

 , Luana Billeri 2, Alfredo Manuli 3, Antonio Iacono 4, Antonino Naro 5
, Luana Billeri 2, Alfredo Manuli 3, Antonio Iacono 4, Antonino Naro 51 IRCCS Centro Neurolesi Bonino Pulejo-Piemonte, 98124 Messina, Italy
2 Istituto Clinico Polispecialistico, C.O.T. Cure Ortopediche Traumatologiche s.p.a., 98124 Messina, Italy
3 AOU Policlinico “G. Martino”, Rehabilitation Unit, 98124 Messina, Italy
4 Ospedali Riuniti Villa Sofia-Cervello, Neurology Unit, 90146 Palermo, Italy
5 AOU Policlinico “G. Martino”, Stroke Unit, 98124 Messina, Italy
Academic Editor: Rafael Franco
Abstract
Transcranial magnetic stimulation (TMS), a non-invasive brain stimulation method, is trying to emerge as a migraine management strategy for both attack treatment and prevention. This scoping review presents 16 among single-pulse (to manage episodic and chronic migraine) and repetitive TMS randomized clinical trials (to manage chronic migraine). The works we reviewed suggest that TMS may be adopted as add-on therapy in those patients who are refractory to pharmacological therapy only with special arrangements for individualized treatment strategies or research. There are still limited clinical research programs and metaanalysis to promote routinely TMS employment, as TMS has been shown either to have no significant effects for any outcome or to be effective for migraine. These diverging conclusions depend on several biasing factors, including the lack of reliable, large, sham-controlled clinical trials, the dyshomogeneity in study designs (including the area of stimulation, the frequency of stimulation, the number of pulses, pulse intensity, and the number of sessions), patient selection criteria (migraine w/o aura, episodic and chronic migraine; TMS contraindication), and the lack of outcomes homogeneity and long-term real-world efficacy data. Therefore, in the future, it will be important to conduct larger randomized trials to confirm TMS usefulness in migraine management (acute attack and prophylactic treatment), identify those patients who may benefit from TMS, maybe independently of pharmacological treatments (i.e., using TMS as an alternative and not only as an add-on treatment). Otherwise, TMS will play a role in treating migraine only with special arrangements for individualized management strategies or research.
Keywords
- transcranial magnetic stimulation (TMS)
- migraine attack treatment
- migraine prophylactic treatment
- clinical trial
Migraine is one of the primary headaches according to the International Classification of Headache Disorder third edition (ICHD-3) beta, affecting about 15% of the population and causing severe impairment of the quality of life [1]. Owing to its genetic, environmental, and hormonal basis, migraine has become one of the most common nervous system diseases worldwide [2].
The physiopathology of migraine is complex (including several biochemical cascades, the cortical spreading depression phenomenon, and an enhanced central sensitization) and still partially unknown [3]. This partial knowledge makes it challenging to find proficient treatments [3]. Furthermore, pharmacologic therapies to relieve symptoms and the prophylaxis of migraine are sometimes inefficacious and can foster the risk of medication overuse headaches in some individuals. For these reasons, non-pharmacological treatments have been the object of research. Among these, single-pulse (sTMS) and repetitive transcranial magnetic stimulation (rTMS) have been studied to be implemented as both acute and preventive migraine add-on treatment options [4, 5, 6, 7, 8]. The rationale of using TMS to treat and prevent migraine attacks resides in the capability of TMS to affect cortical excitability beneath and far beyond the site of TMS application, with relevant effects on brain signaling. This is fundamental because migraine is a neuronal network disorder, whose modulation through different mechanisms and in different sites could be significant for migraine management. Notably, it seems that magnetic pulses could inhibit the cortical spreading depression and the related thalamocortical signaling [9], consistently with the evidence that targeting some brain areas with TMS may interfere with pain [8], thus blocking migraine attack and contributing to reducing migraine pain and frequency [10]. Overall, there seems to be practical, promising effects of TMS in reducing migraine frequency and intensity, but there is still no clear evidence.
The present narrative syntheses aimed at identifying peer-reviewed works describing the TMS paradigms implemented in migraine treatment, focusing on the pros and cons of this approach in the clinical management of migraine.
This literature review was developed according to the guidance for narrative syntheses [11, 12] and the Enhancing Transparency in Reporting the Synthesis of Qualitative Research (ENTREQ) reporting guidelines [13]. Our research focused on papers on TMS and migraine, using the research keywords “migraine” AND “transcranial magnetic stimulation”. Papers were searched from PubMed, MEDLINE, PeDro, Google Scholar, and Cochrane Database. We included peer-reviewed journal and English-written papers, regardless of the date of publication, if they described the clinical impact of TMS on migraine in adult humans. We included only pilot and/or randomized clinical trials to consider different aspects of migraine management. Papers were excluded if they did not fit into the study’s conceptual framework, focused on other headache types, or belonged to gray literature. The search strategies were drafted by A.N. and L.B. and further refined by R.S.C., who also solved any disagreements on article inclusion.
The first search returned 1005 papers (pruned from duplicates by A.N.). Two-hundred seventy-one articles were screened for eligibility using the abovementioned research keywords, main judgment criteria, and publication types. To this end, the papers were assessed, focusing on titles and abstracts. Therefore, 16 articles were included in the present review by a full-text assessment of the papers. All the reviewed studies are summarized in Table 1 (Ref. [14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29]). The flow diagram depicting the flow of information through the different phases of the review is reported in Fig. 1.
| Setup | Sample | Study design | Outcome | |
| Session number and pulses, intensity and site of stimulation | (n, age | |||
| Clarke 2006 [14] | two sTMS 5 s apart* | 42 EM (MA and MO) | randomized | both sTMS produced immediate, 24 h lasting, significant reduction in pain during the MA episode |
| 41.43 |
double-blind | |||
| 36 females | TMS-intensity controlled | |||
| Lipton 2010 [15] | sTMS inion | 164 EM (MA) | randomized | Significant lack of ma episodes up to 48 h compared to the sham group |
| 39.4 |
double-blind | |||
| 65 females | sham-controlled | |||
| O’Reardon 2007 [16] | 10 Hz 3000p 120% AMT left DLPFC | 2 MDD with CM | case-report | decrease in the number of headache days only following the real treatment |
| 1 d 5 w |
51y female | double-blind | ||
| 66y male | sham-controlled | |||
| Conforto 2014 [23] | 32 |
18 CM | randomized | significant decrease in the number of headache days in both groups |
| 3–4 w |
36.8 |
double-blind | ||
| not reported | sham-controlled | |||
| Teepker 2010 [17] | 2 |
27 EM (MA-MO) | randomized | significant decrease of migraine attacks in both groups |
| 1 d |
35.66 |
double-blinded | ||
| 22 females | sham-controlled | |||
| Amin 2020 [19] | 5 Hz 900p 100% RMT left DLPFC | 33 EM (MA-MO) | randomized | significant decrease of headache days compared to the sham group |
| 1 d |
34.8 |
double-blinded | ||
| 22 females | sham-controlled | |||
| Sahu 2019 [20] | 10 |
41 EM (MA-MO) | randomized | significant reduction of migraine severity in the active group up to 12 weeks |
| 2 d |
30.79 |
double-blinded | ||
| 31 females | sham-controlled | |||
| Misra 2012 [21] | 10 |
51 EM | randomized | significant reduction of headache days and migraine severity in both groups up to one month |
| 3 w | aged 16–61 | double-blinded | ||
| 45 females | sham-controlled | |||
| Kalita 2021 [27] | 10 |
83 CM | randomized | significant reduction of headache days in the rTMS + amitripty line group at 2 months; conversion of cm to em in 67% patients in the rTMS + amitriptyline group |
| 3 w |
31.12 |
double-blinded | ||
| w/o amitriptyline 25 mg/d | 72 females | sham-controlled | ||
| Kumar 2021 [24] | 10 |
20 CM | randomized | significant reduction of migraine severity (mean vas rating and midas scoring) up to 1 month in the real group compared to the sham group |
| 5 w |
33.5 |
double-blinded | ||
| 11 females | sham-controlled | |||
| Shehata 2016 [25] | 20 |
29 CM | open-label randomized | significant reduction of migraine severity in both groups, with a lasting effect only in the rTMS + BTX-A group (up to 12 weeks) |
| 3 w |
32.65 |
sham-controlled | ||
| 19 females | ||||
| Kalita 2016 [22] | 10 |
98 CM and chronic tension-type headache | randomized | significant reduction of headache days and severity in both groups, with a lasting effect in the real group |
| 3-real vs. 1-real + 2-sham sessions | 31.73 |
double-blinded | ||
| 79 females | sham-controlled | |||
| Starling 2018 [29] | preventive (4p 2 d every 15 min) and acute treatment (3p |
263 EM (MA-MO) | prospective, open label, observational study | significant reduction of headache days; significant reduction in pain during the MA episode |
| aged 18–65 | ||||
| not reported | ||||
| Brighina 2004 [26] | 10 |
11 CM | randomized | reduction of headache days and severity in the real group |
| 3 w |
47 |
double-blinded | ||
| 7 females | sham-controlled | |||
| Leahu 2021 [28] | 13 |
65 EM (MA-MO) | randomized | significant reduction of headache days and severity in real group |
| 39.7 |
double-blinded | |||
| 52 females | sham-controlled | |||
| Hammad 2021 [18] | 2 |
65 EM (MA-MO) | open label | significant reduction in pain intensity, frequency and duration of migraine attacks |
| 29.75 |
Observational study | |||
| 34 females | ||||
| Legend: AMT, active motor threshold; BTX-A, botulinum toxin A; CM, chronic migraine; DLPFC, dorsolateral prefrontal cortex; EM, episodic migraine; HC, healthy controls; iTBS, intermittent theta-burst stimulation; m, month; M1, primary motor cortex; MA, migraine with aura; MDD, major depressive disorder; p, pulses; RMT, resting motor threshold; sTMS, single-pulse TMS; d, day; w, week; w/o, with or without; *, over the area of perceived pain or over the area of the brain generating the aura (2 paired-pulses soon after attack onset, other paired-pulses every 15 min until pain and symptoms resolve anyway up to 2 h); #, bursts of three stimuli at 50 Hz repeated at 5-Hz frequency each train lasting for 2 s with an inter-train interval of 8 s; VAS, Visual Analogue Scale; MIDAS, Migraine Disability Assessment. | ||||
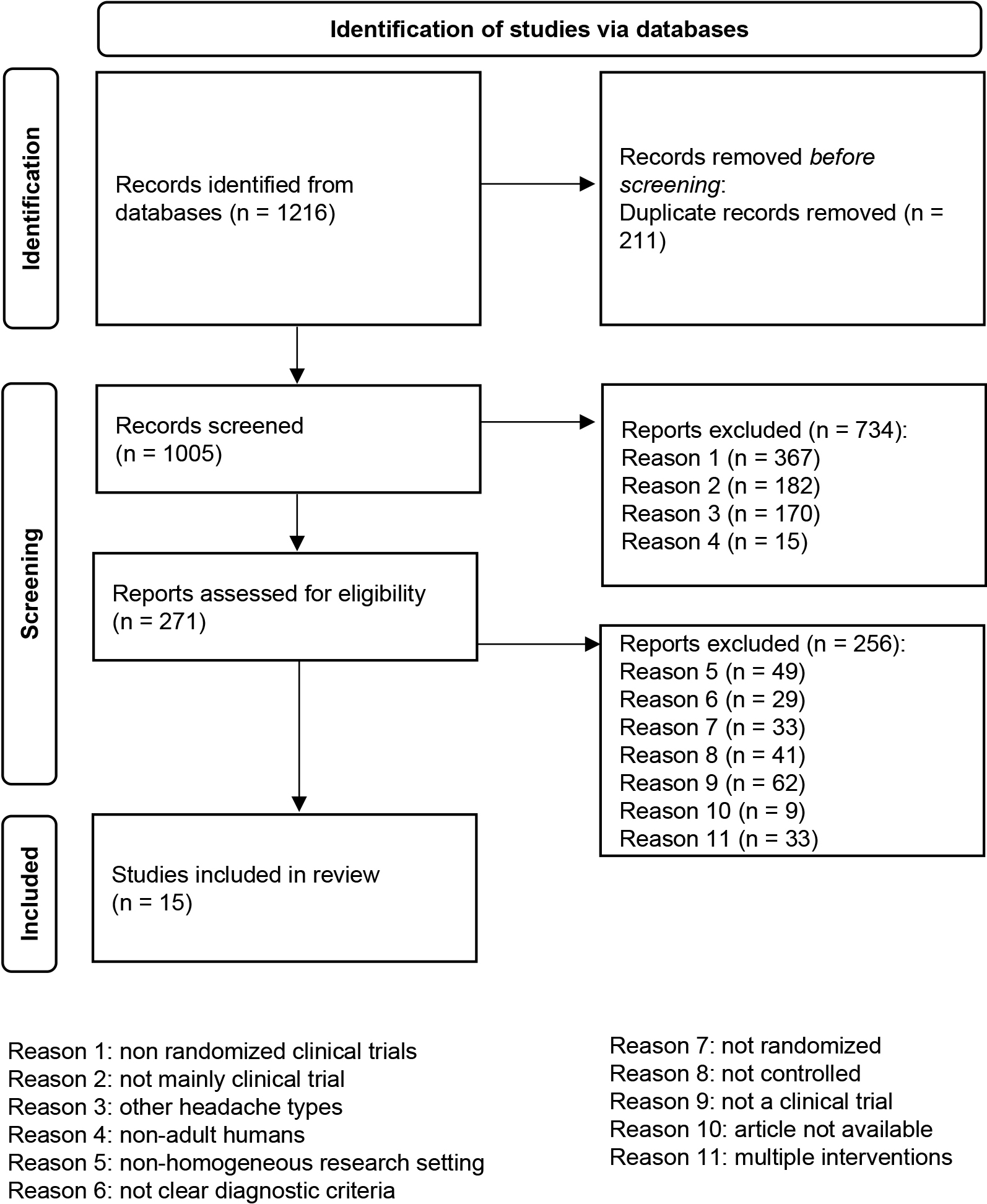 Fig. 1.
Fig. 1.The flow diagram depicts the flow of information through the different phases of the review. It maps out the number of records identified, included and excluded, and the reasons for exclusions.
The available studies on TMS application to migraine can be grouped into (i) treating and (ii) preventing the migraine attack. Regarding the former group, sTMS was applied, whereas both sTMS and rTMS were used to prevent migraine attacks.
sTMS was initially applied as an alternating real and sham pulsed magnetic field to different scalp sites, including the occipital region, in 40 patients with headache (thus, not only migraine), with positive results in terms of headache frequency and intensity reduction [30]. The study by Pelka et al. [31] adopted a global magnetic field with good results in terms of attack interruption.
Other studies applied sTMS in 42 [14] and 164 patients with migraine (82 real sTMS and 82 sham sTMS) [15] over the painful area of the skull (in migraine without an aura) or over the occipital cortex (in migraine with aura) within one hour after the aura onset, achieving a reduction in headache intensity up to the complete headache abortion for 24 h in 32% of the patients reported. Only minor side effects (including headache, migraine, sinusitis, and paresthesia) were appreciable, without significant between-group differences.
Finally, 190 patients (59 individuals with episodic migraine with or without, and 131 with chronic migraine) who were provided with sTMS (according to [14] and [15]), participated in a 3-month telephone survey. The subjects reported a significant clinical improvement in 62% of patients, including the reduction in monthly headache days and attack duration in both episodic and chronic migraine, in addition to a reduction in disability [32].
rTMS has been implemented only for a prophylactic action on migraine. A first double-blind study with real and sham rTMS on two patients with migraine and major depression reported the disappearance of migraine [16]. High-frequency (20 Hz) rTMS over the left dorsolateral prefrontal cortex (DLPFC) in six chronic migraine patients compared to five sham-rTMS patients was shown to be effective for prophylaxis of migraine, including attack frequency, headache index, and the number of acute medications. On the contrary, lower frequency rTMS (10 Hz over the left DLPFC [33], or 1 Hz rTMS over the vertex [17]) were ineffective. On the contrary, an open-label observational study employing 1 Hz rTMS over the vertex obtained a significant reduction in pain intensity, frequency and, and the duration of migraine attacks [18].
Two other studies applying 5 Hz [19] and intermittent theta-burst [20] stimulation of the left DLPFC showed partially positive data in the primary outcome (i.e., reduction of headache-days per month).
Instead, a single session of high-frequency rTMS (600 pulses at 10 Hz) over the left primary motor cortex (M1) reduced the number of headache days per month (of about 3 days), the migraine attack intensity, the quality of life impairment, and the painkiller intake, particularly within the first two weeks after the paradigm application in a chronic migraine sample [21]. Notably, providing the patients with three of these sessions was not significantly superior to the single session [22]. An 8-week, high-frequency rTMS protocol over left DLPFC in chronic migraine individuals was feasible and safe, but inferior to sham rTMS to decrease the number of headache days. Thus, M1 stimulation with rTMS seems a more promising target than the DLPFC does [23]. In a double-blind, parallel-group, randomized clinical trial employing neuronavigated TMS, the researchers delivered 600 pulses at 70% of resting motor threshold patterned in 10 trains at 10 Hz with an inter-train interval of 60 s in a daily session to the left M1. This paradigm was repeated 5 days per week, over two consecutive weeks. The authors found a significant, one-month lasting reduction in the mean pain rating scale, headache frequency, and Migraine Disability Assessment questionnaire in the real rTMS group [24].
High-frequency rTMS (10 Hz, 2000 pulses per session) over the left M1 was not superior to botulinum toxin-A injection up to 8 weeks post-treatment, but it was less effective at 12 weeks [25]. A 20 Hz-rTMS study over left M1 was shown to reduce attack frequency, headache index, and the number of abortive pills used for up to 2 months [26]. Lastly, high-frequency rTMS has been reported effective in converting chronic migraine to episodic migraine, particularly when combined with amitriptyline, compared to rTMS alone [27].
On the sidelines, we report on a deep TMS study aimed at relieving pain in chronic migraine patients. The authors reported that high-frequency deep TMS of both DLPFCs was more effective than the standard pharmacological treatment alone in reducing the frequency and intensity of migraine attacks, drug overuse, and depressive symptoms, thus resulting as a potentially helpful add-on strategy in chronic migraine [34].
An innovative approach described in a randomized, double-blinded, sham-controlled study employing swiping and, soon then, multifocal-spot high-frequency rTMS in episodic migraine patients significantly reduced headache days and severity [28].
sTMS has also been studied as a preventative treatment. In a multi-center, prospective, open-label, observational study, 217 patients were provided with daily sTMS treatment for 3 months (3 consecutive pulses as needed for acute therapy, with the possibility to add other two pulse-sequences if pain relief was not achieved within 15 min; 4 pulses twice daily were instead delivered as a preventative therapy). It was found a mean reduction of about three headache days from baseline versus placebo and a reduction in acute medication use and disability [29].
Forty-two migraine patients with both migraine with aura and migraine without an aura were provided with paired-pulse sTMS (at either 50% or 30% of the maximum stimulator output) soon after attack onset. The percentage of patients complaining of migraine relief, mainly those among migraine with aura, increased with increasing stimulation rounds, suggesting a cumulative effect of sTMS, which was used to treat episodic migraine [14].
Finally, we mention a prospective, open-label, observational study pilot study
carried out on twelve adolescents (12–17 years old, mean age 15
The works we reviewed were carried out in adults aged 18–65 with primary or secondary headaches provided with TMS compared to sham/placebo or alternative standard of care. Headache frequency and duration, medication use, anxiety, quality of Life, and function improved following TMS in about 50% of enrolled patients, but this did not seem statistically different from sham treatment. This limited evidence suggests that TMS may be adopted as add-on therapy in those patients who are refractory to pharmacological treatments only in specific research or clinical contexts. There are still limited clinical research programs and metaanalysis that would lead to a different conclusion. Some reviews and meta-analyses concluded that TMS has no significant effects for any outcome [7, 8, 36], whereas other reviews proposed that TMS is effective for migraine, although admitting that there is still insufficient evidence to promote its large-scale use in clinical settings [4, 5, 6, 37]. These diverging conclusions depend on several biasing factors, including the lack of reliable, large, sham-controlled clinical trials, the dyshomogeneity in study designs (including the area of stimulation, the frequency of stimulation, the number of pulses, pulse intensity, and the number of sessions), patient selection criteria variability (migraine w/o aura, episodic and chronic migraine, absolute contraindication for TMS application), and the lack of outcomes homogeneity and long-term real-world efficacy data. Therefore, we have at first to summarize the pros and cons of TMS in migraine management to achieve a balanced conclusion on TMS usefulness in migraine.
The data from our literature review indicate that TMS can consistently reduce the number of migraine days per month, mitigate the intensity and duration of migraine attacks for several days after TMS application, up to one month, interrupt migraine attack quickly, and improve the quality of life. In addition, TMS is safe and well-tolerated, also considering that the majority of trials employed subthreshold stimulation intensities, as only mild light-headedness, tinnitus, dizziness, paresthesia, tinnitus, scalp discomfort, and worsening of migraine have been reported [38]. Furthermore, the more specific theoretical mechanisms of action of TMS, the reversibility of any potential side effects, and the minimal-risk options for drug interaction (i.e., a prophylactic pharmacologic therapy seems not to influence the efficacy of rTMS) are other strength points [39].
Although such non-invasive neuromodulation devices are relatively expensive, TMS seems cost-effective in some cases (e.g., cheaper than botulinum toxin-A for chronic migraine treatment, cheaper than the whole, complex pharmacological management of chronic migraine) [40, 41, 42, 43, 44, 45, 46].
The effectiveness of TMS in managing migraine critically depends on the stimulation paradigm employed. Migraine reduction improves while increasing the number and intensity of stimuli, suggesting a cumulative effect of TMS stimuli consistently with neuroplasticity principles [47]; however, this is not an absolute rule as sham TMS outperformed real TMS in some clinical trials. There is also a consistent variability in the number of sessions (ranging from one to 12), the overall number of pulses, and the number of pulses per session (from 600 to more than 20000). Another critical factor is the stimulation target. TMS seems more effective when applied to the M1 than to the DLPFC or the vertex [48], although the research of TMS over the DLPFC is growing [49].
Furthermore, TMS efficacy is significantly influenced by the stimulation frequency selection. The number of migraine attacks and days did not differ significantly between real and sham low-frequency rTMS [17]. Conversely, high-frequency rTMS often promoted more evident migraine improvement. The greater efficacy of high-frequency rTMS may lie in its capability to engage several functionally connected brain networks through a spatial summation process [50]. Furthermore, the high-frequency stimulation may have a temporal resolution sufficient to interfere more with the network connectivity (i.e., the migrainous brain is hyperexcitable between attacks), which is related to migraine attack generation.
Patients’ selection is another factor limiting judgement on TMS usefulness in migraine management. Indeed, most of the available clinical trials enrolled female-dominated samples of patients who were refractory to pharmacological therapy, thus limiting the generalizability of the present findings to the entire migraine population [51]. Furthermore, patients with episodic migraine complained of at least four episodes a month. The number of patients with migraine with aura was exiguous. Finally, most studies enrolled episodic and chronic sufferers without differences in improvement, although chronic migraine seems to respond better to rTMS than episodic migraine does [21].
This issue, together with the lack of reliable, large, sham-controlled clinical trials (actually, the reviewed clinical trials were all randomized but lacked random sequence generation or concealed allocation) and the relatively high costs of the devices, limit the widespread use and clinical applications of noninvasive neuromodulation therapies.
A non-negligible problem related to the large-scale clinical use of TMS in migraine is the not yet complete knowledge of TMS mechanisms of action in migraine concerning both the prophylactic treatment (mainly rTMS) and the acute phase treatment (sTMS). However, a solid rationale for adopting TMS to manage migraine remains.
Migraine patients’ cortical excitability and connectivity are largely abnormal
and intimately correlated with migraine attack pathogenesis [52]. Furthermore,
migraineurs’ brain shows an abnormal responsivity to TMS pulses as suggested by
high-amplitude motor evoked potentials [53], lower phosphene threshold [54, 55, 56],
high sensitivity of M1 to light exposure during both the pre-ictal and ictal
phases of migraine [57, 58]. This baseline hyperexcitability concerns the M1 and
DLPFC, which play a significant role as pain modulators, and the secondary
somatosensory cortex. Furthermore, the baseline activity of such brain areas,
which seems largely abnormal in chronic pain conditions [59, 60], has been
proposed to tune other pain-associated neural areas [61]. Similarly, thermal pain
measures and cold and heat pain threshold are largely abnormal in migraineurs
compared to healthy controls, suggesting a reduced intracortical inhibition and a
hypofunction of inhibitory pain modulation mechanisms [62]. All these issues
justify the potentially positive response of patients with migraine with or
without aura to rTMS, which has been estimated putatively capable of reverting
the mentioned above (mal) adaptive plasticity in chronic pain conditions [63, 64].
Contemporarily, these baseline alterations may explain some of the paradoxical
responses of the M1 in migraine to both inhibitory (low-frequency) or
facilitatory (high-frequency) rTMS paradigms [65, 66, 67, 68, 69], explaining the
reason why sham-rTMS was often superior to real-rTMS. However, over and above
that, high-frequency rTMS carries a high potential of inducing a placebo effect,
which can be usefully leveraged to enhance patients’ coping strategies [70].
Furthermore, rTMS over sensorimotor and premotor regions seems to entrain various
biochemical mechanisms related to pain control, including plasma
Regarding migraine with aura, TMS is proposed to challenge the spread of
cortical spreading depolarization, particularly when applied over the occipital
cortex [72]. High-intensity TMS pulses may inhibit the cortical spreading
depolarization by activating inhibitory GABA
Our analysis has some limitations to acknowledge. First, we included only published clinical trials. It is thus necessary to be cautious when making conclusions that come from synthesizing evidence. Even though randomized, double-blind, controlled clinical trials provide reliable results, we had to include only 16 trials in this analysis, thus likely limiting us from achieving any different outcome for TMS employment in migraine management. Furthermore, all studies in the analysis presented lots of heterogeneity, including lack of grouping by migraine severity, sexuality, age, paradigm setup, and migraine pharmacological treatment.
Moreover, the patients enrolled in the studies came from general hospitals or major institutions, which somehow limits data generalizability. Lastly, we did not assess of quality bias or blinding validity in the included trials. However, this type of assessment may be challenging and unreliable, as a quantitative synthesis could be hard to perform consistently with the significant heterogeneity in headache type studied, protocol stimulation parameters, location and duration of treatment, and outcome measures.
To summarize, there is no robust evidence to suggest the application of TMS in migraine due to the few available randomized trials, nearly all with a sham arm but mostly underpowered. Therefore, these data cannot be generalized to all migraine patients [73, 74, 75]. Furthermore, the response rate for TMS seems to be not superior to that of the preventive drug treatment [76]. However, there are several promising data on the prophylactic role of TMS in migraine, as also recognized by the FDA, which approved some TMS devices for the migraine attack treatment. For these reasons, it is trying to reduce the costs of non-invasive brain stimulation related to the underlying engineering and biotechnology research [74].
Therefore, more randomized controlled trials are required to clarify the migraine pathophysiology (particularly the cortical spreading depression and the thalamocortical cross-talk) [77], possibly adopting simultaneously or deferred functional neuroimaging and neurophysiological studies methods, and analyze the safety of long-term or frequent use of TMS. Furthermore, a better pathophysiological knowledge could be important to identify the best migraine candidate o non-invasive brain stimulation. Finally, the potential interaction between non-invasive brain modulation and the newly available drugs for treating and preventing migraine attacks, including ditans, calcitonin gene-related peptide monoclonal antibodies, and gepants is still to be seen. In this regard, it will be very important to conduct larger, properly blinded, and controlled trials to confirm TMS usefulness in migraine management (acute attack treatment and/or prophylactic treatment) maybe independently of pharmacological treatments, i.e., using TMS as an alternative and not only as an add-on treatment. In this way, the patients who may benefit from TMS could also be identified. We, therefore, advise that now TMS should be used only in specific research or clinical contexts until proven otherwise.
CGRP, calcitonin gene-related peptide; CSD, cortical spreading depression; DLPFC, dorsolateral prefrontal cortex; EM, episodic migraine; M1, primary motor cortex; MA, migraine with aura; MEP, motor evoked potentials; MO, migraine without an aura; rTMS, repetitive transcranial magnetic stimulation; sTMS, single pulse transcranial magnetic stimulation; TMS, transcranial magnetic stimulation.
AN and LB conceived and designed the review; LB performed the research; AN analyzed the data; AM and AI supervised the procedures; AN wrote the paper; RSC reviewed and validated the paper.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest. RSC is serving as one of the Editorial Board members/Guest editors of this journal. We declare that RSC had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to RF.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.