


 , Burak Yüksel 1, Uğur Aygün 1
, Burak Yüksel 1, Uğur Aygün 11 Department of Cardiovascular Surgery, Trabzon Ahi Evren Thoracic and Cardiovascular Surgery Training and Research Hospital, 61040 Trabzon, Turkey
Abstract
This study aimed to evaluate the long-term clinical and echocardiographic outcomes of Perceval sutureless aortic valve implantation, with particular emphasis on survival, valve-related events, and hemodynamic performance during extended follow-up.
This retrospective single-center study included 150 consecutive patients aged 70–85 years who underwent Perceval sutureless aortic valve replacement between 2016 and 2025. Of these, 106 patients (70.7%) underwent isolated aortic valve replacement, while 44 (29.3%) underwent additional cardiac procedures. Clinical and echocardiographic data were collected preoperatively, at hospital discharge, and during scheduled long-term follow-up. Overall survival was estimated using Kaplan-Meier analysis.
Thirty-day mortality occurred in 5 patients (3.3%), and five patients (3.3%) required permanent pacemaker implantation. Dialysis-requiring acute kidney injury occurred in three patients (2.0%), and stroke or transient ischemic attack occurred in two patients (1.3%). During long-term follow-up (mean 6.1 ± 1.8 years), three patients (2.0%) required valve-related reintervention, primarily due to technical issues or early prosthetic dysfunction.One patient (0.7%) developed moderate-to-severe transvalvular regurgitation during follow-up. The estimated survival rates from the Kaplan–Meier analysis were 90.0% at 1 year, 78.7% at 5 years, and 71.3% at 8 years. The mean transvalvular gradient decreased from 46 ± 11 mmHg preoperatively to 9.8 ± 3.2 mmHg at discharge and remained stable at 11.2 ± 3.9 mmHg at the last follow-up.
Perceval sutureless aortic valve implantation demonstrated favorable early clinical outcomes and sustained good hemodynamic performance during long-term follow-up. The low incidence of valve-related reintervention and the absence of structural valve deterioration indicate that this prosthesis is durable and clinically feasible for carefully selected older patients.
Keywords
- aortic valve stenosis
- aortic valve replacement
- bioprosthesis
- heart valve prosthesis implantation
- hemodynamics
- treatment outcome
Severe aortic stenosis is one of the most common valvular heart diseases in the aging population and is associated with significant morbidity and mortality if left untreated. Progressive valve calcification leads to obstruction of the left ventricular outflow tract, increased transvalvular gradients, and eventual deterioration of cardiac function. Surgical aortic valve replacement (SAVR) remains an established treatment strategy for patients with symptomatic severe aortic stenosis who are suitable surgical candidates, particularly in elderly individuals with acceptable operative risk profiles. Recent international guidelines emphasize individualized treatment strategies that incorporate both surgical and transcatheter approaches according to patient characteristics, comorbidities, and anatomical suitability [1].
Despite the favorable clinical performance of conventional sutured bioprosthetic valves, longer cardiopulmonary bypass and aortic cross-clamp times may increase perioperative risk, especially in elderly patients and in those undergoing concomitant cardiac procedures. To address these limitations, sutureless aortic valve prostheses were developed to simplify valve implantation and reduce operative times while maintaining effective hemodynamic performance. Among these devices, the Perceval sutureless valve has gained increasing clinical acceptance due to its simplified deployment and reproducible implantation technique [2,3].
Early and mid-term studies evaluating the Perceval valve have demonstrated promising clinical outcomes, including reduced procedural times and satisfactory postoperative hemodynamic performance [4,5]. Multicenter prospective trials and observational studies have reported low early mortality rates and stable transvalvular gradients during follow-up periods extending up to five to seven years [5,6]. In addition, meta-analyses comparing sutureless and conventional bioprosthetic valves have suggested comparable safety profiles, with potential procedural advantages associated with sutureless technology [7].
However, despite the growing clinical adoption of sutureless aortic valve prostheses, long-term outcome data beyond midterm follow-up remain relatively limited, particularly from single-center studies that reflect routine clinical practice. Additional long-term observational data are therefore needed to better define the durability, survival outcomes, and valve-related performance of sutureless prostheses over extended follow-up periods.
Accordingly, the present study aimed to evaluate the long-term clinical and echocardiographic outcomes of Perceval sutureless aortic valve implantation in a consecutive single-center cohort, with particular emphasis on survival, valve-related events, and long-term hemodynamic performance during follow-up extending up to eight years.
This retrospective single-center study included 150 consecutive patients aged 70–85 years who underwent Perceval sutureless aortic valve replacement between January 2016 and December 2025. Both isolated and combined cardiac procedures were included without restriction regarding urgency or redo status.
Clinical, procedural, and outcome data were retrieved from institutional electronic medical records and surgical databases. Baseline demographic and clinical characteristics were recorded for all patients. Follow-up data were obtained through scheduled outpatient visits and, when necessary, structured telephone interviews. Approximately 13% of patients were lost to structured follow-up during the study period.
All procedures were performed through median sternotomy using standard cardiopulmonary bypass with mild systemic hypothermia. After excision of the native aortic valve, extensive annular decalcification was performed to ensure optimal seating of the prosthesis.
Valve sizing was conducted according to manufacturer recommendations. The Perceval sutureless prosthesis was deployed using standard positioning and balloon expansion techniques. Concomitant cardiac procedures were performed as clinically indicated.
Transthoracic echocardiography (TTE) was performed preoperatively, at hospital discharge, and during long-term follow-up in accordance with routine institutional protocols. Mean transvalvular gradient and effective orifice area were measured in accordance with current echocardiographic recommendations. The severity of transvalvular and paravalvular regurgitation was graded as none/trace, mild, moderate, or severe using Doppler echocardiographic criteria. Structural valve deterioration (SVD) was defined according to contemporary consensus criteria as intrinsic, permanent structural changes of the prosthetic valve leading to degeneration, stenosis, or regurgitation. Hemodynamic SVD was considered when an increase in mean transvalvular gradient ≥10 mmHg from baseline or the development of new moderate or severe transvalvular regurgitation was observed during follow-up, in accordance with established consensus definitions.
Early outcomes included 30-day mortality, permanent pacemaker implantation, dialysis-requiring acute kidney injury, stroke or transient ischemic attack, major bleeding, re-exploration for bleeding, and prolonged mechanical ventilation. Long-term outcomes included valve-related reintervention, prosthetic valve dysfunction, and survival. Valve-related reintervention was defined as any repeat surgical or transcatheter procedure performed due to technical complications or prosthetic valve dysfunction. Valve-related mortality was defined as death directly attributable to valve dysfunction or valve-related complications. Clinical and echocardiographic follow-up assessments were performed at hospital discharge, at 6 months postoperatively, and annually thereafter. Long-term follow-up was defined as clinical and echocardiographic assessment performed more than 12 months after surgery. The mean follow-up duration was 6.1 ± 1.8 years.
Continuous variables are presented as mean ± standard deviation, whereas categorical variables are presented as number (percentage). Overall survival was estimated using the Kaplan–Meier method, with patients censored at the date of last available follow-up if death had not occurred. Time-to-event outcomes were described when applicable. Missing data were not imputed due to the retrospective observational design. Given the limited proportion of missing data, descriptive analysis was considered appropriate without formal imputation. Subgroup analyses were descriptive, and no formal statistical comparisons were performed due to the limited sample size.
A total of 150 consecutive patients underwent Perceval sutureless aortic valve implantation during the study period. Baseline clinical characteristics of the study population are summarized in Table 1. The mean age of the study population was 75 ± 3.8 years, with 95 patients (63.3%) aged ≥75 years. Male patients accounted for 60% of the cohort. Hypertension and diabetes mellitus were present in 73% and 43% of patients, respectively. Reduced left ventricular ejection fraction (≤35%) was observed in 25 patients (16.7%).
Isolated aortic valve replacement was performed in 106 patients (70.7%), while 44 patients (29.3%) underwent concomitant cardiac procedures. Redo cardiac surgery was required in 9 patients (6.0%), and urgent surgery was performed in 4 patients (2.7%).
| Variable | Value, n (%) or mean ± SD |
|---|---|
| Age (years) | 75 ± 3.8 |
| Age ≥75 years | 95 (63.3) |
| Age <75 years | 55 (36.7) |
| Male sex | 90 (60.0) |
| Body mass index (kg/m2) | 27.8 ± 4.1 |
| Hypertension | 110 (73.3) |
| Diabetes mellitus | 65 (43.3) |
| Chronic kidney disease | 18 (12.0) |
| Chronic obstructive pulmonary disease | 22 (14.7) |
| Previous myocardial infarction | 30 (20.0) |
| Atrial fibrillation (preoperative) | 28 (18.7) |
| Left ventricular ejection fraction ≤35% | 25 (16.7) |
| Urgent surgery | 4 (2.7) |
| Redo cardiac surgery | 9 (6.0) |
| Combined procedures | 44 (29.3) |
Continuous variables are presented as mean ± standard deviation (SD) where applicable. Categorical variables are presented as number and percentage.
Early operative and postoperative outcomes are summarized in Table 2. The overall 30-day mortality was 3.3% (5/150). Permanent pacemaker implantation was required in 5 patients (3.3%). Dialysis-requiring acute kidney injury occurred in 3 patients (2.0%), and stroke or transient ischemic attack occurred in 2 patients (1.3%). Major bleeding occurred in 5 patients (3.3%), of whom 3 patients (2.0%) required surgical re-exploration. Prolonged mechanical ventilation was required in 5 patients (3.3%). Early adverse events were observed in patients undergoing both isolated and concomitant cardiac procedures. These observations are presented descriptively, and no formal statistical comparison was performed between groups. Technical issues were identified in two patients, including intraoperative valve malposition and prosthesis sizing mismatch requiring valve repositioning. In addition, one early prosthetic failure occurred due to clinically significant paravalvular leakage requiring early surgical reintervention.
| Outcome | Value, n (%) |
|---|---|
| 30-day mortality | 5 (3.3) |
| 30-day mortality in patients ≥75 years | 3 (3.2) |
| 30-day mortality in patients <75 years | 2 (3.6) |
| Permanent pacemaker implantation | 5 (3.3) |
| Major bleeding | 5 (3.3) |
| Re-exploration for bleeding | 3 (2.0) |
| Dialysis-requiring acute kidney injury | 3 (2.0) |
| Stroke/transient ischemic attack | 2 (1.3) |
| Prolonged mechanical ventilation | 5 (3.3) |
Data presented as numbers (percentages). Major bleeding was defined as bleeding requiring ≥2 units of red blood cell transfusion and/or surgical re-exploration. All outcomes represent events occurring within 30 days after surgery.
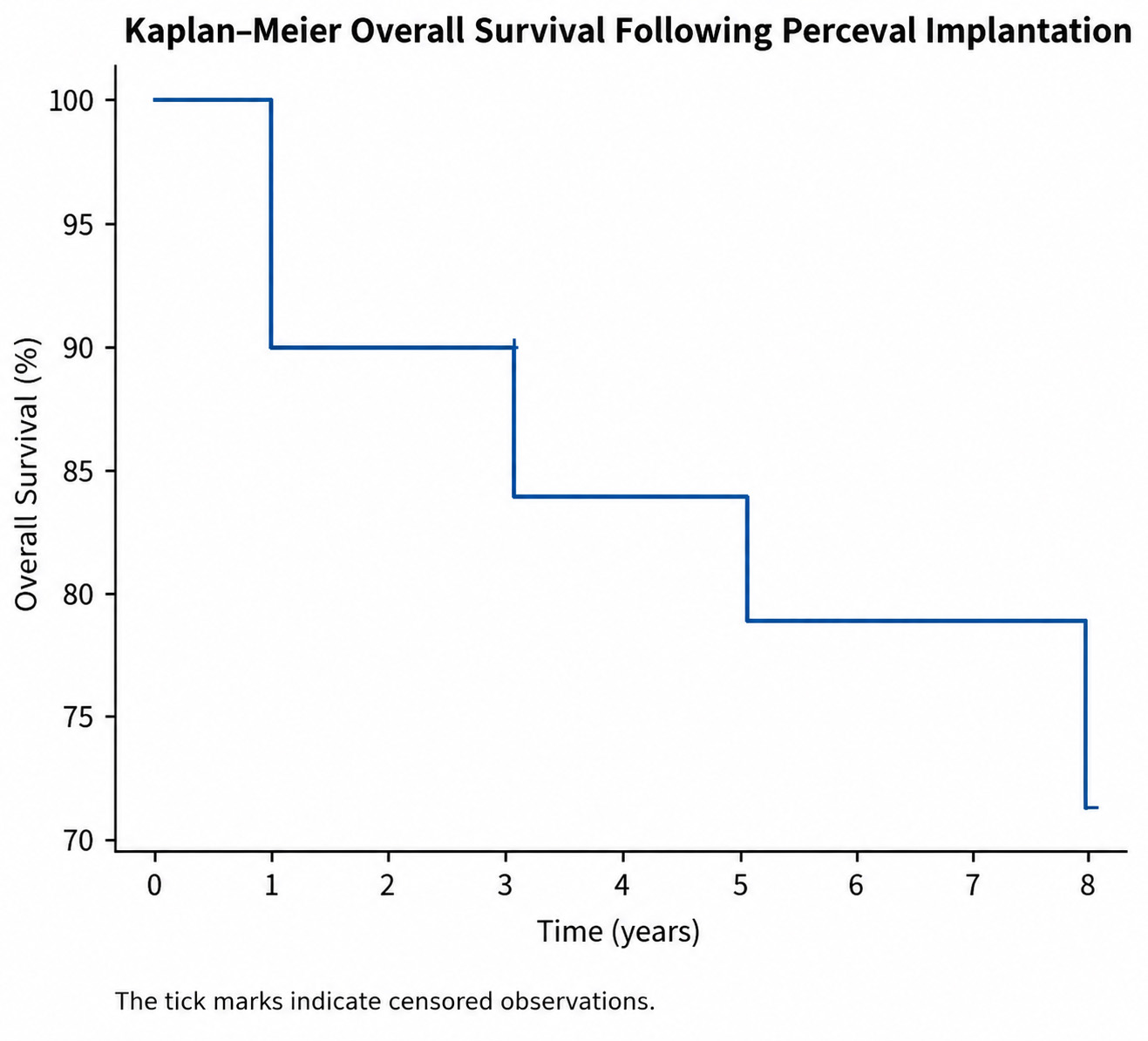
The mean follow-up duration was 6.1 ± 1.8 years, with a median follow-up of 6.3 years (interquartile range: 4.8–7.6 years). Approximately 13% of patients were lost to structured follow-up. During long-term follow-up, three patients (2.0%) underwent valve-related reintervention. Two cases were associated with intraoperative technical issues during the index procedure. The first case involved valve malpositioning and repositioning under a second cross-clamp, while the second case involved a prosthesis sizing mismatch and intraoperative repositioning. The third case occurred during the early postoperative period due to clinically significant paravalvular leakage requiring surgical reintervention. No cases of valve thrombosis were observed during follow-up. Importantly, no structural valve deterioration was detected during the long-term observation period. Kaplan–Meier survival analysis demonstrated estimated overall survival rates of 90.0% at 1 year, 78.7% at 5 years, and 71.3% at 8 years (Fig. 1).
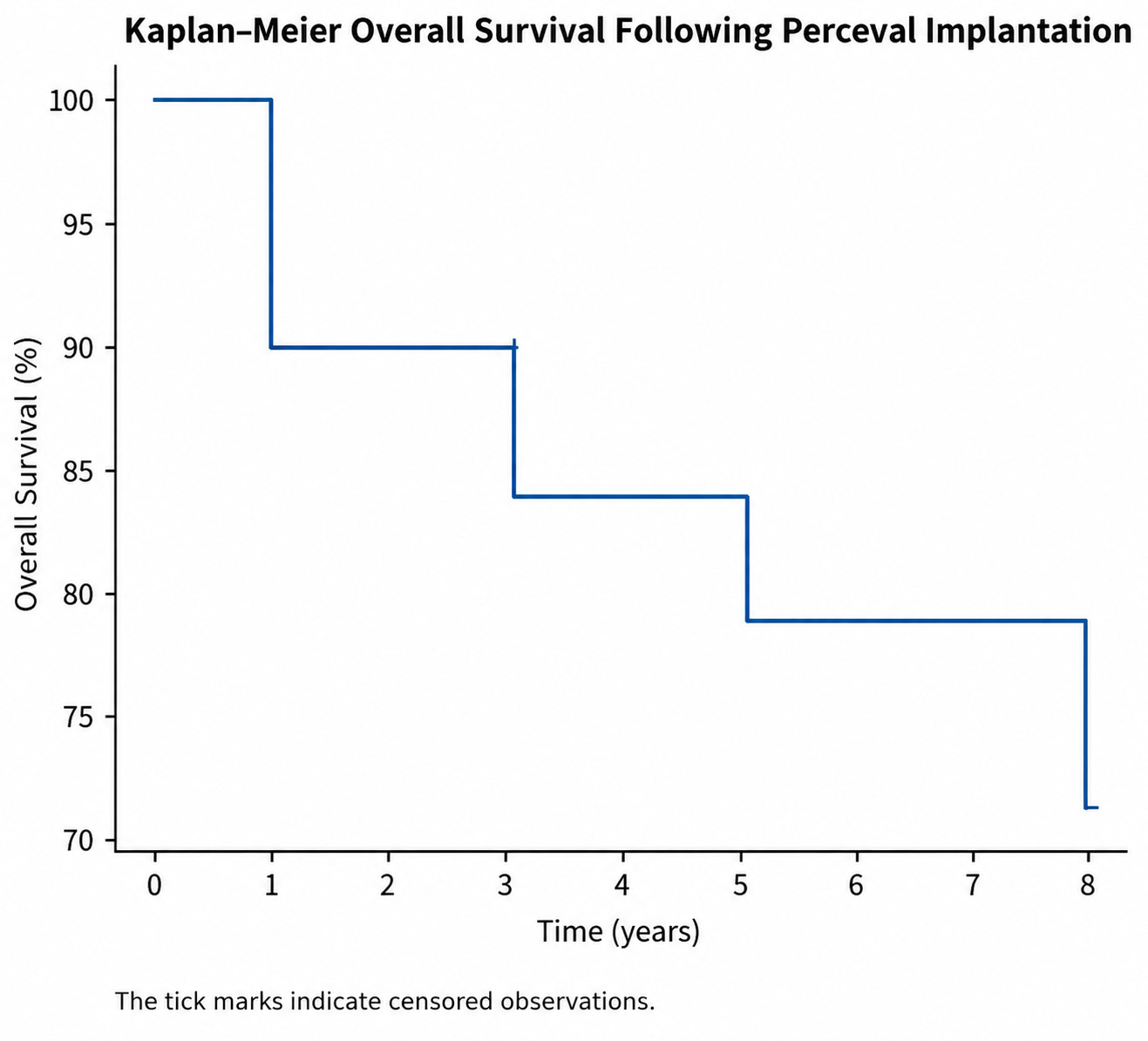 Fig. 1.
Fig. 1.Kaplan–Meier overall survival following perceval sutureless aortic valve replacement. Kaplan–Meier analysis demonstrating overall survival up to 8 years after Perceval implantation in a consecutive single-center cohort of 150 patients. Estimated overall survival rates were 90.0% at 1 year, 84.0% at 3 years, 78.7% at 5 years, and 71.3% at 8 years. Tick marks indicate censored observations. Median survival was not reached during follow-up because estimated survival remained above 50% throughout the observation period. Patients who were alive at the last available follow-up were censored at the date of their most recent clinical assessment.
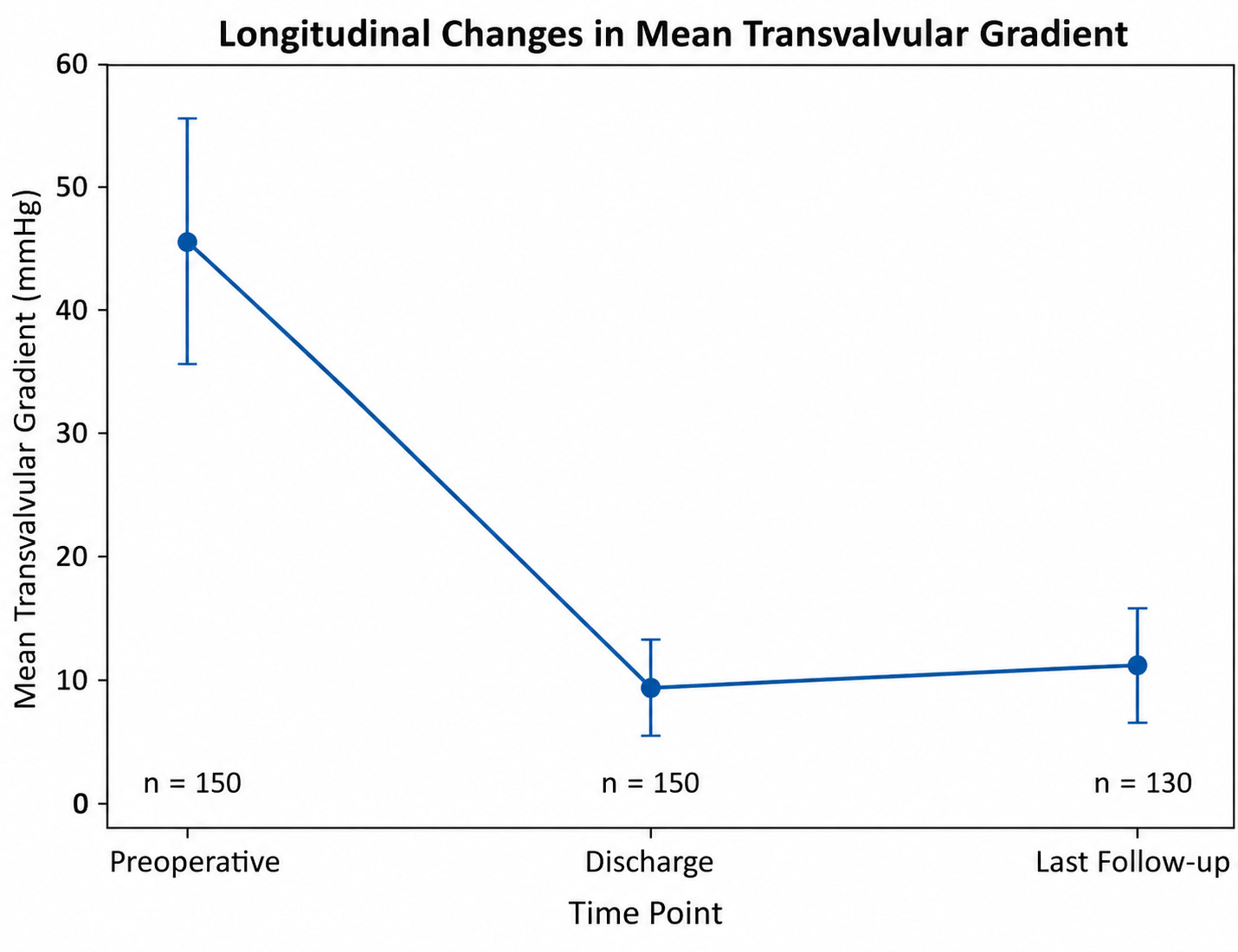
Long-term echocardiographic outcomes are summarized in Table 3. The mean transvalvular gradient decreased significantly from 46 ± 11 mmHg preoperatively to 9.8 ± 3.2 mmHg at discharge and remained stable at 11.2 ± 3.9 mmHg at the last follow-up (Fig. 2).
| Variable | Value, mean ± SD or n (%) |
|---|---|
| Mean transvalvular gradient (mmHg)–discharge | 9.8 ± 3.2 |
| Mean transvalvular gradient (mmHg)–last follow-up | 11.2 ± 3.9 |
| Effective orifice area (cm2)–discharge | 1.8 ± 0.3 |
| Effective orifice area (cm2)–last follow-up | 1.7 ± 0.3 |
| Mild transvalvular aortic regurgitation | 9 (6.0) |
| Moderate/severe transvalvular regurgitation | 1 (0.7) |
| Mild paravalvular regurgitation | 9 (6.0) |
| Moderate/severe paravalvular regurgitation | 1 (0.7) |
| Valve-related reintervention | 3 (2.0) |
Continuous variables are presented as mean ± standard deviation. Clinically significant paravalvular regurgitation refers to moderate or severe regurgitation. Late follow-up values correspond to the last available echocardiographic assessment during long-term follow-up.
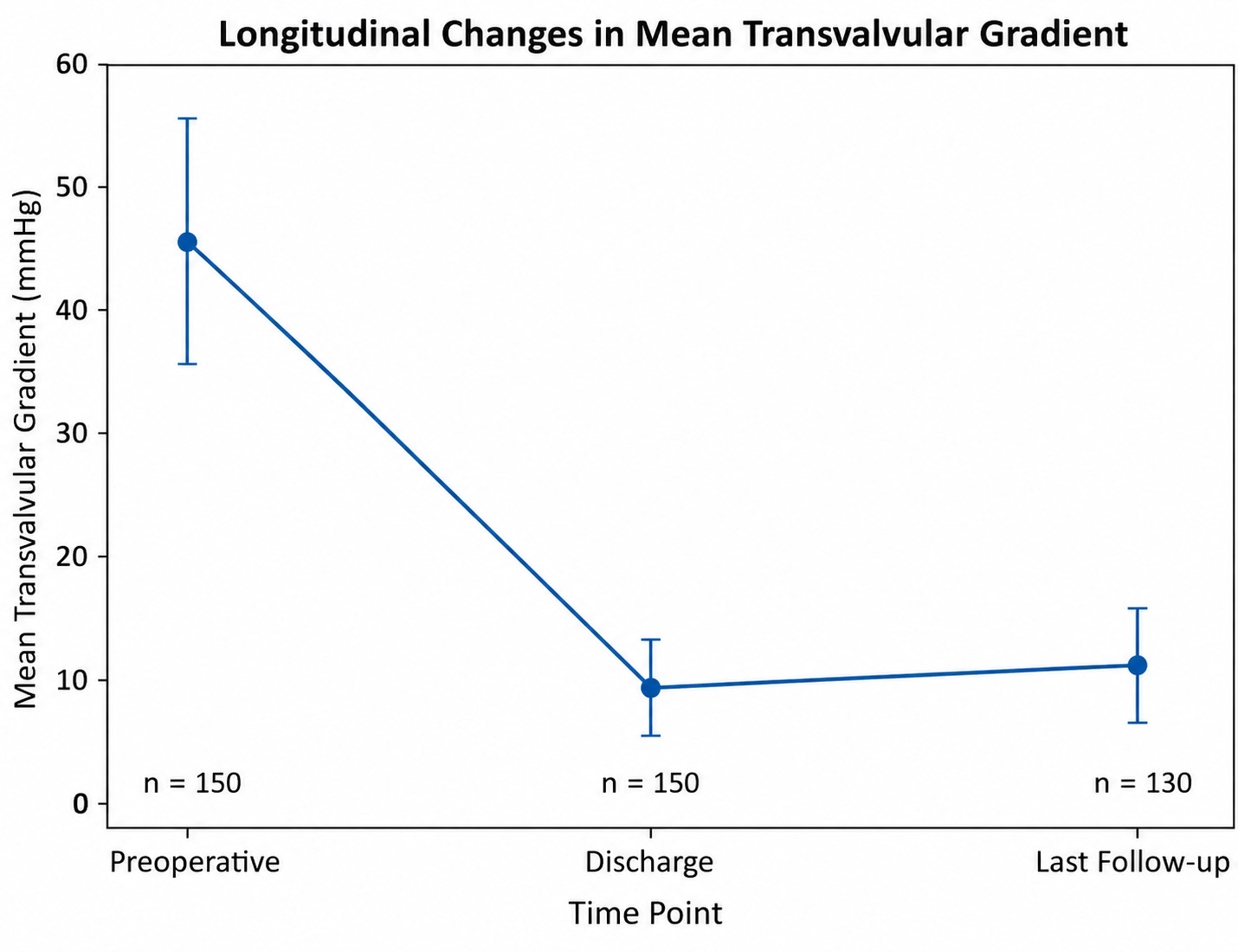 Fig. 2.
Fig. 2.Longitudinal changes in mean transvalvular gradient following Perceval sutureless aortic valve implantation. Mean transvalvular gradient decreased markedly after surgery and remained stable during follow-up. Mean gradient values decreased from 46 ± 11 mmHg preoperatively to 9.8 ± 3.2 mmHg at discharge and remained stable at 11.2 ± 3.9 mmHg at last follow-up. Error bars represent standard deviation. Numbers below the x-axis indicate the number of patients with available echocardiographic assessment at each time point.
The effective orifice area remained stable following implantation, measuring 1.8 ± 0.3 cm2 at discharge and 1.7 ± 0.3 cm2 at the last follow-up.
Mild transvalvular aortic regurgitation was observed in 9 patients (6.0%), whereas moderate-to-severe transvalvular regurgitation was detected in 1 patient (0.7%). Mild paravalvular regurgitation occurred in 9 patients (6.0%), while moderate-to-severe paravalvular regurgitation was observed in 1 patient (0.7%).
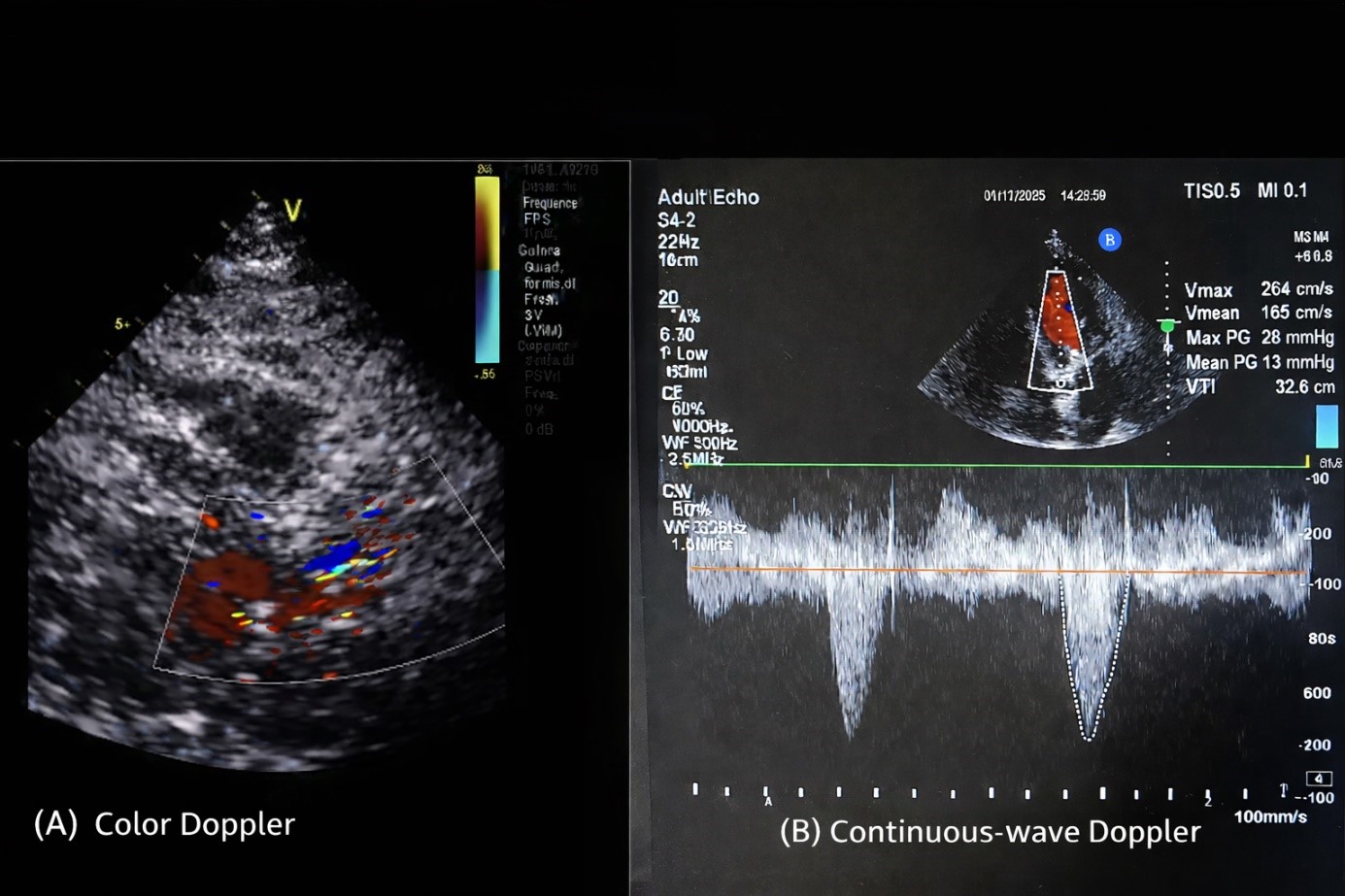
Representative Doppler echocardiographic findings demonstrating preserved prosthetic valve function are shown in Fig. 3.
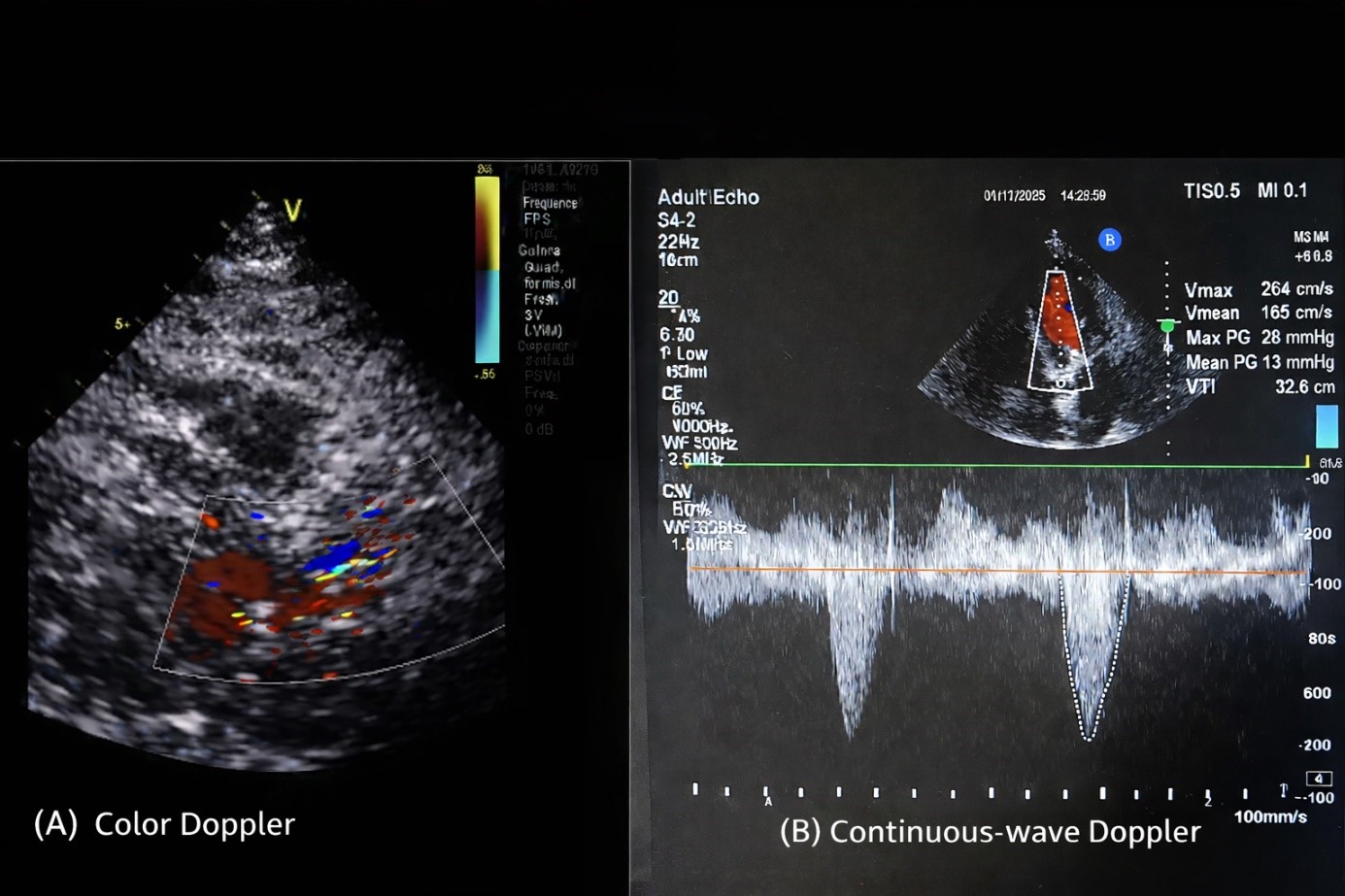 Fig. 3.
Fig. 3.Representative echocardiographic assessment of the Perceval prosthesis during follow-up. (A) Color Doppler imaging demonstrating laminar transvalvular flow without clinically significant paravalvular regurgitation. (B) Continuous-wave Doppler interrogation demonstrating low transvalvular velocities and a low mean gradient consistent with preserved prosthetic valve hemodynamic performance.
The present study demonstrates favorable early clinical outcomes and sustained long-term hemodynamic performance following Perceval sutureless aortic valve implantation in a consecutive single-center cohort with follow-up extending up to eight years. The principal findings of this study include stable transvalvular gradients over time, a low incidence of permanent pacemaker implantation, a limited number of valve-related reinterventions, and absence of structural valve deterioration during long-term follow-up.
Previous multicenter and observational studies evaluating the Perceval valve have reported encouraging early and midterm results, including reduced operative times and satisfactory hemodynamic performance. Long-term observational data have shown sustained gradient stability and acceptable durability profiles over extended follow-up periods [8]. The findings of the present study are consistent with these previous reports, demonstrating that mean transvalvular gradients remained low following implantation and stable throughout long-term observation. Preservation of favorable hemodynamic performance is particularly important in elderly populations, in whom progressive prosthetic dysfunction may negatively influence long-term functional status and survival.
Conduction disturbances remain an important concern following sutureless valve implantation. Reported permanent pacemaker implantation rates following sutureless aortic valve replacement typically range between 5% and 10%, particularly during the early learning phase of device adoption [9,10]. In the present study, permanent pacemaker implantation was required in 3.3% of patients, a lower rate than reported in the literature. This relatively low rate may reflect careful annular decalcification, appropriate prosthesis sizing, and growing institutional experience with the implantation technique.
Valve-related reintervention remains a critical measure of procedural durability. In the present series, valve-related reintervention occurred in 2.0% of patients and was primarily related to intraoperative technical factors or early prosthetic dysfunction rather than late structural valve deterioration. This distinction is clinically important, as early procedural complications should not be interpreted as intrinsic valve degeneration. The definition of SVD is well established in contemporary literature [11]. By definition, the absence of late SVD observed in the present series supports the durability of the Perceval prosthesis during long-term follow-up.
With the current results placed in the context of durability data from conventional bioprosthetic valves, long-term structural performance appears acceptable [12]. Although direct comparison between sutureless and conventional prostheses was not the objective of the present study, previously published learning-curve and procedural-experience studies have emphasized the importance of technical refinement for achieving optimal clinical outcomes [13,14]. Early valve-related reinterventions in the present cohort were primarily associated with technical factors rather than intrinsic prosthetic degeneration. In addition to the stable performance of the Perceval valve, overall long-term patient survival remained within acceptable limits. Kaplan–Meier survival estimates were 90.0% at 1 year, 78.7% at 5 years, and 71.3% at 8 years. These survival outcomes are consistent with previously reported systematic reviews and meta-analyses evaluating outcomes after sutureless or rapid-deployment valve implantation [15]. Importantly, survival outcomes in elderly surgical populations are strongly influenced by baseline comorbidities and concomitant procedures rather than valve-related performance alone.
An additional important observation from the present study is the acceptable early clinical outcome profile observed in elderly patients undergoing isolated procedures. In the subgroup of patients aged ≥75 years, early mortality remained low, particularly among those undergoing isolated aortic valve replacement. The only death observed in this subgroup undergoing isolated surgery was associated with postoperative respiratory failure in a patient with pre-existing chronic obstructive pulmonary disease rather than valve-related complications. These findings are consistent with contemporary guideline recommendations emphasizing individualized treatment selection in elderly patients.
From a broader clinical perspective, the role of sutureless aortic valve implantation continues to evolve within the modern treatment landscape of aortic stenosis. While transcatheter aortic valve implantation (TAVI) has gained widespread acceptance in elderly and high-risk patients, surgical valve replacement—including sutureless techniques—remains an important therapeutic option in patients requiring concomitant procedures or those with anatomical characteristics unsuitable for transcatheter approaches. These findings are consistent with current guideline recommendations emphasizing individualized valve selection strategies based on patient characteristics and procedural considerations.
Overall, the findings of this study reinforce the clinical feasibility and durability of Perceval sutureless aortic valve implantation during extended follow-up. The stability of hemodynamic performance, combined with low rates of valve-related reintervention and absence of structural valve deterioration, supports the long-term reliability of this prosthesis in routine surgical practice.
This study has several limitations that should be acknowledged. First, the retrospective single-center design may limit the generalizability of the findings to broader patient populations. Second, approximately 13% of patients were lost to structured follow-up, limiting the detection of late adverse events. Third, echocardiographic assessments were performed as part of routine clinical practice and were not independently evaluated by a centralized core laboratory. In addition, the absence of a contemporary control group prevented direct comparison with conventional sutured bioprosthetic valves. Finally, standardized surgical risk scores such as EuroSCORE II were not consistently available due to the retrospective nature of the study and therefore could not be included in the analysis.
Perceval sutureless aortic valve implantation demonstrated favorable early clinical outcomes and sustained long-term hemodynamic performance in this single-center cohort with follow-up extending up to eight years. The observed stability of transvalvular gradients, low incidence of permanent pacemaker implantation, and limited number of valve-related reinterventions support the procedural reliability of this technique. Importantly, no structural valve deterioration was detected during long-term follow-up, suggesting acceptable durability of the prosthesis in appropriately selected patients. Overall, these findings support the role of Perceval sutureless aortic valve implantation as a safe and effective surgical option in elderly patients and in those requiring simplified implantation strategies. Further multicenter studies with extended follow-up durations are warranted to confirm the long-term durability and broader clinical applicability of this technology.
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request, in accordance with the journal’s editorial policies.
EK: Study conception and design, data acquisition, analysis and interpretation, manuscript drafting, and final approval. BY: Data acquisition, critical revision of the manuscript, and final approval. UA: Data acquisition, analysis and interpretation, critical revision of the manuscript for important intellectual content, and final approval of the submitted version. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The research has been conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval for this study, which is a retrospective analysis of previously collected clinical data, has been granted by the institutional ethics committee of Trabzon Ahi Evren Thoracic and Cardiovascular Surgery Training and Research Hospital (approval number: 205; date: 02/02/2026). The requirement for written informed consent was waived by the Ethics Committee because of the retrospective nature of the study. The study was based on the review of existing medical records, did not influence patient management, involved minimal risk to participants, and all data were analyzed anonymously.
Not applicable.
This research received no external funding.
The authors declare no conflicts of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.