




 , Pengbo Liu 1,†, Yongzhi Deng 2,*
, Pengbo Liu 1,†, Yongzhi Deng 2,*
1 Department of Cardiovascular Surgery, The Affiliated Hospital of Shanxi Medical University, Shanxi Cardiovascular Hospital (Institute), Shanxi Clinical Medical Research Center for Cardiovascular Disease, 030024 Taiyuan, Shanxi, China
2 Department of Cardiovascular Surgery, Shanxi Cardiovascular Hospital (Institute), The Affiliated Hospital of Shanxi Medical University, Shanxi Clinical Medical Research Center for Cardiovascular Disease, 030024 Taiyuan, Shanxi, China
†These authors contributed equally.
Abstract
Postoperative atrial fibrillation (POAF) is the most common arrhythmia following coronary artery bypass grafting (CABG) and is associated with increased morbidity, mortality, and reduced long-term survival. Inflammation plays a central role in POAF pathogenesis, with interleukin-6 (IL-6) acting as a key mediator of postoperative inflammatory signaling. The multifactorial pathophysiology of POAF involves atrial structural remodeling, autonomic imbalance, and electrophysiological alterations. Elevated IL-6 levels contribute to atrial fibrosis and remodeling, creating a vulnerable substrate that promotes atrial fibrillation initiation and maintenance. Atrial fibrosis represents a critical mechanistic link between inflammation and POAF development, suggesting shared proarrhythmic pathways with other forms of atrial fibrillation. Established clinical predictors of POAF include advanced age, end-stage renal disease, hypertension, obesity, and left atrial enlargement. Emerging preventive strategies, such as partial cardiac autonomic denervation, posterior pericardiotomy, and calcium chloride injection into atrial ganglionated plexi, have demonstrated significant reductions in POAF incidence without additional procedural risk. Pharmacological approaches, including prophylactic corticosteroids, may further reduce POAF rates in selected patients. Clinically, POAF is associated with increased risk of stroke, prolonged hospitalization, heart failure exacerbation, and higher short- and long-term mortality, underscoring the importance of improved risk stratification and effective preventive strategies following CABG.
Keywords
- postoperative atrial fibrillation
- coronary artery bypass graft
- partial cardiac denervation
- atrial fibrillation
- inflammation
- structural remodeling
- IL-6
Postoperative atrial fibrillation (POAF) is the most common arrhythmia following coronary artery bypass grafting (CABG), its prevalence is 15–45% and is associated with poor long-term prognosis [1]. Its occurrence is associated with increased morbidity and mortality, including prolonged hospitalization, heightened risk of reoperation, greater inotrope requirement, persistent congestive heart failure (CHF), and diminished long-term survival [2]. Despite advances in surgical and perioperative care, POAF continues to pose a significant clinical burden. The underlying mechanisms of POAF remain incompletely understood; however, accumulating evidence implicates systemic inflammation and atrial structural remodeling as central contributors [3]. Among inflammatory mediators, interleukin-6 (IL-6) has emerged as a key player in POAF pathogenesis. IL-6 not only orchestrates the acute inflammatory response but also promotes atrial fibrosis by stimulating fibroblast collagen production [4] (Fig. 1). Experimental models of sterile pericarditis have shown that IL-6 dysregulates intracellular calcium handling, creating an electrophysiological substrate conducive to atrial arrhythmogenesis [5].
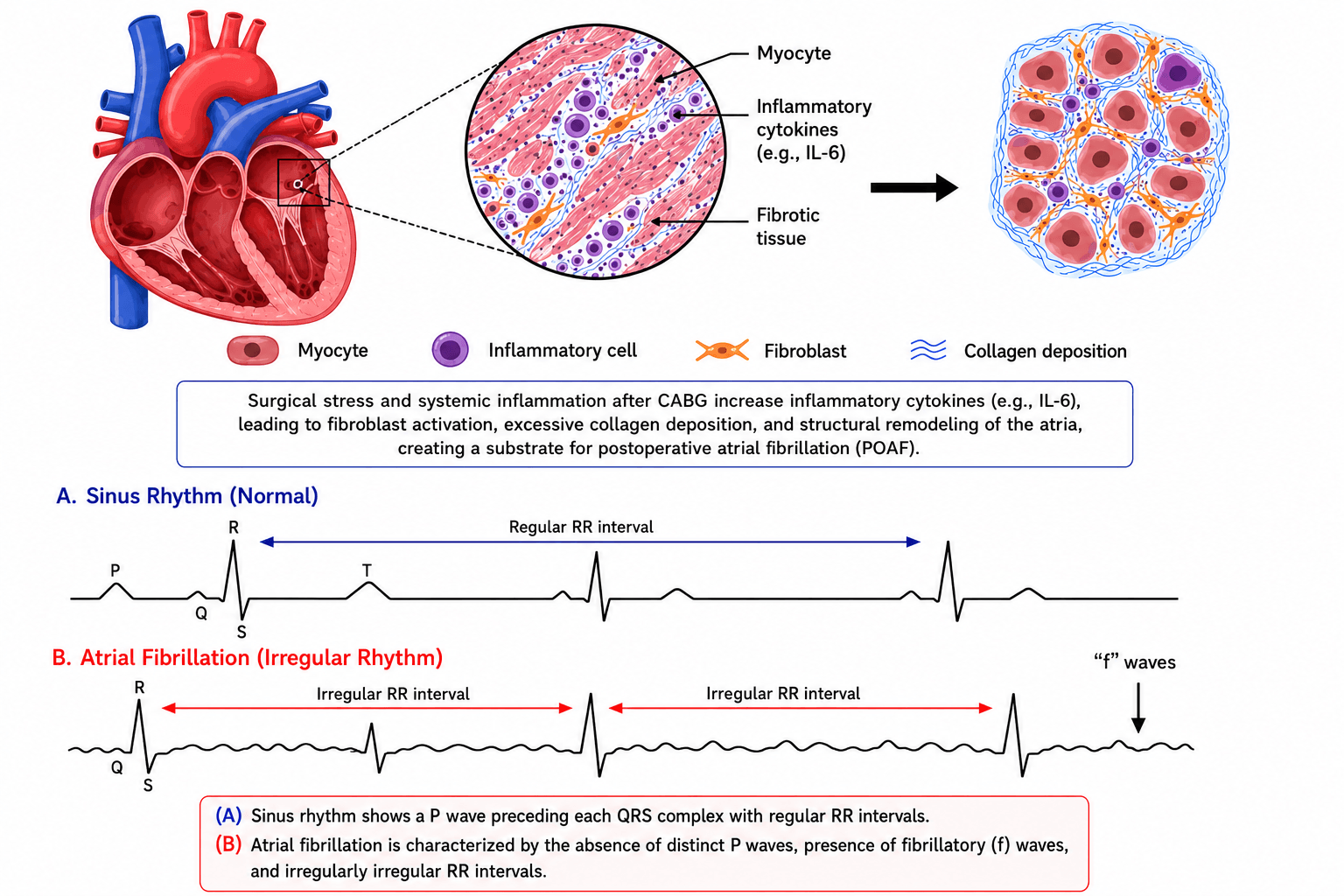 Fig. 1.
Fig. 1.Inflammatory cytokine IL-6 plays role in development of POAF via modulation of TGF-β1, leading to structural remodeling, especially cardiac fibrosis. IL-6, Interleukin-6; POAF, Postoperative atrial fibrillation; TGF-β1, Transforming growth factor beta 1. Comparison of normal sinus rhythm and atrial fibrillation on electrocardiogram (ECG). Sinus rhythm demonstrates regular R–R intervals with organized P waves preceding each QRS complex. In contrast, atrial fibrillation is characterized by irregular R–R intervals, absence of distinct P waves, and the presence of fibrillatory (f) waves, reflecting disorganized atrial electrical activity.
Clinical risk factors for POAF include advanced age, hypertension, obesity, impaired renal function and increased left atrial size all of which may exacerbate the pro-inflammatory and fibrotic milieu [6]. Additionally, perioperative elements such as cardiopulmonary bypass and prolonged perfusion times further elevate the risk. Given its frequency and prognostic impact, there is a growing focus on effective prophylaxis and treatment strategies. Established pharmacological agents like β-blockers and amiodarone remain first-line therapies. Recent innovations include partial cardiac autonomic denervation via excision of the ligament of Marshall and fat pad resection along the Waterston groove as well as calcium chloride injections into atrial ganglionated plexi, both approaches have demonstrated substantial reductions in POAF incidence without added risk [7]. Prophylactic corticosteroids and right atrial pacing have also shown promise in select populations [8].
This review synthesizes the current understanding of POAF in the context of CABG, with a particular focus on inflammatory mechanisms involving IL-6, clinical risk stratification, and the evolving landscape of preventive and therapeutic strategies.
A comprehensive literature search was conducted using PubMed, Scopus, and Web of Science databases for studies published up to 2025. Search terms included combinations of “postoperative atrial fibrillation”, “coronary artery bypass grafting”, “inflammation”, “interleukin-6”, “cardiopulmonary bypass”, and “prevention”. Both experimental and clinical studies, including randomized controlled trials, observational studies, and relevant systematic reviews, were considered. Reference lists of included articles were manually screened to identify additional relevant publications. Only English-language articles were included.
The inflammatory process is a significant and common pathological reaction after coronary artery bypass graft surgery. The acute postoperative inflammatory response may be of great importance in the induction and maintenance of the POAF [9]. Studies measuring IL-6, C-reactive protein (CRP) and complement levels in the blood of CABG patients show an increase in serum levels, which occurs at approximately the same time as the peak incidence of POAF. This was the first evidence suggesting an association between serum levels of inflammatory factors and POAF. Meanwhile, clinical observations and animal studies further support a significant synergistic relationship between inflammation and POAF [10]. Reviews indicate that IL-6 is the most commonly studied cytokine, and cited studies generally show an association between elevated circulating IL-6 levels and the development of POAF [11,12]. However, some studies found no significant association between peripheral venous IL-6 levels and the risk of POAF. In contrast, elevated IL-6 concentrations were detected at intracardiac sites, including the left atrial appendage, right atrial appendage, and left atrial tissue, suggesting a strong local relationship between cardiac IL-6 signaling and POAF development. This review investigates the association between POAF and local cardiac IL-6 levels. Pericardial fluid analysis has been recognized as superior to serum analysis for measuring molecular changes in the early postoperative period after cardiac surgery [13]. Pericardial fluid consists of plasma ultrafiltrate from epicardial capillaries, secretions from pericardial mesothelial cells and fluid from the myocardial interstitium [14]. Unlike serum and peripheral blood, locally produced proteins in pericardial fluid can be present at different concentrations [13]. Researchers have conducted studies on the association between IL-6 in pericardial effusion and POAF. In one study involving two stages, 302 and 207 CABG patients were recruited into derivation and validation groups, respectively. An IL-6 concentration in pericardial fluid samples >166 ng/mL at 12 hours postoperatively after tracheal extubation was one of the six components in the final POAF prediction tool. The AUC of the model was 0.78 and 0.77 in the derivation and validation cohort, respectively. This predictive value was considered to be significantly improved by including IL-6 measurements in pericardial fluid [15]. These findings indicated that high levels of IL-6 in pericardial fluid post-CABG are related to POAF. These findings have been corroborated by simulated CABG surgery in wild-type mice, where elevation of IL-6 levels in the pericardial fluid was associated with the development of POAF [16]. The relationship was further validated in IL-6 knockout mice, with POAF in IL-6 knockout mice, which showed a dramatic decrease in POAF following simulated CABG surgery. All of those findings indicate a potentially causal association between IL-6 levels and POAF [16].
Cardiac fibrosis is caused by an imbalance between fibrillar collagen synthesis and turnover, leading to excessive, impaired collagen deposition and altered collagen type distribution (increased deposition of type Ⅰ/Ⅲ collagen ratios). This process involves connective tissue filling material that serves as a scaffold for new blood vessel generation, fibrin deposition, and chaotic juxtaposition of collagen fibers [17,18]. Changes in the ratio of type Ⅰ to type Ⅲ collagen expression have been demonstrated to affect the elasticity/stiffness of the heart and, consequently, the propensity for AF [19]. Upregulation of type Ⅰ and type Ⅲ collagen and fibronectin has been observed in the left atrial tissue of patients with AF [20], and the ratio of type Ⅲ to type Ⅰ collagen was also markedly reduced [21]. Although a direct linear relationship is complex, accumulating experimental and clinical evidence supports a contributory role of IL-6-mediated fibrosis in POAF. POAF development is further facilitated by structural remodeling processes. Age-related changes, such as myolysis, create circuits required for re-entry, which is necessary for arrhythmogenesis [22]. Fibrosis biomarkers, such as pro-collagen Ⅰ and pro-collagen Ⅲ peptide, correlate significantly with predicting the risk of POAF and responses to therapies aimed at profibrotic pathways, such as inhibition of microRNA-21 [23]. Recent studies found that upregulation of IL-6 similar interleukins in the circulation post-CABG surgery is associated with decreased atrial periostin production and increased atrial collagen production in mice. This increase in collagen synthesis is also observed in patients following valve surgery, suggesting a possible association between IL-6 and increased collagen synthesis in atrial tissue. In a parallel study [24], colchicine was shown to prevent atrial fibrosis in a rat sterile pericarditis model and inhibit POAF promotion by preventing IL-1β-induced IL-6 release. Collagen types Ⅰ and Ⅲ are regulated by matrix-controlled degradation involving matrix metalloproteinases (MMPs) and tissue inhibitors of metalloproteinases (TIMPs). This tissue remodelling is regulated by upstream signals, predominantly transforming growth facor-beta (TGF-β1), which is regarded as a profibrotic factor. TGF-β1 can inhibit the production of MMP-2 and MMP-9 while upregulating TIMP expression. These activities inhibit degradation and result in increased collagen content in the extracellular matrix [25]. Studies have shown that increased level of IL-6 are sufficient to cause myocardial fibrosis, probably mediated by an upregulation of TGF-β1 signaling [26]. Furthermore, it has been well documented that IL-6 induces a STAT3-dependent enhancement of TGF-β signaling, which stimulates fibrosis via upregulation of Smad3 activation [27]. These findings suggest an interaction between IL-6-STAT3 signaling and the TGF-β signaling. A key role of TGF-β in the induction of organ fibrosis has been implicated [28]. TGF-β1 is the major subtype in the TGF-β family and is synthesized by cardiac fibroblasts, myofibroblasts and cardiomyocytes [29]. It has been demonstrated that TGF-β1 plays a role in the fibrosis in vivo. Additionally, myofibroblasts are considered a detrimental factor in cardiac remodelling [30]. TGF-β is important in cardiac remodeling, especially cardiac fibrosis, where it may promote myofibroblast conversion and collagen synthesis [30]. Although TGF-β1 transgenic mice do not exhibit spontaneous AF, they show inducible AF on burst pacing [31]. Increased TGF-β1 in surgery patients has been identified as an independent risk factor for POAF [32]. A correlation between TGF-β transcription levels and the development of POAF in patients who underwent cardiac surgery has also been reported. Based on overwhelming evidence, IL-6 could play a role in the development of POAF via modulation of TGF-β1, influencing the differentiation of fibroblasts to myofibroblasts and increasing collagen protein synthesis. However, this association is poorly characterized and merits further investigation.
The pathophysiology of new-onset POAF after CABG is complex affected by a number of patient, surgical, and biochemical factors [33,34,35]. POAF arises from a multifactorial combination of structural, electrophysiological, and systemic changes triggered by cardiac surgery. Its etiology reflects contributions from pre-existing patient factors, surgical techniques, and postoperative responses, culminating in complications such as thromboembolic events and hemodynamic instability. While often self-limiting, POAF significantly increases morbidity, prolongs hospital stays, and elevates the mortality risk [36,37].
Crucial structural remodelling, such as increased left atrial diameter and reduced left ventricular ejection fraction, directly contributes to POAF. Enlargement of the left atrium and ventricular dysfunction both provide substrates for arrhythmogenesis, allowing the atria to stretch and fibrose, and disrupting normal conduction [38,39]. Preoperative echocardiographic parameters, especially a global peak atrial longitudinal strain (PALS) below 28%, have been established as independent predictors of POAF, especially in elderly patients [40].
Sympathetic nervous system activation is also an important mechanism in the development of POAF. Elevated postoperative norepinephrine concentration, a sign of increased sympathetic tone, is an independent predictor of POAF. This increase in adrenergic activity elevates the sinus rate and atrial ectopic activity, predisposing to arrhythmias. The importance of sympathetic activation is also indicated by the efficacy of β-blockers in the prevention of POAF [41].
Metabolic disturbances, such as postoperative hyperglycemia and electrolytic disorders (particularly hypokalemia), have also been implicated in the mechanism of POAF. Elevated serum glucose and hypokalemia are important risk factors, likely due to their impact on atrial electrophysiology and electrophysiological vulnerability to arrhythmias [41]. Various risk factors for POAF have been identified in comparative studies, including advanced age, CPB use, large left atrial size, low left ventricular ejection fraction, a history of myocardial infarction, and use of an intra-aortic balloon pump [42,43]. Clinical and perioperative risk factors associated with POAF after CABG are summarized in Table 1 [34,44,45,46]. A standardized model incorporating other POAF predictors, such as left ventricular end-diastolic diameter, intraoperative defibrillation, and temporary pacing lead implantation, has been developed and provides improved predictive performance over available models (e.g., H, Hypertension; A, Age >75 years; T, Transient ischemic attack (TIA) or stroke; C, Chronic obstructive pulmonary disease (COPD); H, Heart failure (HATCH) and C, Congestive heart failure; H, Hypertension; A2, Age ≥75 years (2 points); D, Diabetes mellitus; S2, Stroke/TIA/thromboembolism (2 points); V, Vascular disease; A, Age 65–74 years; Sc, Sex category (female) (CHA2DS2-VASc)) [47].
| Risk factor | Association with POAF | Evidence/Effect size |
|---|---|---|
| Advanced age | Strong ↑ risk | OR 1.5–2.0 per decade [44] |
| Left atrial enlargement | Strong ↑ risk | OR 2.0–3.5 |
| Reduced LVEF | Moderate ↑ risk | OR 1.4–2.0 [46] |
| Hypertension | Moderate ↑ risk | OR ~1.3–1.6 |
| Obesity | Moderate ↑ risk | OR ~1.2–1.5 [44] |
| End-stage renal disease | Strong ↑ risk | OR ~2.0–3.0 [45] |
| Cardiopulmonary bypass | Moderate ↑ risk | Higher vs off-pump CABG [34] |
| Inflammation (IL-6, CRP) | Emerging predictor | Independent association |
OR, odds ratio; LVEF, left ventricular ejection fraction; CABG, coronary artery bypass grafting; CRP, c-reactive protein. “↑” indicates increase.
Additional perioperative factors, such as hypertension, renal insufficiency, prolonged CPB time, and high postoperative drainage, increase the risk [48,49]. Consequently, POAF post-CABG results from a mixture of structural atrial remodeling, enhanced inflammation and oxidative stress, sympathetic activation, and metabolic derangements, all interacting to create a proarrhythmic substrate in the postoperative period [38,41,49]. Multicenter studies analyzing results in CABG patients with and without POAF have been conducted on a large scale. One study of nearly 20,000 patients determined that patients who developed POAF were generally older and had more comorbidities, including heart failure, hypertension, cerebrovascular disease, End-Stage Renal Disease (ESRD) and renal insufficiency. POAF was associated with increased 30-day mortality in univariate analysis, but not in multivariate analysis after controlling for confounders. However, POAF was still found to be an independent predictor for perioperative complications, such as permanent stroke, new renal failure, infections, gastrointestinal complications, requirement for reoperation, and decreased in long-term survival [50]. Another large registry study demonstrated that, although POAF was not an independent predictor of long-term mortality after hospital discharge, it was significantly associated with an increased risk of ischemic stroke and an almost tenfold higher risk of major bleeding during five-year follow-up after multivariable adjustment.
Inflammation and oxidative stress play key roles in the development of POAF. These phenomena are augmented by Cardiopulmonary Bypass (CPB) and surgical injury. CPB significantly increase the levels of inflammatory indicators, such as IL-6 and TNF-α, enhances Neutrophil-to-lymphocyte ratio and Pan-immune inflammation value, which are associated with adverse outcomes like prolonged ICU stays [51]. Increased neopterin, a biomarker of cellular immune response and oxidative stress, has been identified as an independent risk factor for POAF, suggesting that preoperative inflammation raises the susceptibility to arrhythmias [33]. Surgical trauma, CPB, and tissue injury contribute to this inflammatory response, promoting atrial electrical instability [34]. Del Nido cardioplegia (DNC) has been shown to reduce markers of myocardial injury, including troponin and creatine kinase–MB, compared with traditional cardioplegic strategies. Several observational studies have suggested a lower incidence of POAF with DNC; however, results remain inconsistent across trials and study populations. At present, available evidence supports a potential myocardial protective effect of DNC, but its role in consistently reducing POAF has not been definitively established and warrants confirmation in adequately powered randomized studies [37]. Remarkably, the incidence of POAF is higher in on-pump CABG compared with off-pump surgery (29.09% vs 10.74%). This difference suggests a potential role of cardiopulmonary bypass in amplifying systemic inflammation and oxidative stress, particularly in high-risk patients with comorbidities such as hypertension or in those requiring vasopressor support [52,53]. POAF is driven by a complex interplay of systemic inflammation and oxidative stress following cardiac surgery. These processes promote structural remodeling, including fibrosis and atrial dilation, along with electrophysiological alterations such as conduction heterogeneity and ion channel dysfunction, ultimately predisposing to arrhythmogenesis (Fig. 2).
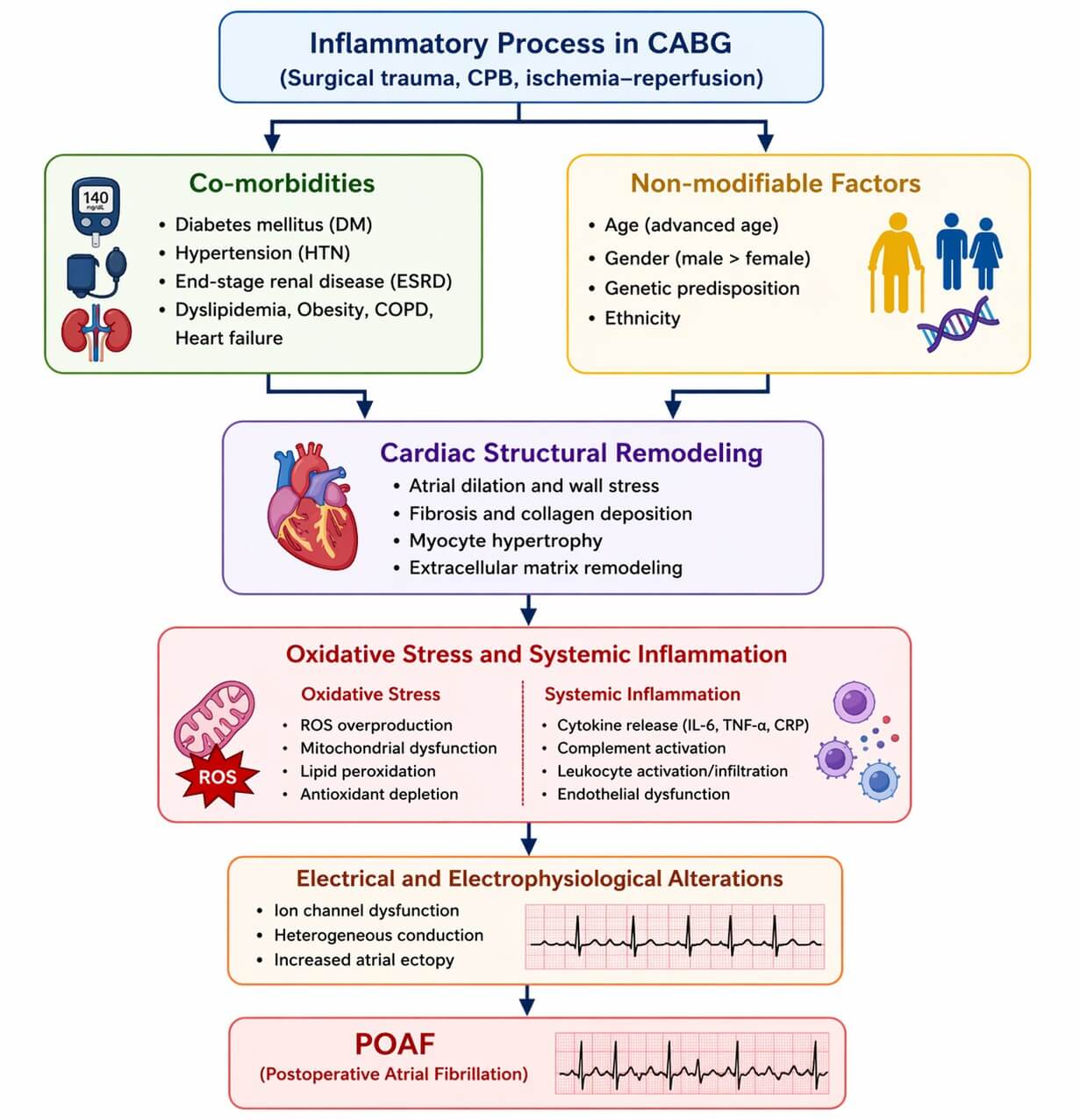 Fig. 2.
Fig. 2.Overview of the inflammatory and structural mechanisms underlying postoperative atrial fibrillation (POAF). Surgical stress, cardiopulmonary bypass, and ischemia–reperfusion injury trigger systemic inflammation and oxidative stress. These processes promote cardiac structural remodeling, including fibrosis, atrial dilation, and extracellular matrix expansion, along with electrophysiological alterations such as ion channel dysfunction and conduction heterogeneity, ultimately leading to POAF.
Several randomized controlled trials have assessed different interventions to prevent POAF. Partial cardiac denervation by sectioning the ligament of Marshall (LOM) and excising a fat pad at the Waterston groove significantly reduces POAF (18.1% vs 31.6%) without additional morbidity or cost compared to traditional CABG [54]. A second Randomized Controlled Trail (RCT) showed that prophylactic steroid administration reduced the incidence of POAF (21% vs 51% with placebo), but the number of minor complications was greater in the steroid group [55].
Elective cardioversion, both electrical and pharmacological, is usually delayed after surgery unless the patient is unstable. The management of anticoagulation is controversial, and there is no clear benefit of early anticoagulation in reducing thromboembolic risk after POAF; it may even increase the risk of bleeding [56,57].
The cardiac autonomic nerve system (CANS) is crucial in the onset of POAF [58]. Despite this, the occurrence of POAF after CABG remains at 21.1%, even with the prevalent use of β-blockers, which are known for their capacity to reduce cardiac sympathetic activity and are the sole class Ⅰ drugs currently endorsed by guidelines for POAF prevention [59]. The intrinsic CANS mainly comprises ganglia and associated nerves located in the epicardial adipose tissue (EAT) that encases the primary cardiac arteries and veins, including the ligament of Marshall (LOM) and the fat pad along the Waterston groove [60]. It is thought that activation of the CANS within the EAT may contribute to the onset of atrial fibrillation (AF), which supports the rationale for the surgical technique involving the division of the LOM and excision of the fat pad along the Waterston groove during the Maze procedure designed to address AF [61]. Consequently, randomized trials have demonstrated that partial cardiac denervation by dividing the ligament of Marshall and dissecting out the fat pad in the Waterston groove reduced the incidence of POAF without an increase in postoperative morbidity or cost [54]. This operation can be offered as a supplemental procedure in specific patient groups undergoing conventional CABG.
Prophylactic pacing of the right atrium in the early postoperative phase has been shown to significantly decrease the rate of POAF [62]. The limited effectiveness of pharmacological interventions in preventing post-CABG AF has prompted investigations into other preventive approaches [63]. Atrial pacing might effectively decrease bradycardia-associated AF and could positively impact intra-atrial conduction, atrial refractoriness, and the occurrence of atrial extrasystoles [64]. We conducted a thorough review of the clinical trial evidence available in the literature concerning the effectiveness of epicardial atrial pacing in preventing AF following CABG [65]. Study populations varied between 21 and 161 participants. Most trials focused on patients receiving isolated CABG. In four of these trials, as many as 15% of patients received valve surgery, either individually or alongside CABG [66]. The comparisons in the trials involved a control group and interventions that included right atrial pacing (RAP), biatrial pacing (BAP) [63,64,67,68], or a combination of both RAP and BAP [66]. However, more extensive trials are needed to substantiate these findings.
Posterior pericardiotomy (PP) is a surgical technique designed to facilitate drainage of the pericardial space into the left pleural cavity [69]. The procedure involves creating a 4–5 cm vertical incision located posterior to the left phrenic nerve, extending from the left inferior pulmonary vein to the diaphragm (Fig. 3) [70]. Before separation from cardiopulmonary bypass, the heart is gently elevated, and a pericardial fold is grasped using two forceps. An incision is then made with diathermy, starting at the level of the inferior pulmonary vein and extending inferiorly to the diaphragmatic attachment of the pericardium [70]. Subsequently, a soft-channel drain is placed to establish communication between the pericardial cavity and the left pleural space. Chest drains may be removed on postoperative day one if drainage is less than 100 mL, or retained longer if output remains higher. Data regarding the long-term patency of the pericardial opening after drain removal are lacking; however, it is presumed that the incision remains open while drainage persists and subsequently closes once drainage ceases.
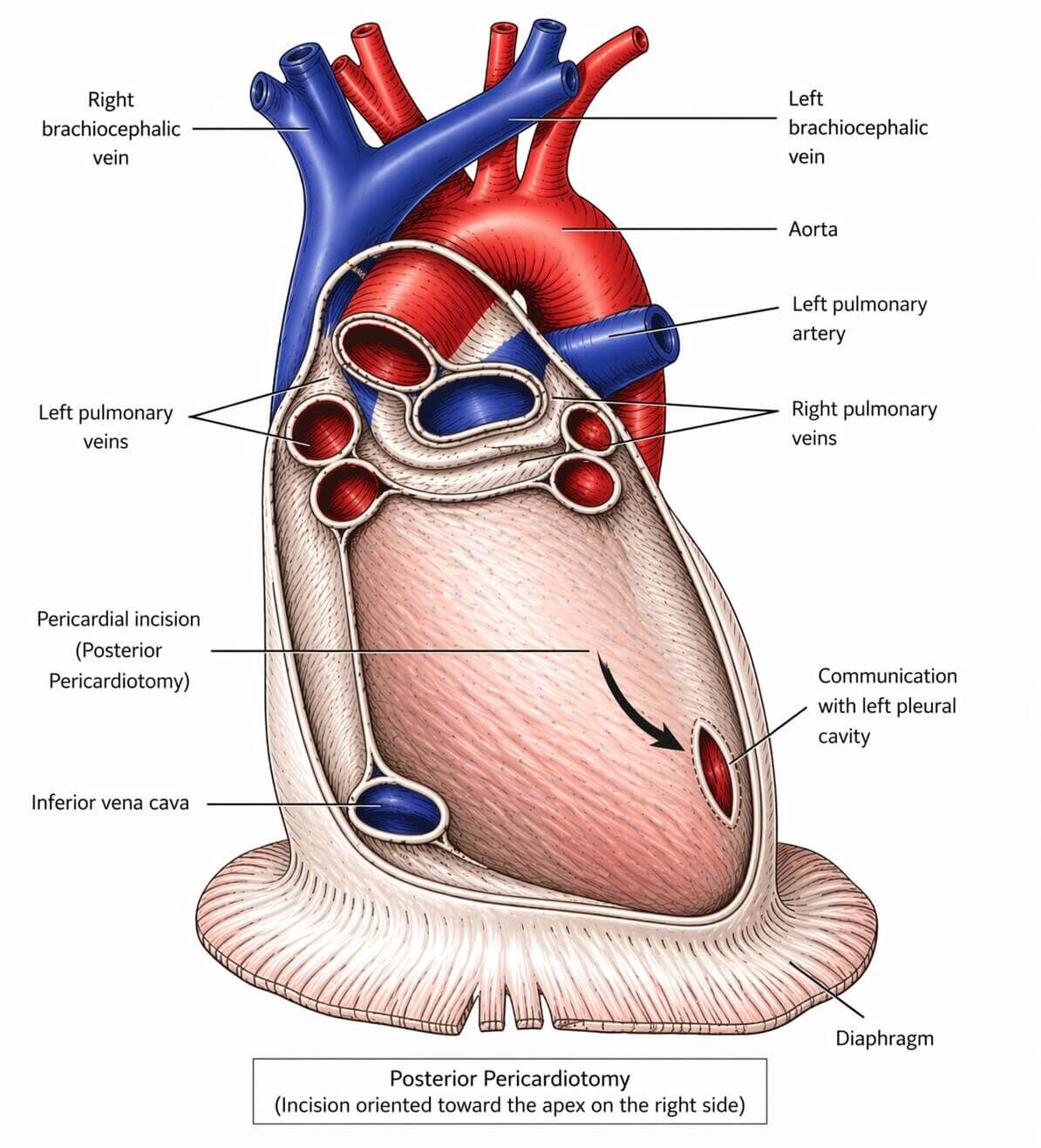 Fig. 3.
Fig. 3.Artist’s representation of the posterior pericardiotomy (black arrow). The red arrow illustration of posterior pericardiotomy showing a pericardial incision near the left atrium and pulmonary vein openings, enabling drainage of pericardial fluid and reducing the risk of postoperative atrial fibrillation.
Posterior left pericardiotomy has been linked to a lower incidence of POAF by facilitating the drainage of blood and fluid from the posterior pericardial space [71,72]. The proposed mechanism by which posterior left pericardiotomy reduces POAF involves enabling posterior pericardial fluid to drain into the left pleural cavity, where it can be removed via a chest tube. This process limits the accumulation of blood and fluid behind the left atrium, thereby reducing atrial irritation that may contribute to the development of POAF. Nevertheless, earlier studies exhibit several limitations, including small sample sizes, restrictive inclusion and exclusion criteria, variability in randomization methods, and inadequate electrocardiographic monitoring approaches. In addition, posterior left pericardiotomy prolongs operative time and may be associated with procedure-specific complications, particularly an increased occurrence of left-sided pleural effusion [73]. These findings support the hypothesis that postoperative surgical drainage of the pericardial space, thereby limiting pericardial exposure to shed mediastinal blood may reduce the incidence of POAF in patients undergoing cardiac surgery. In a study of 231 patients undergoing isolated aortic valve replacement, Tanawuttiwat et al. [74] reported that POAF rates were greatest among patients receiving surgical valve replacement (62%) compared with transapical (53%), transaortic (33%), and transfemoral (14%) transcatheter aortic valve replacement, indicating that minimizing blood exposure within the pericardial cavity may lower POAF risk. Continuous and effective pericardial drainage using multidrainage chest tubes has been associated with both a significant decrease in pericardial effusion volume and a two to threefold reduction in POAF incidence [75,76]. Furthermore, in a cohort of 150 cardiac surgery patients, Karimov et al. [77] demonstrated that obstruction of chest tubes was linked to a higher rate of POAF compared with unobstructed drainage (50% vs 21.9%; p = 0.005).
The PALACS trial (The Effect of Posterior Pericardiotomy on the Incidence of Atrial Fibrillation After Cardiac Surgery) [70] remains the only sufficiently powered randomized controlled trial comparing posterior pericardiotomy with no intervention. In total, 420 patients undergoing elective coronary artery, aortic valve, ascending aorta, or combined procedures were randomized. Rates of pericardial effusion (12% vs 21%; relative risk 0.58, 95% confidence interval [CI] 0.37–0.91) and POAF (17% vs 32%; adjusted odds ratio [OR] 0.44, 95% CI 0.27–0.70) were significantly reduced in the PP group. The additional operative time required for PP was minimal, and no procedure-related complications were observed in the intervention cohort. Overall, the PALACS findings indicate that posterior pericardiotomy should be considered in the majority of cardiac surgical procedures [78].
Beta-adrenergic blockers are considered the most efficacious and the most frequently suggested drugs for prophylaxis of POAF. They achieve a marked reduction in the rate of POAF and are particularly valuable in the postoperative setting when autonomic tone and myocardial stress levels are high [56]. Initial management usually consists of beta-blockers for rate control, especially in stable patients. Prophylactic amiodarone, administered either intravenously or orally, has been demonstrated to decrease the incidence, duration, and ventricular rate of POAF. Trial data suggest that it is well tolerated, does not result in increased major complications, and decreases the length of hospital stay [79,80]. Sotalol and digoxin, however, are less effective in preventing and treating POAF, as is intravenous diltiazem, for which robust supporting evidence is limited [56]. Corticosteroids have been shown to reduce the occurrence of POAF; however, they are also associated with an increase in minor complications and provide minimal benefit in reducing the length of hospital stay [55]. Ivabradine, especially in combination with beta-blockers, shows promise in decreasing POAF compared with individual agents [81]. Various pharmacological and non-pharmacological strategies have been investigated for the prevention of POAF, as summarized inTable 2 [82,83]. In addition to β-blockers and amiodarone, several pharmacological agents targeting inflammation and oxidative stress have been investigated for POAF prevention. Vitamin C, as a potent antioxidant, has been shown in randomized trials and meta-analyses to reduce POAF incidence, likely by attenuating oxidative stress and preserving atrial electrophysiological stability [84]. Colchicine, through inhibition of inflammasome activation and suppression of IL-1β–IL-6 signaling, has demonstrated efficacy in reducing postoperative atrial fibrillation in selected cardiac surgery populations, although gastrointestinal intolerance may limit its routine use [85]. Statins have also been associated with reduced POAF incidence, potentially due to their pleiotropic anti-inflammatory and endothelial-protective effects [86], though results across studies remain heterogeneous. Omega-3 fatty acids and other antioxidant strategies have been explored with mixed outcomes; while some studies suggest modest benefit, others show no significant reduction in POAF, highlighting the need for patient-specific selection and further randomized evaluation [87]. A comparison of therapeutic strategies and their clinical outcomes is presented in (Table 2). Overall, these pharmacological approaches may serve as useful adjuncts to standard therapy, particularly in patients with heightened inflammatory risk profiles.
| Intervention | POAF reduction | ARR/NNT (approx.) | Key comments |
|---|---|---|---|
| β-blockers | ↓ 30–50% | NNT ~6–10 | First-line, guideline recommended [82] |
| Amiodarone | ↓ 40–60% | NNT ~7–9 | Effective but requires monitoring [82] |
| Corticosteroids | ↓ ~30% | NNT ~8–12 | ↑ minor complications [83] |
| Partial cardiac denervation | ↓ ~40% | NNT ~7 | Surgical adjunct |
| Atrial pacing | ↓ ~25–40% | Variable | Evidence heterogeneous [83] |
| Vitamin C/antioxidants | ↓ ~20–30% | NNT ~10–15 | Low cost, mixed evidence |
ARR, absolute risk reduction; NNT, number needed to treat. “↑” indicates increase “↓” indicates decrease.
Understanding the inflammatory basis of POAF, particularly the role of IL-6–mediated atrial remodeling, provides important insight into its pathophysiology and highlights potential targets for preventive strategies. Identification of high-risk patients based on clinical characteristics and markers of atrial remodeling may allow for more individualized perioperative management.
Several risk stratification approaches, including echocardiographic parameters such as left atrial size and strain, clinical risk scores, and inflammatory biomarkers (e.g., IL-6, neopterin, and collagen turnover markers), may help identify patients who would benefit most from intensified prophylactic interventions. Integrating such tools into routine perioperative assessment could improve POAF prediction beyond traditional clinical models alone.
From a practical perspective, cost-effective preventive strategies remain essential, as POAF is associated with prolonged hospitalization and increased healthcare expenditure. While standard pharmacological therapies such as β-blockers and amiodarone remain foundational, adjunctive intraoperative approaches, including partial cardiac autonomic denervation and posterior pericardiotomy, may offer additional benefit in selected high-risk populations without substantially increasing operative risk.
Future research should focus on large, adequately powered randomized trials to clarify the role of anti-inflammatory therapies, surgical modulation of autonomic pathways, and biomarker-guided prevention strategies. A precision-medicine approach integrating clinical, imaging, and inflammatory indices may ultimately reduce the burden of POAF and improve postoperative outcomes following CABG.
This review has several limitations. The included studies demonstrate considerable heterogeneity in patient populations, surgical techniques, perioperative management, and definitions of POAF. Many preventive strategies are supported by observational data or single-center trials, limiting generalizability. In addition, evolving surgical approaches and perioperative care protocols may influence the applicability of earlier studies. Finally, variability in biomarker measurement timing and methodology complicates direct comparisons across studies. These limitations underscore the need for standardized definitions and large, multicenter randomized trials.
Postoperative atrial fibrillation happens a lot after heart surgeries like CABG, and it causes more problems for patients, longer stays in the hospital, and extra costs for everyone involved. Even with better ways to do the surgery and care for people around it, this complication still shows up pretty often. It makes me think we really need to figure out more about what causes it and how to stop it before it starts. One thing that stands out is how inflammation kicks in during the whole process. The cardiopulmonary bypass machine, the trauma from cutting open the chest, and that ischemia reperfusion stuff all ramp up the body's immune response. Cytokines like IL-6 and TNF-alpha get really high, and they are not just signs of trouble, they actually mess with the heart tissue. IL-6 seems to change how TGF-beta1 works, getting fibroblasts going and building up extra matrix, which turns into fibrosis in the atria. That messes up the electrical signals there, making it easier for arrhythmias to happen through reentry circuits or something like that. Oxidative stress ties right into this too, kind of building on the inflammation. Reactive oxygen species come from the bypass and injury to the heart muscle, damaging cells and screwing with ion channels and calcium. It leads to uneven conduction and shorter refractoriness in the atria, which I guess helps AF start and keep going. There is this biomarker, neopterin, that points to oxidative stress making people more prone to POAF, and maybe even their inflammation levels before surgery play a role in how things turn out after. Then there is the damage to cardiomyocytes themselves, with cell death pathways like apoptosis, necrosis, and even ferroptosis involved. Ferroptosis is this iron related lipid peroxidation thing that happens under stress, and it adds to the injury in the heart. All these pieces, the inflammation from CABG, the oxidative part, the cell death, they feed into remodeling of the atrial structure and electricity. Representing an interconnected pathophysiological network, as illustrated in (Fig. 4)
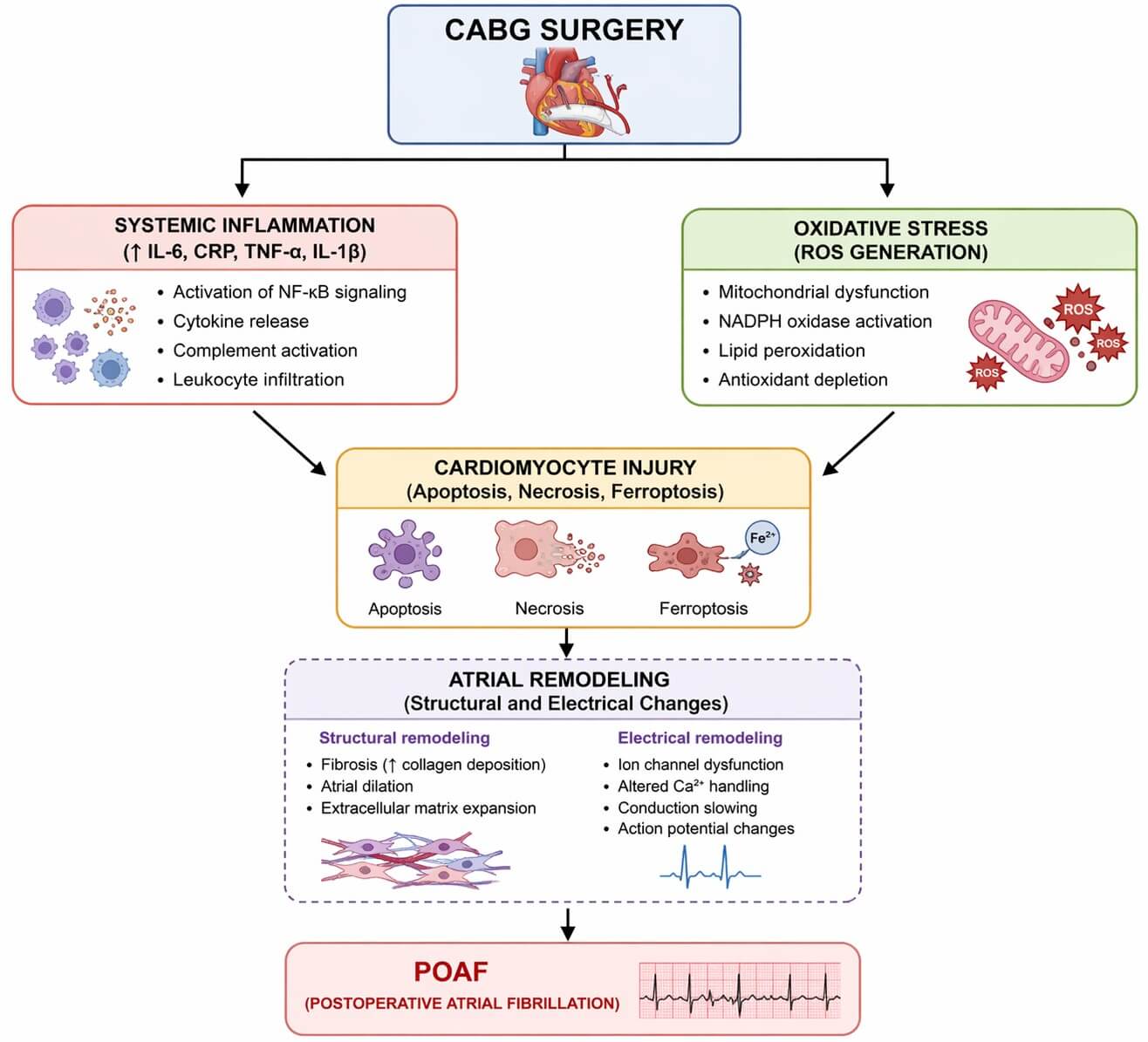 Fig. 4.
Fig. 4.Proposed mechanistic pathway linking coronary artery bypass grafting (CABG) to postoperative atrial fibrillation (POAF). CABG-induced systemic inflammation and oxidative stress lead to cardiomyocyte injury through apoptosis, necrosis, and ferroptosis. These changes contribute to atrial structural and electrical remodeling, characterized by fibrosis, altered calcium handling, and conduction abnormalities, which collectively promote the development of POAF.
Clinically, people have tried different ways to prevent POAF. Beta blockers and amiodarone are common drugs, and some anti-inflammatory ones too, but the results are all over the place, not always working great. Atrial pacing can help with slow heart rates that trigger AF, improving conduction a bit, though studies do not agree on it. Surgical tweaks like using Del Nido solution for cardioplegia or doing CABG without the pump might cut down on injury and inflammation, but it is not clear if they really stop POAF reliably. Some people argue that off-pump techniques reduce the inflammatory hit, but others say the evidence is mixed. It feels like preventive strategies are getting better, yet there are still gaps. The studies out there have issues, like different patient groups, varying surgery methods, and how care is handled around the operation, so findings do not line up. The exact ways inflammation and stress lead to remodeling are not fully sorted out. I think future work needs to look at new biomarkers, maybe targeting those signaling paths or ferroptosis, to make prevention more tailored. It gets a bit messy trying to connect all this, and not everything is settled yet.
POAF is a frequent and severe complication after CABG. The greatest body of evidence indicates that IL-6 participates in the genesis of POAF, which is predominately caused by inflammation, and that IL-6 signaling is particularly significant. IL-6 induces structural remodeling, collagen deposition and fibrosis in arterial tissues, and these responses are modified by age, hypertension, obesity, and renal insufficiency. The effects of electrical remodeling may be sufficient to induce atrial arrhythmias, including POAF. It should be emphasized that IL-6 is just one of many players in the pathogenesis of POAF; other causes, such as preexisting cardiovascular disease and genetic predisposition, also come into play. POAF is a frequent complication after cardiac surgery, with a multifactorial etiology that implicates systemic inflammation, ischemia-reperfusion injury, oxidative stress, and myocardial remodeling. The significance of POAF after CPB remains a reality of modern cardiac surgery, and is a testament to the complexity and risks within the modern era of cardiac surgery, despite decades of investigations and modest incremental progress. The role of other inflammatory markers and IL-6 in the pathogenesis of POAF may also be therapeutically relevant. Modulating IL-6 signaling pathways by blocking inflammatory responses with anti-inflammatory drugs may attenuate the effect, intensity, or incidence of POAF. In addition, despite the development of new techniques to protect the myocardium and blunt the inflammatory response, the prevalence of POAF has not decreased substantially, highlighting an unmet need to translate mechanistic knowledge into effective therapeutics.
Even with standard treatments such as β-blockers and amiodarone, the prevalence of POAF remains; thus, more effective alternative options are needed. Novel intraoperative techniques, such as cardiac autonomic denervation, posterior pericardiotomy and calcium chloride injection, in addition to prophylactic corticosteroids, have potential for POAF risk mitigation. Moving forward, incorporating clinical and inflammatory indices into risk stratification and maintaining long-term follow-up are important elements in the successful prevention and management of POAF.
AF, atrial fibrillation; BAP, biatrial pacing; CABG, coronary artery bypass grafting; CANS, cardiac autonomic nervous system; CPB, cardiopulmonary bypass; EAT, epicardial adipose tissue; ESRD, end-stage renal disease; IL-6, interleukin-6; LOM, ligament of Marshall; PCI, percutaneous coronary intervention; POAF, postoperative atrial fibrillation; RAP, right atrial pacing; TGF-β1, transforming growth factor beta 1; RCT, randomized Controlled Trail; PP, posterior pericardiotomy.
MGY designed and drafted the manuscript. YD and PL designed, reviewed, drafted and supervised the review. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflicts of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.