
 , Georgios Stranjalis 2, Maro Gavra 3, Efstathios Boviatsis 4, Stefanos Korfias 2
, Georgios Stranjalis 2, Maro Gavra 3, Efstathios Boviatsis 4, Stefanos Korfias 21 Neurosurgical Department of Pediatric Hospital of Athens, ‘Agia Sophia’, 11527 Athens, Attica, Greece
2 Medical School, University of Athens, First University Neurosurgical Department, ‘Evangelismos’ Hospital, 10676 Athens, Attica, Greece
3 Radiology Department of Pediatric Hospital of Athens, ‘Agia Sophia’, 11527 Athens, Attica, Greece
4 Medical School, University of Athens, Second University Neurosurgical Department, ‘Attikon’ Hospital, 12462 Athens, Attica, Greece
Academic Editor: Giovanni Grasso
Abstract
The current management strategy of hydrocephalus mainly involves the insertion of a ventriculoperitoneal shunt and is inherently related with a complication widely known as shunt over-drainage. Albeit this is a well-recognized complication, the true incidence and severity of this phenomenon remains undefined and most probably underdiagnosed, necessitating a more comprehensive pathophysiologic and therapeutic consideration. The slit ventricle syndrome is intimately related with the entity of shunt over-drainage, although who’s the definition of the former is implicated by a lack of universally accepted inclusion criteria. Another point of controversy is related with the absence of widely accepted criteria that would be able to discriminate the existing differentiations between these two entities. This is reflected in the fact that there are many proposed, relevant, treatment protocols. The background for all this data is based on the uncertainty and ambiguity regarding the pathophysiological mechanisms that are implicated. Current efforts are centered on the implementation of precautionary measures, as well as on treatment of both of these entities. Currently, there are enough evidence that support the concept that prevention of siphoning via the use of gravitational valves or antisiphon devices is the most efficacious means contained in our current therapeutic armamentarium. We attempt to present an overview of this complex entity, emphasizing on the hydrodynamics of the cerebrospinal fluid circulation in conditions harboring a ventriculoperitoneal shunt, the effect of the siphoning effect and the role of programmable valves and anti-siphon devices in our effort to eliminate this phenomenon. Based on an extensive literature review and on expert opinion, we concluded that the insertion of an anti-siphon device (gravitational shunt valves) could reliably address the issue of over-drainage, when a patient assumes a vertical position. Besides that, there are ongoing prospective studies centered on the safety and efficacy of adjustable gravitational valves, whose results are of ultimate importance. It is of paramount importance to be recognized that, due to the complexity of the pathophysiology of shunted hydrocephalus, lifelong follow-up of patients with ventriculoperitoneal shunts is necessary.
Keywords
- shunt over-drainage
- anti-siphon device
- programmable valve
- pediatric hydrocephalus
Hydrocephalus currently consists the most commonly encountered pathological entity related to neurosurgery in the pediatric population [1, 2, 3, 4]. The affected individuals constitute a relatively large proportion of the children population that is admitted to the hospital [5]. It is common concept that the most commonly selected treatment option involves the insertion of a ventriculoperitoneal shunt. Nevertheless, even-though the insertion of a shunt device is definitively associated with improvement of the survival rate, its use is not devoid of complications that interfere with the quality of life of the affected individuals [3]. In an effort to overcome these shortcomings of the available drainage systems, several technical adjustments have been investigated, in order to ameliorate the inherent limitations that accompany the use of a shunt system [6].
Nowadays, it is common concept that cerebrospinal fluid shunting via the introduction of a ventriculoperitoneal shunt system constitutes the most efficacious treatment modality for the management of hydrocephalus, irrespective of its underlying pathophysiology. Albeit this procedure has definitely proved to be a live-saving operation, capable of improving the quality of life of the affected individuals, we should not ignore the fact that it is accompanied by a wide spectrum of complications. Over-drainage of cerebrospinal fluid (CSF) is currently recognized as one of the most devastating and difficult to manage complications after ventriculoperitoneal shunt implantation. It may present with a wide spectrum of clinical manifestations, ranging from postural headaches, subdural hematomas hygromas, secondary stenosis/occlusion of the aqueduct of Sylvius, secondary craniosynostosis, slit ventricle syndrome, as well as ventricular catheter obstruction [7, 8]. The exact incidence of shunt over-drainage is yet to be specified, as a wide divergence exists between the reported incidence rates, which range between 2% and 71%. This could be attributed to the inhomogeneity that exists between different study populations, duration of follow-up, and to the lack of a uniformly accepted definition for over-drainage [9, 10, 11, 12, 13, 14, 15, 16, 17].
The basic tenet of our study is to review the entities of shunt over-drainage and slit ventricle syndrome, which are among the most devastating complications associated with the insertion of ventriculoperitoneal shunts in the pediatric population, as well as to discuss the relevant technological advancements that aim to counteract these side effects. Namely, the entity of siphoning, as well as the usefulness of anti-siphon devices and programmable valves are analyzed, taking into consideration the current trends in the literature.
The “normal” range of intracranial pressure (ICP) measurements ranges from 10
The basic tenet of the insertion of a VP shunt is to provide a route in order to
effectively bypass the transdural route of CSF absorption, by utilizing a
relatively low resistance pathway, especially in subjects suffering from with
increased CSF outflow resistances. The flow in this pathway is determined by the
perfusion pressure (PP) or the differential pressure (DP) across the valve. There
are several reports that have mentioned that ICP can be in the range of –15 to
–35 cmH
The development of this anatomical configuration of the ventricular system, which is accompanied by a constellation of clinical symptoms, represents a well-known entity that appears secondarily to the insertion of a ventriculoperitoneal shunt, mostly encountered in the pediatric population. Although its true incidence is probably underestimated, it complicates about 4%–37% of patients who are surgically treated for the management of hydrocephalus [23, 24, 25, 26, 27].
As the exact pathophysiologic mechanism that underlies the development of that syndrome is under investigation and not universally accepted, a relevant divergence between authors views persists. This refers to the adoption of a widely accepted definition that could precisely describe the entity of slit ventricle syndrome. As a consequence of that, there is a lack of agreement regarding the development of a protocol that could be considered as a treatment algorithm for the affected individuals. This confusion could be partly attributed to the fact that, although there is a bulk of evidence and reports in the literature which attempt to delimit this entity, there is no consensus about the specific characteristics that should be fulfilled by the affected individuals in order to be classified under this term. Based on strict radiological criteria, a percentage that approaches 50% of shunted children could be regarded as eligible candidates in order to be grouped under the entity of slit ventricle syndrome. When the clinical criterion is taken into consideration, that is the existence of recurrent headaches, these individuals may be categorized under at least 5 clinical groups [28, 29, 30, 31]. The fact that the definition of this syndrome necessitates a combination of imaging and clinical prerequisites and, also, the considerable overlap among the proposed inclusion criteria, constitutes an objective obstacle in our effort to register a widely accepted treatment algorithm.
Table 1 (Ref. [31, 32]) includes the most relevant and widely accepted clinical and radiological criteria that underline the term ‘slit ventricle syndrome’.
| Clinical criteria | A triad that involves intermittent headaches lasting 10 to 90 min, small ventricles on imaging studies, and slow refilling of the pumping mechanism of the valve. | [32] |
| Radiologic criteria | Progressive and excessive reduction of ventricular size. Fronto-occipital horn ratio (mean of the sum of the greatest diameter of the frontal + occipital horn/maximum lateral diameter of the cranium) |
[31] |
According to our opinion, the combination of the clinical and radiographic criteria that are presented above could be proposed as a set of minimum defining criteria for future works.
The most widely accepted clinical patterns which may be associated radiologically with slit ventricles are: true over-drainage with negative pressure, an on-off symptom complex, recurring proximal ventricular dysfunction, chronic subdural collections due to shunt over-drainage and headaches unrelated to shunt function. Our review of literature reports regarding SVS revealed a study based on experts’ experience, which defined SVS as a triad involving intermittent headaches lasting 10 to 90 min, small ventricles on imaging studies, and slow refilling of the pumping mechanism of the valve [7].
The aforementioned clinical groups are related to the proposed underlying mechanism that interfere with their clinical presentation. The first group is associated with intracranial hypotension. More precisely, these patients suffer from severe headaches that are not evident while they adopt a supine position. On the contrary, the headache appears during the activities of daily living and is substantially deteriorated as soon as the patient maintains an upright posture. The only effective means of improvement is the assumption a supine position. Monitoring shows a significantly subnormal ICP.
The second subgroup is related to the entity of intermittent proximal obstruction, or the “on-off symptom complex”. This condition probably represents the most common of the five clinical manifestations of the syndrome and it refers to patients who were originally diagnosed as suffering from SVS. Monitoring shows that the ICP of those patients varies within normal to low range during most of the day, although ICP values increase abruptly with activity. During this time period of raised ICP, the clinical equivalent consists of a worsening headache, until the ventricular catheter regains its patency and the pressure reverts to normal again.
The third group of affected individuals is characterized by the fact that they
suffer from increased ICP with a working shunt, also named as cephalocranial
disproportion. This entity has been universally observed in the context of
hindbrain herniation (Chiari I), as well as is strongly related with underlying
craniofacial disorders such as premature closure of the lambdoid and coronal
sutures, Crouzon’s and Pfeiffer’s syndrome. The next subcategory is universally
considered as the most difficult entity to manage
Mechanisms of ASDs:
Currently, three types of ASD design exist, named diaphragm, gravity, and flow reducing devices. An explanation of what kind of machine structure indicates ASDs follows.
(a) Diaphragm devices (membrane-controlled devices).
This type of anti-siphon includes one or two pressure sensitive membranes, which are located at the upstream of the distal catheter. In 1973, Portnoy and Schulte he first to design a device acting as an antisiphon valve [33, 34]. The diaphragm is normally displaced from the crown seat as long as the inlet pressure, which stands for the ICP, is greater than atmospheric pressure. The net result of this is that CSF is allowed to flow through. On the other hand, in case that the outlet pressure drops below atmospheric pressure, as a result of the suction effect of the distal water column, the diaphragm is pulled towards the crown seat, which eventually closes the water channel. The magnitude of the exerted pressure, that is the value of ICP, required in order to prevail over the siphon effect, that is the vertical length of the distal water column, is proportional to the ratio of inlet and outlet of the diaphragm device.
(b) Gravitational devices (ball-in-cone devices and g-valves).
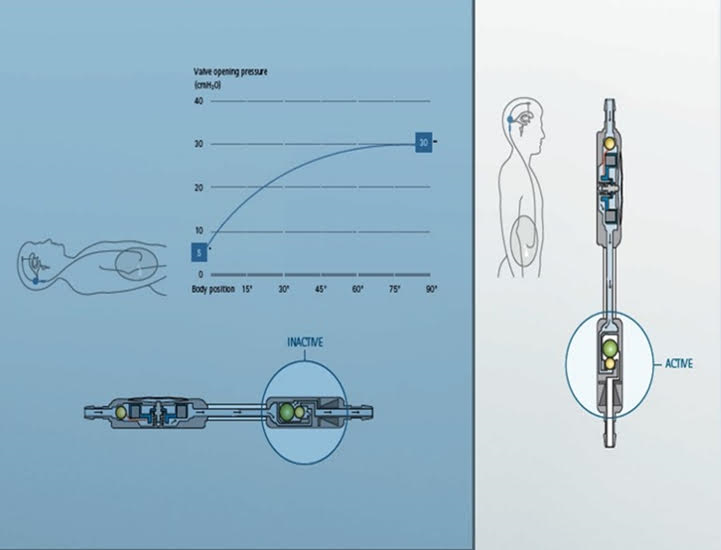
This type of anti-siphon incorporates one or several metal spheres which are included in a titanium cylinder with a cone shaped seat. The middle column of the water channel is with an inverted direction. When the device assumes a horizontal position, the metal balls roll away from the inlet, thus permitting CSF passage. When the device adopts a vertical position, the metal balls seat on the cone. The main structural concept underlying the construction of this device is that the addition of extra pressure depends on the weight of the balls against the entering flow of CSF. The pressure setting of the gravitational device does not interfere in any way the opening pressure in horizontal position. In combined types of valves, the opening pressure in vertical position is calculated as being the sum of the DP unit and the gravitational unit.
(c) Flow reducing devices (names as “flow regulated”, “flow regulating”, “auto-regulating”, “flow controlled”, “low flow”, and “variable-resistance” devices).
This type of device attempts to reduce the flow of CSF depending on the differential pressure, instead of body posture changes. That is, with strict formal criteria, they should not be considered as an “antisiphon” device. Nevertheless, this mechanism is used to be discussed along with true antisiphon devices, as they both share in common an ultimate goal, that is the prevention of over-drainage. The most distinct feature of this subcategory of devices is that their function is not intimately related with body posture. These devices lack the inherent characteristics that accompany an original anti-siphon device. Their function is rather based on flow reducing and not counteracting siphon effect. It deserves special mention that in patients suffering from slit ventricle syndrome, there may not be adequate amount of CSF, capable of producing flow above the threshold of state switching.
When premature neonates (aforementioned as up to 36 weeks gestation) are taken into consideration, the development of slit like ventricles is a common occurrence, manifesting in about 90% [35]. Over-drainage is a phenomenon that should be attributed to a combination of vasogenic and postural mechanisms. In normal individuals, the term vasogenic effect is utilized in order to refer to the intermittent elevations of the intracranial pressure which could be attributed to nocturnal vasogenic events, usually exaggerated by REM sleep. The net effect of such an event is the propulsion of CSF toward the spinal subarachnoid space [36]. When patients harboring a CSF shunt are considered, the result of the combination of nocturnal vasogenic events, along with diurnal postural effect, is the drainage of CSF into the peritoneal cavity and not its maintenance within the subarachnoid spaces.
At this moment, we consider that brief explanations of the theories mentioned below should be provided for those readers less familiar with their details, in order to show how they relate to the topic of discussion. Pascal’s principle, also called Pascal’s law, in fluid (gas or liquid) mechanics, statement that, in a fluid at rest in a closed container, a pressure change in one part is transmitted without loss to every portion of the fluid and to the walls of the container. The principle was first enunciated by the French scientist Blaise Pascal.
The general form of the law is
Molecular Cohesion Theory or Cohesion-tension theory was proposed by Dixon and Jolly in 1894. Water molecules have a strong mutual force of attraction called cohesive force, due to which they cannot be easily separated from one another. The attraction between a water molecule and the wall of the xylem element is called adhesion.
In fluid dynamics, Bernoulli’s principle (equation) states that an increase in the speed of a fluid occurs simultaneously with a decrease in static pressure or a decrease in the fluid’s potential energy. The simple form of Bernoulli’s equation is valid for incompressible flows.
The term ‘siphoning’ refers to the physical phenomenon where fluid continuously flows through an inverted U-shaped tube connecting two containers positioned at different heights. The fluid is “suctioned” from the compartment with higher potential energy, while the lower compartment is always the final destination. The adequate and necessary condition in order to achieve continuous fluid flow is the existence of a hydrostatic pressure differential. The traditional theory, which is based on Pascal’s principle and Stevin’s law, combined with the novel molecular cohesion theory, provides the physical basis of the siphon effect [37].
Studies focusing on siphoning are based on the Bernoulli equation as a theoretical background to elucidate all aspects of this effect. As a general rule, a VP shunt resembles a hydraulic conduit which connects the intracranial and intra-abdominal compartments, which obeys to the laws that are related to the siphoning effect, when the system adopts a vertical position.
Since the 1970s, a lot of efforts have been made in order to adequately manage the consequences that are intimately related with the effect of gravitational forces, that is postural drainage effects. We have to mention that the shunt over-drainage syndrome is affected by a divergent group of parameters postural effect constitutes a significant contributor, but is far from been considered as the only determinant of this phenomenon. Under the general term “Antisiphon”, or more precisely, “over-drainage-preventing” devices, are included accessory devices that are connected in tandem and peripherally to the main valve mechanism of the shunt system, regardless of the underlying mechanism of action that is inherent with each individual device. Although there is significant improvement regarding the technical aspects of the synchronous anti-siphon devices, we are far away from the desired end point, which is to dispose the optimum over-drainage-preventing device.
Regardless of the specific subtype of ASD that is utilized in any individual patient, all of the available devices seem to be efficacious, to a lesser or greater extent, to counteract the negative suction effect of siphoning [7]. As the inclusion criteria for the over-drainage syndrome are not universally accepted in the literature, results should be interpreted carefully. The determination of superiority of one device over another is difficult, mainly due to the paucity of in vivo comparison in the literature [7]. It is well known that this clinical entity is mainly encountered in older children who are suffering from hydrocephalus during infancy, and are harboring a shunt from that period of their life [38]. Nowadays, the insertion of or even the replacement of an ASD or the combination of that device with a programmable valve is considered to be the most widely accepted and scientifically sound treatment option. The insertion (at the time of initial insertion of a shunt or during follow-up) of an ASD has been associated with a significant decrease in the rate of development of SVS, as well as with a lesser incidence of ventricular catheter obstruction [39, 40]. A study has mentioned that its use is positively related with the acquisition of better intellectual outcomes [41]. To the best of our knowledge, an ideal ASD does not exist. This should be a device that could be suitable for patients harboring different underlying etiologies of hydrocephalus, and could adapt its function to parameters such as age, physical activity, and BMI. The most logical explanation is that no one device could be as physiologic as IJV is. Apart from that, the indication of insertion of an ASD and the specific subtype of ASD should be determined according to the individual requirements of any individual patient.
There is ongoing controversy regarding the most appropriate treatment algorithm for patients suffering from pediatric hydrocephalus [1, 10, 32]. A lot of literature reports exist that point out the increased failure rate which is intimately related with the insertion of a VPS estimates exist that it could reach the level of 40% during the first year after shunt insertion. Besides that, an increased tendency toward shunt failure seems to be present, with subsequent VPS revision rates lying between 40% and 60% [42, 43]. Apart from that, when we are treating patients suffering from infantile post-hemorrhagic hydrocephalus of prematurity, they are by definition implicated with the long-term risk of shunt-revision surgeries throughout their lifetimes [44]. According to published series, the selection of fixed opening pressure valvular mechanisms has been shown to be a safe and efficacious option for a great number of patients [45]. Nevertheless, this strategy could be inappropriate for an unknown number of patients, eventually leading to CSF over-drainage due to siphoning effect or, on the other hand, inadequate drainage of the ventricular system. Although both of these conditions are diametrically opposed to each other, they share in common the fact that they are potentially life-threating complications [45]. There is a wide spectrum of relevant side effects, which incorporate the development of slit-ventricle syndrome, loss of cerebral compliance [46, 47, 48], and occasionally, cranio-cephalic disproportion [37]. Undoubtedly, the selection of the optimum opening pressure of shunts in children remains an unresolved problem. Currently, there is lack of widely accepted guidelines regarding the optimum functional characteristics of ventriculoperitoneal shunts [49].
The designation and widespread utilization of programmable valvular mechanisms is based on our effort to eliminate the adverse effects that accompany the insertion of fixed, non-programmable, opening pressure valves [3]. The ultimate goal that is inherently related with their selection is to enhance our capability to regulate CSF flow and to adapt the rate of drainage to the individual patient requirements. The ultimate goal is to eliminate the possibility of development of proximal (central ventricular) shunt obstruction. These complications are better described under the terms of slit ventricle syndrome and CSF under- and over-drainage [3]. On a theoretical basis, the selection of a programmable valve in situ offers the opportunity to decrease the number of shunt revision procedures that are intimately related with a suboptimal regulation of the rate of CSF drainage. This advantage is related to the ability to non-invasively adjust the shunt valve opening pressure [50, 51]. Undoubtedly, this option is definitively an important aid in our effort to optimally manage issues related to CSF drainage. Nevertheless, we should mention that there is lack of randomized controlled trials, based on a large cohort of patients, aiming to compare the relative efficacy of the different valve systems. More precisely, these studies should consider that there exists a divergent group of underlying pathological conditions encountered in the pediatric population. Given the inherent heterogeneity that is associated with the pathologic substrate that accompanies the cases of pediatric hydrocephalus, the individual characteristics of every patient should be taken into consideration in order to make our ultimate choice regarding the most appropriate PSV. According to a recent publication [1], there are very specific indications that render the utilization of programmable opening pressure valves as mandatory. These include all patients for whom there is uncertainty regarding the selection of the optimum opening pressure, along with a specific subgroup of patients that are prone to the development of alterations in CSF dynamics over time. Under this general term are included all patients suffering from slit ventricle syndrome, as well as those at risk of CSF over-drainage. The aforementioned study supports that the use of PSV is of potential benefit for those patients that are prone to demonstrate shunt-related complications of failure, over drainage and cerebral non-compliance.
In concordance with the aforementioned observations, we attempt to briefly present the technical advancements that are intended to eliminate these adverse effects of the commercially available shunt systems. A first step was the innovation of the programmable shunt valves, which undoubtedly have been selected as the most indicated option for patients suffering from hydrocephalus. This is based on the concept that the incorporation of a valvular mechanism offering the ability to adjust the opening pressure, enables the treating physician to alter this pressure in a non-invasively manner. These adjustments should be performed in accordance with the ongoing alterations of the patient’s clinical course that are recorded after VPS insertion [52, 53]. However, the existing evidence regarding the effectiveness of PSV are misleading and difficult to interpret. More precisely, there are reports that were unable to compose a statistically significant differentiation when they compared the relevant shunt failure rates that were associated with the use of PSV, in comparison with traditional fixed opening pressure valve systems in children [17, 49]. On the other hand, several studies exist that argue against the opposite [6, 54]. To the best of our knowledge, there is no universal agreement regarding the definition of the optimum shunt characteristics that are dedicated to the pediatric population. Besides that, there is no uniform agreement regarding the existence of peculiar patient characteristics, that should be taken into consideration, in order to make our ultimate choice [17, 42, 55, 56, 57, 58, 59, 60, 61, 62]. In order to fully elucidate the challenges relevant to the management of children harboring shunts, we should strongly take into consideration the fact that this subgroup of patients is subject to physiological alterations that may interfere with CSF drainage rates during their lifetimes.
In order to explain in more details some concepts, such as ‘pressure differentials in various positions’, as well as the antisiphon phenomenon attributed to the IJV, we considered that adding Figs. 1,2,3,4,5,6,7,8 along with some diagrams, could illustrate better all these issues. The following features are designed in order to explain the mechanism of action of ASDs, as well as to explain the role of IJV, in conjunction with the antisiphon phenomenon.
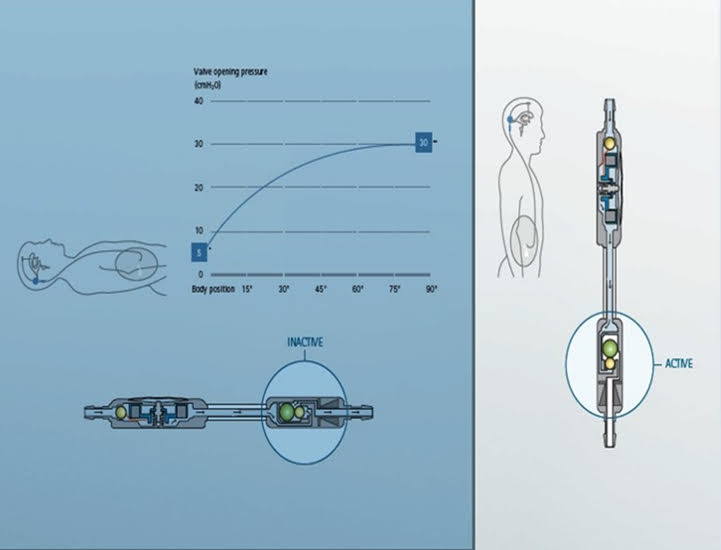 Fig. 1.
Fig. 1.When the patient lies in the supine position, only the
adjustable unit is active (at this figure, the selected opening pressure is 5
mmH
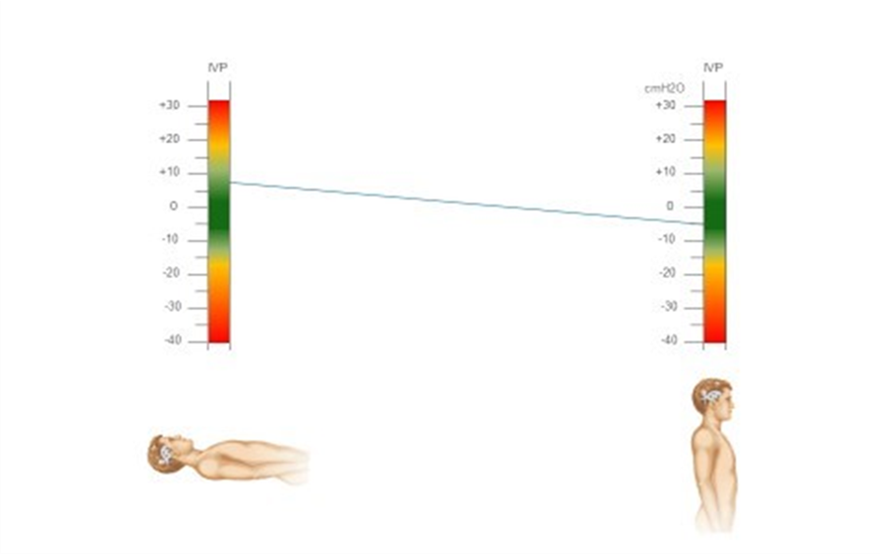 Fig. 2.
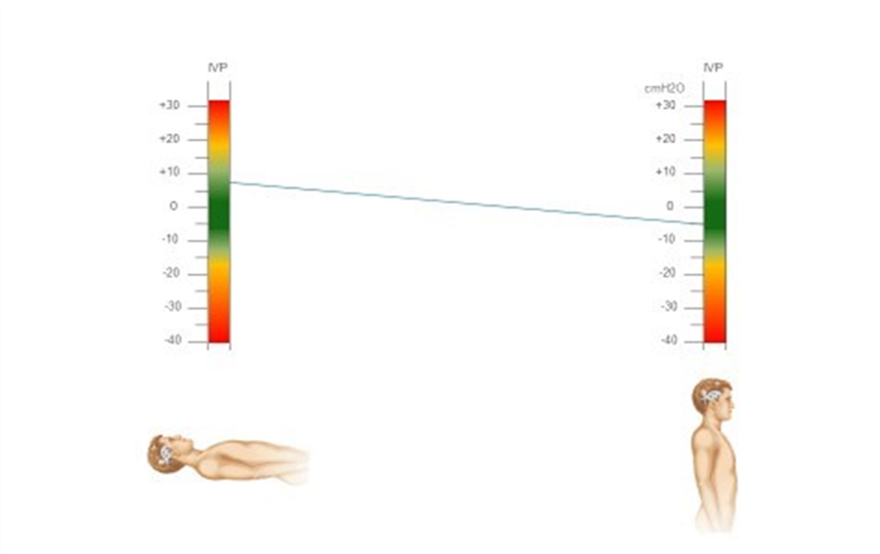
Fig. 2.ICP values in normal subjects, as measured at different body positions.
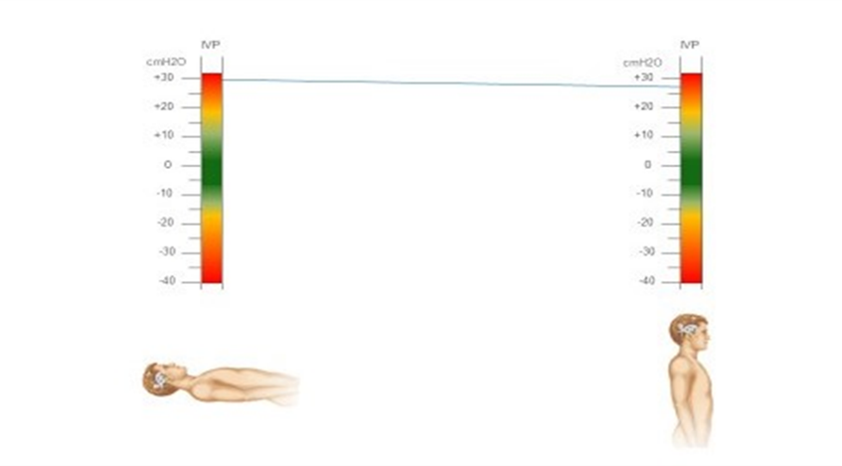 Fig. 3.
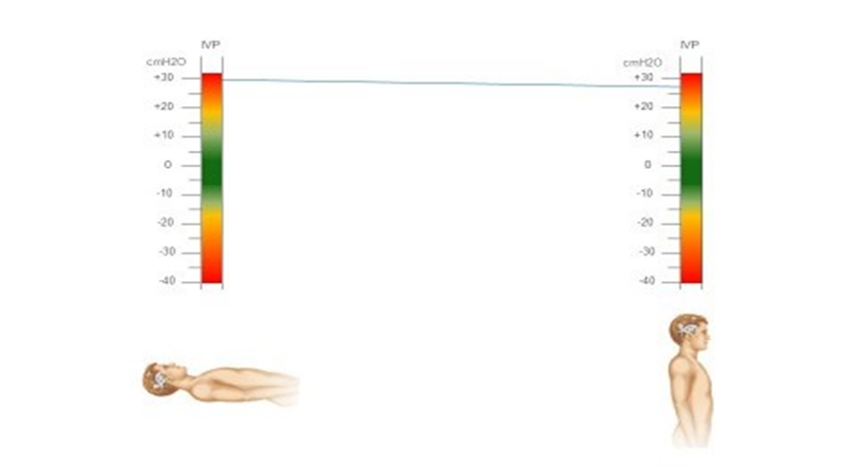
Fig. 3.ICP measurements in patients suffering from hydrocephalus (without shunt insertion).
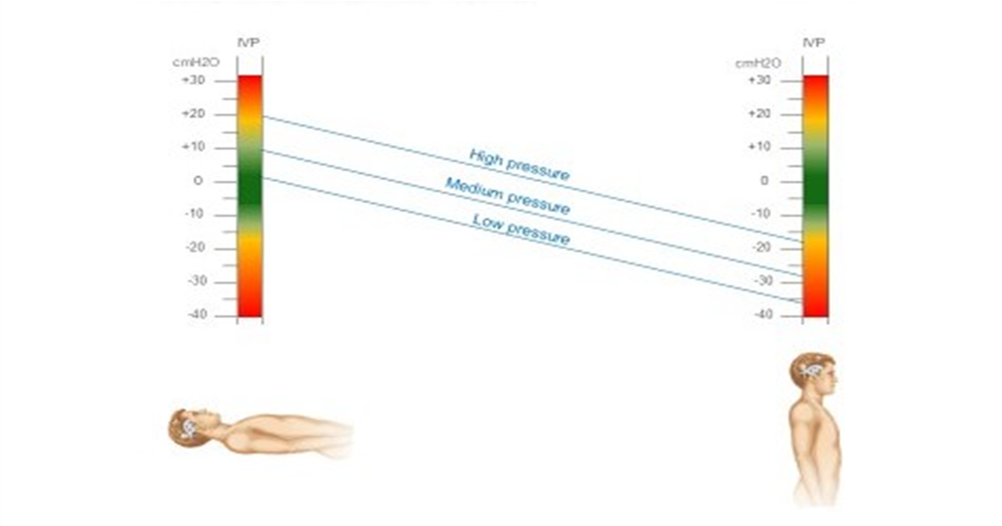 Fig. 4.
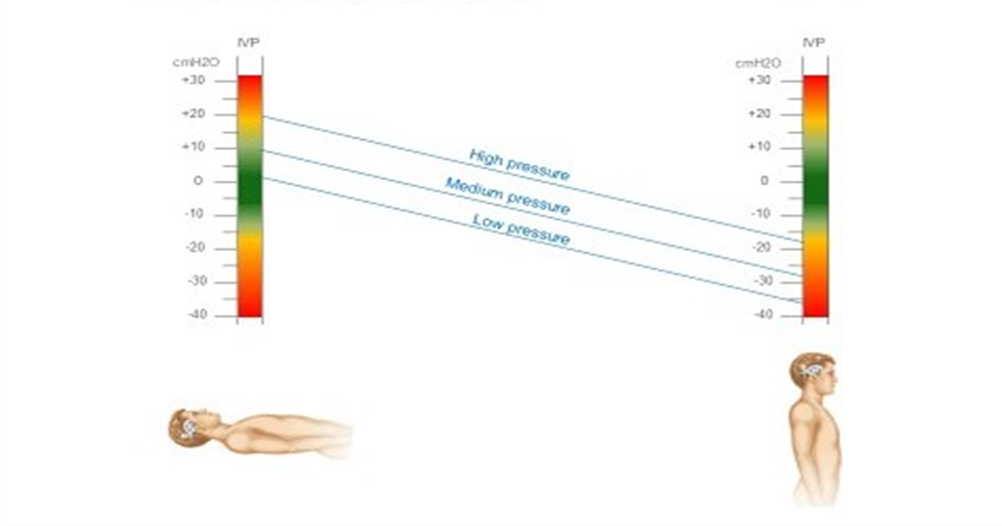
Fig. 4.Variation in ICP values in patients harboring a non-adjustable valvular mechanism for hydrocephalus (low pressure, medium pressure, high pressure) without an ASD, when moving from supine to upright posture.
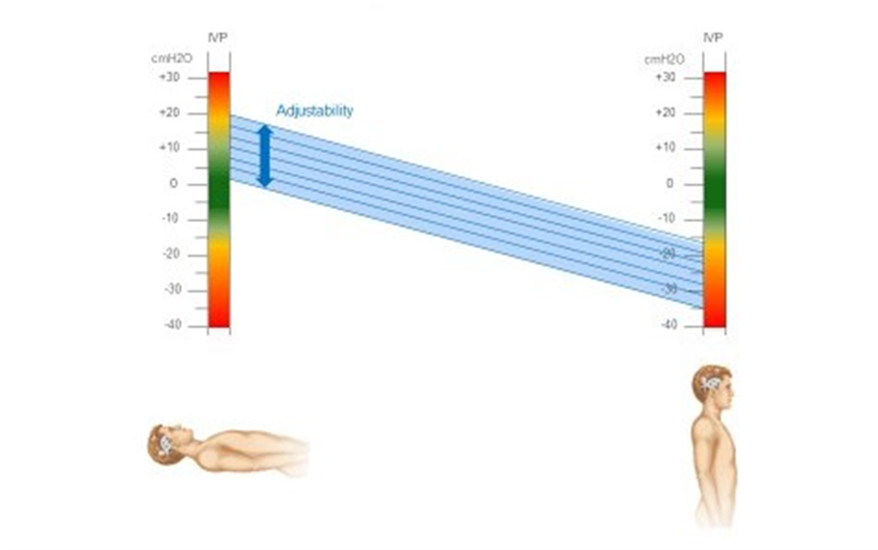 Fig. 5.
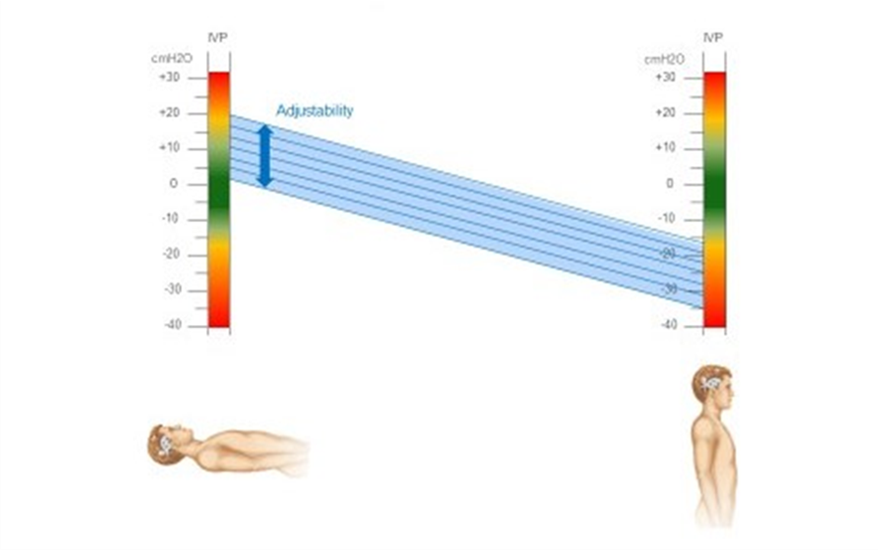
Fig. 5.Variation in ICP values in patients harboring an adjustable valvular mechanism for hydrocephalus without an ASD, when moving from supine to upright posture.
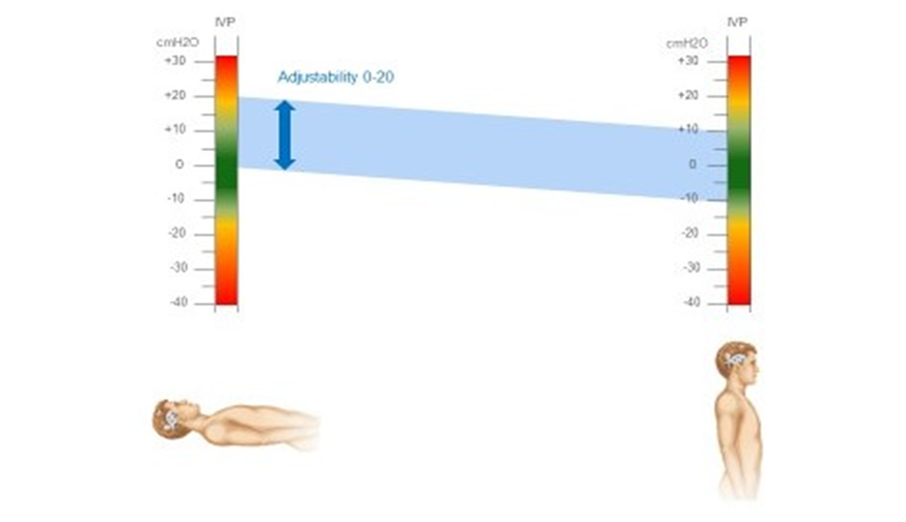 Fig. 6.
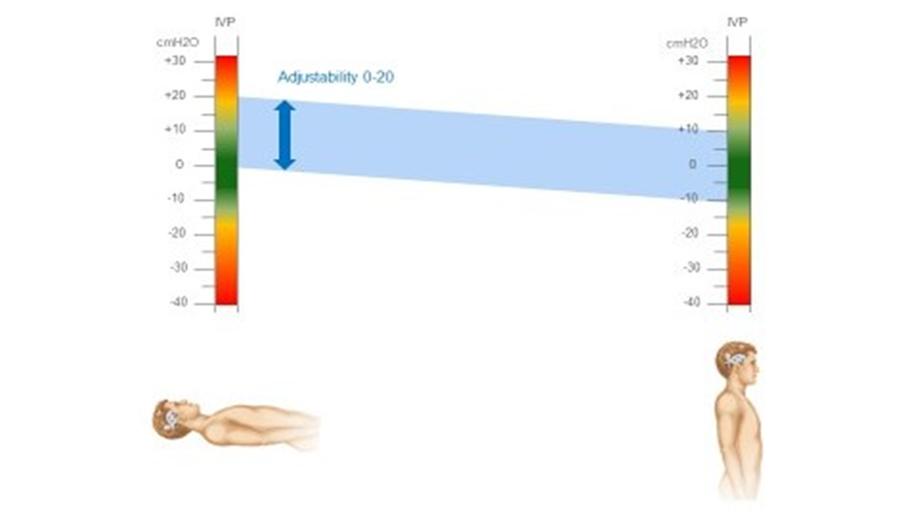
Fig. 6.Variation in ICP values in patients harboring an adjustable
valvular mechanism with a non-adjustable ASD, when moving from supine to upright
posture. In this paradigm, we present the case of an adjustable valvular
mechanism between 0–20 cmH
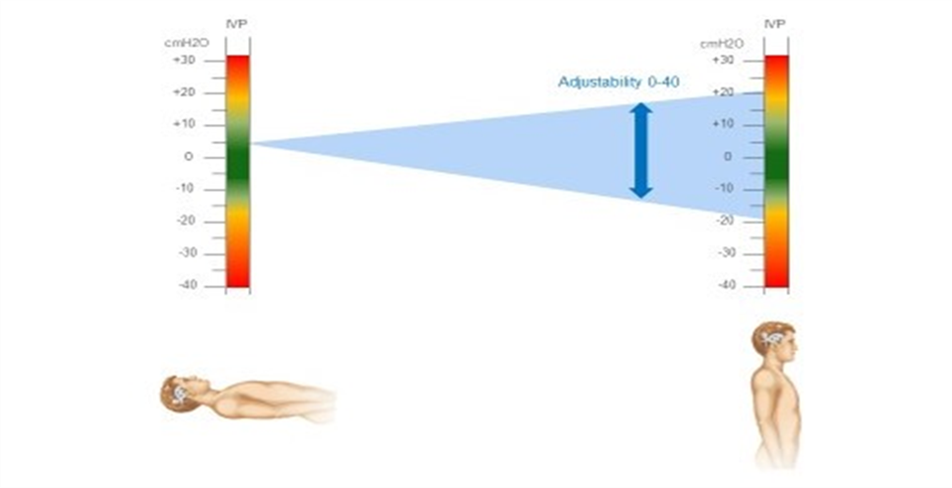 Fig. 7.
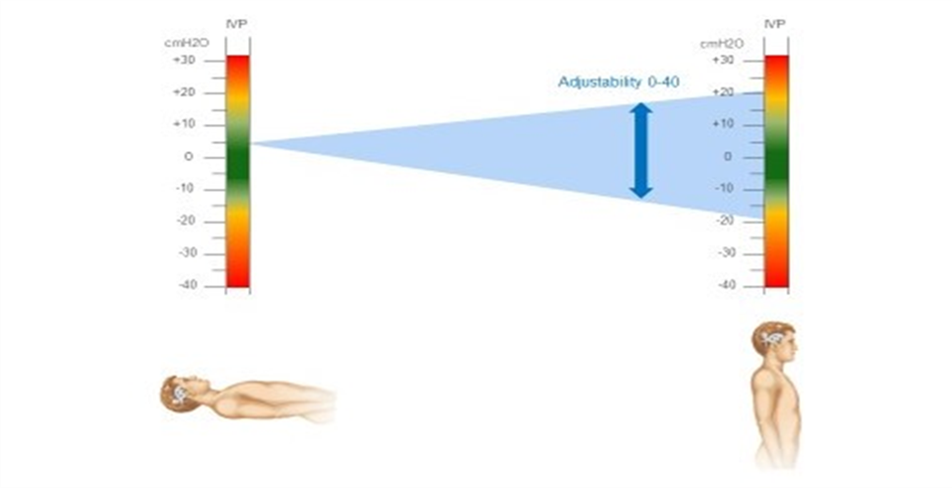
Fig. 7.Variation in ICP values in patients harboring a non-adjustable
valvular mechanism and an adjustable ASD for hydrocephalus, when moving from
supine to upright posture. In this paradigm, we present the case of an adjustable
ASD between 0–40 cmH
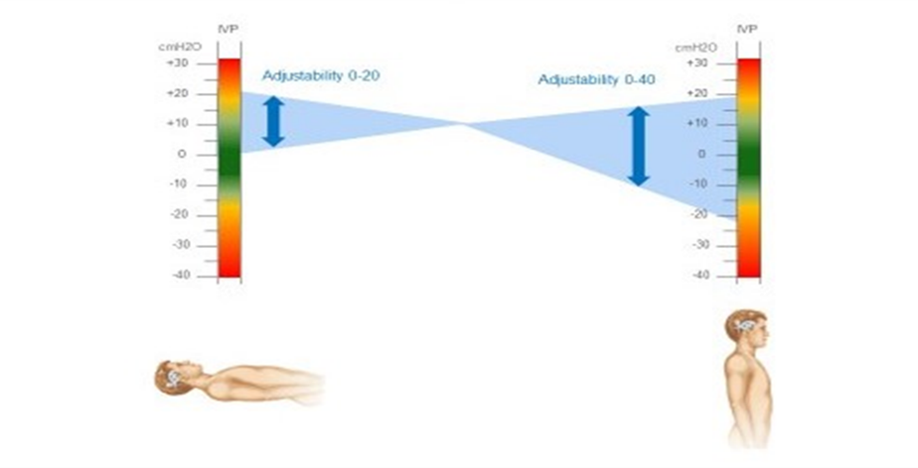 Fig. 8.
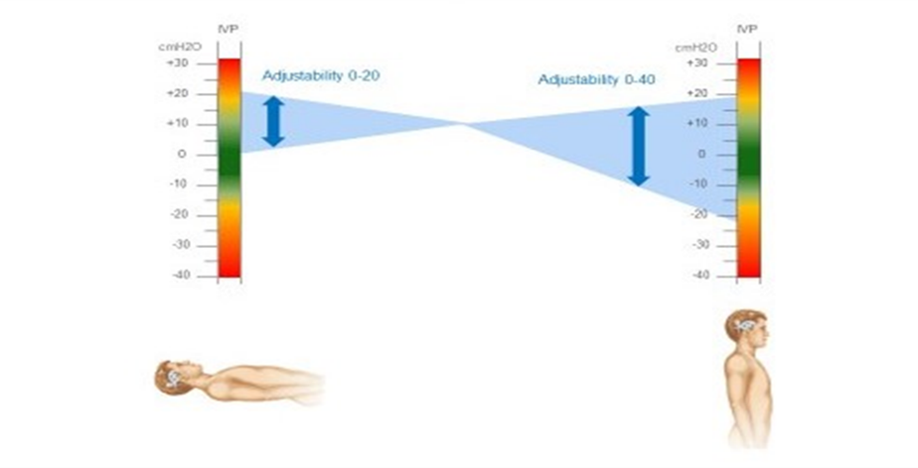
Fig. 8.Variation in ICP values in patients harboring an adjustable
valvular mechanism and an adjustable ASD for hydrocephalus, when moving from
supine to upright posture. In this paradigm, we present the case of an adjustable
ASD between 0–40 cmH
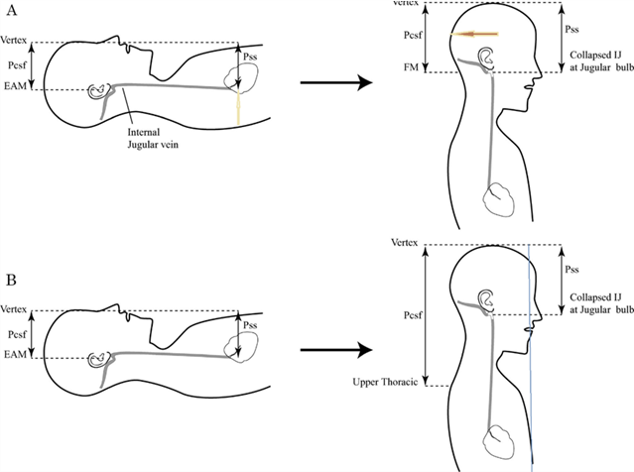
Patient with CSF diversion in supine position (Fig. 9B). Under such
circumstances, pressures are similar to the normal counterpart yet during upright
positioning. Moreover, the CSF zero point of the craniospinal axis has shifted
caudally to the upper thoracic region. Because of that, CSF pressure (Pcsf) will
be less (more negative since further away from the zero point) relative to
sagittal sinus pressure (Pss) (Pcsf
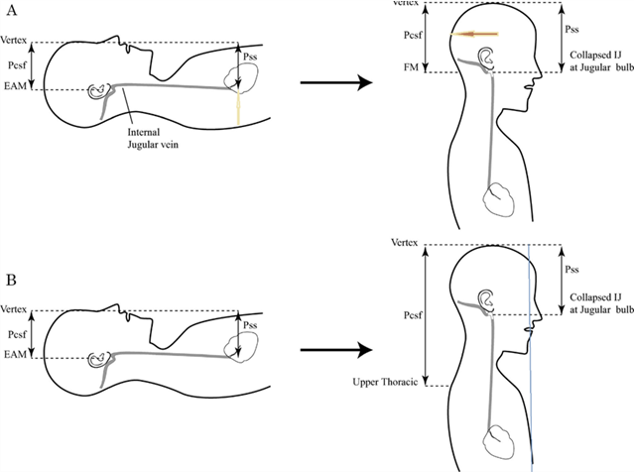 Fig. 9.
Fig. 9.Schematic diagram presenting a normal individual in supine position. (A) Where the patient adopts an upright posture. (B) Patient in the upright position. In this condition, CSF pressure (Pcsf), which is measured from the EAM to the vertex, as well as sagittal sinus pressure (Pss), that is measured from the right atrium, are closely approximated. When the patient adopts an upright posture, Pcsf (as measured from the foramen magnum) and Pss (measured from the collapsed internal jugular vein at the jugular bulb to the vertex), are in close proximity. EAM, external auditory meatus; FM, foramen magnum; IJ, internal jugular.
The vertical arrow in (Fig. 9A) represents the approximate location of the right atrium, whereas the horizontal (blue) arrow in (Fig. 9A) and the horizontal (yellow-red) arrow in (Fig. 9A) (where the patient adopts an upright posture) represent the most common position that the valvular mechanism and, adjacent to it, the ASD, are inserted. The vertical line that is drawn in figure (Fig. 9B) (patient in the upright position), represents an approximate estimation of the distance between the vertex of the skull and the abdominal cavity which plays a major role in the siphoning effect in patients harboring a ventriculo-peritoneal shunt.
We should mention that, while collapse of ventricles around an over-draining shunt could cause shunt failure, one argument used against them is that the antisiphon mechanism introduces an additional point of restricted and irregular flow where the shunt mechanism can become obstructed by protein/debris. Although the majority of the published manuscripts mention that there is superiority, regarding the clinical outcome, in the group of patients that are harboring an ASD, this issue remains unresolved. Well-organized, prospective studies are missing, comparing the long-term shunt failure rates of the ASD devices, especially in patients who are prone to occlusion at any point of the shunt system (i.e., patients with post-hemorrhagic hydrocephalus who are characterized by increased protein concentration in their CSF).
The entities of shunt over-drainage and slit ventricle syndrome were recognized soon after the initial treatment of hydrocephalus via the aid of ventriculoperitoneal shunts. Although a lot of experts have made excellent contribution in the field of pathophysiology and clinical determination of these syndromes, several aspects of them remain undetectable. This is mainly due to the fact that there is a lack of unified definition criteria regarding these entities, as well as absence of a commonly accepted strategy regarding their treatment and their avoidance. As several pathophysiological mechanisms are implicated, each one to a lesser or greater extent, a further work-up is required in order to specify the precise role of each one of them, and their interrelation. Indeed, new technological insights in the field of valve technology largely reflect our temptation to enhance our available options, regarding the control of CSF drainage, as well as the avoidance of siphoning effect. Our ultimate target would be a simulation of the physiological CSF drainage characteristics. A critical point refers to the capacity of our body to maintain a physiologic, and stable, ICP value, adapted to, and irrespective of, different body positions. It seems that gravitational valves, which incorporate an anti-siphon device, represent a construct that is capable of simulating the sequence of events that accompany the counteraction of hydrodynamic effects that refer to the assumption of the upright position in normal individuals. Apart from that, the use of programmable valves seems to be beneficial for these patients, as they could be able to avoid the development of potential shunt-related complications, such as central ventricular catheter obstruction, over-drainage and loss of cerebral compliance. As far as safety and efficacy of gravitational valves have been established, long-term prospective follow-up studies are warranted, in order to enhance even further the validity of our current considerations.
We would like to mention that a bibliographic search was performed from our side, using Thomson Reuters web of Science and Pubmed databases, in order to identify the most noteworthy papers related to our study.
CSF, cerebrospinal fluid; ICP, intracranial pressure; ASD, anti-siphon device; PP, perfusion pressure; DP, differential pressure; SVS, slit ventricle syndrome; REM, rapid-eye movement; IJV, internal jugular vein; BMI, Body-mass index; VPS, ventriculo-peritoneal shunt; PSV, programmable shunt valve.
Conceptualization—DP, GS, EB, SK. Methodology—DP. Software—DP, MG. Validation—DP, GS, EB, SK, MG. Formal Analysis—DP. Investigation—DP. Resources—DP, MG. Data Curation—DP. Writing - Original Draft Preparation—DP, GS, EB, SK. Writing - Review & Editing—DP, GS, EB, SK, MG. Visualization—MG. Supervision—DP.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.