



1 Department of Neurology, The Second Hospital of Dalian Medical University, 116027 Dalian, Liaoning, China
2 Department of Cardiology, The Second Hospital of Dalian Medical University, 116027 Dalian, Liaoning, China
3 Department of Neurosurgery, Yantian District People's Hospital, 518000 Shenzhen, Guangdong, China
Academic Editor: Mauro Silvestrini
Abstract
Background: In recent years, an overlapping syndrome, MNOS, of MOG encephalomyelitis and NMDARE has been clinically identified. In these diseases, both MOG-Ab and NMDAR-Ab are positive. Previous studies were almost case reports and incomprehensive which focused on this kind of overlapping syndrome in adults. Methods: We reported a rare case of MNOS. In addition, we reviewed the clinical characteristics, diagnosis, and treatment of MNOS in adults by consulting relevant literature. Results: The patient initially presented with CNS demyelination symptoms followed by recurrent encephalitis, concomitant anti-MOG, and NMDAR antibodies. His symptoms improved significantly after initiating hormonal therapy. We searched previous MNOS case reports and 17 adult MNOS cases were retrieved. The previous history of all patients was unremarkable. Most of these patients (72.2%, 13/18) first developed NMDR encephalitis-related symptoms, such as cognitive behavior abnormalities, cognitive decline, and epilepsy. Some patients (16.7%, 3/18) first developed MOG-related demyelinating symptoms, such as visual deterioration, walking instability, and dizziness. The most common site of new brain lesions was the supratentorial region. In the acute phase, MNOS patients were sensitive to hormone therapy. During the follow-up, 72.2% (13/18) of the patients relapsed, with a median interval of 12.25 months. Immunotherapy was still effective after recurrence, and no deaths were reported. Conclusions: (1) The clinical manifestations of MNOS are atypical, sometimes like MOG encephalomyelitis, sometimes like NMDARE, sometimes both of the characteristic clinical manifestations are present. (2) Immunotherapy is the primary treatment of patients with MNOS. (3) MNOS are prone to recurrence, and serum MOG and tumor markers should be monitored.
Keywords
- Myelin oligodendrocyte glycoprotein (MOG)
- N-methyl-D-aspartate receptor (NMDAR)
- Anti-N-methyl-D-aspartate receptor
- Autoimmune encephalitis (AIE)
In 2007, O’Connor et al. [1] described anti-Myelin Oligodendrocyte Glycoprotein (anti-MOG) antibodies in children with Acute Disseminated Encephalomyelitis (ADEM) by tetramer radioimmunoassay for the first time. Research results in recent years indicate that MOG-IgG-associated diseases may be an independent disease, different from Multiple Sclerosis (MS), ADEM, and AQP4-IgG-positive Neuromyelitis Optica Spectrum Disorder (NMOSD) [2]. The clinical features of MOG-IgG-associated diseases in adults were mainly optic nerve damage, spinal cord damage and lenient reoccurrence [2]. MOG encephalomyelitis rarely presents the following symptoms: mental behavior abnormalities, epilepsy, and cognitive impairment, which manifest in N-Methyl-D-Aspartate Receptor (NMDAR) encephalitis [3]. The immune coexistence of MOG and NMDAR antibodies is not common. In recent years, several cases have been reported. And the overlapping syndrome of MOG-Ab disease and anti-NMDAR encephalitis (NMDARE) was abbreviated as MNOS [4]. We report a patient who initially presented with Central Nervous System (CNS) demyelination symptoms followed by recurrent encephalitis, concomitant anti-MOG, and NMDAR antibodies. Furthermore, we analyzed the clinical features of MNOS in adults.
A 36-year-old male developed a headache in late December 2018. Seven days later,
he experienced left facial numbness and slurred speech (Table 1). Neurological
examination revealed slurred speech, stiff neck, and decreased left facial
perception. Magnetic Resonance Imaging (MRI) revealed a fluid attenuation
inversion recovery (FLAIR) high-intensity lesion involving the left pontine and
cerebral peduncle, and the boundaries were unclear with a range of about 20
| 2019-1 | 2019-2 | 2019-4 | 2020-2 | |
| Clinical manifestation | Headache, left facial numbness and slurred speech | normal | normal | Behavioral change and psychosis |
| Inducement | Caught a cold 1 week ago | na | na | Fracture of left upper limb |
| Neurological examination | Slurred speech, | normal | normal | Finger agnosia, |
| stiff-neck, | acalculia, | |||
| left facial perception | left-right disorientation | |||
| CSF | 205 mm H |
na | na | normal |
| Leucocytes: 170/µL, 34% mononuclear | ||||
| Pandy’s test ( | ||||
| Serum MOG-Ab | pos | pos | pos | pos |
| CSF MOG-Ab | pos | na | na | pos |
| CSF and serum | neg | na | na | neg |
| MBP-Ab, AQP4-Ab | ||||
| Serum NMDAR-Ab | pos 1: 10 | na | na | pos 1: 10 |
| CSF NMDAR-Ab | neg | na | na | pos 1: 3.2 |
| Autoimmune encephalitis associated antibodies (AMPAR1, AMPAR2, CASPR2, GABAR, LGI1) | neg | na | na | neg |
| Paraneoplastic nerve syndrome associated antibodies (Anti-Hu, Anti-Yo, Anti-Ri, Anti-CV2, Anti-Amphiphysin, Anti-ANNA-3, Anti-Tr, Anti-PCA-2, Anti-GAD, Anti-Ma2) | neg | na | na | neg |
| Therapy | Dexamethasone (10 mg/day, for 5 days), later prednisone (initial 60 mg/day and decreased 5 mg every 2 weeks) | Prednisone (20 mg/day) | Stop steroid without permission for 1 month | HDMT (1000 mg/day, for 5 days) and MMF (500 mg/day) |
| MOG, myelin oligodendrocyte glycoprotein; MMF, Mycophenolate Mofetil; NMDAR,
N-methyl-D-aspartate receptor; AQP4, aquaporin 4; MBP, myelin basic protein;
AMPAR, anti-alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor;
CASPR2, contactin-associated protein-like 2; GABAR, anti- | ||||
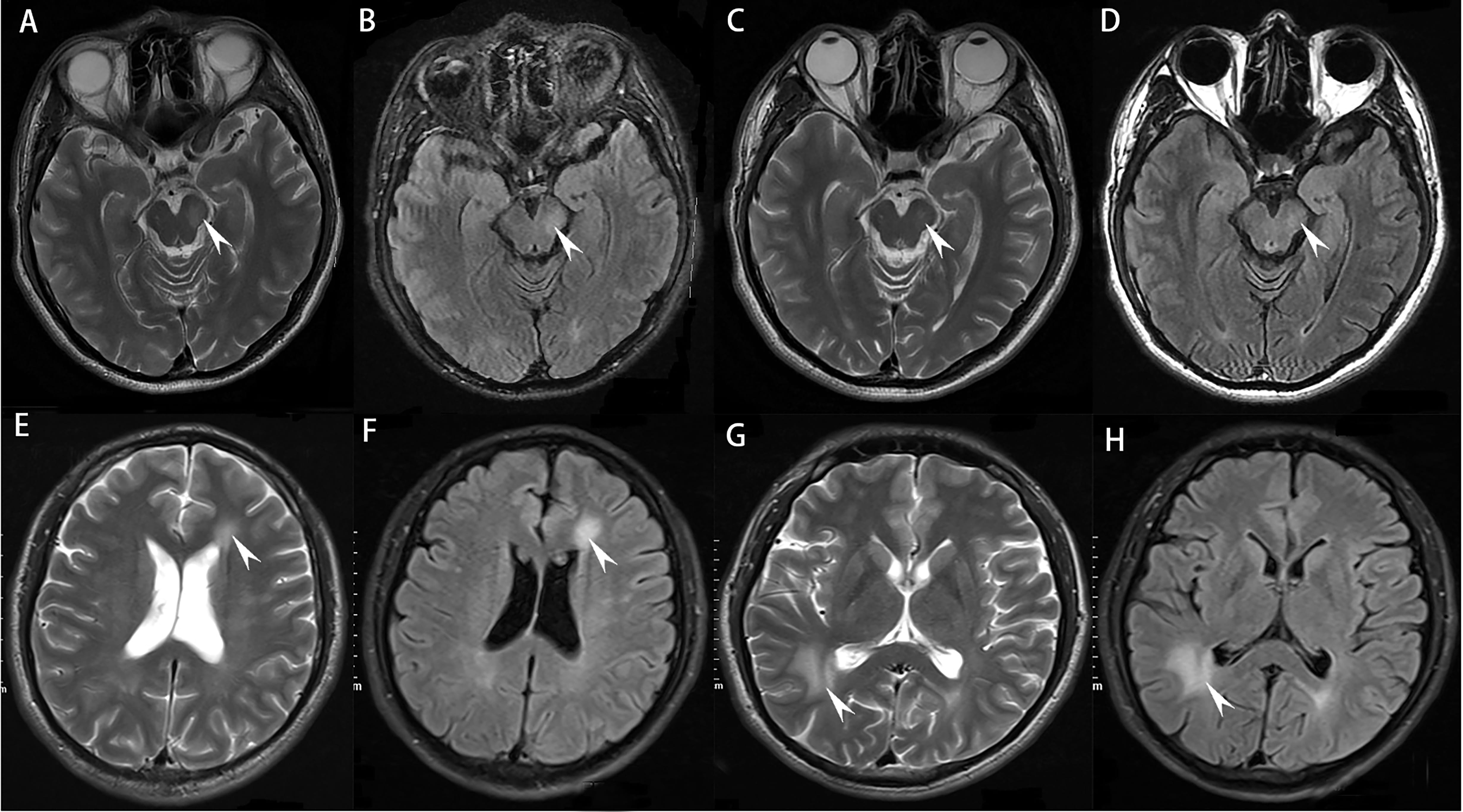 Fig. 1.
Fig. 1. MRI presentations during different episodes. (A,B) T2-weighted images (T2WI) and fluid-attenuated inversion recovery (Flair)
images showed the left pontine and cerebral feet, and the boundaries are unclear
with a range of about 20
In late February 2020, the patient fell and had a fracture of the left humerus. A week later, he developed behavioral changes and psychosis. Dominant symptoms were mental excitement, speaking too much, and forgetting his general knowledge of objects. Neurological examination revealed finger agnosia, acalculia and left-right disorientation. MRI demonstrated deep white matter demyelination lesions in the left lateral ventricle frontal and right lateral ventricle occipital angles (Fig. 1E–H). Cervical and thoracic MRI showed no abnormality. CSF biochemistry was normal. The serum MOG antibody and CSF NMDAR antibody, which were re-examined in the same laboratory as previous tests (Table 1), were both positive. Other antibodies related to autoimmune encephalitis and paraneoplastic syndrome in serum and CSF were negative. Blood tests for other systematic autoimmune diseases were normal. Furthermore, serum tumor markers were negative and the abdominal CT scan revealed no underlying neoplasm (not shown). This time positive NMDAR antibodies in the CSF were found. Therefore, High Dose Methylprednisolone pulse Therapy (HDMT) and oral mycophenolate mofetil therapy were added. His symptoms improved significantly after therapy. Throughout his one year follow-up, no recurrence was observed. Assays for serum and CSF MOG-Ab, MBP-Ab, NMDAR-Ab, LGI1-Ab, CASPR2-Ab, AMPAR1/R2-Ab, and GABAB R-Ab were carried out at Beijing Hightrust diagnostic Medical Diagnostics Laboratory (Beijing Hightrust Diagnostics, Co., Ltd) by cell-based Indirect Immune-Fluorescence Test (IIFT) employing BIOCHIPs. An AQP4-Ab was carried out by Enzyme-Linked Immunosorbent Assay (ELISA). Written informed consent for publication was obtained from the patient. The Medical Ethics Committee approved the study of the Second Hospital of Dalian Medical University.
We searched PubMed (Medline) through May 11, 2021, for articles published in any language with the search string (“Receptors, N-Methyl-D-Aspartate” [MeSH Terms] OR “N-Methyl-D-Aspartate” OR “NMDA”) AND (“Myelin Oligodendrocyte Glycoprotein” [MeSH Terms] OR “MOG”). Furthermore, we also searched the references for related published articles. We examined studies that have presented the cases of overlapping MOG-Ab disease and NMDARE. Our review identified 87 patients with overlapping MOG Ab-associated disorders and anti-NMDAR encephalitis. We excluded 51 pediatric cases because MNOS patients can behave very differently by age spectrum. A further 9 patients were excluded due to insufficient information. Finally, 18 patients (including our case) were included in the review (Fig. 2). All patients fulfilled the diagnostic criteria for definite anti-NMDAR encephalitis and MOG-IgG-associated diseases [2, 9].
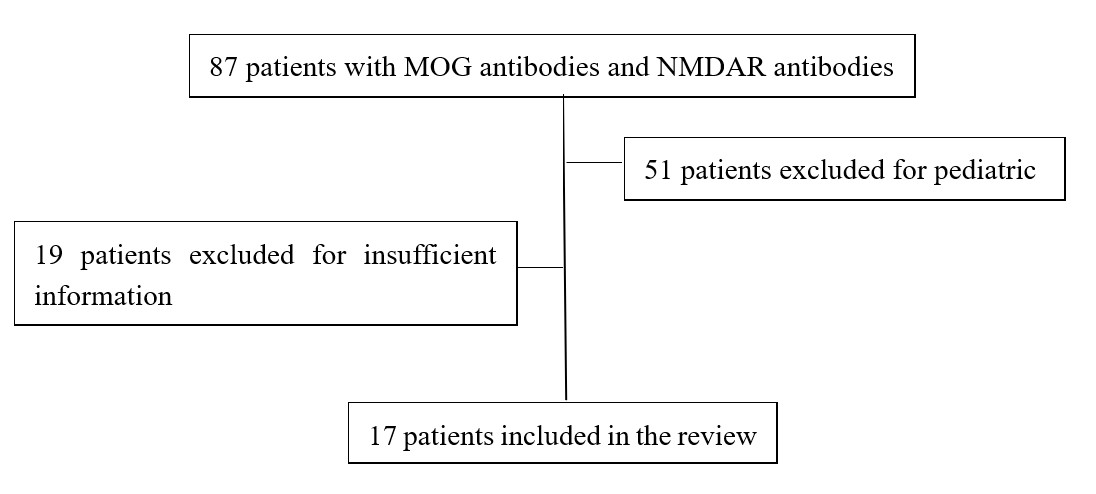 Fig. 2.
Fig. 2.Review flow-chart.
Of these patients, 7 were female and 11 were male (Table 2 Ref. [4, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20] and Table 3). The median age at presentation was 30.5 years for adults
(range, 18–54). The previous history of all patients was unremarkable, and none
had tumors. Most of these patients (72.2%, 13/18) first developed NMDR
encephalitis-related symptoms, such as cognitive behavior abnormalities,
cognitive decline, and epilepsy. Some patients (16.7%, 3/18) first developed
MOG-related demyelinating symptoms, such as visual deterioration, walking
instability, and dizziness. During the course of the disease, 44.4% of patients
had blurred vision, 61.1% of the patients showed abnormal mental behavior, such
as paroxysmal irritability, moodiness, 38.9% of the patients had seizures,
27.8% of the patients showed a cognitive decline, manifested as deterioration of
the memory, 22.2% of the patients had speech disorders, manifested as silence
aphasia, 27.8% of the patients showed movement disorders, including facial,
tongue, and limb movement disorders, 27.8% of the patients showed paresthesia,
as numbness, and 38.9% of the patients showed dizziness and walking instability
(Tables 2,3). Imaging found that 16/18 (88.9%) of brain MRI showed new lesions
during the acute attack. The most common site of new brain lesions was the
supratentorial region. In the acute phase, MNOS patients were sensitive to
hormone therapy and most of the patients improved after receiving HDMT. Some
patients with severe conditions were treated with Intravenous Immunoglobulin
(IVIG) (0.4 g/kg
| Source | Age at onset, year | Sex | MOG-vs NMDARE-like episodes | MRI findings (Brain/Spine) | Immunotherapy | Disease course | Interval months |
| Titulaer et al. (2014) [12] | |||||||
| Case 1 | 18 | F | NMDARE-like episodes | Normal | Steroid, IVIG, PE, CTX, RTX | MONO | 0.8 |
| Case 2 | 45 | F | NMDARE-like episodes | Normal | Steroid | MONO | 1.8 |
| Kaneko et al. (2014) [14] | 28 | F | NMDARE-like episodes | In the cerebral deep gray matter and white matter. | HDMP, PRED | RR | - |
| Zhou et al. (2017) [11] | 31 | M | NMDARE-like episodes; MOG-like episodes; both | Right side of the cerebral cortex; left medulla oblongata; brainstem | DXMS; IVIG, AZA; HDMP, later MMF | RR | 6; 2 |
| Fan et al. (2018) [4] | |||||||
| Case 1 | 23 | M | NMDARE-like episodes; both; NMDARE-like episodes | Right cerebral peduncle; left posterior cerebral cortex; extensive cortical lesion | HDMP, orally corticosteroids treatment; IVIG, MMF | RR | 24; 20 |
| Case 2 | 25 | M | NMDARE-like episodes | The cortex of right hemisphere. | HDMP, orally corticosteroids treatment | MONO | - |
| Zhou et al. (2018) [15] | 54 | M | NMDARE-like episodes | Dorsal brainstem, the brain parenchyma surrounding the third and fourth ventricles | HDMP, IVIG, PRED, RTX | MONO | - |
| Nagata et al. (2018) [16] | 20 | F | Both | Frontal cortex, cingulate gyRus | HDMP, IVIG, PE | MONO | - |
| Rojc et al. (2019) [17] | 47 | M | MOG-like episodes; NMDARE-like episodes | Left optic nerve; right front parietal white matter | HDMP | RR | 18 (1, 1, 1, 2, 4, 8 year) |
| Ren et al. (2019) [10] | 31.5, 27–43 | F(2); M(2) | 6.5 (0.5–12 months) | ||||
| Case 1 | NMDARE-like episodes; MOG-like episodes | Abnormal swelling of the left hippocampus; both right and hippocampal region | HDMP, orally corticosteroids treatment | RR | |||
| Case 2 | NMDARE-like episodes; MOG-like episodes | Callosum and around the ventricle; centrum semiovale; the left optical nerve | HDMP, IVIG, natalizumab infusions (600 mg), MMF; later MMF (500 mg/day) | RR | |||
| Case 3 | MOG-like episodes | Extensive intracranial lesions; right cerebellar hemisphere and posterior horn of lateral ventricle | HDMP, orally corticosteroids treatment, MMF; AZA | RR | |||
| Case 4 | NMDARE-like episodes; MOG-like episodes | Midbrain, C7-T1/T7-T12 spinal cord plane; right pons and aqueduct of sylvius | HDMP, orally corticosteroids treatment, AZA; later AZA (150 mg/day) | RR | |||
| Aoe et al. (2019) [18] | 36 | F | NMDARE-like episodes | Frontal lobes; basal ganglia, temporal lobe, cerebellar hemisphere. | HDMP, IVIG | RR | 420 |
| Perez et al. (2020) [13] | 29 | M | Both; MOG-like episodes | Temporal lobe; thalamus, medulla, optic nerve | Oral corticosteroids; PE, later RTX | RR | 1 |
| Cherian et al. (2020) [19] | 30 | M | NMDARE-like episodes | Cingulate gyri, limbic lobe, bilateral pulvinar, brainstem, cerebellar | HDMP, later MMF | MONO | - |
| Fujimori et al. (2020) [20] | 39 | M | NMDARE-like episodes | Frontal cortex and cingulate gyrus | IVIG, later PRED | RR | 39; 50 |
| AZA, Azathioprine; CTX, cyclophosphamide; DXMS, Dexamethasone; F, female; IVIg, intravenous immunoglobulin; HDMT, high dose methylprednisolone pulse therapy; M, male; MMF, mycophenolate mofetil; MOG, myelin oligodendrocyte glycoprotein; MONO, Monophasic; mo., months; MRI, magnetic resonance imaging; NMDARE, anti–N-methyl-D-aspartate receptor encephalitis; PE, Plasma exchange; PRED, Prednisone; RR, Relapsing remitting; RTX, rituximab. | |||||||
| Clinical characteristics | Number of cases | Percentage/% | |
| Gender | |||
| Male | 11 | 61.1 | |
| Female | 7 | 38.9 | |
| Presenting manifestations | |||
| Seizures | 7 | 38.9 | |
| Abnormal mental behavior | 11 | 61.1 | |
| Cognitive decline | 5 | 27.8 | |
| Speech disorders | 4 | 22.2 | |
| Dyskinesia | 5 | 27.8 | |
| ON | 8 | 44.4 | |
| ABS | 7 | 38.9 | |
| Numbness | 5 | 27.8 | |
| Disturbance of consciousness | 1 | 5.6 | |
| MRI findings | |||
| Optical nerve | 3 | 16.7 | |
| Cortical | 10 | 55.6 | |
| White matter | 8 | 44.4 | |
| Deep gray matter | 3 | 16.7 | |
| Brainstem | 8 | 44.4 | |
| Cerebellum | 5 | 27.8 | |
| Spinal cord | 1 | 5.6 | |
| Normal | 2 | 11.1 | |
| Immunotherapy | |||
| Steroid | 18 | 100 | |
| IVIG | 8 | 44.4 | |
| PE | 5 | 27.8 | |
| MMF | 6 | 33.3 | |
| RTX | 3 | 16.7 | |
| AZA | 3 | 16.7 | |
| CTX | 1 | 5.6 | |
| Natalizumab | 1 | 5.6 | |
| Disease course | |||
| RR | 13 | 72.2 | |
| MONO | 5 | 27.8 | |
| ABS, acute brainstem syndrome; AZA, Azathioprine; CTX, cyclophosphamide; IVIg, intravenous immunoglobulin; MMF, mycophenolate mofetil; MOG, myelin oligodendrocyte glycoprotein; MONO, Monophasic; MRI, magnetic resonance imaging; PE, Plasma exchange; RR, Relapsing remitting; RTX, rituximab. | |||
Myelin oligodendrocyte glycoprotein (MOG) is a glycoprotein, which is expressed explicitly on oligodendrocytes’ surface in the CNS at the myelin’s outermost layer sheath. MOG participates in myelin adhesion and maintains the myelin sheath of oligodendrocyte microtubules [21]. MOG-Ab can be divided into non-pathogenic antibodies (linear glycoproteins) and pathogenic antibodies (folded glycoproteins). Currently, cell-based assay (CBA) is the most commonly used method for detecting pathogenic MOG-IgG [22]. MOG encephalomyelitis has clinical manifestations of vision loss, walking instability, dizziness, etc. [2]. In 2005, Vitaliani et al. [23] first reported anti-NMDAR encephalitis, and later Dalmau et al. [24] subsequently confirmed its pathogenic target antigen NMDAR. Anti-NMDA receptor encephalitis (NMDARE) is a kind of autoimmune encephalitis caused by neuron surface antibodies against the NMDA receptor GluN1 subunit. Patients often show abnormal mental behavior, seizures, involuntary movement, consciousness alterations, and autonomic nervous system dysfunction [25].
In recent years, an overlapping syndrome, MNOS, of MOG encephalomyelitis and NMDARE has been clinically identified. In these diseases, both MOG-Ab and NMDAR-Ab are positive. The clinical manifestations of MNOS are atypical, sometimes like MOG encephalomyelitis, sometimes like NMDARE; sometimes both of the characteristic clinical manifestations are present. However, the clinical manifestations of the overlapping syndrome were milder than those of NMDARE alone [12]. Therefore, we need to be vigilant when patients with NMDAR encephalitis develop optic neuritis, myelitis, or other demyelinating diseases inconsistent with autoimmune encephalitis and should be evaluated for serological antibodies associated with demyelinating diseases. Similarly, coexisting immune-mediated encephalitis should be suspected when patients with MOG encephalomyelitis or other demyelinating diseases have atypical symptoms, such as psychosis or seizures.
At present, the mechanism of the simultaneous appearance of these two antibodies is not exact. In our case, the patient was exhausted, and he stayed up late with heavy work pressure before the disease. Furthermore, the patient’s first symptom was headache. The pathological mechanism may be as follows. Firstly, the patient may be invaded by the virus (Considering it is not a common virus, no obvious abnormality was observed in the virus spectrum). The Blood-Brain Barrier (BBB) was damaged, and the MOG-Ags of the CNS were exposed and the corresponding antibodies were produced, which led to the aggravation of the BBB damage and the exposure of NMDAR-Ags and the generation of NMDAR-Abs. Secondly, it is worth noting that oligodendrocytes can express NMDA receptors [12], so oligodendrocyte damage associated with MOG antibody disease may lead to secondary damage to NMDA receptors [13]. These hypothesis could explain why our patients were positive for NMDAR-Abs even without tumors, and perhaps why serum NMDAR-Abs were positive before CSF was positive. Castillo-Gómez et al. [26] showed that all circulating NMDAR antibodies could cause disease in the presence of increased BBB permeability. Therefore, when the serum NMDAR antibody is positive but CSF is negative, we need to be alert and measure CSF and serum NMDAR antibody again.
Immunotherapy is the primary treatment of patients with MNOS. The first-line treatment mainly includes steroids, IVIG, and PE. Most MNOS patients responded well to first-line therapy in the acute phase [4]. Previous studies have shown that most patients received High-Dose Methylprednisolone pulse Therapy (HDMT) as a steroid regimen. However, in this case, the patient was treated with dexamethasone 10 mg, and the curative effect was also significant. Therefore, it is possible that these diseases may also be treated with routine doses of hormones rather than high-dose hormonal pulse therapy. However, this case is an isolated case, which will require extensive clinical trials in the future. In addition to first-line treatment, some patients received second-line treatment such as MMF, RTX, AZA, CTX, natalizumab. After the acute phase, some patients relapsed during or after oral prednisolone reduction therapy [10, 13]. This was especially the case in patients who did not receive second-line treatment at the time of the first attack. The timing and scheme of starting second-line therapy might be a future research direction.
Prior to the second episode (spontaneous discontinuation of prednisone), the patient fell and fractured his arm. We analyzed whether this fall event might have been related to vertigo, limb weakness, epileptic seizure, or gait instability caused by MNOS recurrence. Of course, it is not excluded that the patient may have accidentally tripped, and this accidental fall resulted in disease recurrence. To reduce the risk of future recurrence, we decided to add mycophenolate mofetil treatment to this patient. According to the literature review [27], the recurrence rate of anti-NMDAR encephalitis was between 4% and 26% [28, 29], while the recurrence rate of MOG antibody disease is between 60% and 90% [30, 31, 32, 33]. Of the 18 patients in this group, 13 had a recurrence and was closer to the recurrence rate of MOG antibody disease. Therefore, MOG antibodies might play an important role in the recurrence of MNOS. Serum MOG antibody monitoring is essential in future follow-ups. Another study [34] suggested that some patients with anti-NMDAR encephalitis relapse due to concurrent tumors. Therefore, this study will continue tumor screening during the follow-up period.
To sum up, MNOS is still in the exploratory stage. And the mechanism and treatment are not yet perfect. It is hoped that this article can provide some modest help for future expert guidelines or consensus to guide the diagnosis and treatment of MNOS.
ADEM, acute disseminated encephalomyelitis; AIE, autoimmune encephalitis; anti-NMDAR-Abs, anti-N-Methyl-D-aspartate receptor antibodies; anti-MOG, anti-myelin oligodendrocyte glycoprotein; AQP4, Aquaporin-4; AZA, azathioprine; BBB, blood-brain barrier; CBA, cell-based assay; CMV, cytomegalovirus; CSF, cerebrospinal fluid; CTX, cyclophosphamide; EB, epstein–barr; ELISA, enzyme-linked immunosorbent assay; FLAIR, fluid attenuation inversion recovery; HDMT, high-dose methylprednisolone pulse therapy; HSV, herpes simplex virus; IIFT, indirect immune-fluorescence test; IVIG, intravenous immunoglobulin; MBP, myelin basic protein; MMF, mycophenolate mofetil; MNOS, MOG antibody disease and NMDARE overlapping syndrome; MOG, myelin oligodendrocyte glycoprotein; MOG-Abs, myelin oligodendrocyte glycoprotein-antibodies; MRI, magnetic resonance imaging; MS, multiple sclerosis; NMDAR, N-methyl-D-aspartate receptor; NMDARE, anti-NMDAR encephalitis; NMOSD, neuromyelitis optica spectrum disorder; OCT, optical coherence tomography; PE, plasmapheresis; RTX, rituximab; VEEG, video electroencephalogram; VZV, varicella-zoster virus.
YL, MW, and JT provided assistance and advice on patient diagnosis and treatment. MW, ZZ, YW, YY and SYB collected relevant literature and data. MW, JT and SYB wrote the paper.
The case report was approved by the Ethics Committee of the Second Hospital of Dalian Medical University (No. 2021-064).
We sincerely thank the patient and his family for their invaluable participation and cooperation.
This study was supported by grants from the Science and Technology Innovation Foundation of Dalian City (No. 2020JJ26SN054) and United Fund of the Second Hospital of Dalian Medical University and Dalian Institute of Chemical Physics, Chinese Academy of Sciences (No. UF-QN-202002).
The authors declare no conflict of interest.