




 , Hui Zhang 1, Kai Yuan 2, Yanhua Bi 1, Quanyu Wang 1,*,†, Jinlong Zhang 2, Jiangkui Liu 1, Limei Zhi 1, Fengxia Guo 1, Jinguo Cui 3, Fei Liang 1
, Hui Zhang 1, Kai Yuan 2, Yanhua Bi 1, Quanyu Wang 1,*,†, Jinlong Zhang 2, Jiangkui Liu 1, Limei Zhi 1, Fengxia Guo 1, Jinguo Cui 3, Fei Liang 11 Department of Interventional Surgery, General Hospital of Huabei Petroleum Administration Bureau, 062550 Cangzhou, Hebei, China
2 Department of Radiology, Beijing Tongren Hospital, Capital Medical University, 100730 Beijing, China
3 Department of Interventional Surgery, Bethune International Peace Hospital, 050000 Shijiazhuang, Hebei, China
†These authors contributed equally.
Abstract
There is no universally accepted understanding of the complex pathogenesis of Benign Prostatic Hyperplasia (BPH). Precision prostate artery embolization (PPAE) is performed under the guidance of digital subtraction angiography and can alleviate clinical symptoms caused by BPH. This research assessed the effectiveness of PPAE combined with highly specific α1 blockers for elderly BPH patients.
The 144 elderly BPH patients were split into two groups: 80 for observation and 64 for control. The study treated all participants with α1 blockers, while the observation group additionally received precise prostatic artery embolization (PPAE). Changes in clinical symptoms before and after therapy were monitored.The statistical assessment was done by SPSS 22.00. Count data were reported as a percentage (%), while data were expressed as the Mean ± Standard Deviation (SD). The threshold of significance was p < 0.05.
The treatment led to a significantly greater overall effective rate in the observation group than in the control group (p < 0.05). Both groups had lower international prognostic scoring system (IPSS) and urinary symptom distress (BS) levels than before therapy (p < 0.05), with the observation group also having lower scores. After 2 weeks, 1 month, 6 months and 1 year of therapy, both groups saw substantial increases in Qmax, while the fraction of residual urine volume (RU), prostate volume (PV) and ischemia were reduced. The observation group improved more significantly than the control group. The observation group was considerably lower than the control group (p < 0.05).
High selectivity α1-receptor blockers have good feasibility in the treatment of elderly BPH and combined with precise PAE can improve the treatment effect, with good safety and reliability.
Keywords
- precision prostatic artery embolization
- benign prostatic hyperplasia
- α-receptor blocker
- pathogenesis
- urinary symptom distress
The etiology of Benign Prostatic Hyperplasia (BPH) is intricate and a definitive
agreement has not been achieved. Modern studies have shown that the occurrence of
BPH is affected by adjacent organ lesions, physical and chemical factors,
immunological factors, pathogen infection and other factors [1]. Due to the deep
location of the prostate and the special structure of its lipid envelope, it has
special anatomical and physiological characteristics, which makes it difficult to
deliver drugs deep into the lesion and easy to relapse [2]. However,
The precision prostate artery embolization (PPAE) is performed under the guidance of digital subtraction angiography, which can achieve necrosis and atrophy of prostate tissue, thereby alleviating clinical symptoms caused by BPH [5]. Its clinical application is a minimally invasive treatment technology that can directly reach the lesion with a high absorption rate, obvious therapeutic effect, minimal trauma, low side effects, fast patient recovery and fewer complications which is especially suitable for elderly BPH patients who are not suitable for surgical treatment [6].
This research aimed to assess the effectiveness of PPAE in combination with silodosin for treating elderly individuals with benign prostatic hyperplasia (BPH), and to evaluate the clinical outcomes of different treatment approaches.
The current investigation used a retrospective study design to assess 144 senior individuals with elderly BPH who were diagnosed at the General Hospital of Huabei Petroleum Administration Bureau between January, 2021 and January, 2022.
The inclusion criteria of patients were (1) Age
The control group (64 patients) received
The efficacy evaluation criteria were determined as per the Guiding Principles
for Clinical Research of New Traditional Chinese Medicine: Markedly effective:
International Prognostic Scoring System (IPSS) score
All patients underwent IPSS and urinary symptom distress (BS) scores before and after treatment, with a total score of 0–35 for both IPSS and BS. As the score increases, the severity of the overall symptoms or urine distress also increases. Before and after treatment, ultrasound was used to measure RU and urinary flow rate was checked for Qmax, prostate volume and ischemic ratio. Follow up and observe the changes in various indicators at different times within 1 year after surgery.
The statistical assessment was done by SPSS 22.00 (IBM Corporation, Armonk, NY, USA). Count
data were reported as a percentage (%), while data was expressed as the Mean
The clinical information of all patients was summarized in Table 1. There was no
statistically significant difference in clinical information between the two
groups of patients (p
| Group | n | Age (year) | BMI (kg/m2) | Degree of proliferation (degree I/II/III) | Complicated diseases (hypertension/diabetes/hyperlipidemia) | Prostate volume (mL) | Course of disease (years) |
| Observation group | 80 | 68.22 |
22.23 |
40/28/12 | 16/12/14 | 76.22 |
7.18 |
| Control group | 64 | 68.11 |
22.89 |
36/20/8 | 12/8/12 | 76.03 |
7.23 |
| t or |
0.212 | 1.407 | 0.573 | 0.346 | 0.163 | 0.778 | |
| p-value | 0.832 | 0.162 | 0.751 | 0.951 | 0.870 | 0.438 |
All patients completed embolization without any serious complications during the
surgery. The embolization surgery time was 65.4
Table 2 presented a comparison of the overall effective rates between the two
groups. Following the administration of the therapy, the observation group
exhibited a total effective rate of 98.75%, while the control group exhibited a
total effective rate of 84.4% (p
| Group | Total (n) | Markedly effective (n) | Effective (n) | Invalid (n) | Total effective rate |
| Observation group | 80 | 72 | 7 | 1 | 79 (98.75%) |
| Control group | 64 | 41 | 13 | 10 | 54 (84.38%) |
| 3.885 | |||||
| p-value |
Table 3 illustrated a comparison of the changes in the IPSS and urinary symptom
distress (BS) ratings between the two groups before and after therapy. Following
therapy, both groups saw a substantial decrease in their IPSS and BS ratings
compared to before treatment (p
| IPSS | BS | ||||||||||
| Group | n | Before treatment | 2 weeks after treatment | 1 month after treatment | 6 months after treatment | 1 year after treatment | After treatment | 2 weeks after treatment | 1 month after treatment | 6 months after treatment | 1 year after treatment |
| Observation group | 80 | 21.49 |
14.29 |
10.51 |
6.03 |
3.29 |
22.77 |
13.98 |
7.84 |
3.92 |
0.98 |
| Control group | 64 | 22.88 |
18.49 |
15.51 |
9.32 |
5.86 |
22.19 |
17.02 |
10.03 |
5.27 |
1.48 |
| t | 2.230 | 5.181 | 6.742 | 9.392 | 12.160 | 0.685 | 3.515 | 2.400 | 2.010 | 5.128 | |
| p | 0.027 | 0.495 | 0.0006 | 0.018 | 0.046 | ||||||
Compared to before treatment, *p
Table 4 presented a comparison of the changes in RU and Qmax before and
after therapy in the two groups. Both groups exhibited a noteworthy rise in
Qmax and a notable decrease in RU at various time points after the therapy
(p
| RU (mL) | Qmax (mL/sec) | ||||||||||
| Group | n | Before treatment | 2 weeks after treatment | 1 month after treatment | 6 months after treatment | 1 year after treatment | After treatment | 2 weeks after treatment | 1 month after treatment | 6 months after treatment | 1 year after treatment |
| Observation group | 80 | 36.44 |
22.19 |
17.53 |
15.45 |
12.93 |
9.78 |
13.39 |
15.12 |
18.58 |
20.51 |
| Control group | 64 | 36.10 |
27.44 |
21.68 |
18.08 |
20.92 |
9.89 |
12.48 |
13.93 |
16.29 |
17.77 |
| t | 0.259 | 6.102 | 5.380 | 3.464 | 14.000 | 0.476 | 2.518 | 3.031 | 4.485 | 5.129 | |
| p | 0.796 | 0.000 | 0.000 | 0.000 | 0.000 | 0.635 | 0.013 | 0.003 | 0.000 | 0.000 | |
Compared to before treatment, *p
Table 5 illustrated a comparison of prostate volume (PV) and ischemia ratio
between the two groups before and after therapy. At the 2 week, 1 month, 6 month
and 1 year follow-up intervals after treatment, there was a substantial reduction
in the proportion of ischemia and PV in both groups compared to before treatment.
Furthermore, the observation group exhibited a considerably greater drop than the
control group (p
| PV (mL) | Ischemic ratio (%) | ||||||||||
| Group | n | Before treatment | 2 weeks after treatment | 1 month after treatment | 6 months after treatment | 1 year after treatment | After treatment (%) | 2 weeks after treatment (%) | 1 month after treatment (%) | 6 months after treatment (%) | 1 year after treatment (%) |
| Observation group | 80 | 116.23 |
93.47 |
80.52 |
73.10 |
70.53 |
50.53 |
41.90 |
40.90 |
38.89 |
35.23 |
| Control group | 64 | 114.27 |
99.01 |
93.19 |
88.26 |
80.17 |
52.34 |
46.24 |
44.45 |
43.89 |
38.53 |
| t | 0.633 | 1.917 | 4.729 | 6.863 | 4.613 | 1.107 | 2.321 | 2.354 | 2.847 | 2.343 | |
| p | 0.528 | 0.057 | 0.000 | 0.000 | 0.000 | 0.270 | 0.022 | 0.020 | 0.005 | 0.021 | |
Compared to before treatment, *p
This study specifically states that the duration of treatment in two groups was
4 weeks. In the observation group, there was no recurrence within 1 month after
treatment. However, 1 case had a recurrence within 3 months, 3 cases experienced
a recurrence within 6 months and 5 cases experienced a recurrence within 12
months. In the control group, there were 10 cases of recurrence within 1 month
after treatment, 13 cases within 3 months and 23 cases within 12 months.
Recurrent patients were followed up with the study group’s treatment method and
the treatment effect was the same in the study group. All patients in this study
did not experience serious complications, only mild complications such as low
fever, burning sensation at the urethral opening, hematospermia, transient
hematuria and mild pain in the pubic region. The incidence rate in the
observation group was much lower than that in the control group and that
variation was statistically noteworthy (p
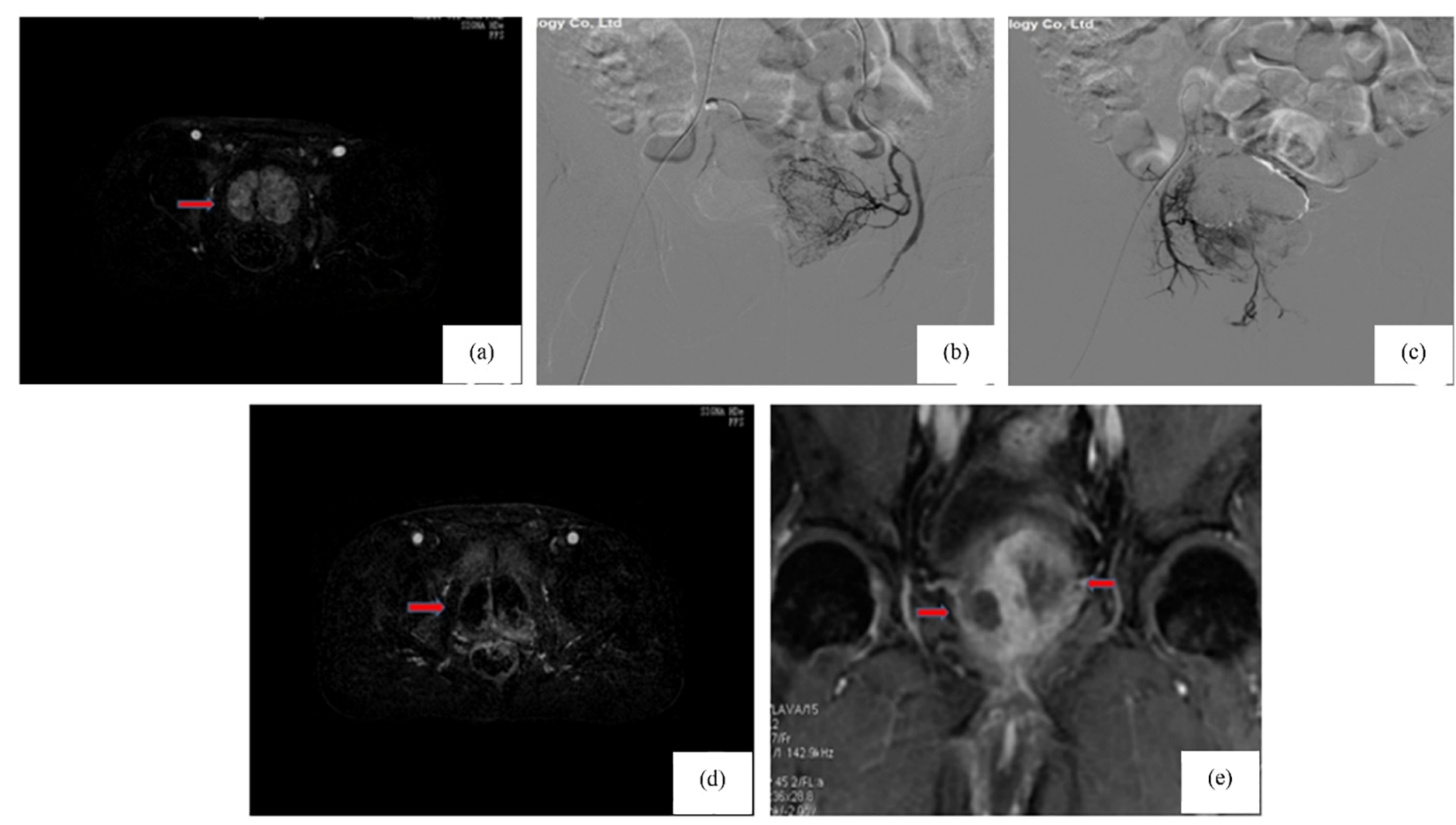 Fig. 1.
Fig. 1.
Changes in the prostate gland’s magnetic resonance imaging before and after treatment in the observation group. (a) Preoperative MRI shows prostate enlargement with marked heterogeneous enhancement (arrow); (b) Left prostatic artery; (c) Right prostatic artery; (d) Day 7 post-op: reduced prostate volume and diminished enhancement (arrow), indicating early ischemic necrosis. (e) One year post-op: further shrinkage and patchy non-enhancing areas in the central lobe (arrow), consistent with ischemic necrosis.
Pre-operative enhanced magnetic resonance imaging of the prostate shows (Fig. 1a) approximately 7.2
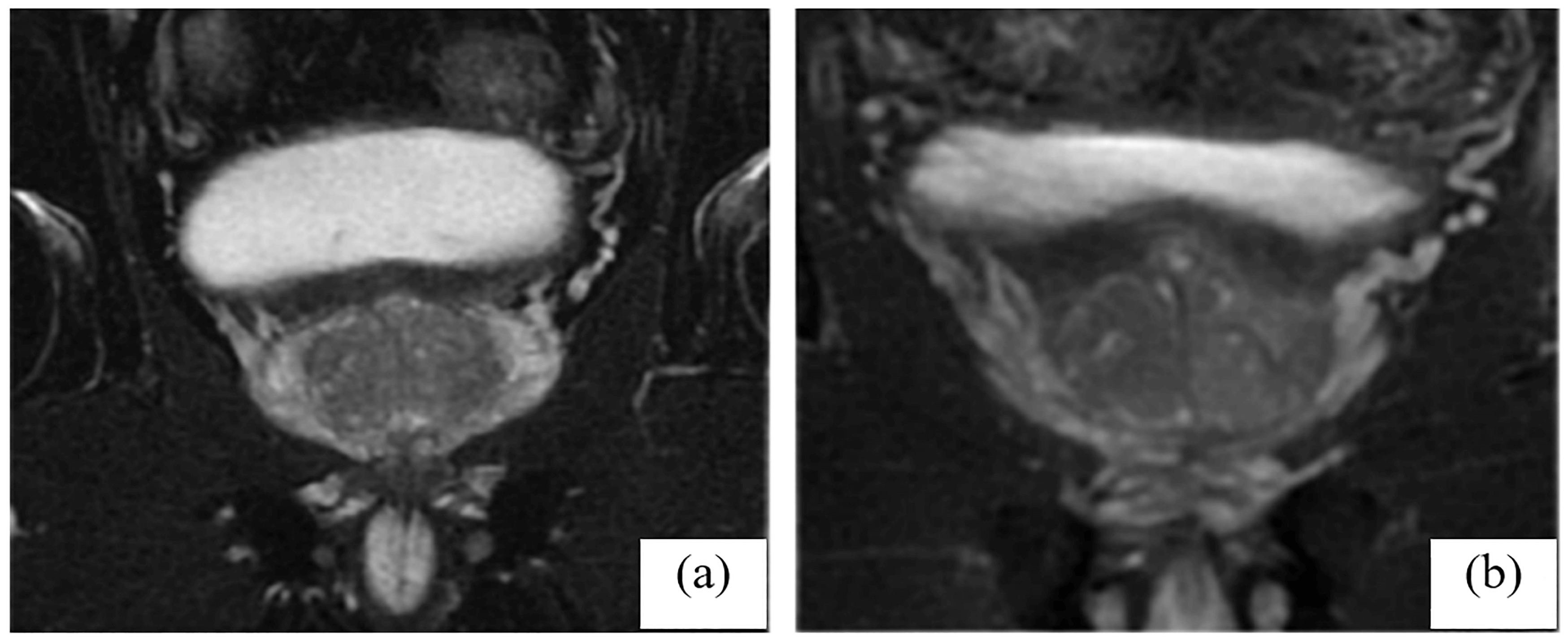 Fig. 2.
Fig. 2.
Dimensions of the prostate’s magnetic resonance imaging before and after treatment in the observation group. (a) Prostate’s dimensions before therapy and (b) Prostate’s dimensions and an uneven signal in the central lobe after therapy.
The research found that the observation group had a considerably greater
effective rate compared to the control group. After therapy, both groups showed a
substantial decrease in their IPSS and BS levels compared to prior therapy.
Additionally, the observation group had lower scores than the control group. The
occurrence of negative responses and complications in the observation group was
drastically reduced compared to the control group. This study demonstrated that
following therapy, there was a significant increase in the Qmax and a
significant decrease in the resistance to RU in both groups (p
Finally, follow-up revealed no recurrence in the observation group. Then 1 month
after treatment, 1 case recurred in 3 months, 3 cases recurred in 6 months and 5
cases recurred in 12 months. In the control group, 10 cases recurred 1 month
after treatment, 13 cases recurred 3 months after treatment and 23 cases recurred
12 months after treatment. Patients with recurrence were treated with follow-up
treatment in the study group and the treatment effect was the same in the study
group. All patients in this study had no serious complications, only mild
complications such as low-grade fever, burning sensation at the urethral orifice,
blood in the urine, transient hematuria, mild pain in the pubic region and so on.
The occurrence rate in the observation group was considerably reduced compared to
the control group and the imaging results of the observation group indicated a
favourable prognosis before, during and after follow-up. This further illustrates
that precise prostatic artery embolization combined with high selectivity
The BPH is more prevalent in older men and its incidence has been increasing in recent years as the population gets older. The purpose of BPH treatment is to prevent and delay the progression of hyperplasia to alleviate symptoms and improve quality of life [7]. However, as organs age and various physiological functions deteriorate, the tolerance of many patients to surgery is significantly reduced. The BPH is often accompanied by increased blood supply to the prostate, which provides an important theoretical basis for the treatment of precise prostatic artery embolization [8].
Silodosin for
Increased blood supply is the basic condition of BPH and the arterial source of
the prostate is abundant [18]. Under the condition of cutting off the blood
supply and nutrition of the tumor, the local tumor will atrophy or necrosis,
which provides a theoretical basis for embolization treatment. Silodosin is a
prostate
Overall, this study demonstrates that precise prostatic artery embolization
combined with highly selective
This study demonstrates that precise prostatic artery embolization combined with
highly selective
The datasets used or analyzed during the current study are available from the corresponding author on reasonable request.
QW and HZ designed and supervised the research and WH drafted the initial version of the article. KY, JZ and JL examined unprocessed data. YB, LZ, FG, WH, JC and FL conducted statistical and bioinformatics analysis. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The Ethics Committee of the General Hospital of Huabei Petroleum Administration Bureau is approved the probe (Reg No: 2023/BPH/345). Informed consent was obtained from all participants prior to enrollment. This manuscript describes a clinical intervention involving human subjects and was conducted in full accordance with the ethical principles set forth in the Declaration of Helsinki.
The authors appreciate the amenities provided by the institution.
The research was funded by Medical Science Research Project Plan of Hebei Provincial Health Commission (20212736).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.