






 , Karl Dossche 2, Anthony Vanermen 2, Ivo Deblier 2
, Karl Dossche 2, Anthony Vanermen 2, Ivo Deblier 21 Rehabilitation Sciences and Physiotherapy, Faculty of Medicine and Health Sciences, University of Antwerp, 2650 Antwerp, Belgium
2 Department of Cardiovascular Surgery, ZAS Middelheim, 2020 Antwerp, Belgium
Abstract
Age and the need for urgent surgical aortic valve replacement (SAVR) could affect 30-day mortality and long-term survival. These factors were assessed in a stratified manner to assess the subsequent effects on these outcomes. A retrospective chart review was performed in patients undergoing SAVR. Urgent SAVR was defined as the need for surgery during admission in patients diagnosed with aortic valve disease. Preoperative predictors of urgent SAVR were identified by entering significant factors into a logistic regression model. Predictors of 30-day mortality were identified in parallel stratified analyses by age (<80 years, 80 to 85 years, and >85 years) and operative status (elective vs. urgent). The effect of age groups on long-term mortality, stratified by operative status, was assessed using Kaplan–Meier analysis. Predictors of this outcome were identified using Cox proportional hazards analysis. Cardiac factors were the main predictors of the need for urgent SAVR, whereas age had an effect only in univariate analysis. Thirty-day mortality increased significantly in patients older than 80 years, which was central to the subsequent age-stratified analyses. The need for urgent SAVR was the dominant predictor of mortality across all age groups. Conversely, age over 80 years was the dominant predictor of 30-day mortality in patients undergoing both elective and urgent SAVR. Advanced age and the need for urgent SAVR reduced long-term survival to a comparable degree, but only age was identified as an independent predictor. The need for urgent surgery in patients older than 85 years was associated with very poor short-term and long-term survival outcomes. The need for urgent SAVR likely represents exhaustion of the cardiac compensatory mechanisms required to maintain adequate circulation. With increasing age, patients become more vulnerable to the need for urgent SAVR. This condition should be avoided through timely valve replacement.
Keywords
- aortic valve replacement
- urgent surgery
- age
- survival
The incidence of aortic valve stenosis (AS) increases with age. Moreover, AS affects up to 10% of the population older than 70 years and is highly fatal once the condition becomes symptomatic [1]. As rheumatic disease has become less common, the age at onset of severe obstruction has shifted from the sixth to the eighth decade of life. Although symptom onset is an important determinant of outcome, advanced age can make distinguishing symptoms of valvular origin from those of other age-related comorbidities more difficult [2]. The development of left ventricular hypertrophy and a decrease in aortic valve area have been identified as predictors of symptoms. Although asymptomatic patients could be considered low risk, the course of the condition at this stage is not considered benign because myocardial fibrosis may already be present [1]. Once symptoms of AS develop, life expectancy without adequate treatment decreases drastically. Only aortic valve replacement improves prognosis [2]. Furthermore, the clinically relevant burden of AS on the left ventricle might be underestimated [3]. A meta-analysis showed that the baseline severity of AS predicted disease progression with respect to mean transvalvular gradient, peak velocity, and aortic valve calcium score. Thus, patients with rapid disease progression may benefit from early valve replacement, even if they remain asymptomatic [4]. Surgical aortic valve replacement (SAVR) has been the gold-standard treatment for decades and is the oldest treatment shown to alter prognosis. However, over the past 10 to 15 years, transcatheter aortic valve implantation (TAVI) has emerged as an attractive, less invasive option for appropriately selected patients [5]. A marked and rapid increase in the annual combined SAVR and TAVI volume was observed over an 18-year study period beginning in 2000. This rise paralleled the rapid increase in the number of patients with an indication for valve replacement. This observation might indicate significant underutilization of valve replacement for severe AS, particularly in patients with low-gradient severe AS. Given the mortality rate of untreated symptomatic severe AS, recognition of the risks associated with undertreatment should prompt timely intervention [6]. Although TAVI has been introduced as a less invasive alternative, SAVR remains a treatment option, even in older patients. Indeed, an increase in the number of older patients referred for surgery was observed until recently [7], which may be related to the reimbursement policy for TAVI in Belgium. Postoperative outcomes with respect to 30-day mortality and long-term survival are generally favorable. However, outcomes decrease with age and with the need for urgent valve replacement [8]. Initial observations indicate that the need for urgent SAVR was higher among elderly patients, complicating disentangling the effects of age and elective status. The recent need for urgent SAVR in 16% of patients underscores the importance of this problem [9]. Reports examining the effects of age stratification and selective status are scarce. Therefore, the following research questions need to be addressed: What is the distribution of the need for urgent SAVR across age categories? Which factors predict the need for urgent SAVR? What is the dominant predictor of 30-day mortality and long-term survival within separate age categories? How does the need for urgent SAVR influence the effect of age on outcomes?
This retrospective file study included 2500 consecutive patients undergoing 2538 SAVR operations, with or without concomitant procedures such as coronary artery bypass grafting (CABG), mitral valve repair, or ascending aorta procedures. Patients with mechanical valves or prosthetic valves in another position were excluded. Urgent SAVR was defined as the need for surgery during the admission in which the diagnosis of valve disease was made (i.e., within days) or when SAVR could not be postponed. Patients requiring emergency SAVR (i.e., on the same day) were also included in this definition but were not analyzed as a separate group. Patients for whom this status was uncertain were also excluded. Chronic kidney disease (CKD) was defined as creatinine clearance <60 mL/min, and chronic obstructive pulmonary disease (COPD) as a forced expiratory volume in one second below 70% of the predicted value. Diabetes was defined as plasma glucose >126 mg% or use of antidiabetic treatment, whereas arterial hypertension was defined as blood pressure >140/90 mm Hg or use of antihypertensive treatment. Peripheral artery disease (PAD) and coronary artery disease (CAD) were defined as lesions >50% on angiography or the need for invasive treatment. Left ventricular ejection fraction (LVEF) and the severity of valve disease were documented by echocardiography, while atrial fibrillation and conduction defects were diagnosed by electrocardiography. Duke’s criteria were used to diagnose endocarditis, and myocardial infarction was documented by electrocardiography and elevated heart enzymes. Cardiopulmonary bypass (CPB) and aortic cross-clamp (ACC) times were measured in minutes. The outcomes under study were 30-day and long-term mortality.
The analysis was performed in several steps. First, associations between preoperative and operative factors and the need for urgent versus elective SAVR were assessed using chi-square analysis for categorical variables and Student’s t-test for continuous variables. The latter was selected because the large sample size allowed calculation of Cohen’s d as a measure of effect size. Logistic regression analysis was then used to identify predictors of urgent SAVR. The effect of requiring urgent SAVR on postoperative adverse events and resource use was analyzed using a chi-square test. This was followed by a univariate analysis of 30-day mortality across stratified age categories according to elective status. Predictors of 30-day mortality were identified in parallel multivariate logistic regression analyses for (1) the whole group, (2) separate age categories, and (3) urgent versus elective SAVR. Age thresholds >80 and >85 years were identified as important in this context and had also been used in earlier investigations [7,8]. In the final step, the effects of age and elective status on long-term survival were analyzed using Kaplan–Meier analysis with the log-rank test. These data are also presented as curves. To emphasize the combined effect of age and elective status, additional curves show the outcome as 30-day mortality plus long-term mortality. Predictors of long-term mortality by elective status were identified using Cox proportional hazards analysis. Analyses were performed using SPSS version (31.0.1.0, IBM, Chicago, USA). The study was approved by the ZNA ethical committee under protocol No. 2656.
Elective status could be documented for 2252 patients. Of these, 417 (18.5%) patients underwent urgent SAVR. Table 1 shows the associations between the need for urgent SAVR and preoperative factors. The most important factors were cardiac in nature and were ranked by chi-square value, which represents the strength of the association. Prior congestive heart failure showed the strongest association. Infective endocarditis was another important factor in the decision to operate on an urgent basis. Of the 134 patients with preoperative myocardial infarction, 88 had experienced a recent event, i.e., had occurred within three weeks before surgery. An LVEF below 50% was also an important factor; however, the effect of left ventricular function on the outcome was evident at an earlier stage: an ejection fraction of less than 65% was present in 604/1237 (48.8%) of patients undergoing elective SAVR versus 163/257 (63.4%) of those undergoing urgent surgery (p < 0.001), although with a lower χ2 value of 8.1. Mean LVEF also differed significantly between the groups (62.7 ± 15.1% vs. 54.4 ± 17.8%; p < 0.001; Cohen’s d = 0.535). In contrast, the difference in severity of valve disease in terms of aortic valve area did not differ significantly (75.0 ± 24.7 mm2 vs. 73.1 ± 27.0 mm2; p = 0.295; Cohen’s d = 0.076). The presence of CAD was associated with urgent SAVR only when a significant left main stem lesion was present. Significant non-cardiac factors included CKD and COPD, with differences in plasma creatinine (1.04 ± 0.42 mg% vs. 1.36 ± 1.04 mg%; p < 0.001; Cohen’s d = 0.553) and forced expiratory volume in 1 second (93.9 ± 20.9% vs. 81.5 ± 22.7%; p < 0.001; Cohen’s d = 0.584). There was also an increased need for urgent SAVR in patients >80 years, and even more so in those >85 years. Diabetes had a borderline effect. The difference in EuroSCORE II between the two groups was large (4.9 ± 4.8% vs. 14.6 ± 12.4%; p < 0.001; Cohen’s d = 1.405), which was expected because the need for urgent surgery is included in this score.
| Preoperative factor | Elective SAVR (%) | Urgent SAVR (%) | p-value | χ2 | ||
|---|---|---|---|---|---|---|
| Demographic | ||||||
| Age | <0.001 | 22.3 | ||||
| <70 years | 281/343 (81.9) | 62/343 (18.1) | ||||
| 70–75 years | 477/563 (84.7) | 86/563 (15.3) | ||||
| 75–80 years | 566/679 (83.4) | 113/679 (16.6) | ||||
| 80–85 years | 406/515 (78.8) | 109/515 (21.2) | ||||
| >85 years | 105/151 (69.5) | 46/151 (30.5) | ||||
| Era >2008 | 1011/1835 (55.1) | 241/415 (58.1) | 0.270 | |||
| Male gender | 1061/1835 (57.8) | 230/416 (55.3) | 0.346 | |||
| Cardiovascular | ||||||
| Congestive heart failure | 263/1833 (19.8) | 244/415 (58.8) | <0.001 | 261.0 | ||
| Endocarditis | 27/1833 (1.5) | 39/417 (9.4) | <0.001 | 74.1 | ||
| Myocardial infarction | 236/1831 (12.9) | 134/413 (32.4) | <0.001 | 93.6 | ||
| LVEF <50% | 232/1332 (17.4) | 110/293 (37.5) | <0.001 | 58.5 | ||
| Atrial fibrillation | 415/1832 (22.7) | 146/414 (35.3) | <0.001 | 28.7 | ||
| Left main CAD | 177/1835 (9.6) | 66/415 (15.9) | <0.001 | 13.8 | ||
| Pulmonary artery hypertension | 350/1259 (27.8) | 12/298 (40.3) | <0.001 | 17.8 | ||
| Ischemic neurologic event | 255/1835 (13.9) | 73/414 (17.6) | 0.052 | |||
| Prior cardiac surgery | 188/1833 (10.3) | 55/417 (13.2) | 0.082 | |||
| Peripheral artery disease | 362/1729 (20.9) | 92/390 (23.6) | 0.249 | |||
| Conduction defects | 584/1829 (31.9) | 126/414 (30.4) | 0.555 | |||
| Arterial hypertension | 1308/1831 (71.4) | 296/411 (72.0) | 0.813 | |||
| Permanent pacemaker | 79/1832 (4.3) | 17/414 (4.1) | 0.852 | |||
| Non-cardiac | ||||||
| CKD | 286/1830 (15.6) | 126/411 (30.7) | <0.001 | 50.5 | ||
| COPD | 476/1794 (26.5) | 154/384 (40.1) | <0.001 | 28.3 | ||
| Diabetes mellitus | 380/1835 (20.7) | 128/415 (30.8) | <0.001 | 19.9 | ||
| BMI >30 kg/m2 | 338/1236 (27.3) | 73/284 (25.7) | 0.574 | |||
| Malignancy | 293/1827 (16.0) | 69/414 (16.7) | 0.753 | |||
SAVR, surgical aortic valve replacement; BMI, body mass index; CKD, chronic kidney disease; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; LVEF, left ventricular ejection fraction; χ2, chi-square.
Table 2 shows that the need for urgent SAVR was significantly associated with a CPB time of 120 minutes (min) or more. The CPB run was nearly 20 minutes longer (118.2 ± 41.5 min vs. 137.8 ± 49.4 min; p < 0.001; Cohen’s d = 0.455). A similar, although weaker, association was observed for an ACC time >60 min. The ACC time was about 8 minutes longer (67.3 ± 21.5 min vs. 75.2 ± 29.3 min; p < 0.001; Cohen’s d = 0.345). These findings are consistent with the need for two or more procedures, particularly for mitral valve repair.
| Operative factor | Elective (%) | Urgent (%) | p-value | χ2 |
|---|---|---|---|---|
| CPB time >120 min | 582/1647 (35.3) | 199/373 (53.4) | <0.001 | 41.6 |
| ACC time >60 min | 860/1449 (59.4) | 226/316 (71.5) | <0.001 | 16.2 |
| Two or more procedures | 1137/1835 (62.0) | 299/417 (71.7) | <0.001 | 14.0 |
| Mitral valve repair | 63/1835 (3.4) | 26/416 (6.3) | 0.008 | - |
| Concomitant CABG | 1069/1835 (58.3) | 266/416 (63.9) | 0.033 | - |
| Incomplete revascularization | 214/1831 (11.7) | 52/404 (12.9) | 0.506 | - |
| Procedure ascending aorta | 156/1833 (8.5) | 33/516 (7.7) | 0.701 | - |
ACC, aortic cross-clamp; CABG, coronary artery bypass grafting; CPB, cardiopulmonary bypass; min, minutes.
The development of a need for urgent SAVR could be considered an endpoint in the preoperative trajectory; the associated predictors are presented in Table 3. The three factors with odds ratios >2 were all cardiac. In cases of endocarditis, the reasons for urgent SAVR were protracted sepsis, structural damage to the heart, and heart failure. For most patients who had suffered a recent myocardial infarction, the presence of severe CAD as a comorbid condition prompted the decision for urgent surgery. The fourth cardiac factor for left main coronary stenosis did not reach an odds ratio of 2 but remained highly significant. Chronic renal and pulmonary dysfunction were also predictive, whereas age could not be identified as a predictor.
| Predictor | OR | 95% CI | p-value |
|---|---|---|---|
| Endocarditis | 6.67 | 3.64–11.86 | <0.001 |
| Congestive heart failure | 4.50 | 3.50–5.78 | <0.001 |
| Myocardial infarction | 2.28 | 1.72–3.03 | <0.001 |
| Left main CAD | 1.77 | 1.25–2.51 | 0.001 |
| CKD | 1.39 | 1.04–1.85 | 0.027 |
| COPD | 1.33 | 1.03–1.72 | 0.028 |
CAD, coronary artery disease; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; OR, odds ratio; 95% CI, 95% confidence interval.
Table 4 shows the association between the need for urgent SAVR and resource use, laboratory test values, clinical parameters, and adverse postoperative events. The need for urgent SAVR was associated with a fivefold increase in 30-day mortality. This outcome is the most impactful finding in both current and prior research [8]. The EuroSCORE II overestimated observed mortality in the elective group (4.9% vs. 3.3%) but underestimated this outcome in the urgent group (14.6% vs. 16.4%). The current results also suggest that the increase in mortality is associated with low cardiac output syndrome, acute renal injury, and pulmonary complications. The need for urgent SAVR was associated with a significantly higher postoperative peak glucose level (+22 mg%), a lower peak partial oxygen pressure (–7 mm Hg), a higher peak plasma creatinine (+0.5 mg%); the need for urgent SAVR was also coupled with a nearly twofold greater increase in plasma creatinine (0.34 mg% vs. 0.62 mg%) and a threefold greater need for renal replacement therapy. The reduction in glomerular filtration rate was also higher in patients who required urgent SAVR, although less pronounced. The difference in the lowest postoperative hematocrit between the two groups was smaller, yet still significant. While the rate of postoperative bleeding and the need for reintervention did not differ between the groups, the increased need for packed cells after urgent SAVR (about 1.7 units) was significant. The need for urgent SAVR was also associated with longer lengths of stay in the intensive care unit (two more days) and in the postoperative period (three more days). The mechanical ventilation time was increased by 16 hours. All of these differences were significant with p< 0.05.
| Factor | Elective (%) | Urgent (%) | p-value | χ2 | |
|---|---|---|---|---|---|
| Need for resources | |||||
| LOS in ICU >1 day | 414/1521 (27.2) | 200/351 (57.0) | <0.001 | 114.6 | |
| >4 units packed cells | 225/1237 (18.2) | 97/281 (34.5) | <0.001 | 36.5 | |
| Renal replacement therapy | 59/1831 (3.2) | 41/513 (8.0) | <0.001 | 35.6 | |
| Mechanical ventilation >8 h | 443/1231 (36.0) | 147/284 (51.8) | <0.001 | 24.1 | |
| Thrombocyte concentration | 129/1237 (10.4) | 58/279 (20.8) | <0.001 | 22.6 | |
| Plasma derivatives | 330/1236 (26.7) | 106/279 (38.0) | <0.001 | 14.2 | |
| Permanent PM implantation | 50/1833 (2.7) | 16/416 (3.8) | 0.222 | - | |
| Reintervention | 63/1835 (3.4) | 10/415 (2.4) | 0.288 | - | |
| Adverse events | |||||
| Mortality | 61/1833 (3.3) | 68/415 (16.4) | <0.001 | 106.7 | |
| Low cardiac output | 107/1831 (5.8) | 69/414 (16.7) | <0.001 | 54.7 | |
| Acute renal injury | 339/1833 (18.5) | 126/412 (30.6) | <0.001 | 29.9 | |
| Pulmonary complications | 229/1834 (12.5) | 94/414 (22.7) | <0.001 | 28.7 | |
| Delirium | 172/1749 (9.8) | 59/378 (15.6) | 0.001 | - | |
| Atrial fibrillation | 746/1833 (40.7) | 147/414 (35.5) | 0.051 | - | |
| Bleeding | 117/1832 (6.4) | 34/414 (8.2) | 0.180 | - | |
| Thromboembolism | 63/1832 (3.4) | 18/414 (4.3) | 0.370 | - | |
| Laboratory values | |||||
| Plasma creatinine (mg%) | 0.99 (0.76–1.48) | 1.31 (0.92–2.23) | <0.001 | - | |
| Plasma glucose (mg%) | 156 (135–181) | 175 (152–212) | <0.001 | - | |
| Increase in creatinine (mg%) | 0.20 (0.06–0.55) | 0.27 (0.11–1.09) | <0.001 | - | |
| Arterial pO2 (mm Hg) | 80 (63–99) | 75 (63–88) | <0.001 | - | |
| Hematocrit (%) | 24.3 (21.8–26.8) | 23.9 (21.7–26.3) | <0.001 | - | |
| Reduction of GFR (mL/min) | 14 (8–22) | 17 (8–31) | 0.017 | - | |
| Clinical parameters | |||||
| Left atrial pressure (cm H2O) | 16 (12–19) | 17 (13–20) | <0.001 | - | |
| Peak TVG (mm Hg) | 17 (10–20) | 16 (11–18) | 0.623 | - | |
| Mean TVG (mm Hg) | 9 (6–13) | 9 (7–13) | 0.497 | - | |
| Need for resources | |||||
| Units packed cells | 1 (0–3) | 3 (1–6) | <0.001 | - | |
| Postoperative LOS (days) | 8 (7–10) | 8 (7–10) | <0.001 | - | |
| Mechanical ventilation (h) | 6 (4–9) | 8 (5–13) | <0.001 | - | |
| LOS in ICU (days) | 1 (1–2) | 1 (1–3) | <0.001 | - | |
GFR, glomerular filtration rate; ICU, intensive care unit; LOS, length of stay; TVG, transvalvular gradient; pO2, partial oxygen pressure; PM, pacemaker.
Table 5 shows the univariate association between age class and 30-day mortality, for all patients and after stratification by elective status. This association was highly significant (p < 0.001) across all age groups. The overall 30-day mortality was 138/2538 (5.4%). Mortality increased only slightly with age among patients younger than 80 years but doubled in those aged 80 to 85 years. In patients older than 85 years, mortality increased fourfold to 16.1%. A similar effect was observed for urgent SAVR, with a mortality rate of 68/417 (16.4%) across all age classes. Mortality after non-elective SAVR was comparable to that in patients under 80 years. These observations justified stratification by age group and elective status, with 80 and 85 years chosen as the age cutoffs because of the impact of these age groups on the outcome.
| Age group (years) | All (%) | Elective (%) | Urgent (%) |
|---|---|---|---|
| <70 | 13/343 (3.8) | 5/281 (1.8) | 8/62 (12.9) |
| 70–75 | 18/662 (2.7) | 11/576 (1.9) | 7/86 (8.1) |
| 75–80 | 31/678 (4.6) | 14/565 (2.5) | 17/113 (15.0) |
| 80–85 | 42/514 (8.2) | 22/406 (5.4) | 20/108 (18.5) |
| >85 | 25/151 (16.6) | 9/105 (8.6) | 16/46 (34.8) |
SAVR, surgical aortic valve replacement.
Table 6 shows the predictors of 30-day mortality for all patients. Age, as a potential predictor, was entered into the analysis at thresholds of >70, >75, >80, and >85 years as part of a sensitivity analysis. This analysis did not show a significant effect of age at any threshold, except for age >80 years. This finding is supported by the observation that the need for urgent SAVR and 30-day mortality increased in patients >80 years of age.
| Predictor | OR | 95% CI | p-value |
|---|---|---|---|
| Urgent SAVR | 4.03 | 2.63–6.17*** | <0.001 |
| Aged >80 years | 2.53 | 1.66–3.85*** | <0.001 |
| COPD | 2.00 | 1.31–3.04** | 0.001 |
| Diabetes | 1.96 | 1.27–3.02** | 0.002 |
| CPB time >120 min | 1.92 | 1.25–2.94** | 0.003 |
| Atrial fibrillation | 1.82 | 1.19–2.78** | 0.006 |
| Incomplete revascularization | 2.02 | 1.21–3.38** | 0.007 |
| CKD | 1.76 | 1.13–2.73* | 0.013 |
CPB, cardiopulmonary bypass; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; OR, odds ratio; SAVR, surgical aortic valve replacement; 95% CI, 95% confidence interval; ***, p < 0.001; **, p < 0.01; *, p < 0.05.
Table 7 shows the predictors stratified by each of the three age categories. In each age category, the need for urgent SAVR remains the most important predictor, with an odds ratio greater than four. The need for urgent SAVR is also the only consistent predictor, whereas diabetes, COPD, and CPB time are predictive in only one or two age categories and have lower odds ratios.
| Predictor | <80 years | 80–85 years | >85 years | |||
|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Urgent SAVR | 4.45 | 2.45–8.07*** | 5.08 | 2.14–12.07*** | 4.97 | 1.90–13.01** |
| Diabetes | 2.80 | 1.58–4.98*** | - | - | - | - |
| COPD | 2.26 | 1.27–4.03** | 2.64 | 1.18–5.94* | - | - |
| CPB time >120 min | 2.25 | 1.23–4.09** | - | - | 3.43 | 1.26–9.31* |
CPB, cardiopulmonary bypass; COPD, chronic obstructive pulmonary disease; OR, odds ratio; SAVR, surgical aortic valve replacement; 95% CI, 95% confidence interval; ***, p < 0.001; **, p < 0.01; *, p < 0.05.
A parallel analysis, stratified by elective status, is shown in Table 8. This analysis compares predictors among patients undergoing elective versus urgent SAVR. In this model, ages >80 were included for the reasons previously provided.
| Predictor | Urgent SAVR | Elective SAVR | ||
|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | |
| Aged >80 years | 2.51 | 1.47–4.31*** | 2.63 | 1.54–4.50** |
| COPD | 2.24 | 1.30–3.83** | 2.28 | 1.33–3.92** |
| Atrial fibrillation | 2.05 | 1.18–3.55* | 2.03 | 1.17–3.52* |
| Incomplete revascularization | 2.01 | 1.05–3.84* | - | - |
COPD, chronic obstructive pulmonary disease; OR, odds ratio; 95% CI, 95% confidence interval; ***, p < 0.001; **, p < 0.01; *, p < 0.05.
Table 9, alongside Figs. 1,2, and Tables 10,11, show the effect of age stratification by elective status on long-term survival, which was significant (p < 0.001) in all groups. From Table 9, the effect of increasing age category can be derived. In the elective SAVR group, mean survival decreases by 23 to 30 months across age categories, except in the highest age category. In the urgent SAVR group, the decrease in mean survival ranged from 17 to 23 months, including the highest age categories. Conversely, the decrease in survival associated with the need for urgent SAVR was comparable across almost all age categories: 33 months in the lowest age category, followed by 20, 20, 12, and 25 months in the higher age categories, respectively. This suggests that the effect of the need for urgent SAVR on long-term survival is comparable to that of age.
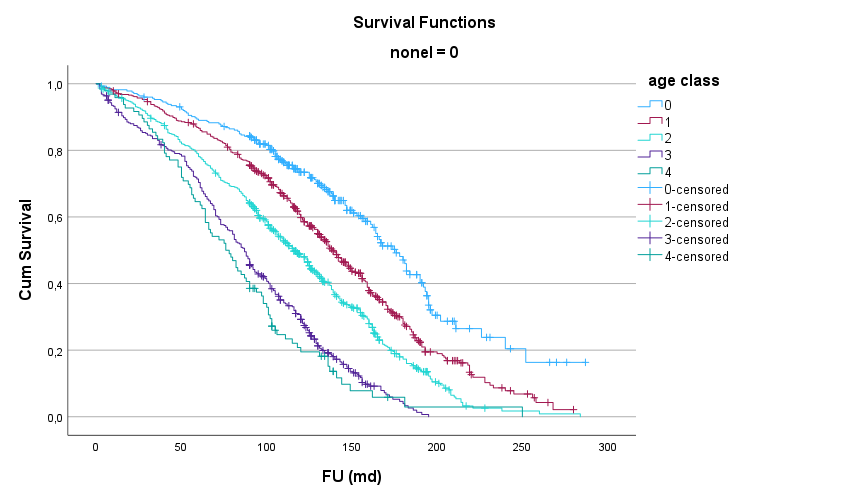 Fig. 1.
Fig. 1.Effect of age categories on long-term mortality after elective SAVR. Cum survival, cumulative survival; FU (md): follow-up in months; Non-elective (Non-el) = 0: elective; age class 0, <70 y; age class 1, 70–<75 y; age class 2, 75–<80 y; age class 3, 80–<85 y; age class 4, >85 y.
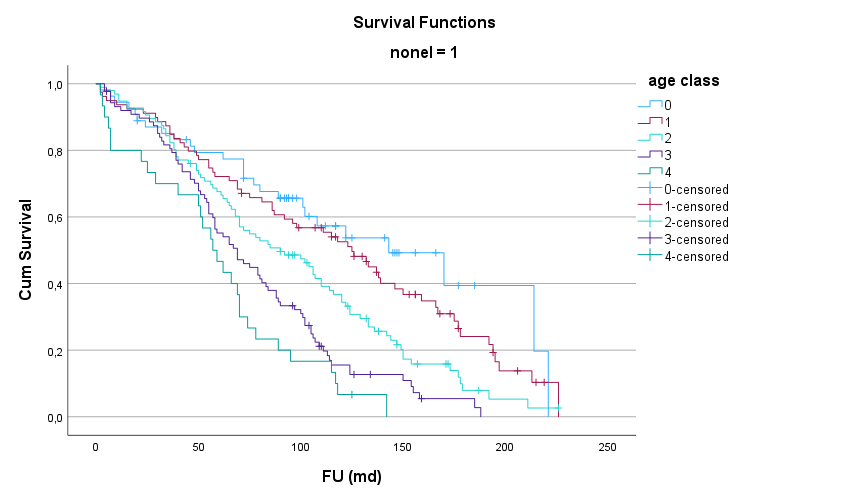 Fig. 2.
Fig. 2.Effect of age categories on long-term mortality after urgent SAVR. Cum survival, cumulative survival; FU (md), follow-up in months; nonel = 1, urgent; age class 0, <70 y; age class 1, 70–<75 y; age class 2, 75–<80 y; age class 3, 80–<85 y; age class 4, >85 y.
| Months (mean with 95% CI) | Difference | 60 months | 120 months | 180 months | ||
|---|---|---|---|---|---|---|
| Elective SAVR (years) | ||||||
| <70 | 170 (158–182) | 89.0 ± 1.9% | 73.4 ± 3.8% | 47.1 ± 4.2% | ||
| 70–75 | 140 (133–147) | 30 | 86.6 ± 1.6% | 59.8 ± 2.3% | 28.0 ± 2.5% | |
| 75–80 | 117 (112–123) | 23 | 78.1 ± 1.8% | 48.0 ± 2.2% | 17.3 ± 1.9% | |
| 80–85 | 89 (84–94) | 28 | 70.3 ± 2.3% | 29.2 ± 2.4% | 3.9 ± 1.4% | |
| >85 | 84 (73–95) | 5 | 63.5 ± 4.9% | 19.5 ± 4.3% | 2.9 ± 2.6% | |
| Urgent SAVR (years) | ||||||
| <70 | 137 (113–161) | 77.4 ± 5.1% | 53.7 ± 7.7% | 39.4 ± 11.0% | ||
| 70–75 | 120 (104–136) | 17 | 72.2 ± 5.0% | 52.7 ± 5.7% | 24.1 ± 5.7% | |
| 75–80 | 97 (85–109) | 23 | 67.6 ± 4.8% | 34.4 ± 5.0% | 7.9 ± 3.5% | |
| 80–85 | 77 (67–87) | 20 | 55.2 ± 5.3% | 15.5 ± 4.1% | 5.4 ± 2.9% | |
| >85 | 59 (45–74) | 18 | 46.7 ± 9.1% | 6.7 ± 4.6% | None | |
SAVR, surgical aortic valve replacement; 95% CI, 95% confidence interval.
| Age class | 1 month | 60 months | 120 months | 180 months |
|---|---|---|---|---|
| 0 | 274 | 242 | 138 | 44 |
| 1 | 465 | 399 | 245 | 71 |
| 2 | 552 | 431 | 222 | 53 |
| 3 | 384 | 270 | 103 | 6 |
| 4 | 95 | 61 | 15 | 2 |
| Age class | 1 month | 60 months | 120 months | 180 months |
|---|---|---|---|---|
| 0 | 53 | 41 | 16 | 4 |
| 1 | 78 | 57 | 36 | 10 |
| 2 | 95 | 64 | 30 | 4 |
| 3 | 87 | 48 | 11 | 2 |
| 4 | 29 | 14 | 2 | None |
Figs. 3,4 and Tables 12,13 demonstrate, stratified by elective status, the combined effect of age on 30-day and long-term mortality. Under elective conditions, there was no significant age effect in the younger age groups (0–2) on short-term outcomes, whereas an age effect on hospital mortality was observed in the older age groups (3–4). Under urgent conditions, a higher 30-day mortality was observed across all age groups, but the results are catastrophic for patients aged 85 years and older (category 5).
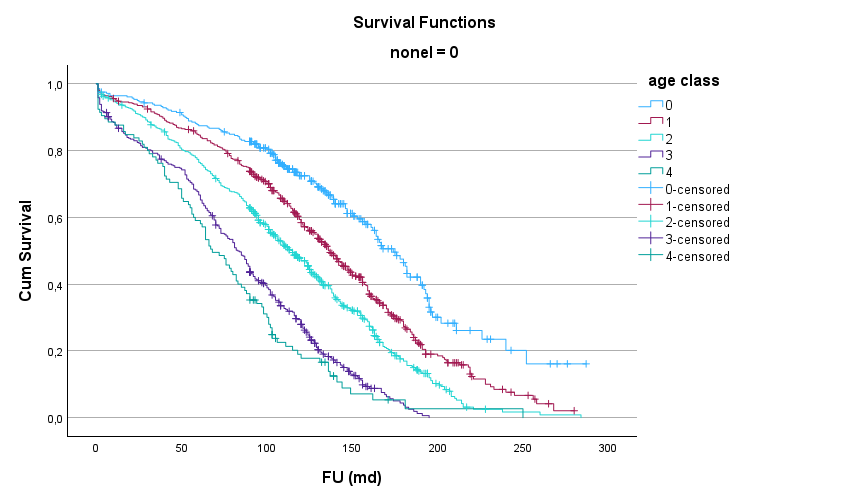 Fig. 3.
Fig. 3.Effect of age categories for elective SAVR on 30-day and long-term mortality. Cum survival, cumulative survival; FU (md), follow-up in months; nonel = 0, elective; age class 0, <70 y; age class 1, 70–75 y; age class 2, 75–80 y; age class 3, 80–85 y; age class 4, >85 y.
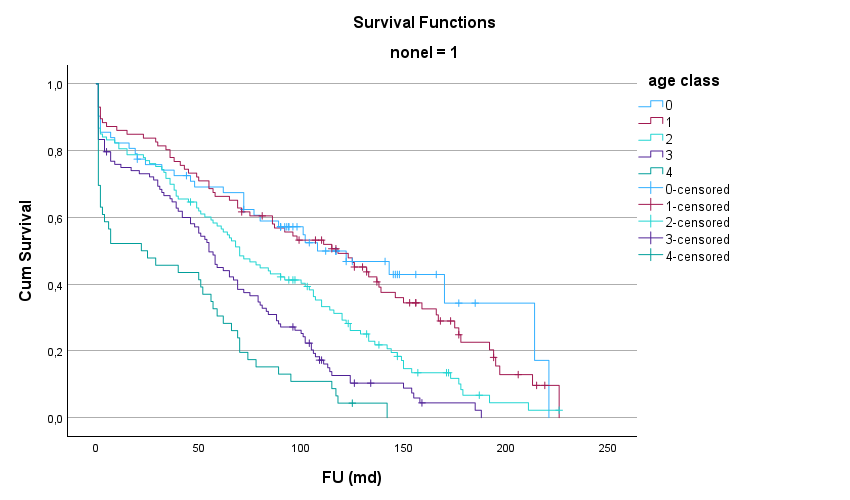 Fig. 4.
Fig. 4.Effect of age categories on 30-day and long-term mortality after urgent SAVR. Cum survival, cumulative survival; FU (md), follow-up in months; nonel = 1, urgent; age class 0, <70 y; age class 1, 70–75 y; age class 2, 75–80 y; age class 3, 80–85 y; age class 4, >85 y.
| Age class | 1 month | 60 months | 120 months | 180 months |
|---|---|---|---|---|
| 0 | 279 | 242 | 136 | 43 |
| 1 | 476 | 399 | 245 | 71 |
| 2 | 564 | 431 | 222 | 53 |
| 3 | 405 | 270 | 103 | 6 |
| 4 | 104 | 62 | 15 | 2 |
| Age class | 1 month | 60 months | 120 months | 180 months |
|---|---|---|---|---|
| 0 | 61 | 41 | 16 | 3 |
| 1 | 85 | 57 | 36 | 10 |
| 2 | 112 | 64 | 30 | 4 |
| 3 | 107 | 48 | 11 | 1 |
| 4 | 45 | 14 | 2 | 0 |
Table 14 shows the predictors of long-term mortality for the overall patient group and after stratification by elective status. Ages over 80 and COPD were the only consistent predictors. Ages over 80 years remained the dominant predictor, with an odds ratio greater than two.
| Predictor | All patients | Elective SAVR | Urgent SAVR | |||
|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Aged >80 years | 2.19 | 1.82–2.63*** | 2.25 | 1.83–2.76*** | 2.11 | 1.55–2.87*** |
| Malignancy | 1.26 | 1.00–1.58* | 1.31 | 1.02–1.69* | - | - |
| COPD | 1.35 | 1.08–1.70** | 1.36 | 1.05–1.74* | 1.73 | 1.23–2.42** |
| LVEF <50% | 1.33 | 1.09–1.64** | 1.51 | 1.20–1.91*** | - | - |
| PAD | 1.58 | 1.29–1.93*** | 1.60 | 1.29–2.00*** | - | - |
| CKD | 1.43 | 1.15–1.78** | 1.53 | 1.21–1.94*** | - | - |
| NYHA class III/IV | 1.46 | 1.20–1.78*** | 1.45 | 1.18–1.79*** | - | - |
| Atrial fibrillation | 1.25 | 1.03–1.53* | - | - | 1.62 | 1.20–2.20** |
| Incomplete revascularization | 1.34 | 1.03–1.75* | - | - | 1.79 | 1.04–3.08* |
CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; LVEF, left ventricular ejection fraction; NYHA, New York Heart Association; OR, odds ratio; 95% CI, 95% confidence interval; PAD, peripheral artery disease; ***, p < 0.001; **, p < 0.01; *, p < 0.05.
Several observations can be made from this investigation. The rate of patients requiring urgent surgery was closely similar to that reported in recent studies [9,10]. The likelihood of requiring urgent SAVR was higher in patients aged 80 years or older and, even higher in those aged 85 years or older, although this was observed only in the univariate analysis. This age effect has been reported previously [7]. The main predictors of urgent SAVR were endocarditis, prior episodes of congestive heart failure, myocardial infarction, and involvement of the left main coronary artery. For the latter two factors, severe CAD was often the indication for cardiac surgery, which also included CABG. In the current series, CKD and pulmonary disease were non-cardiac predictors. The need for urgent SAVR was associated with increased resource use, most postoperative adverse events, and, most significantly, with 30-day mortality. The 30-day mortality rate increased significantly in patients aged over 80 years and even more so in those aged over 85 years. Stratification by elective status showed that the age-related increase in mortality among patients undergoing elective SAVR was less pronounced. In the urgent patient group, 30-day mortality was much higher at all ages, but became catastrophic in patients older than 85 years. The need for urgent SAVR was the dominant predictor of 30-day mortality, followed by age >80 years. A similar finding was reported previously in patients undergoing SAVR with or without CABG [11]. In subsequent logistic regression analyses stratified by the three age groups, the need for urgent SAVR was the strongest and only common predictor of 30-day mortality. Conversely, after stratification by elective status, age >80 years was the strongest predictor. Unsurprisingly, long-term survival was affected by age and the need for urgent SAVR. The incremental decrease in survival across 5-year age classes was comparable to the decrease in survival attributable to the need for urgent SAVR. Additionally, the effect of a need for urgent surgery has had a devastating effect on global postoperative mortality in older patients, especially in those aged 85 years and older.
The importance of timely aortic valve replacement is underscored by the risk of rapid functional deterioration in patients with untreated severe AS and should be emphasized [12]. Meanwhile, a reasonable assumption is that delayed diagnosis or treatment of aortic valve disease is also an important factor in the decreased compensatory mechanisms of the left ventricle to maintain adequate circulation, ultimately resulting in the need for urgent valve replacement. A recent review showed that only about half of patients with symptomatic severe AS underwent aortic valve replacement within 2 years of diagnosis. Among patients with normal LVEF and a class I indication for aortic valve replacement, either by TAVI or SAVR, only 70% received a timely valve prosthesis. In patients with reduced LVEF, this proportion was only 53%. For patients with low-flow, low-gradient AS, the percentages were even lower [13]. Several reasons for delayed valve replacement have been identified, including diagnostic barriers such as uncertain symptomatic status, doubtful clinical significance of a cardiac murmur, and delayed transfer to a cardiac center after a non-cardiologist ordered a transthoracic echocardiography. Treatment barriers, such as delayed transfer, inadequate reimbursement, unavailability of intensive care unit (ICU) beds, or perceived futility of valve replacement, may also contribute to a delayed valve replacement [13,14]. Patient-related factors, including advanced age and comorbid conditions such as a history of stroke, COPD, low LVEF, CAD, diabetes, and obesity [15,16], as well as refusal of surgery by patients [17], could also delay adequate treatment of valve disease. Deprivation, accompanied by low health index scores, has also been a serious issue in some regions and countries [9,10,18]. Delayed SAVR in patients with AS may result in higher preoperative mortality [14,19]. Previous studies have shown that delayed SAVR, high New York Heart Association (NYHA) functional class, and advanced age were associated with increased early postoperative and long-term mortality. This effect was already apparent after only a 3-month delay in treatment. The NYHA functional class appears to be independent of treatment delay; the effect of delay is more pronounced in patients with CAD [14].
Factors associated with the need for urgent valve replacement appear to parallel those associated with delayed valve replacement. Heart failure, with or without endocarditis, reduced LVEF, and cardiogenic shock have all been reported as reasons for urgent intervention [9,20,21,22]. For TAVI, procedural success and adjusted 30-day mortality were comparable to those in elective cases, but 1-year mortality was higher in urgent cases [23]. The urgency of TAVI can also be illustrated by the IMPACT score, which enables accurate risk stratification and identifies patients who require urgent intervention [24]. The presence of advanced symptoms and the need for urgent or emergent intervention were associated with an increased postoperative mortality rate [9,10]. The overall length of stay and ICU-related financial costs were also higher, whereas those for discharge to home were lower [9]. The need for urgent TAVI was associated with higher 30-day mortality [20,25,26] and 1-year mortality [25]. Initial refusal of TAVI was also associated with worse outcomes. However, age, surgical risk scores, and frailty were higher in the refusal group than in the non-refusal group [17], making interpretation of these findings more difficult. Nevertheless, valve replacement by either method is feasible under urgent conditions.
Since this is a retrospective series, some inherent limitations should be noted. The risk of selection bias was reduced by the consecutive inclusion of all patients undergoing SAVR with a biological valve. Patients with an unknown elective status were excluded from this analysis. Since this group underwent SAVR before 2000, this could have introduced bias. However, the rate of urgent SAVR need and long-term outcomes did not change significantly over time, thereby reducing the risk of inclusion bias. The most important preoperative comorbid conditions were included in the analysis, although this could raise concerns about unadjusted multiple comparisons. This issue is partly addressed by the identification of independent predictors of urgent SAVR. Patients requiring urgent SAVR were not separated from those needing emergency surgery (i.e., those requiring surgery within hours of admission), as doing so would have complicated the analysis. The changes in operative techniques and improvements in perioperative care over the long inclusion period were not considered in the analysis. Earlier published results showed that, over time, patient age, comorbidity rate, and surgical complexity increased, accompanied by a concomitant, but non-significant increase in early mortality, without affecting long-term survival [27]. These findings applied to both isolated SAVR and SAVR combined with another procedure, such as CABG. However, the effects of increased surgical complexity and improved operative techniques and perioperative care could not be disentangled. Patient refusal, health deprivation indices, ethnicity, and socioeconomic status as possible reasons for delay were not investigated. The major strengths of this study are the large sample size, stratified analysis, long follow-up duration, and parallel identification of outcome predictors across age categories by elective status.
This study has some strengths but also some limitations, which are due to its retrospective and observational character. The patient charts are not designed for collecting research data, and some information may be missing. However, this reflects the 'real world' character of this study. Retrospective and observational studies can only identify associations. Nevertheless, some causal relation between the need for urgent surgery and the outcome can be assumed by the timeline: the need for urgent surgery precedes mortality. Any selection bias has been minimized by the consecutive inclusion of the patients and of scrutinizing of all available medical data in the files. The elective status was derived from referral letters, the timeline between diagnosis and surgery as well as from discharge reports. This information could be retrieved with certainty in about 90% of the patients. Loss of follow-up with respect to survival was reduced to zero by accessing the national mortality register. Confounding variables included all major comorbid conditions and were taken into account by a multivariate analysis. Additionally, this analysis was performed for patients operated under urgent and elective conditions separately.
The need for urgent SAVR was predicted mainly by cardiac factors. The need for urgent SAVR was associated with an increased 30-day mortality, postoperative complication rate, and need for resources. The effect on mortality was most marked in the older age groups. Age and need for urgent SAVR were the most important independent predictors of 30-day mortality. The need for urgent SAVR also reduced long-term survival by approximately 2 years across all age classes. The need for urgent SAVR has devastating effects on older patients who appear to be particularly vulnerable to this condition. Thus, improved screening efforts for aortic valve disease and timely treatment may reduce adverse postoperative outcomes, the need for postoperative resources, and improve long-term survival. Specifically, valve replacement in older patients, once indicated, should not be postponed until all cardiac mechanisms required to maintain adequate circulation have been exhausted.
The results were derived from a database which is still under development. Future publications will be prepared. For this reason, these data cannot be publicly made available.
Conceptualization, WM; methodology, WM and ID; formal analysis, WM and ID; investigation, WM, ID, KD and AV; data curation, WM, ID, KD and AV; writing—original draft preparation, WM; writing—review and editing, WM, ID, KD and AV. All authors have read and agreed to the published version of the manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study was approved by the Ziekenhuis Netwerk Antwerpen (ZNA) ethical committee under the protocol N.2656. The study was carried out in accordance with the guidelines of the Declaration of Helsinki. The informed consent was waived because of the retrospective character of the study.
Not applicable.
This research received no external funding.
The authors declare no conflicts of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.