




1 Department of Cardiothoracic Surgery, St. Bartholomew’s Hospital, Barts Health NHS Trust, EC1A 7BE London, UK
2 Institute for Cardio-Metabolic Medicine & Departments of Cardiology/Cardiothoracic Surgery, University Hospitals Coventry and Warwickshire, CV2 2DX Coventry, UK
3 Department of Cardiothoracic Surgery, St. Vincent’s Hospital, Darlinghurst, NSW 2010, Australia
4 Centre for Health & Life Sciences, Coventry University, CV1 2DS Coventry, UK
5 Warwick Medical School, CV4 7AL Coventry, UK
Abstract
In patients with persistent atrial fibrillation (AF) and chronic severe mitral valve (MV) regurgitation, the success rate of cardioversion and long-term maintenance of sinus rhythm is poor. Concomitant AF ablation during MV surgery may improve outcomes. We report short- and medium-term results in patients undergoing concomitant AF ablation during MV surgery.
This was a retrospective study of all consecutive patients with long-standing persistent AF who underwent MV surgery for severe MV regurgitation with concomitant biatrial surgical ablation (biatrial modified Cox-maze IV with completion of the full lesion set) between June 2015 and June 2018. Patients were followed at 3, 6, and 12 months postoperatively. Data from 24-hour Holter monitoring, baseline clinical parameters, complications, and AF recurrence were collected.
A total of 62 patients with severe mitral regurgitation and long-standing persistent AF underwent MV surgery with concomitant AF ablation. A standardized energy source (bipolar radiofrequency plus cryoablation) was used in all cases. The mean age was 70 ± 11 years; 32 (51.6%) were female, and the mean CHA2DS2-VASc score was 2.7 ± 1. At 12 months, sinus rhythm was documented in 43 (69.4%) patients on 24-hour Holter monitoring; 88.4% of those in sinus rhythm at follow-up demonstrated atrial contractility on echocardiography. Pacemaker implantation was required in 5 (8.1%) patients, and cerebrovascular events occurred in 3 (4.8%). Meanwhile, two patients (3.2%) required re-exploration for bleeding, but none needed re-intervention on the MV.
Biatrial surgical AF ablation is a safe and effective adjunct in patients with long-standing persistent AF undergoing concomitant MV surgery and may be beneficial in the long term for maintaining a normal rhythm.
Keywords
- maze ablation
- atrial fibrillation
- radiofrequency ablation
- cryoablation
- Cox-maze IV procedure
Atrial fibrillation (AF) is the most common sustained arrhythmia and is associated with a significant risk of morbidity and mortality [1]. Indeed, up to 50% of patients admitted for mitral valve (MV) surgery present with AF, which can adversely affect long-term outcomes [2]. Growing evidence highlights the considerable morbidity burden of AF, including an increased incidence of cerebrovascular and other thromboembolic events, anticoagulant-related hemorrhage, hemodynamic compromise, more frequent hospitalizations, early cognitive decline, and reduced quality of life [1]. Long-term success after surgical AF ablation is influenced by the preoperative duration of AF; nevertheless, encouraging results have been reported even in patients with longstanding persistent AF [3]. The Cox-maze procedure, introduced by James Cox in 1987 [4], remains the surgical standard of care. However, the original cut-and-sew technique has been simplified over time by replacing the original surgical incisions with continuous ablation lines created using various energy sources, and the biatrial Cox-maze III procedure has demonstrated excellent long-term outcomes [5]. Nonetheless, several institutions advocate performing only a left-sided lesion set and omitting certain conventional right-sided ablation lines [6]. Recurrence of AF during follow-up remains a concern, and current guidelines acknowledge the absence of a unified approach for surveillance and management in this patient group [1]. Consequently, the modified Cox-maze IV procedure is now recommended as the standard approach (class I, level of evidence A) [7].
Therefore, this study aimed to evaluate the effectiveness of biatrial ablation in patients with long-standing persistent AF undergoing concomitant MV surgery, with a 1-year postoperative follow-up.
We performed a retrospective study of all consecutive patients undergoing MV surgery with concomitant biatrial surgical ablation using the modified Cox-maze IV lesion set between June 2015 and June 2018. MV regurgitation was severe in accordance with the updated 2017 Society of Thoracic Surgeons (STS) guidelines [7]. All patients had long-standing persistent AF, defined as duration ≥1 year, according to international guidelines [1]. Patients with prior catheter ablation for AF were excluded. Ethics approval was obtained from our hospital’s research and audit department via the Governance arrangements for Research Ethics Committee (GafREC), approval reference GF1022.
All patients underwent detailed perioperative assessment of valve pathology, and transesophageal echocardiography was used to exclude left atrial thrombus. No patient was excluded based on the maximum preoperative left atrial dimension. Standard median sternotomy and cardiopulmonary bypass were established with bicaval drainage and ascending aortic return. Mild systemic hypothermic cardiopulmonary bypass was used, and myocardial protection was achieved using intermittent antegrade cold blood cardioplegia at 8 ℃. The modified Cox-maze IV procedure was performed using a combination of radiofrequency (RF) ablation and cryoablation (CA). Attention was first directed to the pulmonary veins (PVs). The right PVs were bluntly dissected and encircled with an umbilical tape, and a left atriotomy was performed via Sondergaard’s groove, extending inferiorly beneath the inferior vena cava and superiorly onto the dome of the left atrium. The AtriCure Isolator Synergy bipolar RF clamp (OLL2/OSL2, AtriCure Inc, Mason, OH, USA) was then carefully positioned, and electrical ablation of the PVs was performed. Two successive ablation lines were applied, creating two closely spaced concentric circles. Two clamp applications were used only when impedance fell immediately after the second ablation; further ablation was conducted if impedance did not fall. Next, the ligament of Marshall was divided using diathermy, and the left PVs were bluntly dissected, encircled with umbilical tape, and ablated with RF to complete left-sided PV isolation. To complete RF ablation of the posterior left atrium, a “box” lesion set was also completed. The bipolar RF clamp was used to create an ablation line across the floor of the left atrium, connecting the inferior right PV to the inferior left PV, followed by a superior line connecting the right and left upper PVs.
RF energy was also utilized to isolate the left atrial appendage, and the AtriCure cryoICE CA probe (AtriCure Inc, Mason, OH, USA) was used to connect the left atrial appendage to the left superior PV, with freezing at –70 ℃. The mitral isthmus lesion was created using the cryo-probe, crossing the epicardial coronary sinus. The left atrial appendage was excluded in all patients by oversewing the orifice from within the left atrium using a running 4-0 non-absorbable, monofilament polypropylene suture (Johnson & Johnson Ltd, New Brunswick, NJ, USA). This was the surgical preference at the time; our practice has since evolved to use the AtriClip (AtriCure Inc, Mason, OH, USA), following local data demonstrating high rates of left atrial appendage recanalization on computed tomography (CT). Right atrial lesion sets were completed by passing the RF clamp through a vertical incision and applying three individual ablation lines toward the superior vena cava (SVC), inferior vena cava, and right atrial appendage, respectively. Finally, endocardial CA was performed on the tricuspid annulus to prevent cavo-tricuspid isthmus-dependent atrial flutter. Repair or replacement of the MV, along with any other concomitant procedures, was performed, as appropriate. Two right atrial and two right ventricular epicardial pacing wires were placed to provide backup dual-chamber pacing, if required postoperatively. Left atrial size was reduced by suturing to buttress the tissue and decrease chamber volume.
Patients were continuously monitored for rhythm disturbances for at least 72 hours post-procedure. Pacing wires were removed 24 hours before discharge. In-hospital recurrence of AF or atrial flutter was treated with an intravenous loading infusion of amiodarone (1200 mg IV over 24 hours), followed by oral maintenance therapy for 3 months if the resting heart rate was ≥60 bpm. Beta-blockers were added for persistent high ventricular rates and continued in most patients. If medical treatment was ineffective, external cardioversion was considered. All patients were anticoagulated with warfarin postoperatively, regardless of the procedure type or underlying rhythm. An international normalized ratio (INR) >2.0, depending on the concomitant surgical procedure, was targeted before hospital discharge. Follow-up was conducted at 3, 6, and 12 months post-discharge. Holter monitoring was performed at each time point if a sinus rhythm was present on a 12-lead electrocardiogram (ECG); additional monitoring was performed as clinically indicated. Some patients underwent additional follow-up at 9 months when clinically warranted.
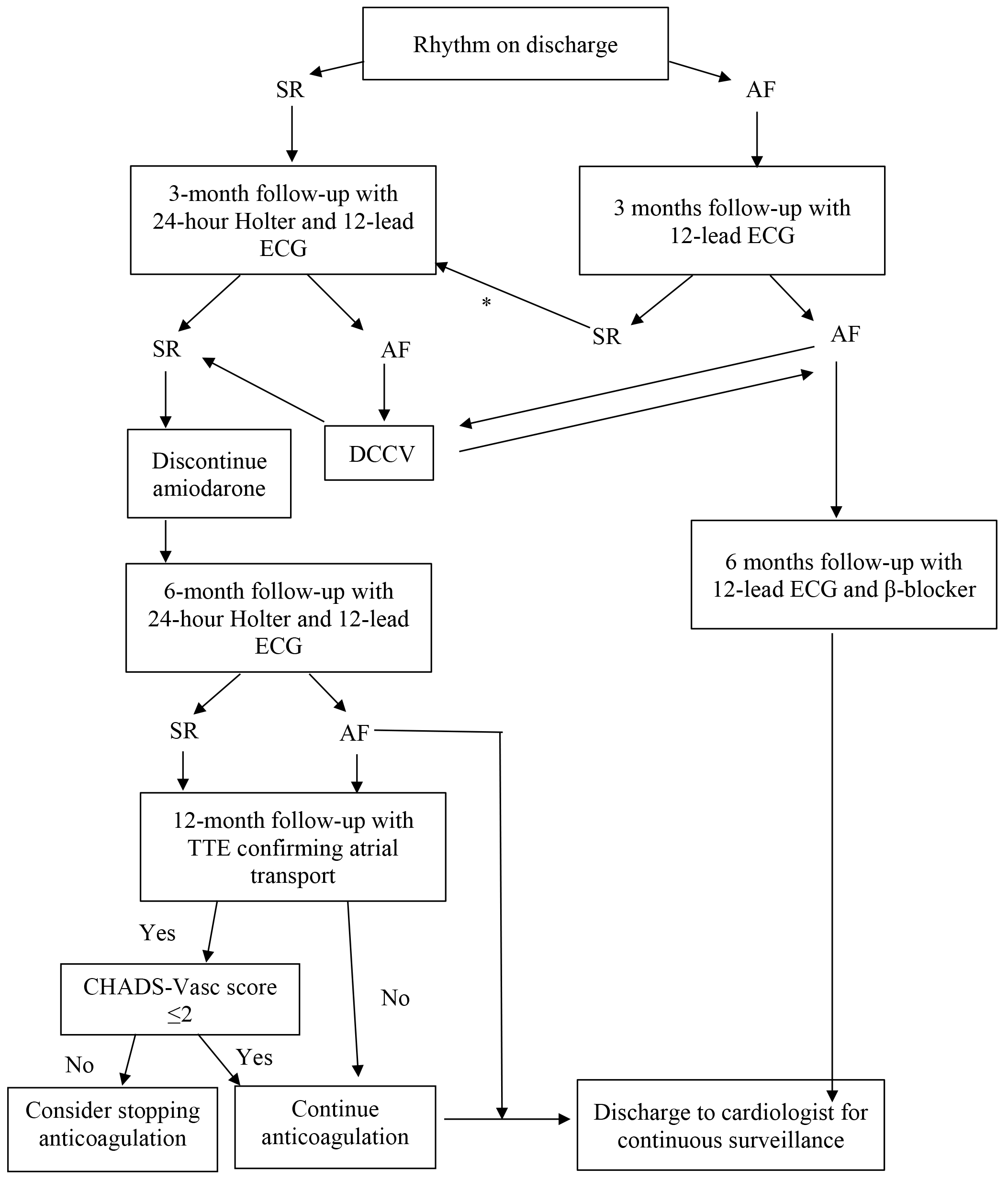
Atrial arrhythmia recurrence was defined as any atrial arrhythmia (AF, atrial flutter, or atrial tachycardia) lasting ≥30 seconds on a 24-hour Holter monitor [1,8]. A successful modified Cox-maze procedure was defined as a normal sinus rhythm (either intrinsic or paced atrial rhythm) at 12-month follow-up, freedom from class I or III antiarrhythmic drugs, and evidence of atrial contractility on transthoracic echocardiography (TTE), as evidenced by mitral inflow pulse-wave Doppler. All echocardiograms were performed and reported by fully trained British Society of Echocardiography physiologists, in accordance with international guidelines [1]. If a patient was discharged in AF but found to be in sinus rhythm at follow-up, an additional outpatient review with a 24-hour Holter monitor was requested. After the outpatient visit, patients were referred back to the associated cardiologist for ongoing surveillance to detect late arrhythmia recurrence. The follow-up and arrhythmia management pathways are shown in Fig. 1.
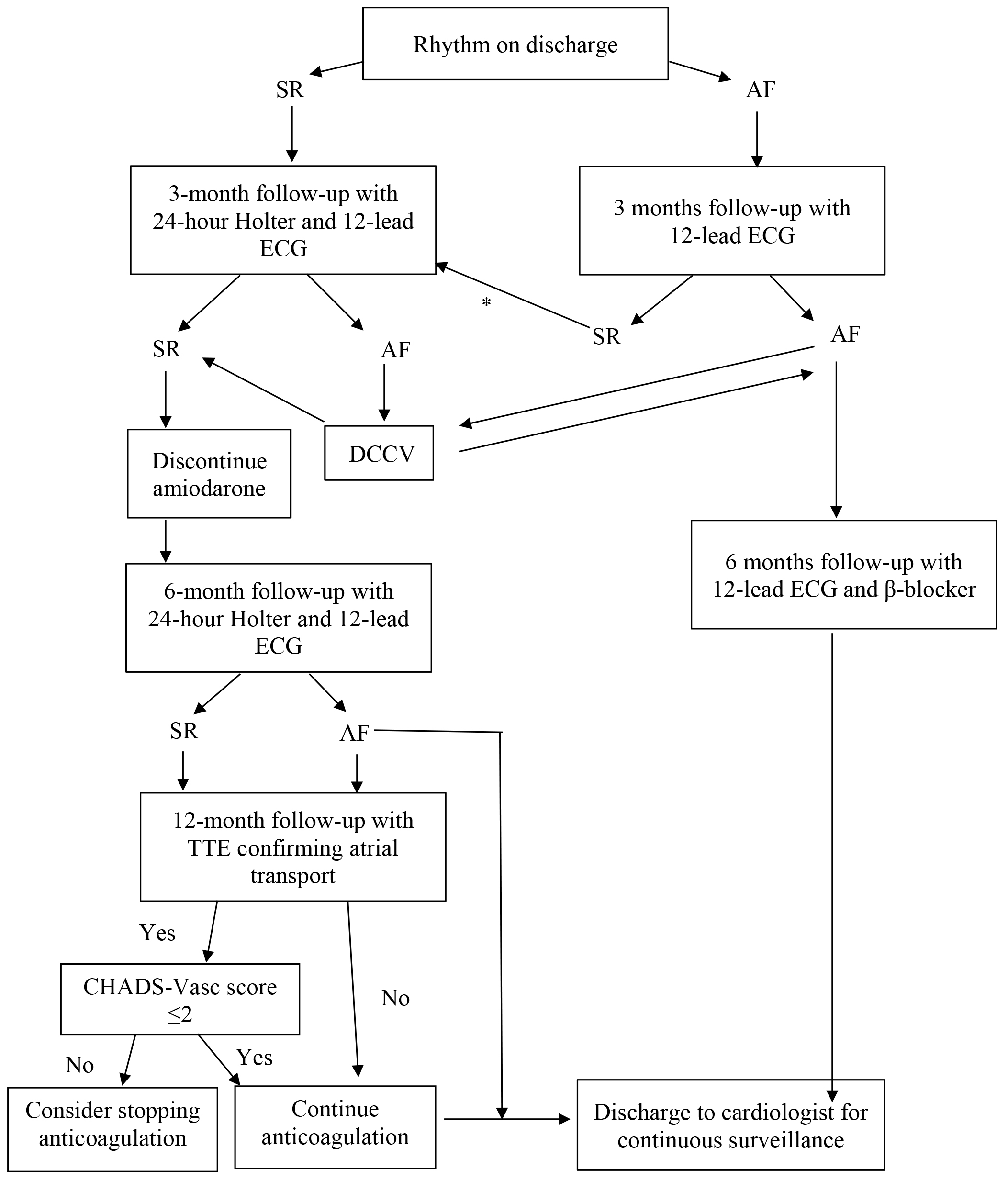 Fig. 1.
Fig. 1.
Follow-up protocol for patients undergoing surgical AF ablation. *Additional outpatient visit to confirm rhythm status using a 24-hour Holter monitor. SR, sinus rhythm; AF, atrial fibrillation; DCCV, direct current cardioversion; TTE, transthoracic echocardiogram; ECG, electrocardiogram.
Statistical analysis was performed using SPSS version 25 (IBM, Chicago, IL, USA). Categorical variables are expressed as frequency (n) and percentage (%), and continuous variables as mean ± standard deviation (SD). Fisher’s exact test and the chi-square test were used to compare categorical variables between groups. The Mann–Whitney U test was used to compare continuous variables between groups. Logistic regression analysis was performed to identify independent predictors of AF recurrence at 12-month follow-up, and results are reported as odds ratios (ORs) with 95% confidence intervals (CIs). For all tests, p-values < 0.05 were considered statistically significant. Time to AF recurrence was assessed using survival analysis techniques. The cumulative probability of freedom from AF recurrence during both the early and 1-year (12-month) follow-up periods was estimated using the Kaplan–Meier method. The primary endpoint was defined as the first documented recurrence of AF. Patients with early recurrence underwent cardioversion or received rhythm-control strategies and were reassessed for AF recurrence at 12-month follow-up. Patients without an event were right-censored at the time of the last clinical follow-up or at exactly 12 months for those completing the full 1-year study period without recurrence. Kaplan–Meier curves were generated to display the estimated survival probability and the number of patients at risk at 2-month intervals, with 95% CIs. This statistical analysis and plot generation were performed in R version 4.5.2 (R Foundation for Statistical Computing, Vienna, Austria), using the survival and survminer packages.
A total of 62 patients were included in the study. The mean age ± SD was 70 ± 11 years, and 30 patients were male (48.4%). Baseline characteristics are summarized in Table 1. No patient received amiodarone before surgery, and none had a left-sided SVC. The mean left atrial diameter was 5.5 ± 0.7 cm. Clinical follow-up was complete for all patients, who underwent postoperative TTE and cardiac rhythm assessment. All but two patients (n = 60) underwent MV repair, primarily due to the available surgical expertise rather than the severity of the MV lesion. There were no in-hospital deaths and one late death at 20 months, unrelated to the cardiac surgery. Permanent pacemaker implantation was required in five patients (8.1%) immediately postoperatively: two (3.2%) for sinus node disease and three patients (4.8%) for AV node disease. Transient ischemic attack occurred in three patients (4.8%) at 12-month follow-up, and two patients (3.2%) required re-exploration for bleeding during the same admission. No reoperation for recurrent MV regurgitation was reported, and no patient underwent percutaneous AF ablation during the study period.
| Characteristics | n = 62 | |
|---|---|---|
| Female (n, %) | 32 (51.6) | |
| Age (mean ± SD, y) | 70 ± 11 | |
| Mean preoperative creatinine clearance (mL/min/1.73 m2) | 66 ± 23 | |
| Diabetes (n, %) | 10 (16.1) | |
| Hypertension (n, %) | 33 (53.2) | |
| Cerebrovascular event (n, %) | 5 (8.1) | |
| Left ventricular ejection fraction on TTE (n, %) | ||
| ≥60% | 33 (53.2) | |
| 31–59% | 22 (35.5) | |
| ≤30% | 7 (11.2) | |
| NYHA class III or IV (n, %) | 34 (54.8) | |
| History of CHF (n, %) | 48 (77.4) | |
| CHA2DS2-VASc score (mean ± SD) | 2.7 ± 1 | |
| Body surface area (m2, mean ± SD) | 1.8 ± 0.2 | |
| Previous percutaneous AF ablation | 0 | |
| Logistic EuroSCORE | 11 ± 7 | |
| Systolic pulmonary artery pressure (mmHg, mean ± SD) | 49 ± 12 | |
| Mitral valve pathology (%) | ||
| Myxomatous | 44 (70.9) | |
| Rheumatic | 13 (20.9) | |
| Ischemic | 4 (6.5) | |
| Functional | 1 (1.6) | |
| Mitral valve surgery performed (n, %) | ||
| Repair | 60 (96.8) | |
| Replacement | 2 (3.2) | |
| Left atrial diameter (cm, mean ± SD) | 5.5 ± 0.7 | |
NYHA, New York Heart Association classification; CHF, congestive heart failure. Continuous data are presented as mean (standard deviation), and categorical data are presented as frequency (%).
A total of 29 patients (47%) maintained sinus rhythm at discharge, as evidenced by 24-hour Holter monitoring. A total of 35 patients (56%) and 43 patients (69.4%) maintained sinus rhythm at 6- and 12-month follow-up, respectively; 8 patients underwent external cardioversion between the 6- and 12-month follow-ups. None of these patients were receiving class I or class III antiarrhythmic therapy, and no patients underwent percutaneous catheter ablation for AF during the 12-month follow-up period. Of the 43 patients in sinus rhythm at 12 months, anticoagulation was discontinued in 34 (79%). There was an 88.4% correlation (38/43 patients) between post-ablation sinus rhythm on 24-hour Holter monitoring and atrial contractility on subsequent TTE at 12 months. Table 2 compares patients who maintained sinus rhythm at the 12-month follow-up with those who did not. Overall, 19 patients (31%) had recurrence of AF. There were no significant differences between the two groups, and none of the patients with AF recurrence had worsening mitral regurgitation at follow-up.
| Patient group | Maintained sinus rhythm (n = 43) | AF recurrence (n = 19) | p-value | |
|---|---|---|---|---|
| Females | 21 (49%) | 10 (53%) | >0.99 | |
| Age (years) | 69.8 ± 11.9 | 70.6 ± 7.4 | 0.69 | |
| Preoperative creatinine clearance (mL/min/1.73 m2) | 101.7 ± 61 | 90 ± 20 | 0.44 | |
| Preoperative hemoglobin (g/L) | 130 ± 23 | 137 ± 13 | 0.13 | |
| Preoperative urea (mmol/L) | 7.6 ± 2.6 | 6.9 ± 1.9 | 0.33 | |
| Diabetes | 6 (14%) | 4 (21%) | 0.48 | |
| Hypertension | 25 (58%) | 11 (58%) | >0.99 | |
| Prior cerebrovascular event | 7 (16%) | 3 (16%) | >0.99 | |
| Left ventricular ejection fraction | ||||
| ≥60% | 29 (67%) | 14 (74%) | 0.10 | |
| 31–59% | 12 (28%) | 5 (26%) | 0.29 | |
| ≤30% | 2 (5%) | 0 (0%) | 0.45 | |
| NYHA class III or IV (%) | 23 (53%) | 11 (58%) | 0.06 | |
| History of CHF (%) | 32 (74%) | 16 (84%) | 0.52 | |
| CHA2DS2-VASc score | 2.6 ± 1.1 | 2.8 ± 1.4 | 0.80 | |
| Body surface area (m2) | 1.8 ± 0.2 | 1.8 ± 0.3 | 0.51 | |
| Logistic EuroSCORE | 10.5 ± 6.1 | 11.9 ± 8.6 | 0.82 | |
| Systolic pulmonary artery pressure (mmHg) | 46.9 ± 11.4 | 52.6 ± 13 | 0.14 | |
| Mitral valve pathology (%) | ||||
| Myxomatous | 31 (72%) | 13 (69%) | 0.10 | |
| Rheumatic | 9 (21%) | 4 (21%) | 0.27 | |
| Ischemic | 3 (7%) | 1 (5%) | 0.63 | |
| Functional | 0 | 1 (5%) | >0.99 | |
| Left atrial diameter (cm) | 5.4 ± 0.7 | 6.2 ± 0.8 | 0.40 | |
| Mitral valve surgery (%) | ||||
| Repair | 42 (98%) | 18 (95%) | >0.99 | |
| Replacement | 1 (2%) | 1 (5%) | >0.99 | |
| Concomitant procedure (%) | 28 (65%) | 14 (74%) | 0.06 | |
| Tricuspid valvuloplasty | 21 (49%) | 10 (53%) | 0.07 | |
| Aortic valve replacement | 3 (7%) | 1 (5%) | 0.63 | |
| CABG | 6 (14%) | 5 (26%) | >0.99 | |
| Cumulative bypass time (min) | 122 ± 28 | 123 ± 26 | 0.80 | |
| Cumulative cross-clamp time (min) | 101 ± 25 | 149 ± 22 | 0.82 | |
| Length of in-hospital stay (days) | 11 ± 5.7 | 8 ± 3.7 | 0.03* | |
Values are shown as n with % or mean ± SD. * marks p < 0.05. NYHA, New York Heart Association; CHF, congestive heart failure; CABG, coronary artery bypass grafting.
Table 3 summarizes the outcomes from our cohort. There were no in-hospital deaths. Three patients developed a transient cerebrovascular event postoperatively; two of these three were in sinus rhythm during the early postoperative period, and all three were in sinus rhythm at 6 months. Anticoagulation was continued postoperatively in all three patients. Five patients required permanent pacemaker implantation prior to hospital discharge. Two patients required re-exploration for excessive bleeding from sternal wires; the issue was managed appropriately, and all patients made a good recovery.
| Outcome measure | n (%) |
|---|---|
| In-hospital mortality | 0 |
| Late mortality (after 12-month follow-up) | 1 (1.6) |
| Perioperative transient ischemic event | 3 (4.8) |
| Permanent pacemaker implantation during same admission | 5 (8.1) |
| Re-exploration for bleeding | 2 (3.2) |
Fig. 2 illustrates Kaplan–Meier analysis of AF recurrence probability at early follow-up (3 months, above) and at 12-month follow-up (below); a 3-month blanking period was applied for the 12-month follow-up, as patients with early recurrence were either cardioverted or initiated on antiarrhythmic drugs. The 12-month freedom from AF recurrence probability was 69.4% (95% confidence interval (CI) 58.8–81.8%); median time to AF recurrence was not reached, as more than half of the cohort remained free from recurrence at the end of the study period.
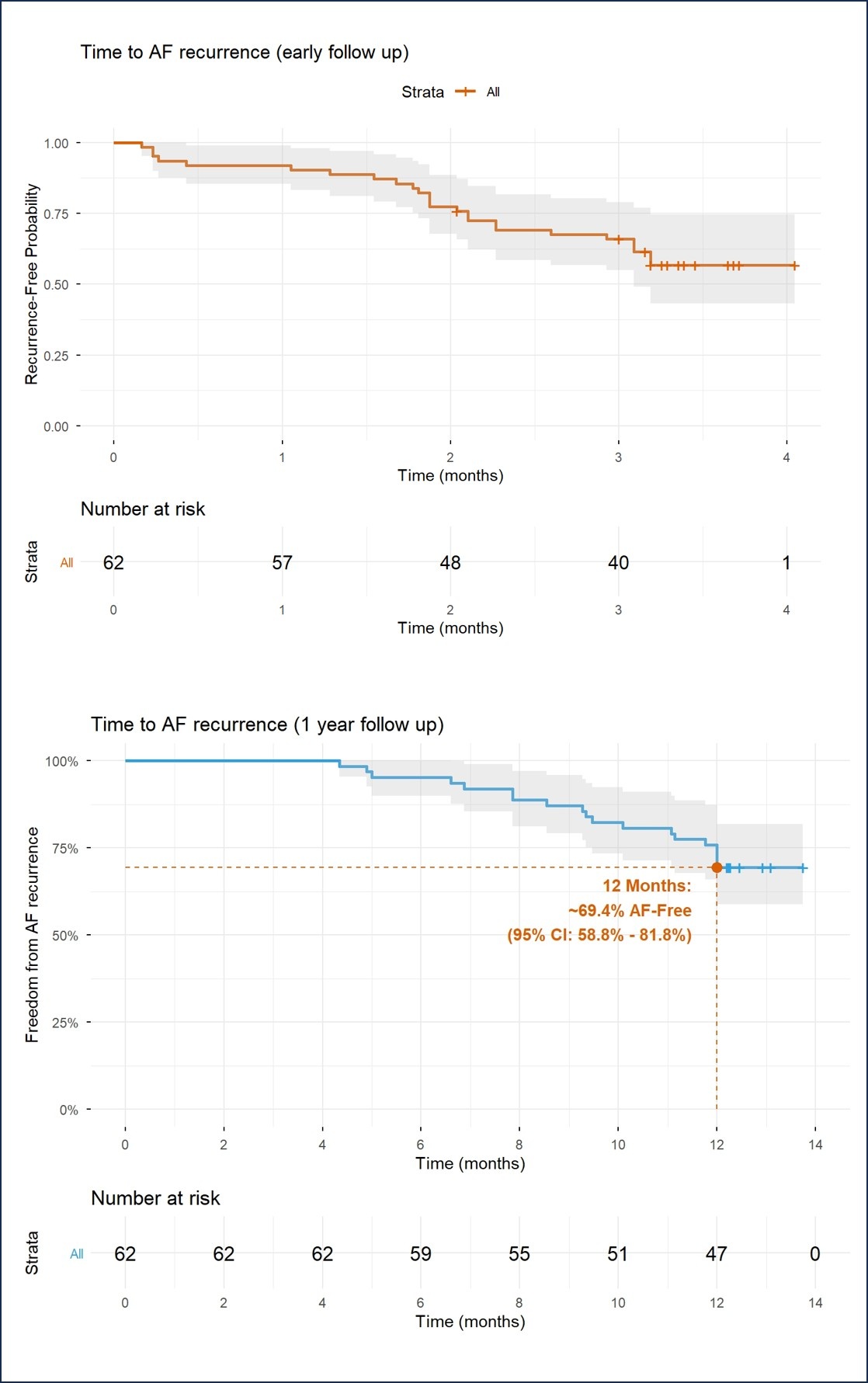 Fig. 2.
Fig. 2.
Kaplan Meier analysis of time to AF recurrence (early recurrence during blanking period) and at 12-month follow up. 95% confidence intervals (CI) are shaded in grey on each curve. AF, atrial fibrillation.
We report our experience with concomitant biatrial modified Cox-maze IV ablation for long-standing persistent AF (using RF plus CA) in patients undergoing MV surgery, demonstrating favorable outcomes at 12-month follow-up. Patients were managed according to a standardized local follow-up protocol that included regular visits for 12-lead ECG, 24-hour Holter monitoring, and TTE. We found that concomitant surgical ablation for long-standing persistent AF at the time of MV surgery was safe and effective, with a high proportion of patients maintaining sinus rhythm at 12-month follow-up. This included patients at high risk for both mortality and cerebrovascular events, as defined by the logistic EuroSCORE [9] and the CHA2DS2-VASc score [1]. Postoperative complications were limited, with five patients requiring a permanent pacemaker implantation and three patients experiencing a new cerebrovascular event either during the index hospitalization or follow-up. In our study, we demonstrated a 12-month sinus rhythm maintenance success rate of 69.4% among patients with long-standing persistent AF undergoing a complete biatrial lesion set, which is consistent with a previous meta-analysis [10]. However, the comparative effectiveness of isolated left atrial ablation versus biatrial ablation remains uncertain. A recent meta-analysis by Li et al. [11] of three randomized controlled trials and 18 retrospective studies found that left and biatrial ablation were equally effective in restoring sinus rhythm. These studies collectively included patients with both paroxysmal and long-standing persistent AF, without accounting for the significant differences in atrial substrate between these two disease states. In patients with paroxysmal AF, focal triggers are predominantly localized to the PVs, whereas in long-standing persistent AF, triggers may arise from either atrium [1,7]. Furthermore, expert opinion suggests that omission of right-sided tricuspid lesions may result in a higher prevalence of cavo-tricuspid isthmus-dependent atrial flutter [7]. Blackstone et al. [12] randomized 260 patients to receive MV surgery with surgical ablation versus MV surgery alone; among those receiving ablation, patients were further randomized to PV isolation or a biatrial maze. At 12 months, the estimated prevalence of AF was 58% after MV surgery alone, 36% after PV isolation, and 23% after a biatrial maze. Our study reports a well-defined population of patients with long-standing persistent AF undergoing both right and left atrial lesion sets, along with the associated outcomes at 12-month follow-up. Notably, most patients underwent MV repair rather than replacement; however, whether this contributed to the success in maintaining normal rhythm at follow-up is unknown.
The surgical approach to managing AF can vary, and multiple successful techniques have been described. Cox et al. [4] originally advocated the cut-and-sew maze, which, although effective, was invasive and time-consuming. The introduction of RF and CA has facilitated broader adoption by simplifying the procedure and enabling more reproducible lesion sets [13], with an emphasis on achieving reliable transmural lesions. In our practice, we used a combination of RF and CA in all patients to obtain transmural ablation lesions. Our mid-term outcomes appear acceptable, particularly given the high-risk profile of our cohort. AF coexists with MV pathology in up to 60% of cases, and successful MV surgery alone may restore sinus rhythm in more than 40% of patients [14]. Although this may have influenced our results, we consider this factor unlikely to be the main driver of rhythm restoration in this cohort of patients with long-standing persistent AF.
Several predictors of AF recurrence have been reported, including advanced age, longer AF duration, and a larger left atrium [15]. Frailty has also been identified as an important factor; frail patients had a 6-fold higher risk of AF recurrence after ablation compared with non-frail patients, suggesting that the frailty index may serve as a risk predictor of recurrent AF [16]. Calvert et al. [17] recently reported that patients undergoing redo AF ablation with silent PVs at the start of the procedure had worse clinical outcomes. Postoperative AF episodes lasting ≥48 hours have similarly been associated with a higher risk of late AF recurrence after cardiac surgery [18]. Lower post-ablation levels of the systemic immune inflammation index have been reported to predict AF recurrence following cryoballoon ablation [19], and prolonged atrial conduction intervals, especially in the left atrium, have been associated with susceptibility to post-ablation AF recurrence and may facilitate earlier detection and management [20].
Obliteration of the left atrial appendage has been associated with more than a 50% reduction in stroke rates and a modest reduction in mortality in previous studies [21]. In addition to successfully treating the arrhythmia, surgical AF ablation aims to restore the atrial “kick”, thereby increasing stroke volume and possibly reducing the likelihood of thromboembolic events [22]. The restoration of both atrial contraction and sinus rhythm has been reported variably from 21% to 75% depending on the type of AF [23,24]. This contradicts our results, as we found a direct correlation between re-establishment of sinus rhythm on a 24-hour Holter monitor and left atrial activity in all cases. Outpatient echocardiography was deliberately scheduled at follow-up, allowing time for the potentially “stunned” myocardium to recover and restore atrial contractility. However, there was no correlation between left atrial diameter and the success of the AF ablation procedure, which may reflect the relatively small patient cohort and the aggressive intraoperative reduction in left atrial size.
The strategy of long-term anticoagulation to prevent thromboembolic events remains an important question, especially for patients without clear evidence of recurrence. For patients undergoing catheter ablation, the baseline CHA2DS2-VASc score is used to identify patients at risk of thromboembolic events, and patients with a high score remain on anticoagulation despite successful AF ablation [1]. Guidelines for surgical AF treatment recommend continuation of anticoagulants until a durable sinus rhythm is established, defined as freedom from AF and from antiarrhythmic drugs at 12 months [7]. Furthermore, international guidelines for AF management recommend left atrial closure for all at-risk patients undergoing cardiac surgery [1]. In our practice, left atrial appendage closure is considered an integral component of the Maze procedure, and is believed to reduce the risk of perioperative stroke [1,7]. Therefore, anticoagulation therapy is discontinued only if there is documented stable sinus rhythm on follow-up 24-hour Holter monitor, absence of class III antiarrhythmic drugs, and echocardiographic evidence of left atrial contraction. Notably, 88.4% of patients who maintained sinus rhythm demonstrated some degree of atrial contraction on echocardiography. Although atrial contraction is likely important in the long term, it remains unclear whether this translates into a lower incidence of late neurological events through reduced stasis and thromboembolism.
Present guidelines [25,26] recommend standards for following up patients after AF ablation; however, this can be difficult to implement in everyday clinical practice [26],as institutions may not have the capacity to support long-term monitoring. These guidelines also require a multidisciplinary approach to review the patients on an ongoing basis. Therefore, this study implemented a rigid follow-up regimen to guide patient management. Ad et al. [27] reported that efficient follow-up was associated with greater freedom from AF during long-term follow-up. This involved entering patients into an AF registry and collecting clinical data at 3, 6, 9, 12, and 24 months, then yearly thereafter. In addition, the authors developed a protocol/algorithm to guide the associated follow-up. We were particularly active in pursuing a rhythm-control strategy for our patients with AF recurrence to avoid premature acceptance of rate control. We readmitted patients for external electrical cardioversion and resumed antiarrhythmic agents if needed. Current expert consensus is to monitor arrhythmia by non-continuous or continuous monitoring tools [25]. We chose to screen patients with a 24-hour Holter monitor, and more intensive monitoring is associated with a higher likelihood of detecting recurrent AF episodes [25]. The study by Osmancik et al. [28] found that concomitant surgical ablation of AF was associated with a greater likelihood of maintaining sinus rhythm and a decreased risk of stroke at 5-year follow-up, findings consistent with the rhythm outcomes observed in our series.
Our study has several important limitations. This research was a retrospective observational study from a single center. AF recurrences at follow-up were assessed via 24-hour Holter monitoring, which may have failed to detect episodes occurring outside the monitoring window. The low incidence of mortality and cerebrovascular events precluded meaningful multivariate analysis, limiting our ability to identify independent predictors. Thus, larger cohorts with longer follow-up are needed to address this limitation. During surgical AF ablation, we did not use any intraoperative mapping techniques to confirm bidirectional block across ablation lines; this may have resulted in some lines being incomplete. Concomitant use of a three-dimensional mapping system, as used by electrophysiologists, could enable real-time visualization of the ablated tissue in both atria and may improve the accuracy of controlled power delivery and assessment of transmural lesions. We also lacked precise data on the duration of persistent AF before cardiac surgery, a parameter known to influence outcomes. Some patients can have asymptomatic AF, which would also make calculating AF duration difficult. We also had no serial echocardiography data postoperatively to track changes in atrial contractility. Other important limitations include the absence of a control arm and the evolution of ablation technologies since 2018, both of which may affect the generalizability of our longer-term outcomes.
Concomitant complete left and right atrial surgical ablation for long-standing persistent AF in patients undergoing MV surgery appears safe and effective. Implementation of a standardized, protocol-driven local follow-up strategy may help optimize outcomes for both patients and surgeons.
The datasets analyzed during this retrospective study are not publicly available. Public sharing of the data is not feasible, as it would contravene the ethical standards under which this study was approved, compromise participant confidentiality, and breach governing legal requirements regarding data protection. However, restricted access to the data may be granted to specific authorized parties (e.g., peer reviewers, journal editors) upon a legitimate request to the corresponding author, subject to necessary data sharing agreements and ethical oversight.
DA, TAB, SMZR, IC, SE, RLP, and FO contributed to data collection, analysis and interpretation. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was in accordance with the Declaration of Helsinki. Ethics approval was obtained from University Hospitals Coventry and Warwickshire Research & Development department via the Governance arrangements for Research Ethics Committee (GafREC), approval reference number GF1022. The paper is a retrospective series without patient identifiers and individual patient consent is not applicable.
We would like to thank our UHCW Research and Development Department.
SMZ Rahim is supported by a Medtronic fellowship.
The authors declare no conflicts of interest. SMZ Rahim is supported by a Medtronic fellowship.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.