

 , Cenyuan Dong 1,2, Mengpan Liu 1,2, Qin Qin 1,2, Lin Teng 1,3,*
, Cenyuan Dong 1,2, Mengpan Liu 1,2, Qin Qin 1,2, Lin Teng 1,3,*
1 Department of Cardiology, Yichang Central People’s Hospital/The First Clinical Medical College, Three Gorges University, 443003 Yichang, Hubei, China
2 School of Basic Medicine, China Three Gorges University, 443000 Yichang, Hubei, China
3 Institute of Cardiovascular Diseases, Three Gorges University, 443003 Yichang, Hubei, China
Abstract
Patent ductus arteriosus (PDA) is a congenital cardiovascular anomaly characterized by the persistent patency of the fetal ductus arteriosus after birth, resulting in left-to-right shunting and hemodynamic compromise. While PDA is common in preterm neonates, this anomaly is rare in adults and often complicated by secondary cardiac pathologies, such as valvular disease, pulmonary hypertension, and arrhythmias. Optimal management of complex adult cases requires coordinated multidisciplinary care that balances surgical and transcatheter interventions.
A 32-year-old male with a history of untreated PDA presented with progressive palpitations and dyspnea. A subsequent diagnostic evaluation revealed severe mitral regurgitation, mild aortic regurgitation, ascending aortic dilation, and persistent atrial fibrillation. Multimodal imaging (computed tomography (CT), transthoracic echocardiography (TTE) and electrocardiography (ECG)) confirmed a PDA measuring approximately 9–10 mm × 15 mm (by TTE) with a left-to-right shunt. The patient underwent single-stage surgical repair, including PDA double-end ligation and oversewing under TEE guidance, mechanical mitral and aortic valve replacement, modified Maze procedure, left atrial reduction, and external wrapping plasty of the ascending aorta using a #28 synthetic graft (non-Bentall). Postoperatively, the patient developed acute kidney injury, hepatic dysfunction, and sepsis, requiring continuous renal replacement therapy (CRRT), vasopressors, and targeted antibiotics. Despite complications, multidisciplinary care stabilized the patient.
This case highlights the challenges of managing complex PDA in adults, particularly when complicated by multivalvular disease and arrhythmias. A one-stage surgical approach may reduce reoperation risks but requires vigilant postoperative monitoring for multiorgan dysfunction. Long-term follow-up with hemodynamic and imaging surveillance is essential for optimal recovery. Early identification and individualized strategy selection are crucial in high-risk adults with concomitant structural heart disease.
Keywords
- patent ductus arteriosus
- adult congenital heart disease
- cardiac surgery
- case report
Patent ductus arteriosus (PDA), a failure of the fetal ductus arteriosus to close postnatally, represents one of the most common congenital cardiovascular anomalies, accounting for 5–10% of all congenital heart diseases [1, 2]. While typically diagnosed and managed in infancy, persistent PDA in adulthood presents unique clinical challenges due to frequent associations with secondary complications including pulmonary hypertension, left heart volume overload, and irreversible ventricular remodeling [3, 4]. The hemodynamic consequences of chronic left-to-right shunting often precipitate valvular dysfunction, particularly mitral regurgitation, and may progress to Eisenmenger syndrome if left untreated [5].
Current management strategies for adult PDA remain controversial, with treatment decisions influenced by anatomical characteristics, shunt severity, and comorbid conditions [6]. While transcatheter closure has become first-line therapy for simple defects, complex cases involving large ductal dimensions or concurrent cardiac pathologies often necessitate open surgical repair [7]. Furthermore, the coexistence of PDA with acquired valvular disease and arrhythmias, as illustrated in our case, creates therapeutic dilemmas regarding single-stage versus staged interventions [8]. Emerging evidence suggests that combined procedures may reduce reoperation risks but require careful perioperative planning to address potential multi-organ dysfunction [9].
This case report describes a 32-year-old male with previously undiagnosed PDA presenting with advanced cardiac complications, including severe mitral regurgitation, ascending aortic dilation, and persistent atrial fibrillation. The clinical course underscores several critical aspects of adult PDA management: (i) the challenges of late diagnosis in asymptomatic patients, (ii) the technical considerations of combined valve and ductal surgery, and (iii) the high-risk nature of postoperative recovery in patients with chronic volume overload. Through this demonstration, we aim to contribute to the growing literature on optimal intervention timing and strategy selection for complex adult congenital heart disease.
A 32-year-old man with no prior medical history presented to our tertiary cardiac centre with one week of progressive palpitations and dyspnoea (New York Heart Association (NYHA) class III). He had a childhood cardiac murmur but remained asymptomatic until the current episode. On examination, he was haemodynamically unstable (BP 93/61 mmHg) with absolute arrhythmia (HR 95 bpm). Auscultation revealed a continuous machinery murmur (grade 4/6) at the left second intercostal space and a systolic murmur (grade 2/6) at the apex; peripheral pulses were weak and delayed, without peripheral oedema.
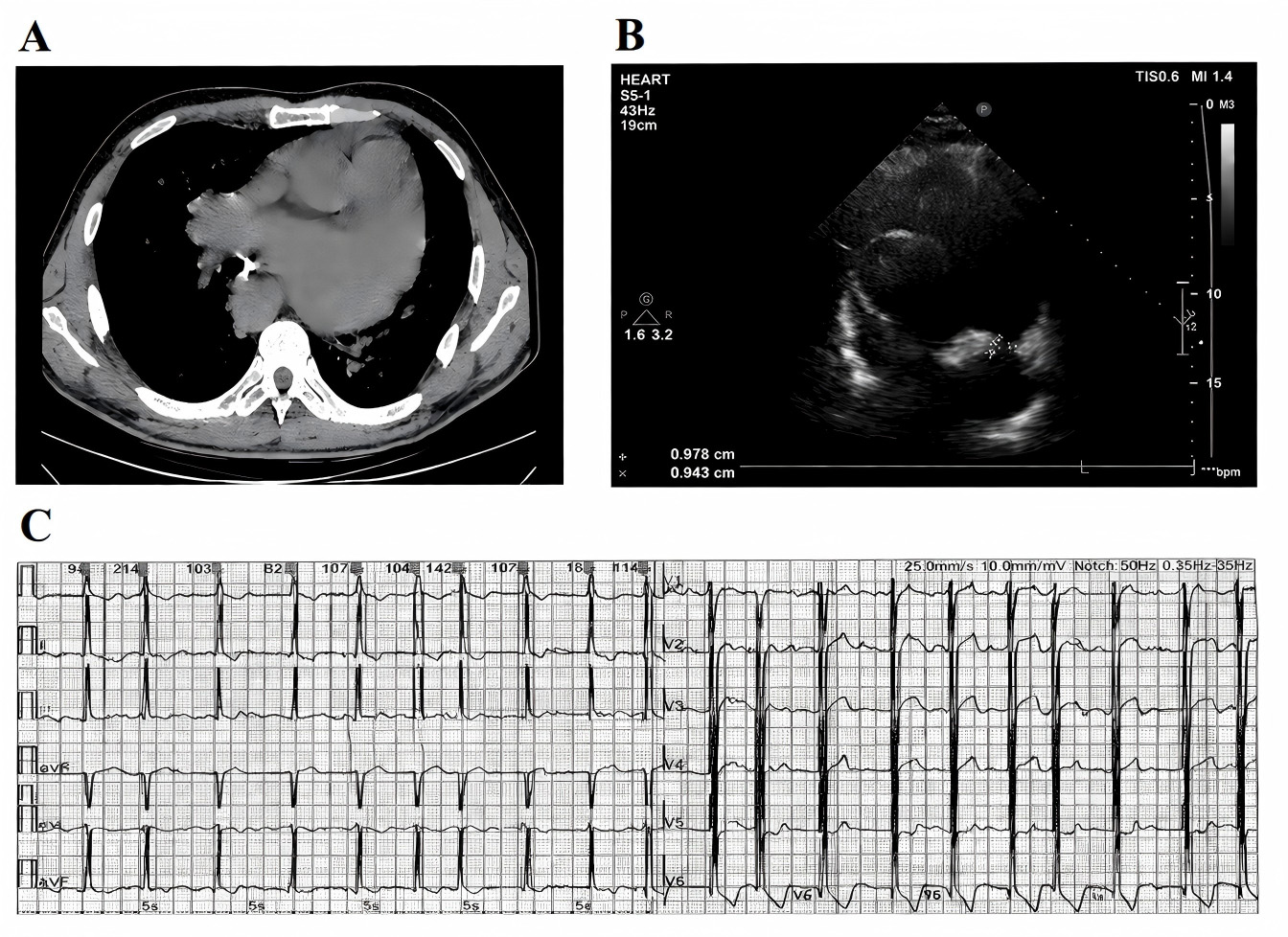
Multimodal imaging confirmed the diagnosis. Computed tomography (CT) showed
cardiomegaly with a small pericardial effusion and calcification at the pulmonary
end of the duct, and quantified the aortic root as normal—annulus 24 mm, sinus
of Valsalva 30 mm, sinotubular junction 30 mm—with isolated dilatation of the
proximal ascending aorta to 41 mm; main pulmonary artery 46 mm, right pulmonary
artery 21 mm, and left pulmonary artery 17 mm (Fig. 1A). Transthoracic
echocardiography (TTE) identified a tubular echolucent connection between the
descending aorta and the pulmonary artery—consistent with a PDA—with a width
of approximately 9 mm and a length of approximately 15 mm; left-sided enlargement
(left ventricular end-diastolic diameter (LVEDD) 88 mm; left atrial volume index
48 mL/m2), severe mitral regurgitation (vena contracta 6.5 mm, effective
regurgitant orifice area (EROA) 0.40 cm2), and preserved biventricular
systolic function (left ventricular ejection fraction (LVEF) 60%). Tricuspid
annular plane systolic excursion (TAPSE) was 17 mm, and the estimated pulmonary
artery systolic pressure (PASP) was approximately 56 mmHg (Fig. 1B). Chamber
quantification showed marked left atrial dilatation (superior–inferior 89 mm,
medial–lateral 102 mm), right atrial size (superior–inferior 56 mm,
medial–lateral 49 mm), and right ventricular basal diameter 36 mm.
Electrocardiography (ECG) demonstrated atrial fibrillation with a rapid
ventricular response (140 bpm) (Fig. 1C). Laboratory studies (Table 1) showed
N-terminal pro–B-type natriuretic peptide (NT-proBNP) 2089 pg/mL and creatinine
67 µmol/L (
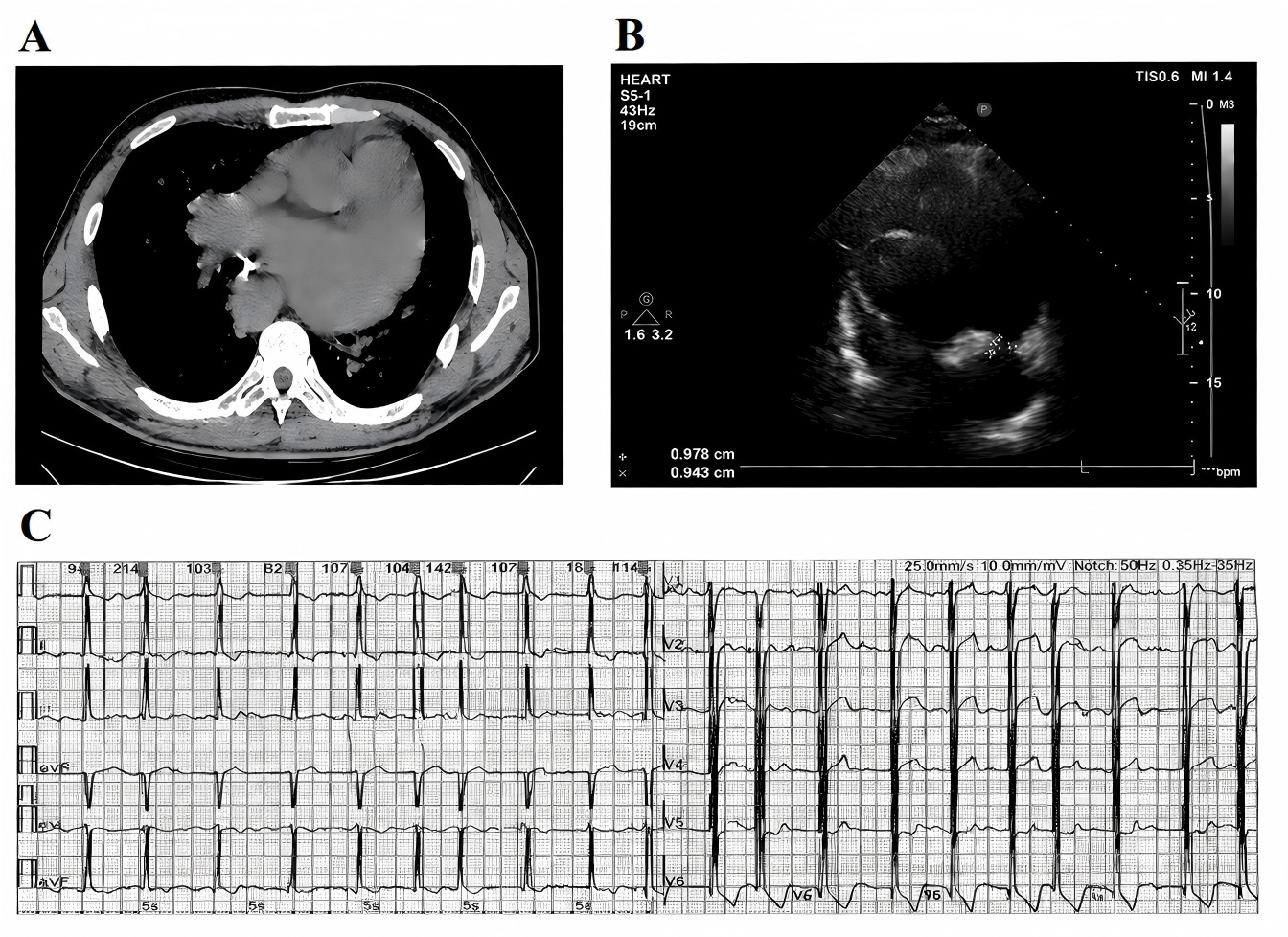 Fig. 1.
Fig. 1.
Preoperative examination. (A) A CT showed a significantly enlarged heart, a small amount of fluid in the pericardium, and calcification at the end of the pulmonary artery. (B) A TTE showed that the descending aorta and the main pulmonary artery were connected by a tube with a width of about 9–10 mm and a length of about 15 mm. (C) ECG suggests atrial fibrillation (fast ventricular rate type). CT, computed tomography; TTE, transthoracic echocardiography; ECG, electrocardiography.
| Test item | Result | Reference range | |
| Blood type | Type B RH positive | ||
| Blood routine | |||
| White blood cell (WBC) count | 5.51 |
4.0–10.0 | |
| Red blood cell (RBC) count | 4.86 |
4.3–5.8 | |
| Hemoglobin (HB) | 153 g/L | 130–175 | |
| Platelet count (PLT) | 131 |
125–350 | |
| Erythrocyte sedimentation rate (ESR) | 10 mm/h | 0–15 | |
| Liver function | |||
| Alanine aminotransferase (ALT) | 281 U/L | 0–40 | |
| Aspartate aminotransferase (AST) | 77 U/L | 0–40 | |
| Total bilirubin (TBil) | 20.2 µmol/L | 0–21 | |
| Direct bilirubin (DBil) | 9.2 µmol/L | 0–7 | |
| Total protein (TP) | 66.73 g/L | 65–85 | |
| Albumin (ALB) | 40.47 g/L | 40–55 | |
| Lactate dehydrogenase (LDH) | 244 IU/L | 120–250 | |
| Cardiac markers | |||
| Creatine kinase (CK) | 68 IU/L | 38–174 | |
| Myoglobin (Mb) | 0–85 | ||
| hs-cTnT | 19.06 pg/mL | 0–14 | |
| CK-MB | 1.96 µg/L | 0–5 | |
| NT-proBNP | 2089 pg/mL | ||
| Renal function & electrolytes | |||
| Potassium (K) | 4.41 mmol/L | 3.5–5.5 | |
| Sodium (Na) | 139.9 mmol/L | 135–145 | |
| Blood urea nitrogen (BUN) | 5.46 mmol/L | 2.9–7.1 | |
| Creatinine (Cr) | 67 µmol/L | 57–111 | |
| Uric acid (UA) | 348 µmol/L | 208–428 | |
| Coagulation | |||
| Prothrombin time (PT) | 13.9 s | 11–14.5 | |
| Prothrombin activity (PTA) | 89% | 80–120 | |
| International normalized ratio (INR) | 1.07 | 0.8–1.2 | |
| Activated partial thromboplastin time (APTT) | 41.2 s | 25–38 | |
| Fibrinogen (FIB) | 2.71 g/L | 2–4 | |
| Thrombin time (TT) | 17.1 s | 14–21 | |
| Infection and inflammatory indicators | |||
| Procalcitonin (PCT) | |||
| C-reactive protein (CRP) | 1.61 mg/L | ||
| Antistreptolysin O (ASO) | 71 IU/mL | ||
| Rheumatoid factor (RF) | 10.28 IU/mL | ||
| Thyroid function | |||
| FT3 | 5.59 pmol/L | 3.1–6.8 | |
| FT4 | 18.63 pmol/L | 12–22 | |
| Thyroid-stimulating hormone (TSH) | 2.449 µIU/mL | 0.27–4.2 | |
Preoperative blood test results of the patient. Findings indicate elevated cardiac biomarker (NT-proBNP), and mild abnormalities in hematologic and liver function parameters. Abbreviations: FT3, Free triiodothyronine; FT4, Free thyroxine; CK-MB, Creatine kinase-MB isoenzyme; hscTnT, High-sensitivity cardiac troponin T; NT-proBNP, N-terminal pro–B-type natriuretic peptide.
A multidisciplinary heart team concluded that the patient had a haemodynamically
significant PDA (approximately 9–10 mm
The determination to undertake closure of the PDA, modified Maze with radiofrequency ablation, left atrial reduction plasty, mechanical mitral valve replacement (MVR), mechanical aortic valve replacement (AVR), closure of the patent foramen ovale (PFO), ascending aorta external wrapping plasty, and temporary epicardial pacing lead implantation was predicated on several critical considerations:
After the administration of adequate anesthesia, the patient is positioned in the supine position, followed by routine skin antisepsis and draping. The right femoral artery is exposed for subsequent cannulation. A median sternotomy is performed, and the pericardium is opened, revealing mild pericardial effusion with a pale yellow hue, alongside significant cardiac enlargement, primarily affecting the left atrium and ventricle. The aortic-to-pulmonary artery ratio is 1:1, with dilation of the aortic sinus and ascending aorta. Palpable tremors are noted at the apex and aortic root. The left superior vena cava is absent.
After administering heparin, extracorporeal circulation is established, ensuring an activated clotting time (ACT) greater than 480 seconds while maintaining systemic perfusion. With the heart beating, the PDA is exposed through the pericardial reflection between the distal main pulmonary artery and the descending aorta. Under continuous transesophageal echocardiographic (TEE) color-Doppler guidance, the duct is circumferentially mobilized using a right-angle clamp and blunt dissection, taking care to avoid injury to the recurrent laryngeal nerve and to protect the calcified pulmonary arterial end. Vessel loops are passed around both the aortic and pulmonary ends to permit a brief test occlusion while systemic arterial and pulmonary artery pressures are monitored; abolition of the continuous shunt signal on TEE confirms effective interruption. Definitive closure is then achieved by double-end ligation (2-0 silk ties buttressed with felt), followed by over-sewing of the pulmonary arterial stump with a continuous 4-0 polypropylene suture to address the calcified edge. Fibrin sealant is applied to the suture line, and final TEE demonstrates no residual color-Doppler flow across the duct. Bipolar clamp ablation is subsequently performed on the right atrium.
Cooling is initiated, and ventricular fibrillation is induced. The ascending aorta and both the superior and inferior vena cavae are then occluded. The aortic root is incised, allowing for coronary perfusion with oxygenated blood and myocardial protection solution. The interatrial septum is opened, and the oval foramen is found to be patent. The patent foramen ovale was primarily closed with 4-0 polypropylene sutures. The mitral valve is thickened, with shortened and constricted chordae tendineae, resulting in severe stenosis and incompetence. The aortic valve is mildly thickened, without commissural fusion, and exhibits mild incompetence. Both the mitral and aortic valves are excised, retaining a portion of the posterior mitral leaflet and chordae tendineae.
The left atrial appendage is excised, and left atrial ablation is performed. Partial resection of the posterior wall and roof of the left atrium is followed by left atrial plasty.
A mitral valve sizer (#31) and an aortic valve sizer (#25) are used to determine the appropriate sizes. The #31 Chinese mechanical mitral valve is implanted with interrupted 2-0 polyester sutures. After knotting, the valve opens and closes as expected. A portion of the interatrial septum is excised, and the heart cavity is irrigated with saline. The septum is then sutured with 4-0 Prolene sutures, and after lung deflation in the head-down position, the knots are secured.
The tricuspid valve is assessed by inserting three fingers, revealing mild regurgitation, which does not require intervention. The #25 Chinese mechanical aortic valve is implanted using continuous 2-0 Prolene sutures, and after knotting, the valve function is confirmed.
The aortic incision is closed with continuous 5-0 Prolene sutures. Following lung deflation in the head-down position, the knot is tied, and the patient is rewarmed. A defibrillation shock (20 J) is delivered, restoring normal sinus rhythm, as confirmed by ECG.
An external wrapping plasty of the ascending aorta is performed using a #28 synthetic graft; the aortic root remains intact and no coronary reimplantation is undertaken, therefore this is not a Bentall procedure.
Extracorporeal circulation is discontinued, blood is returned, and heparin is neutralized with protamine sulfate. All cannulation tubes are removed without complication. Bleeding is noted at the junction of the aortic root and left atrial roof. Five interrupted sutures fail to control the bleeding, and an autologous pericardial patch is used to cover the area, with drainage directed into the right atrium. A temporary pacing wire is placed on the epicardium to ensure hemostasis. Three mediastinal drainage tubes are inserted, and the sternum is closed with wire.
After confirming that all instruments and sponges are accounted for, the chest is closed in layers.
On the first postoperative day following complex corrective cardiac surgery, the patient developed acute kidney injury, hepatic dysfunction, circulatory shock, and postoperative sepsis, indicative of severe multiple organ dysfunction (Table 2). Continuous renal replacement therapy (CRRT) was initiated to maintain fluid and electrolyte balance, as well as to mitigate the accumulation of uremic toxins. Hepatoprotective treatment, including reduced glutathione and polyene phosphatidylcholine, was administered to alleviate hepatocellular damage.
| Test item | Result | Reference range | |
| Blood routine | |||
| WBC count | 25.95 |
4.0–10.0 | |
| RBC count | 3.18 |
4.0–5.5 | |
| HB | 101 g/L | 120–160 g/L | |
| PLT | 110 |
100–300 | |
| Coagulation | |||
| PT | 18.8 s | 11–15 s | |
| PTA | 52% | 80–120% | |
| INR | 1.57 | 0.8–1.2 | |
| Liver function | |||
| ALT | 49 U/L | 0–40 U/L | |
| AST | 240 U/L | 0–40 U/L | |
| TBil | 56 µmol/L | 3.4–20.5 µmol/L | |
| DBil | 41.5 µmol/L | 0–6.8 µmol/L | |
| TP | 47.22 g/L | 60–83 g/L | |
| ALB | 30.67 g/L | 35–50 g/L | |
| Renal function & electrolytes | |||
| Na | 147.9 mmol/L | 135–145 mmol/L | |
| K | 4.13 mmol/L | 3.5–5.5 mmol/L | |
| Urea | 14.38 mmol/L | 2.8–7.2 mmol/L | |
| Cr | 317 µmol/L | 45–104 µmol/L | |
| Cardiac markers | |||
| PCT | |||
| NT-proBNP | 6496 pg/mL | ||
| Myoglobin | 2299 µg/L | ||
| hs-Troponin T | |||
| CK-MB | 47.16 µg/L | ||
| LDH | 1281 IU/L | 120–250 IU/L | |
| 973 IU/L | 72–182 IU/L | ||
| CK | 2753 IU/L | 40–200 IU/L | |
| Troponin I | |||
Postoperative blood test results of the patient. The results suggest acute
kidney injury, hepatic dysfunction, and inflammatory response, consistent with
multiple organ dysfunction syndrome (MODS). Abbreviations:
Hemodynamic instability was managed with escalating vasopressor support, utilizing dopamine, norepinephrine, and epinephrine, titrated to maintain the target mean arterial pressure. Empirical antimicrobial therapy with piperacillin-tazobactam was commenced, and subsequently escalated to imipenem upon microbiological confirmation of Klebsiella pneumoniae infection. Additional supportive measures included transfusions of leukocyte-depleted red blood cells and fresh frozen plasma to correct anemia and coagulopathy, alongside continuous pericardial and mediastinal drainage to prevent cardiac tamponade.
During the early postoperative period, the patient experienced supraventricular tachycardia that was refractory to pharmacological cardioversion with amiodarone. As a result, synchronized direct-current cardioversion was performed. This multidisciplinary, multimodal management approach aimed to stabilize hemodynamics, halt the progression of organ dysfunction, and reduce perioperative mortality risk, particularly given the high-risk nature of the patient’s congenital and acquired structural heart disease.
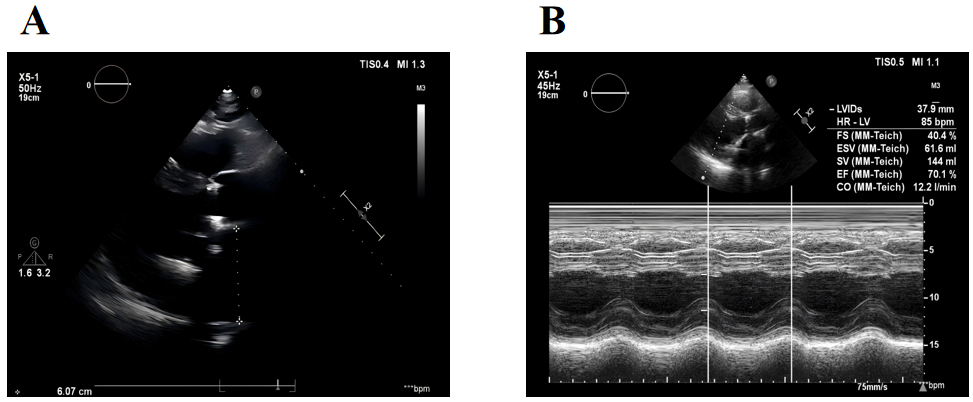
At 1-year follow-up, transthoracic echocardiography demonstrated a pronounced reduction in cardiac volume overload with substantial regression of left atrial and ventricular dilation: left atrial diameter decreased from 89 mm preoperatively to 61 mm, and LVEDD from 88 mm to 63 mm. LVEF improved from 60% to 70%, and pulmonary artery systolic pressure remained consistently below baseline values, confirming effective elimination of the left-to-right shunt and restoration of cardiac function (Fig. 2). The NYHA functional class improved from III before surgery to I, with the patient able to undertake normal daily and moderate physical activities without limitation; palpitations and exertional dyspnoea had largely resolved, and exercise tolerance was markedly enhanced.
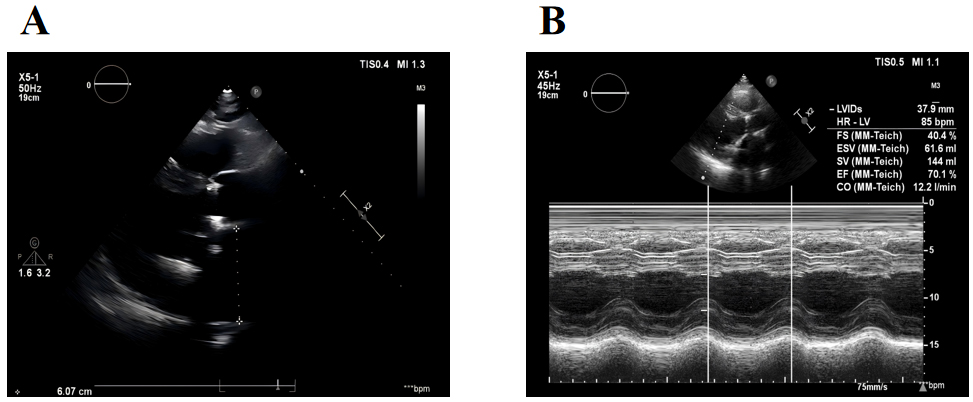 Fig. 2.
Fig. 2.
TTE in the first year after surgery. (A) The left heart is enlarged, but it is better than before. (B) Heart function is restored.
Between the second and third postoperative years, cardiac chamber dimensions and function remained stable, with LVEF maintained at about 60% and PASP persistently below preoperative levels. NYHA functional class remained at I, and there were no arrhythmia-related symptoms or signs of heart failure.
By the fourth postoperative year, LVEF was preserved at 60%, although mild mitral regurgitation (vena contracta 5 mm) was detected and judged to be clinically insignificant. At the 5-year review, echocardiography continued to show stable cardiac structure and function, with mild mitral regurgitation and PASP within non-significant ranges. No further atrial or ventricular enlargement was observed, indicating durable haemodynamic correction.
Throughout the entire follow-up period, the patient remained in NYHA class I, continued oral warfarin and metoprolol therapy, and reported no restrictions in occupational or social activities. These findings indicate that PDA closure in this context provided sustained improvement in cardiac structure and function, without major late complications, over a 5-year period.
At the most recent visit, on June 6, 2025, the patient reported that daily life and work remained unaffected. Occasional palpitations and chest tightness occurred only during vigorous exertion, resolving with rest. He continued anticoagulation and beta-blocker therapy, and his clinical condition remained stable.
This case illustrates several key issues in the management of PDA persisting into adulthood. Diagnosis was delayed in a previously asymptomatic individual, consistent with reports that about 0.5% of PDAs remain undetected until adulthood [11]. As described by Backes and colleagues [4], chronic left heart volume overload can be well tolerated for decades before decompensation occurs, as exemplified by this presentation.
Management decisions in such complex cases remain contentious. Although
transcatheter closure is the standard for isolated PDA, our experience aligns
with Hamrick and colleagues’ observation that coexistent severe valvular
disease—particularly grade
Current recommendations for adult PDA assessment include measurement of oxygen
saturation in both upper and lower extremities to detect right-to-left shunts,
and consideration of cardiac catheterisation in suspected pulmonary hypertension.
Closure is indicated in the presence of left heart dilatation and a net
left-to-right shunt if pulmonary artery systolic pressure is
In this high-risk adult with complex PDA, multivalvular disease, and arrhythmia, a single-stage surgical approach achieved durable haemodynamic stability, symptom resolution, and favourable 5-year outcomes. The results support comprehensive, specialist-led intervention in selected patients, while highlighting the importance of early detection to avoid secondary complications.
The datasets upon which the manuscript’s conclusions are based in the current study are available from the corresponding author upon reasonable request.
ZZ contributions to the design of the work; LT contributions to the conception of the work; CD, ML and QQ contributions to the acquisition of data for the work. All authors have participated sufficiently in the work. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
The study was conducted in accordance with the Declaration of Helsinki. As this was a retrospective case report, the Ethics Committee of Yichang Central People’s Hospital waived the requirement for formal ethical approval and informed consent (Approval Number: 2025-479-01). For any images or data in this article that may identify individual identities, the relevant individuals have given their written informed consent.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/HSF54243.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.