

1 Department of Neurosurgery, The Second Affiliated Hospital of Nanjing Medical University, Nanjing, 210011, P. R. China
2 Department of Geriatrics, Jinling Hospital of Nanjing, Nanjing, 210013, P. R. China
#These authors contributed equally.
Abstract
The two most common surgical interventions for spontaneous intracerebral hemorrhage in the basal ganglia of patients more than 65 years old are either minimally invasive puncture and drainage or craniotomy. This study aimed to compare the curative effects of these two procedures in such patients. A retrospective study of patients older than years with spontaneous intracerebral hemorrhage was conducted between January 2012 and December 2015. Of the 86 patients, 47 received minimally invasive puncture and drainage and 39 underwent craniotomy. One year after surgery no statistically significant difference was observed between the two groups with respect to: evacuation rate of the hematoma five days after the operation, volume of residual hematoma, occurrence of rebleeding, development of infectious meningitis, length of hospitalization, fatality, or Glasgow Outcome Scale and Barthel Index scores. However, the amount of blood loss during the procedure (P < 0.001), total cost of hospitalization (P = 0.004), and incidence of epilepsy (P = 0.045) were significantly higher for the craniotomy group than the minimally invasive puncture and drainage group. It was found that, in patients older than 65 years with basal ganglia hemorrhage, minimally invasive puncture and drainage is less invasive, more cost efficient and induces less bleeding during surgery than craniotomy.
Keywords
- Intracerebral hemorrhage
- minimally invasive puncture and drainage
- craniotomy
- neurosurgery
Spontaneous intracerebral hemorrhage (ICH) is a devastating manifestation of cerebrovascular disease, with extremely high disability and mortality rate (Bae et al., 1992; Jianwei et al., 2009). The basal ganglia are the most frequent sites of ICH (Dye et al., 2012; Mendelow et al., 2005). The incidence of senile hypertensive ICH is increaseing due to the rising age of the population. When compared with younger patients, elderly patients with ICH often have other underlying diseases. Their treatment therefore becomes more complicated and selecting the optimal treatment is critical for good functional outcomes.
The treatment of ICH involves the administration of antihypertensive drugs, symptomatic treatment and surgical intervention whenever necessary. Pharmacological therapy is suitable for patients with little bleeding or deeply located hemorrhage. Close observation of patient consciousness and pupillary change is essential, in addition to controlling blood pressure and intracranial pressure. Surgical treatment is suitable for patients with blood loss > 30 ml when a hematoma is located near the basal ganglia (Cordonnier et al., 2018; Veltkamp and Purrucker, 2017). Several conventional surgical methods are available for the treatment of ICH in patients more than 65 years old. The two most commonly used surgical techniques are minimally invasive puncture and drainage (MIPD) and craniotomy (Di et al., 2018). Craniotomy has been the conventional procedure for treating ICH for several years. During the procedure, the hematoma is removed quickly and intracranial pressure is reduced by separating the lateral fissure or cortical fistulas. However, the craniotomy procedure is itself traumatic for patients with ICH. Particularly in older patients, this trauma can lead to major disability or death. Therefore, MIPD may be a better option than crainotomy as it is less invasive and involves less manipulation of viable brain tissue during the procedure, although MIPD does not necessarily clear the hematoma as quickly. Moreover, drainage-tube placement can be time-consuming, increasing the risk of infection (Table 1). Despite the widespread use of these two surgical techniques, the best treatment option for ICH in the basal ganglia in patients older than 65 years has not been established. Hence, the aim of this study was to compare the curative effects of either MIPD or craniotomy for spontaneous ICH in the basal ganglia of patients older than 65 years to determine the better method of treatment.
| MIPD | Craniotomy | |
|---|---|---|
| trauma | less | great |
| Intraoperative bleeding volume | less | more |
| Operation time-consuming | short | long |
| intracranial pressure reduced | slowly | quickly |
| hematoma removed | slowly | quickly |
| risk of infection | high | low |
MIPD, minimally invasive puncture and drainage.
Eighty-six patients older than 65 years with spontaneous ICT that underwent MIPD or craniotomy between January 2012 and December 2015 were included in this retrospective study. The study was approved by the Jinling Hospital Ethics Institutional Committee (JLEC-LCYJ-20180676). Each patient involved in the study provided informed consent. All methods were carried out in accordance with approved institutional guidelines and regulations and the surgeries were performed by the same group of neurosurgeons. The diagnosis of ICH was confirmed by computer tomography (CT) imaging of the head and was made according to the diagnostic criteria described in the guidelines for the primary prevention of stroke (Meschia et al., 2014). The criteria for patient selection were the presence of ICH in the basal ganglia with a volume > 30 ml and an interval of < 24 hours between hemorrhage onset and surgery. The volume of the hematoma (excluding the hematocele in the ventricle and subarachnoid space) was accurately calculated by three-dimensional slicer software. Hematoma evacuation magnitude was calculated as (preoperative hematoma volume-postoperative hematoma volume) / preoperative hematoma volume (Kaya et al., 2003). The midline shift was defined as the distance from the midline to the fornix or the foramen of Monro. Preoperative clinical grading of the disease was performed using the Glasgow Coma Scale (GCS). Patients with mainly thalamic or subcortical hemorrhage were excluded.
2.1.1 MIPD group
A total of 47 patients underwent MIPD for the study, including 26 men and 21 women aged 65-93 years old (mean age, 74.1 ± 8.6 years). The preoperative hemorrhage volume, as measured from axial CT imaging, ranged from 32-89 ml (mean volume, 44.6 ± 12.6 ml). The midline shift, as measured from preoperative CT images, ranged from 2-16 mm (mean shift, 8.1 ± 4.6 mm). The mean preoperative GCS score for patients was 8.3 ± 3.9 (Table 2).
| MIPD | Craniotomy | P | |
|---|---|---|---|
| Patient (n) | 47 | 39 | |
| Mean age (y) | 74.1 ± 8.6 | 72.8 ± 10.6 | 0.41 |
| Sex, male:female | 26: 21 | 24: 15 | 0.56 |
| Location, right:left | 18: 29 | 14: 25 | 0.82 |
| Pre-operative hematoma volume (mL) | 44.6 ± 12.6 | 48.6 ± 15.2 | 0.63 |
| Midline shifting (mm) | 8.1 ± 4.6 | 10.2 ± 6.9 | 0.26 |
| Pre-operative GCS score | 8.3 ± 3.9 | 7.6 ± 4.6 | 0.38 |
MIPD, minimally invasive puncture and drainage.
2.1.2 Craniotomy group
A total of 39 patients underwent craniotomy for the study, including 24 men and 15 women aged 66-84 years (mean age, 72.8 ± 10.6 years). The preoperative hemorrhage volume, as measured from axial CT imaging, ranged from 36-92 ml (mean volume, 48.6 ± 15.2 ml). The midline shift, as measured from preoperative CT imaging, ranged from 3-22 mm (mean shift, 10.2 ± 6.9 mm). The mean preoperative GCS score for patients was 7.6 ± 4.6 (Table 2).
2.2.1 MIPD group
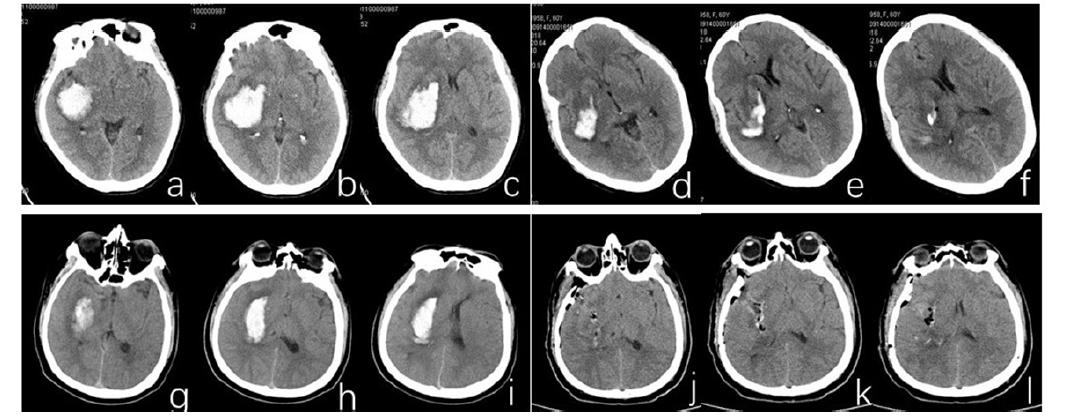
The patient was placed in a supine position with the head slightly flexed. A Medtronic StealthStation AxiEM7 TM navigation system was used. The entry point was Kocher’s area, ipsilaterally. A 12 French drainage catheter was inserted into the center of the hematoma cavity. Hematoma evacuation was performed by manual suction using a 20 ml syringe. The total volume of the evacuated hematoma ranged from 10-20 ml. The drainage tube was fixed to the scalp and connected to an extracranial disposable drainage device with a three-way valve at the distal end to control the drainage pressure. The drainage device was placed < 10 cm above the position of the external ear hole on the patient’s head. Following this, 20,000 units of urokinase dissolved in 2- 5 ml of normal saline was injected 1-2 times each day to liquefy the clot. The three-way valve was opened for drainage every two hours. Brain CT was performed, and changes in the hematoma were observed continuously. The tube was closed for 24 hours when the hematoma and cerebroventricular hematocele were no longer visible, and the drainage tube was removed when no obvious headaches or increased intracranial pressure were observed (Fig. 1a-f).
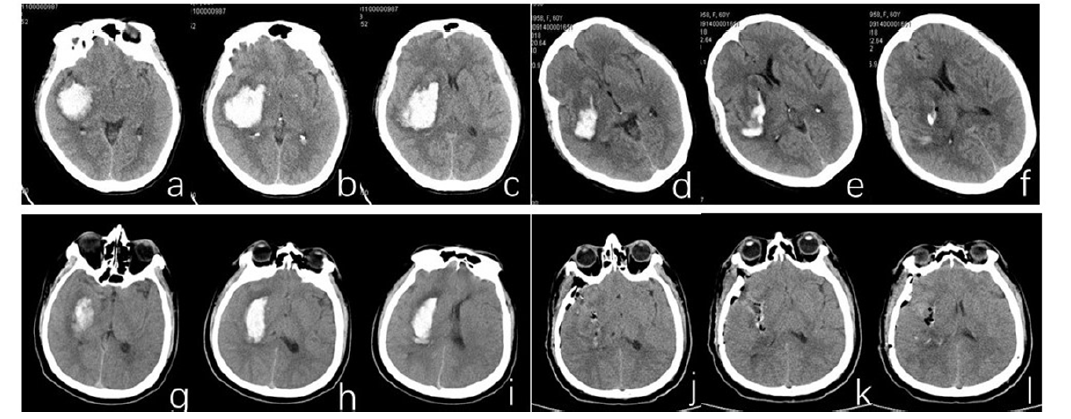 Figure 1.
Figure 1.Computer tomography images acquired from a 71-year-old patient with basal ganglia hemorrhage (a-c) before and (d-f) three days after a minimally invasive puncture and drainage procedure. Computer tomography images acquired from a 68-year-old patient with basal ganglia hemorrhage (g-i) before and (j-l) one day after a craniotomy operation.
2.2.2 Craniotomy group
The patient was placed in a supine position, adjust the head angle so that intracranial hematoma was most easily exposed. The (Dandy’s) craniotomy size varied from small to large and was determined by the preoperative neurological condition of the patient. A small corticectomy site was created and the hematoma cavity was entered. Hematoma evacuation was performed using suction and bipolar cautery. The hematoma cavity was covered with Surgicel. A hematoma catheter was inserted into the hematoma cavity in case of residual hematoma. Replacement of the skull bone was determined based on the condition of the brain after ICH evacuation (Fig. 1g).
To assess and establish the curative effects of the two surgical procedures the following parameters were evaluated: the evacuation rate at days one and five, occurrence of rebleeding, residual hematoma, blood loss during surgery, and total cost of hospitalization. The patient's functional independence was assessed by GOS and Barthel index (BI) one year after surgery. Cumulative case fatality and incidence of epilepsy were also recorded.
Statistical analyses were performed using SAS version 9.1.3 (SAS Institute Inc., Cary, NC, USA). Continuous variables are presented as mean ± standard deviation, and categorical variables are presented as frequency (%). Age, sex, location of lesion and surgical outcomes were compared between the groups using a chisquare test (n ≥ 5, total n ≥ 40), chi-square test with continuity correction (n < 5, total n ≥ 40) or unpaired t-tests. A P-value < 0.05 was assumed to indicate a statistically significant difference between groups.
The MIPD and craniotomy groups consisted of 47 and 39 patients, respectively. The mean patient age was not significantly different for the two groups (P = 0.41; Table 3). No significant differences were observed for sex, hematoma location, preoperative hematoma volume, displacement of the midline of the brain, or initial GCS score (Table 3).
| MIPD Craniotomy | |||
|---|---|---|---|
| Clinical outcomes | MIPD (47) Craniotomy (39) | P | |
| ER at day 1 (%) | 38.9 ± 18.7 | 85.8 ± 20.9 | 0.003 |
| ER at day 5 (%) | 84.1 ± 11.6 | 89.3 ± 12.4 | 0.71 |
| Residue hematoma (ml) | 6.7 ± 3.6 | 7.9 ± 4.2 | 0.55 |
| Rebleeding (n) | 3 | 2 | 1.00 |
| Blood loss during OP (ml) | 18.9 ± 8.4 | 124.6 ± 33.2 | < 0.001 |
| infectious meningitis | 2 | 2 | 1.00 |
| hospitalization length (day) | 14.8 ± 4.6 | 16.2 ± 5.1 | 0.47 |
| Total expenditure (¥, thousand yuan) | 35.3 ± 6.4 | 52.2 ± 9.7 | 0.004 |
| case fatality (n) | 10 | 8 | 0.93 |
| Epilepsy (n) | 2 | 8 | 0.045 |
| GOS at 1 year after OP | 3.8 ± 0.9 | 3.5 ± 0.7 | 0.61 |
| BI at 1 year after OP | 78.6 ± 13.2 | 77.6 ± 14.5 | 0.37 |
MIPD, minimally invasive puncture and drainage; ER, evacuation rate; OP: operation; GOS: Glasgow Outcome Scale; BI: Barthel Index.
One day postoperatively the evacuation magnitude of the hematoma was significantly higher (P = 0.003) for the craniotomy group (85.8 ± 20.9) than for the MIPD group (38.9 ± 18.7). Following several days of urokinase administration, the evacuation magnitude of the hematoma on postoperative day five was not significantly different between the MIPD and craniotomy groups (P = 0.71). Further, no significant difference in residual hematoma volume was observed between the two groups (P = 0.55). One year after surgery no significant differences between the two groups were observed with respect to rebleeding, the presence of infectious meningitis, length of hospitalization, case fatality, or GOS and BI scores (Table 3).
The amount of blood loss during surgery was significantly higher for the craniotomy group (124.6 ± 33.2 ml) than for the MIPD group (18.9 ± 8.4 ml) (P < 0.001). The total cost of hospitalization was also significantly higher for the craniotomy group than for the MIPD group (P = 0.004). The incidence of epilepsy in the craniotomy group was significantly higher than that of the MIPD group one year after surgery (P = 0.045, Table 3).
The prognosis of spontaneous hypertensive ICH is related to the severity of bleeding, hematoma size and location of bleeding (Mitra et al., 1995; Poon et al., 2014). Elderly patients with ICH often have an underlying disease that renders their treatment more complexand difficult. Surgical intervention can improve both the possibility and duration of survival of these patients. Treatment is generally classified into one of two major types: hematoma evacuation by craniotomy or drainage through burr holes (Bosel et al., 2015; Hanley et al., 2016; Sangha and Gonzales, 2011).
Evacuating the hematoma through craniotomy can remove the hematoma and quickly reduce the intracranial pressure in patients with spontaneous ICH. It is possible to explore the bleeding point and conduct electrocoagulation and compression hemostasis during evacuation of the intracranial hematoma. Vascular malformations, if detected, can be simultaneously removed. However, this procedure requires an incision in the temporal cortex in order to access and effectively evacuate the hematoma. Intraoperative traction causes considerable trauma to the brain tissue (Zhu et al., 2012). Further, the craniotomy itself is traumatic. The trauma of surgery may aggravate the condition of patients, particularly those older than 65 years. The follow-up evaluation of the craniotomy group in the present study revealed that the clearance rate of the intracranial hematoma was as high as 85.8% and the residual hematoma rate was as low as 7.9% at the time of discharge.
In MIPD, drainage and surgery are performed by making a small incision in the skin and a small drilled hole in the skull. Compared to craniotomy, MIPD is advantageous because of lower operative trauma and blood loss and a shorter operation time; however, a hematoma typically cannot be completely removed and effective hemostasis is not possible, resulting in recurrent hemorrhage after surgery. Moreover, the time required for placement of the drainage tube may increase the risk of intracranial infection. Nevertheless, such disadvantages can be managed by using a navigation system (Dye et al., 2012). In this study, only three patients in the MIPD group experienced rebleeding. Moreover, the average hematoma drain retention period was 4.6 days and only two patients developed infectious meningitis.
In this study, comparisons of craniotomy and MIPD found no statistically significant difference between the two procedures in terms of evacuation magnitude of the hematoma five days after surgery, volume of residual hematoma, occurrence of rebleeding, development of infectious meningitis, length of hospitalization, case fatality, or GOS and BI scores one year after surgery. Although the hematoma clearance rate of the MIPD group was lower than that of the craniotomy group on day one after surgery, following administration of urokinasethere there was no significant difference identified between the two groups on postoperative day five. Moreover, one year after surgery no significant differences in the GOS and BI scores were found between the two groups.
This study revealed that the amount of blood lost during surgery, total cost of hospitalization, and incidence of epilepsy were significantly higher in the craniotomy group than the MIPD group. This suggests that, compared to MIPD, craniotomy is associated with greater trauma and economic burden for patients.
The results of the current study indicate that for patients with ICH in the basal ganglia who are older than 65 years, MIPD is less invasive, more economic, and involves less bleeding during surgery than craniotomy. With the administration of urokinase after surgery, no significant difference in hematoma clearance was found for either surgical treatment. Long-term follow-up evaluation did not reveal significant differences in the operative results of the two treatment types. Collectively, however, this study suggests that MIPD is more suited than crainotomy to patients older than 65 years with cerebral hemorrhage.
Fund: Nanjing Military Region Medical and Health Research Fund (11MA101).
The authors declare no competing interests.