

 , Min Lu 2, Xuee Shi 3, Fang Feng 3,*
, Min Lu 2, Xuee Shi 3, Fang Feng 3,* , Jinquan Zhou 3
, Jinquan Zhou 31 Department of Emergency Intensive Care Unit, Gansu Provincial Central Hospital, 730000 Lanzhou, Gansu, China
2 Department of Medical Oncology of the Second Hospital of Gansu Province, 730015 Lanzhou, Gansu, China
3 Department of Critical Care Medicine, The Second Hospital & Clinical Medical School of Lanzhou University, 730000 Lanzhou, Gansu, China
Abstract
To explore whether vitamin C supplementation in sepsis patients can reduce the occurrence of acute kidney injury.
A prospective, randomized and controlled pilot trial was conducted. All individuals participating in the study received comprehensive initial treatment for sepsis. This involved monitoring lactate levels, ensuring appropriate fluid resuscitation, administering empiric broad-spectrum antibiotics, and using vasoactive medications, with a preference for norepinephrine. If the norepinephrine dosage exceeded 20 μg/min, vasopressin was introduced at a rate of 0.03 U/min to sustain a mean arterial pressure of at least 65 mmHg. The experimental group was given vitamin C (1.5 g every 6 h by intravenous infusion) for 3 consecutive days, while the control group was given placebo.
A total of 40 patients with sepsis were included in the study following application of the inclusion and exclusion criteria. Patients were randomized into control (n = 20) and experimental (n = 20) groups. No significant differences in baseline characteristics were found between the two groups (all p > 0.05). Among the 40 sepsis patients, 5 (25%) in the experimental group and 14 (70%) in the control group developed acute kidney injury, all of whom required support with continuous renal replacement therapy (RRT). The main site of infection was pulmonary, accounting for 70% of cases in the experimental group and 75% in the control group. The most common pathogenic bacteria were gram-negative bacilli (26/40, 65%). The experimental group had a significantly shorter length of stay in intensive care unit (ICU) compared to the control group (11.8 ± 2.7 days vs. 13.9 ± 2.1 days, p = 0.008), less frequent use of vasoactive drugs (35% vs. 75%, p = 0.011), and less frequent need for RRT within 72 h of admission (25% vs. 70%, p = 0.004). However, the mortality rate in ICU was not significantly different (10% vs. 15%, p = 0.633).
The use of vitamin C in patients with sepsis is associated with a reduced incidence of acute kidney injury, although a larger sample size is required to confirm this finding.
This trial was registered at Chinese Clinical Trial Registry (ChiCTR2400093794, https://www.chictr.org.cn/hvshowproject.html?id=265499&v=1.0).
Keywords
- sepsis
- oxidative stress
- acute kidney injury
Sepsis is the leading cause of acute kidney injury (AKI), contributing almost half the cases of renal insufficiency in intensive care units [1]. The development of AKI during episodes of sepsis is a significant and independent prognostic indicator of extended hospital stays and in-hospital mortality [2]. Moreover, epidemiological data increasingly suggests that individuals who survive mild or brief episodes of AKI face an increased risk of subsequently developing chronic kidney disease (CKD) and end-stage renal disease [3]. The essential treatment for sepsis currently includes antibiotics, fluid resuscitation, and vasopressor support. Renal replacement therapy (RRT) is advised for patients experiencing severe septic AKI [4]. Nevertheless, these interventions are primarily palliative and aimed at sustaining life with the goal of kidney recovery. Consequently, a deeper understanding of the pathophysiological mechanisms underlying septic AKI is crucial for the development of effective, mechanism-based therapeutic strategies.
Ascorbic acid, commonly known as vitamin C, is a water-soluble vitamin integral to various bodily functions. This antioxidant acts as an electron donor to effectively neutralize free radicals. By inhibiting the NADPH oxidase (NOX) pathway, vitamin C limits the formation of new free radicals, which also increases the activity of other antioxidants [5]. The antioxidant properties of vitamin C can lead to decreased endothelial permeability, thereby improving the function of both microvascular and macrovascular systems, and diminishing cell apoptosis in pathological states [6, 7]. Vitamin C also plays a crucial role in the synthesis of endogenous vasopressin, and can influence the responsiveness of patients to this hormone. Consequently, we designed a prospective, randomized and controlled pilot study to investigate whether the administration of vitamin C to patients experiencing sepsis can reduce the incidence of AKI.
Under sepsis conditions, the body’s intake and absorption are known to decrease, while metabolism increases, resulting in a lower level of plasma vitamin C [8]. In about 90% of sepsis patients, the plasma vitamin C level is less than 23 µmol/L. Severe vitamin C deficiency can lead to multiple organ dysfunction, while exogenous supplementation of vitamin C is effective at reducing the mortality rate. A randomized controlled trial reported that giving high-dose vitamin C to patients with sepsis can reduce oxidative damage to endothelial cells and other cell types, thereby improving tissue perfusion and oxygenation and reducing subsequent organ dysfunction [9]. Vitamin C is widely used in clinical practice and can protect cell components from reactive oxygen and free radical-mediated oxidative stress responses, while also participating in collagen secretion and the biosynthesis of dopamine and other molecules.
The impact of vitamin C on clinical outcomes in critically ill patients remains controversial, and research findings are inconclusive. A retrospective observational cohort study [10] evaluated the effects of vitamin C treatment on AKI and mortality in patients with sepsis. The electronic medical records of 1390 patients from a single institute were analyzed, with the data revealing that vitamin C treatment was associated with an increased risk of AKI (OR = 2.07, 95% CI [1.46–2.93]) and in-hospital mortality (OR = 1.67, 95% CI [1.003–2.78]) after adjusting for demographic and clinical covariates. When stratifying for intensive care unit (ICU) patients, vitamin C treatment remained a significant risk factor for AKI (OR = 1.61, 95% CI [1.09–2.39]) and did not protect against mortality (OR = 0.79, 95% CI [0.48–1.31]) [11]. Given these reported associations with AKI and mortality, the continued use of high-dose vitamin C in sepsis patients requires further evaluation.
Clinically relevant data including age, sex, SOFA score, APACHE II score, infection site, type of bacterial infection, comorbidities, and vasoactive drug use were collected in tabular form from patients with sepsis and septic shock who were admitted to our hospital between December 2024 and February 2025.
Trial design and sample size calculation: This was a prospective, randomized,
and controlled pilot trial. The study was approved by the Ethics Committee of the
Second Hospital of Lanzhou University (approval number 2024A-1348). It was
registered with the China Clinical Trial Center (registration number
ChiCTR2400093794). A priori power analysis was performed by an
independent statistician to determine the required sample size. Large effect size
was calculated by PASS software Version: 25.0.3 NCSS LLC (Kaysville, UT, USA)
and the power for the primary endpoint (incidence of AKI) was calculated based on
a two-sided t-test with a significance level of 5%. The power with
regard to the co-primary dichotomous endpoints (proportion of subjects with 5%
incidence of AKI) was calculated based on a two-sided chi-square test. With a
sample size of 40, the study was estimated to have 80% statistical power at the
Inclusion Criteria: the patient met the Sepsis 3.0 diagnostic criteria.
Exclusion Criteria: age
Patients admitted to hospital from December 2024 to February 2025 for sepsis were prospectively enrolled in the study. They were randomly divided into experimental and control groups according to a computer-generated random sequence list that was subsequently placed in a sealed envelope. All study personnel were blind to treatment allocation, and had no influence on whether the participant received vitamin C or placebo. The blank preparation was consistent with the test drug in terms of appearance, shape, odor, and specifications. All patients included in the study received a combination basic treatment for sepsis that included measurement of lactate levels, adequate fluid resuscitation, empiric broad-spectrum antibiotics, and vasoactive drugs. Norepinephrine was used as the preferred vasoactive drug, but when the dosage exceeded 20 µg/min, vasopressin (0.03 U/min) was added to maintain the mean arterial pressure above 65 mmHg. In addition, the experimental group was given vitamin C (1.5 g every 6 h by intravenous infusion) for 3 consecutive days, while the control group was given placebo. The vitamin C infusion mixture was 5 mL:1 g (Shanghai Modern Hasen [Shangqiu] Pharmaceutical Co., Ltd, Shanghai, China. Batch number: National Drug Approval No. H20053054).
Definitions: The diagnostic criteria for AKI were as specified in the KDIGO guidelines [12]. The Sepsis 3.0 guidelines [13] were used to define sepsis.
Primary outcome: The occurrence of AKI, as defined by simultaneous presence of the sepsis consensus criteria (Sepsis 3.0 recommended definition) and the AKI criteria (KDIGO criteria), within 7 days after the diagnosis of sepsis.
Secondary outcomes: Length of stay in ICU, need for vasoactive drug support, number of RRTs required within 72 h of admission, ICU mortality rate, and the levels of IL-6 and Neutrophil Gelatinase-associated Lipocalin (NGAL) as determined by the ELISA detection method.
Statistical analysis of the data was conducted using SPSS 21.0 software (SPSS
Inc., Chicago, IL, USA). The Shapiro-Wilk test and Levene’s test were used to
assess the normality of data distribution and the equality of variance. For
datasets exhibiting a normal distribution, results were expressed as the mean
Following application of the inclusion and exclusion criteria, a total of 40
patients with sepsis and septic shock were included in the trial, with 20 each in
the experimental and control groups (Fig. 1). Table 1 presents the general
characteristics for the two groups. Among the 40 sepsis patients included in the
study, 5 (25%) in the experimental group and 14 (70%) in the control group
developed AKI, with all requiring continuous RRT support. The main infection site
in both groups was pulmonary (70% in the experimental group and 75% in the
control group). The main pathogenic bacteria were gram-negative bacilli (26/40,
65%). The average length of stay in the ICU was 11.8
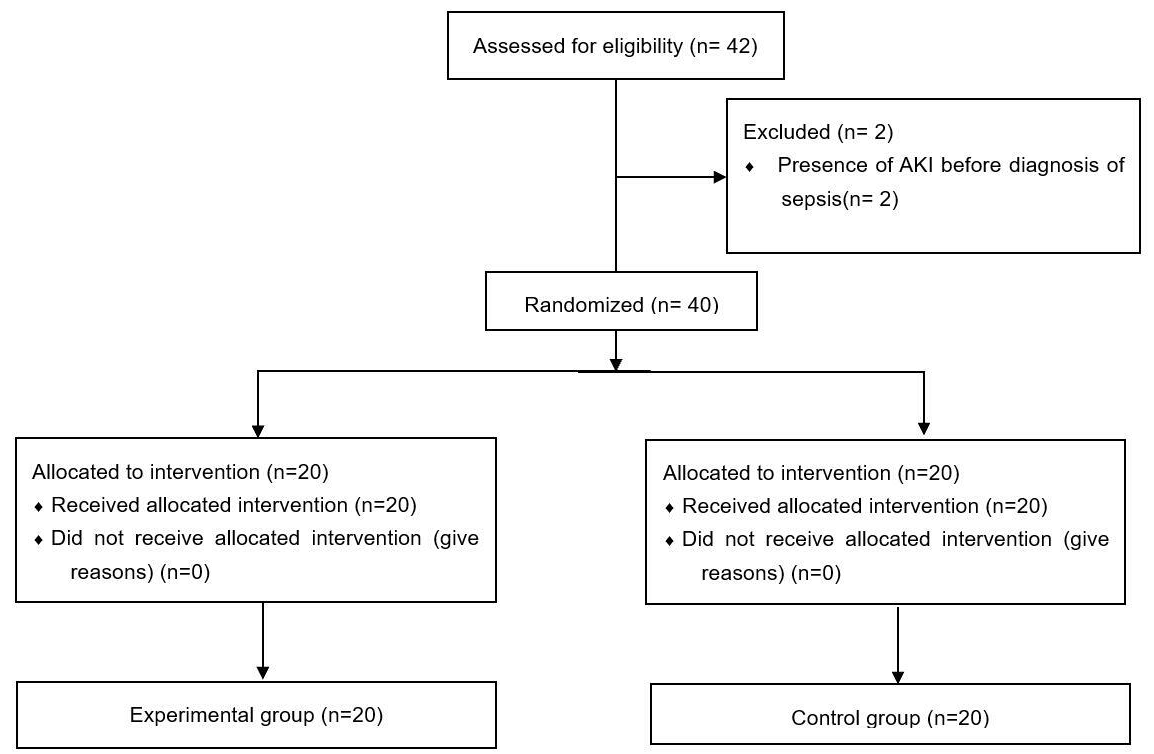 Fig. 1.
Fig. 1.
Flow diagram.
| Experimental group (n = 20) | Control group (n = 20) | p-value | ||
| Age (years) | 55.6 |
52.6 |
0.607 | |
| Sex (male) | 12 (60%) | 11 (55%) | 0.749 | |
| Source of Infection | 0.881 | |||
| Pneumonia | 14 (70%) | 13 (65%) | ||
| BSI | 3 (15%) | 2 (10%) | ||
| Urosepsis | 2 (10%) | 2 (10%) | ||
| Other | 1 (5%) | 3 (15%) | ||
| Comorbidities | ||||
| Diabetes | 12 (60%) | 14 (70%) | 0.797 | |
| Hypertension | 10 (50%) | 12 (60%) | 0.444 | |
| Mechanical ventilation | 9 (45%) | 8 (40%) | 0.756 | |
| Arterial lactate level (mmol/L) | 2.9 |
3.5 |
0.001 | |
| Procalcitonin level (ng/mL) | 35 (28–100) | 31 (19–47) | 0.069 | |
| SOFA score | 9.7 |
10.7 |
0.356 | |
| Change in SOFA score at 72 h | –4 (–6 to –1) | –2 (–3 to 0) | 0.043 | |
| APACHE II score | 10.4 |
9.8 |
0.236 | |
| sCr initial (µmol/L) | 81.1 |
87.5 |
0.199 | |
| IL-6 (pg/mL) | 79.35 |
76.44 |
0.334 | |
| NGAL (ng/mL) | 4.9 |
5.1 |
0.238 | |
| Pathogenic bacteria | ||||
| Gram-negative bacilli | 11 | 15 | 0.312 | |
| Negative cultures | 9 | 5 | 0.291 | |
BSI, blood stream infection; sCr, serum creatinine; SOFA, sepsis-related organ failure assessment; APACHE, Acute Physiology and Chronic Health Evaluation; NGAL, Neutrophil Gelatinase-associated Lipocalin.
| Experimental group (n = 20) | Control group (n = 20) | p-value | |
| Use of vasoactive drugs | 7 (35%) | 15 (75%) | 0.011 |
| ICU stay (days) | 11.8 |
13.9 |
0.008 |
| Need CRRT at 72 h | 5 (25%) | 14 (70%) | 0.004 |
| ICU Mortality | 2 (10%) | 3 (15%) | 0.633 |
| IL-6 (pg/mL) | 16.41 |
39.82 |
0.003 |
ICU, intensive care unit; CRRT, continuous renal replacement therapy.
Vitamin C is an essential cyclic antioxidant that plays a vital role in directly neutralizing reactive oxygen species (ROS) and boosting the levels of endogenous glutathione, thereby helping to regenerate the host’s antioxidant defense system. It also acts as an immune enhancer to stimulate macrophage activity [14], while having the capacity to directly inhibit bacterial cations [15, 16]. Additionally, vitamin C can reduce the expression of adhesion molecule 1 in human endothelial cells in a dose-dependent manner following stimulation by TNF. This suggests a potential capacity to mitigate microvascular obstruction by white blood cells and the impairment of microcirculation. Furthermore, vitamin C serves as a crucial auxiliary factor for the synthesis of endogenous vasoconstrictors, such as norepinephrine, and for vessel compression, allowing patients to respond more effectively to vasoactive drug therapies. It is worth noting that critically ill patients often exhibit significantly lower plasma levels of vitamin C [17]. Humans cannot naturally synthesize vitamin C, partially explaining the decrease in vitamin C during sepsis. Because of the presence of saturated intestinal sodium-dependent vitamin C transfer protein (SVCTS), intake through the intestine is insufficient to ensure normal levels of plasma vitamin C, thus requiring intravenous treatment [18].
Monocytes and granulocytes in sepsis patients can be separated by differential sedimentation and centrifugation, and their vitamin C content measured with the dinitrophenylhydrazine method. The concentration of vitamin C in monocytes is 80-fold higher than in plasma, while its concentration in granulocytes is 25-fold higher [19]. Vitamin C is known to play an important role in both monocytes and granulocytes. In clinical trials involving intravenous injection of 1 g of vitamin C in septic shock patients and healthy controls, the vitamin C level decreased more rapidly in the septic shock patients, suggesting higher consumption in these patients and possible accumulation in monocytes and granulocytes [20].
In a randomized double-blind trial in the USA [21], 137 patients with sepsis
were randomly divided into treatment and control groups. The treatment group was
given vitamin C, hydrocortisone and thiamine, while the control group was given a
combination of hydrocortisone and thiamine. The shock reversal time, sequential
organ failure score, procalcitonin clearance rate, and hospitalization time for
the two groups were compared to evaluate the therapeutic effect of vitamin C. The
SOFA score in the treatment group was significantly lower compared to the control
group (p
While animal studies on early sepsis have shown advantages with vitamin C, its effectiveness in human subjects is still debated. Two small-scale (n = 24 and n = 28), single-center randomized clinical trials demonstrated that intravenous vitamin C doses of between 50 and 200 mg/kg/day led to a reduction in inflammatory biomarkers and SOFA scores [22] and improved patient sensitivity to vasoactive drugs (25 mg/kg every 6 h) [23]. However, in three subsequent multicenter RCTs (VITAMINS [24], ACTS [25] and ATESS [26]), no difference in hospital mortality was observed when vitamin C (6 g/day) was combined with thiamine and corticosteroids, and RRT support was needed at 72 h.
Our study found that patients with sepsis who received venous infusion of 1.5 g
of vitamin C for 6 h showed reduced RRT support at 72 h, with only 25% requiring
RRT in the experimental group compared to 70% in the control group. Upon
admission, NGAL levels were normal in both groups, indicating the absence of any
underlying AKI in either group. Since NGAL is an early predictor of AKI, it was
not reassessed after treatment. Following the administration of vitamin C, the
IL-6 level in the experimental group decreased from 79.35
The administration of vitamin C to patients with sepsis could reduce the occurrence of AKI. However, more studies with a larger sample size are needed to confirm this finding.
Data is provided within the manuscript.
Conducted the study: YC, FF. Collected all data: ML, XES, JQZ. Performed the statistical analysis: YC. All authors have contributed to the editorial changes made to the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was approved by the Ethics Committee of the Second Hospital of Lanzhou University (approval number 2024A-1348). The study was registered with the China Clinical Trial Center (registration number ChiCTR2400093794). Informed consent was signed by the patient or a family member in all 40 cases included in the study. If the patient was unable to complete the signature due to the use of sedative drugs, coma, etc., his or her immediate family members were consulted to provide informed consent. The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Not applicable.
Gansu Provincial Science and Technology Plan Funding (Natural Science Foundation Project 23JRRA0965, 24JRRA357).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.