesity, physical inactivity and psychological factors [5]. In addition, genetic factors including genetic polymorphism have been widely investigated and proven to contribute to the occurrence of ischemic stroke [6, 7, 8, 9]. In various polymorphism studies, many have focused on the correlation between ischemic stroke and single nucleotide polymorphisms (SNPs) of low density lipoprotein receptor (LDLR) genes including rs11669576, rs5925 (AvaII), rs688, rs1122608 [10, 11, 12, 13, 14]. However, most studies investigated the frequencies and correlation of different SNP loci independently, and further studies are needed for the correlation between SNP loci as the linked gene and ischemic stroke [15, 16, 17].
Base on the correlation of rs688, AvaII and rs5742911 (NcoI) with ischemic stroke, we conducted this study to further investigate the linkage disequilibrium among the three genes and the combination of genes correlated with ischemic stroke.
We screened the patients with ischemic stroke who visited Quanzhou First Hospital between January 2019 and November 2019. Eligible subjects were those diagnosed as ischemic stroke for clinical manifestations including progressive dizziness, limb weakness, sudden headache, obnubilation and imaging findings on Magnetic Resonance Imaging (MRI) of intracranial or extracranial arterial stenosis or occlusion, new lesion of ischemic cerebral infarction, and etiology of large artery stenosis or small vessel occlusion. All the subjects did not receive standardized hypolipidemic therapy. Patients with obvious inducement for ischemic stroke such as trauma, infection, heart disease, and those with other cardiovascular and cerebrovascular diseases including coronary heart disease, heart failure and pulmonary vascular disease were excluded. Subjects with single comorbidity such as hypertension and head and neck atherosclerosis were included.
During the same period, patients with similar clinical manifestations but no intracranial or extracranial arterial stenosis or occlusion on MRI and diagnosed as cerebral hemorrhage, subarachnoid hemorrhage, intracranial aneurysm or other cerebrovascular diseases were included in the control group.
Healthy controls were matched from physical examination center synchronously for similar age and gender.
Clinical characteristics including age, gender, smoking history, alcohol consumption, underlying diseases including diabetes and hypertension were collected.
Height, weight and body mass index were not collected, for most of the patients were admitted in emergency and needed to rest in bed for the whole treatment. The protocol was approved by the Ethics Committee of Quanzhou First Hospital (approval number: [2018]213).
We tested serum lipid level and genetic polymorphism of peripheral venous blood samples which were obtained before treatment in the stroke group and other cerebrovascular disease group, and during physical examination in the control group.
Chemistry Analyzer (AU5800, Beckman Coulter Inc., Brea, CA, USA) was used for the test of triglyceride (TG), total cholesterol (TC), high density lipoprotein cholesterol (HDL-C), low density lipoprotein cholesterol (LDL-C), apolipoprotein A1 (ApoA1) and apolipoprotein B (ApoB). Calibration and quality control for instruments and reagents were applied before the test to ensure the accuracy of results.
DNA extraction Kit (Tiangen Biotech, Beijing, China) was used for the extraction of DNA from whole blood specimens. Primer was designed synthesized by Sangon Biotech (Shanghai, China), and the primer sequences and PCR products for rs688, AvaII and NcoI are listed in Table 1.
| Gene | Prime sequence | Allelic gene (WT/MT) | Polymerase chain reaction (PCR) product | |
| rs688 | F | CCCTCTGGGACTGGCATCA | C/T | 304 bp |
| R | AAGACCTCCTCCTAGTCACAAC | |||
| AvaII (rs5925) | F | GTCATCTTCCTTGCTGCCTGTTTAG | T/C | 219 bp |
| R | GGTTCCACAAGGAGGTTTCAAGGTT | |||
| NcoI (rs5742911) | F | GTCGTCTTTATGTCCGCCCA | A/G | 972 bp |
| R | CAGTGCAACAGTAACACGGC | |||
WT/MT, wild-type/mutant.
(1) PCR reaction system: 10
Clinical features and lipid level were described by
A total of 140 patients with ischemic stroke were included, 81 males and 59 females, with a median age of 64 years (range, 46–75 years). Another 122 patients with other cerebrovascular diseases were included, 59 males and 63 females, whose median age was 61 years (range, 46–83 years). 129 healthy controls consisted of 65 males and 64 females, with their median age being 61 years (range, 54–74 years). For clinical characteristics of the three groups, there were significant differences in smoking, hypertension, diabetes, systolic pressure, diastolic pressure, TG, HDL-C, ApoA1 between ischemic stroke group and healthy control group, while smoking, diabetes and diastolic pressure were also different between ischemic stroke group and other cerebrovascular disease group (Table 2).
| Healthy control | Patients with other cerebrovascular disease | Patients with ischemic stroke | |
| (n = 129) | (n = 122) | (n = 140) | |
| Age (years) | 61.87 |
61.89 |
62.40 |
| Male (%) | 50.77 | 48.36 | 57.86 |
| Smoking (%) | 13.85 | 9.02 | 27.86* |
| Alcohol intake (%) | 6.92 | 4.92 | 10.00 |
| Hypertesion (%) | 4.62 | 73.77* | 75.71* |
| Diabetes (%) | 7.69 | 14.75 | 34.29* |
| Systolic pressure (mmHg) | 125.87 |
155.74 |
149.04 |
| Diastolic pressure (mmHg) | 77.78 |
89.61 |
84.73 |
| TG (mmol/L) | 1.07 |
1.49 |
1.39 |
| TC (mmol/L) | 4.69 |
4.86 |
4.70 |
| HDL-C (mmol/L) | 1.38 |
1.20 |
1.14 |
| LDL-C (mmol/L) | 2.84 |
3.01 |
2.93 |
| ApoA1 (g/L) | 1.53 |
1.33 |
1.29 |
| ApoB (g/L) | 0.95 |
1.04 |
1.00 |
* p
The genetic polymorphism of LDLR rs688, AvaII, NcoI conformed to Hardy-Weinberg equilibrium, and all the alleles reached genetic equilibrium with group representativeness. The gene distribution and allele frequency of rs688 and AvaII in the ischemic stroke group were significantly different from those in the healthy control group and other cerebrovascular disease group, and there was no significant difference found in NcoI among the three groups (Table 3).
| LDLR gene | Genotype/ | Healthy control | Patients with other cerebrovascular disease | Patients with ischemic stroke | |
| allele [n (%)] | (n = 129) | (n = 122) | (n = 140) | ||
| rs688 | CC | 112 (86.82) | 86 (70.49) | 62 (44.29) | |
| CT | 15 (11.63) | 30 (24.59) | 66 (47.14) | ||
| TT | 2 (1.55) | 6 (4.92) | 12 (8.57) | ||
| HW (p-value)* | 0.093 | ||||
| X |
53.261 | 18.241 | |||
| p | |||||
| C | 239 (92.64) | 202 (82.79) | 190 (67.86) | ||
| T | 19 (7.36) | 42 (17.21) | 90 (32.14) | ||
| X |
51.030 | 15.421 | |||
| p | |||||
| AvaII | TT | 73 (56.59) | 68 (55.74) | 53 (37.86) | |
| TC | 53 (41.09) | 50 (40.98) | 66 (47.14) | ||
| CC | 3 (2.33) | 4 (3.28) | 21 (15.00) | ||
| HW (p-value)* | 0.061 | ||||
| X |
17.675 | 14.458 | |||
| p | 0.001 | ||||
| T | 199 (77.13) | 186 (76.23) | 172 (61.43) | ||
| C | 59 (22.87) | 58 (23.77) | 108 (38.57) | ||
| X |
15.468 | 13.197 | |||
| p | |||||
| NcoI | AA | 74 (57.36) | 56 (45.90) | 80 (57.14) | |
| AG | 48 (37.21) | 61 (50.00) | 54 (38.57) | ||
| GG | 7 (5.43) | 5 (4.10) | 6 (4.29) | ||
| HW (p-value)* | 0.828 | ||||
| X |
0.224 | 3.532 | |||
| p | 0.898 | 0.171 | |||
| A | 196 (75.97) | 173 (70.90) | 214 (76.43) | ||
| G | 62 (24.03) | 71 (29.10) | 66 (23.57) | ||
| X |
0.016* | 2.063 | |||
| p | 0.920* | 0.151 | |||
* HW (p-value): p value tested with Hardy-Weinberg law by
taking healthy control group; X
In comparison with healthy controls and a linkage disequilibrium between rs688 and AvaⅡ was observed in the patients with ischemic stroke (Fig. 1 and Table 4). In case-control
correlation analysis, the alleles found correlating ischemic stroke included
T of rs688 (X
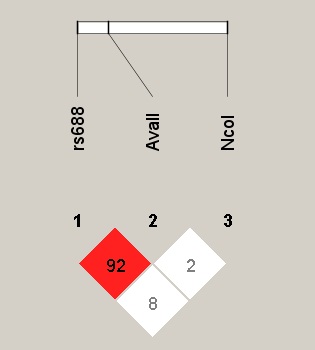 Fig. 1.
Fig. 1.LDLR rs688, AvaII, NcoI linkage disequilibrium. LDLR, low density lipoprotein receptor.
| Gene | D’ | LOD | R |
| rs688/AvaII | 0.927 | 56.4 | 0.509 |
| rs688/NcoI | 0.083 | 0.39 | 0.005 |
| AvaII/NcoI | 0.028 | 0.01 | 0.001 |
D’, degree of linkage disequilibrium; LOD, logarithm of odds.
Due to the linkage disequilibrium existing between LDLR rs688 and AvaII, rs688/AvaII as a whole was included in the analysis of risk factors of ischemic stroke. In comparison with healthy controls and patients with other cerebrovascular diseases, single factor analysis of patients with ischemic stroke showed that smoking, hypertension, diabetes, systolic pressure, HDL-C, ApoA1, rs688/AvaII were significantly correlated with the incidence of ischemic stroke (Table 5).
| Co-variants | B | S.E | Wals | p | OR (95% CI) |
| Age (years) | 0.025 | 0.014 | 3.299 | 0.069 | 1.025 (0.998 |
| Male (%) | –0.341 | 0.213 | 2.568 | 0.109 | 0.711 (0.469 |
| Smoking (%) | 1.084 | 0.273 | 15.761 | 2.956 (1.731 | |
| Alcohol intake (%) | 0.559 | 0.388 | 2.076 | 0.150 | 1.748 (0.818 |
| Hypertesion (%) | 1.616 | 0.236 | 46.882 | 5.034 (3.169 | |
| Diabetes (%) | 1.414 | 0.268 | 28.217 | 4.155 (2.457 | |
| Systolic pressure (mmHg) | 0.010 | 0.004 | 5.863 | 0.015 | 1.011 (1.002 |
| Diastolic pressure (mmHg) | 0.002 | 0.008 | 0.079 | 0.779 | 1.002 (0.987 |
| TG (mmol/L) | 0.107 | 0.101 | 1.115 | 0.291 | 1.113 (0.913 |
| TC (mmol/L) | –0.088 | 0.120 | 0.537 | 0.464 | 0.916 (0.723 |
| HDL-C (mmol/L) | –1.782 | 0.383 | 21.630 | 0.168 (0.079 | |
| LDL-C (mmol/L) | 0.018 | 0.136 | 0.017 | 0.895 | 1.018 (0.780 |
| ApoA1 (g/L) | –2.430 | 0.476 | 26.104 | 0.098 (0.035 | |
| ApoB (g/L) | 0.038 | 0.450 | 0.007 | 0.932 | 1.039 (0.431 |
| rs688/AvaII | 0.362 | 0.064 | 31.974 | 1.436 (1.267 | |
| NcoI | –0.173 | 0.183 | 0.896 | 0.344 | 0.841 (0.588 |
B, regression coefficient; S.E, standard error.
Multivariate analysis was performed on the above co-variants which were significantly related to the incidence of ischemic stroke. With the wild type gene (WT) of rs688/AvaII: CC/TT as reference, the logistic binary regression analysis showed that the incidence of ischemic stroke increased in rs688/AvaII: CT/TC, CT/CC and TT/CC, while decreased in rs688/AvaII: CC/TC (Table 6).
| Co-variants | B | S.E | Wals | p | OR (95% CI) |
| Smoking (%) | 0.962 | 0.351 | 7.510 | 0.006 | 2.617 (1.315 |
| Hypertesion (%) | 0.544 | 0.369 | 2.177 | 0.140 | 1.723 (0.836 |
| Diabetes (%) | 1.023 | 0.327 | 9.792 | 0.002 | 2.781 (1.466 |
| Systolic pressure (mmHg) | 0.003 | 0.007 | 0.145 | 0.703 | 1.003 (0.990 |
| HDL-C (mmol/L) | –0.862 | 0.864 | 0.994 | 0.319 | 0.423 (0.078 |
| ApoA1 (g/L) | –1.662 | 1.065 | 2.438 | 0.118 | 0.190 (0.024 |
| rs688/AvaII* | |||||
| CC/TC | –1.032 | 0.506 | 4.153 | 0.042 | 0.356 (0.132 |
| CC/CC | 22.669 | 23205.422 | 0.000 | 0.999 | 0.000 (/) |
| CT/TC | 1.482 | 0.322 | 21.129 | 4.400 (2.342 | |
| CT/CC | 3.026 | 0.839 | 13.005 | 20.615 (3.980 | |
| TT/TT | –20.174 | 28420.722 | 0.000 | 0.999 | 0.000 (/) |
| TT/TC | –21.007 | 28420.722 | 0.000 | 0.999 | 0.000 (/) |
| TT/CC | 1.980 | 0.673 | 8.664 | 0.003 | 7.240 (1.938 |
* With the WT genotype of rs688/AvaII: CC/TT as reference, we calculated the relative incidence rate of each rs688/AvaII gene polymorphism combination. There was no rs688/AvaII: CT/TT found in this study.
LDLR is a cell surface glycoprotein with a length of 839 amino acids which distributes widely in tissue cells. LDLR mediates the endocytosis of LDL and regulates serum LDL level via the recognition of apoprotein B-100 and chylomicron residues on LDL particles and apoprotein E on intermediate density lipoprotein [18, 19]. The coding gene of LDLR locates across 45 kb on chromosome 19p13.1-13.1, including 18 exons and 17 introns. Mutations of LDLR gene are common including point mutations, fragment deletions, insertions and rearrangements, and until now there have been more than 800 mutation types found worldwide [20]. The correlations between SNP site mutations of LDLR gene and atherosclerotic diseases such as coronary heart disease, carotid atherosclerosis, and ischemic stroke have been investigated extensively. Sinha and Salazar et al. [21, 22] proposed that AvaII may be a risk factor for coronary heart disease through the regulation of serum lipid level. The research of Jha suggested that TT genotype and allele T of rs688 might be susceptibility genes of coronary heart disease [23]. Meng reported that the efficacy of rosuvastatin in carotid atherosclerosis was closely related to the genetic polymorphism of rs688, and patients with CT type had limited relief of plaque [24]. Besides, rs11669576, AvaII, rs688, rs1122608, rs1433099 were also found to be correlated with atherosclerotic disease [10, 11, 12, 13, 14, 16, 25].
The above studies are mainly on the correlation of disease with genetic polymorphism of single SNP loci and the combination of different SNP loci, which fail to cover the analysis for linkage disequilibrium of genes. The correlation between the occurrence of disease and certain combination of genotypes needs to be further illustrated. In this study, we chose three common LDLR SNP loci, analyzed their frequency distribution in ischemic stroke, and further investigated the linkage disequilibrium between genes to find the specific genotype combination with linkage disequilibrium which may be important for the occurrence of ischemic stroke.
In our study, patients with ischemic stroke had a higher rate of C
Results of our analysis showed that linkage disequilibrium existed between
rs688 and AvaII genes (D’ = 0.927, R
Accordingly, it was indicated that there was a significant correlation between rs688/AvaII and ischemic stroke. Further in the multivariate analysis for ischemic stroke, with the WT genotype (rs688/AvaII: CC/TT) as reference, rs688/AvaII: CT/TC, CT/CC and TT/CC were found increasing the incidence of ischemic stroke, whereas rs688/AvaII: CC/TC reducing the incidence.
Patients selected in the ischemic stroke group in this study were all atherosclerotic, a type whose occlusions have already been proved in some works to be with a worse outcome compared to thromboembolic disease [28]. Therefore, the detection of rs688/AvaII genotype polymorphism combination may help to screen out the high-risk population of ischemic stroke. Early monitoring and predicting for these population will help prevent them from severe ischemic stroke with poor prognosis in the future.
Compared with control groups, the frequency distributions of LDLR rs688, AvaII gene polymorphism were significantly different in patients with ischemic stroke. Linkage disequilibrium was found between rs688 and AvaII genes. The genotype polymorphism combination of rs688/AvaII: CT/TC, CT/CC, TT/CC increased the incidence of ischemic stroke, which might be a genetic marker to be used for screening high-risk population, contributing to the prevention of the disease.
All authors consent to submit the manuscript for publication.
The data used to support the findings of this study are included within the article. The data and materials in the current study are available from the corresponding author on reasonable request.
YC—contributed to the study design and drafted of the manuscript; HC, YS—performed the experiment; JZ, ZZ—acquired the data and revised the manuscript; YW, ZL—performed data analysis. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study was approved by the Ethics Committee at Quanzhou First Hospital (NO. [2018]213), and subjects provided the informed consent authorizing the use of their clinical information and blood samples.
Not applicable.
The authors disclosed receipt of the following financial support for the research: Quanzhou City Science & Technology Program of China, grant number: 2018N060S.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.