












 , Sijing Huang 1,2, Yanheng Wang 1, Yunfei Zheng 1, Yi Liang 1, Weizhao Huang 1,2,3,4,*
, Sijing Huang 1,2, Yanheng Wang 1, Yunfei Zheng 1, Yi Liang 1, Weizhao Huang 1,2,3,4,*
1 Zhongshan City People's Hospital, 528403 Zhongshan, Guangdong, China
2 The First School of Clinical Medicine, Guangdong Medical University, 524023 Zhanjiang, Guangdong, China
3 Zhongshan Clinical Medicine Research Institute, 528403 Zhongshan, Guangdong, China
4 Institution of Advanced Diagnostic and Clinical Medicine, 528403 Zhongshan, Guangdong, China
Abstract
The clinical outcomes of rheumatic mitral valve repair (MVP) remain controversial, particularly regarding reoperation rates. Therefore, we conducted a meta-analysis to comprehensively and systematically evaluate clinical outcomes, with a focus on reoperation rates.
PubMed, EMBASE, Web of Science, and the Cochrane Library were searched for articles and abstracts published from 1 January 1990 to 21 September 2023, to compare the clinical outcomes of MVP versus mitral valve replacement (MVR) in patients with rheumatic heart disease (RHD).
After screening the titles and abstracts of 2703 articles, a total of 165 articles were reviewed. A total of 20 articles met the inclusion criteria, comprising 4492 MVP and 7913 MVR cases. MVP was associated with lower early mortality (odds ratio (OR): 0.63, 95% confidence interval (CI): 0.50–0.78; p < 0.001) and long-term mortality (OR: 0.57, 95% CI: 0.42–0.77; p < 0.001), as well as reduced rates of thromboembolism (OR: 0.58, 95% CI: 0.46–0.74; p < 0.001), bleeding (OR: 0.70, 95% CI: 0.55–0.89; p = 0.004), and heart failure (OR: 0.28, 95% CI: 0.12–0.67; p = 0.004). There were no significant differences between groups in the incidence of infective endocarditis (p = 0.786), stroke (p = 0.503), or atrial fibrillation (p = 0.180). To analyze reoperation rates more objectively, studies were stratified by surgical era into three subgroups. The risk of reoperation after MVP was high before 2000 (OR: 3.67, 95% CI: 1.98–6.78; p < 0.001). However, from 2000 to 2010, the risk of reoperation decreased but remained high overall, whereas after 2010, the reoperation rate was similar to that observed with MVR.
In patients with RHD, MVP is associated with lower early and long-term mortality, as well as reduced thromboembolism, bleeding, and heart failure compared with MVR. Although MVP historically carried a higher reoperation rate than MVR, this rate has gradually declined in recent years, and since 2010, reoperation rates have not differed significantly between MVP and MVR.
Keywords
- rheumatic heart disease
- mitral valve surgery
- mitral valve repair
- replacement
- reoperation rate
Rheumatic heart disease (RHD) remains the most prevalent valvular heart condition globally, affecting approximately 30 million individuals and causing more than 300,000 deaths annually, with a high incidence in developing countries [1, 2]. RHD most commonly affects the mitral valve and presents with mitral stenosis, mitral regurgitation, or both [3]. The mainstays of treatment are percutaneous balloon mitral valvuloplasty and mitral valve surgery [4, 5]. Although percutaneous balloon mitral valvuloplasty (PMBV) is an important therapeutic option, this method remains unsuitable for cases of severe calcified mitral stenosis, severe mitral regurgitation, or fresh thrombus formation in the left atrium [6]. In severe degenerative mitral valve disease, mitral valve repair (MVP) has been shown to provide significantly better outcomes than mitral valve replacement (MVR) [7, 8]. However, this remains controversial in rheumatic mitral valve disease [9, 10]. Therefore, this study conducted a meta-analysis to compare the clinical outcomes of these two approaches, with a particular focus on reoperation rates.
This meta-analysis was registered with Prospective Register of Systematic Reviews (PROSPERO) (under number CRD42024497774) and follows the guidelines outlined by the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA, Supplementary Content 1) [11], and the A Measurement Tool to Assess Systematic Reviews 2 checklist(Supplementary Content 2) [12].
Four electronic databases (PubMed, EMBASE, Web of Science, and Cochrane Library) were searched to identify relevant articles and abstracts published between 1 January 1990 and 21 September 2023, to compare the clinical outcomes of MVP and MVR in patients with RHD. The keywords searched were “mitral valve” AND (“repair” OR “annuloplasty” OR “reconstruction”) AND “replacement” AND (“rheumatic” OR “Bouillaud’s disease” OR “RHD”).
Studies that (1) involved patients with RHD, (2) directly compared MVP and MVR, and (3) reported at least one clinical outcome were included. Studies were eligible even if concomitant procedures (e.g., aortic valve replacement) were performed, provided a direct comparison between MVP and MVR was reported. Studies that (1) involved patients without RHD; (2) focused exclusively on either MVP or MVR; or (3) were conference proceedings or reviews were excluded. Early mortality was defined as mortality from any cause during hospitalization or within 30 days after surgery. Long-term mortality was defined as death from any cause beyond 30 days after surgery or during follow-up. Reoperation was defined as any subsequent procedure involving the mitral valve. Valve-related events included infective endocarditis, thromboembolism, and bleeding. Adverse events included heart failure, stroke, and atrial fibrillation. Heart failure was defined as a new postoperative heart failure or death due to heart failure. Stroke and atrial fibrillation were defined as new postoperative stroke and new atrial fibrillation after discharge, respectively.
Two reviewers independently extracted and summarized the data according to a uniform format. The reviewers first screened out duplicate or irrelevant studies based on titles and abstracts, then reviewed the full texts to confirm eligibility and extract key data. The extracted information included the names of the study authors, country of origin, and patient statistics (intervention, year of surgery, sample size, age, sex, cardiac function, atrial fibrillation, type of valve replacement, characteristics of mitral lesions, and major additional procedures), as well as results of the main outcome measures. For propensity score-matching studies, data were extracted separately for the pre- and post-matching periods. Any disagreements were resolved through discussion, with a third reviewer consulted as needed to reach consensus.
The risk of bias of the included studies was assessed using the Risk Of Bias In Non-Randomized Studies - of Interventions (ROBINS-I) [13]. Two independent reviewers assessed the risk of bias for each study. In case of disagreement, a third reviewer assessed the data and made the final risk-of-bias judgment.
The odds ratio (OR) was chosen as the primary effect measure for all dichotomous
outcomes because this measure can be calculated from event and sample size data
available in most included studies. Studies that reported only hazard ratios
(HRs) without sufficient data to calculate ORs were noted and considered in
sensitivity analyses but were excluded from the primary pooled synthesis. Stata
18.0 was used to conduct the meta-analysis and generate the relevant graphs.
Heterogeneity among independent studies was assessed using the Q and I2
tests; when heterogeneity was low or absent (I2
After screening the titles and abstracts of 2703 articles, 165 articles were reviewed, of which 20 met our inclusion criteria [14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33]. All 20 were observational studies, which comprised 4492 cases of MVP and 7913 cases of MVR. Following the PRISMA guidelines, the results of the literature search are shown in Fig. 1, a summary of the characteristics of individual studies is shown in Table 1 [14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33], and the prevalence of the main risk factors in each study is shown in Table 2 [14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33].
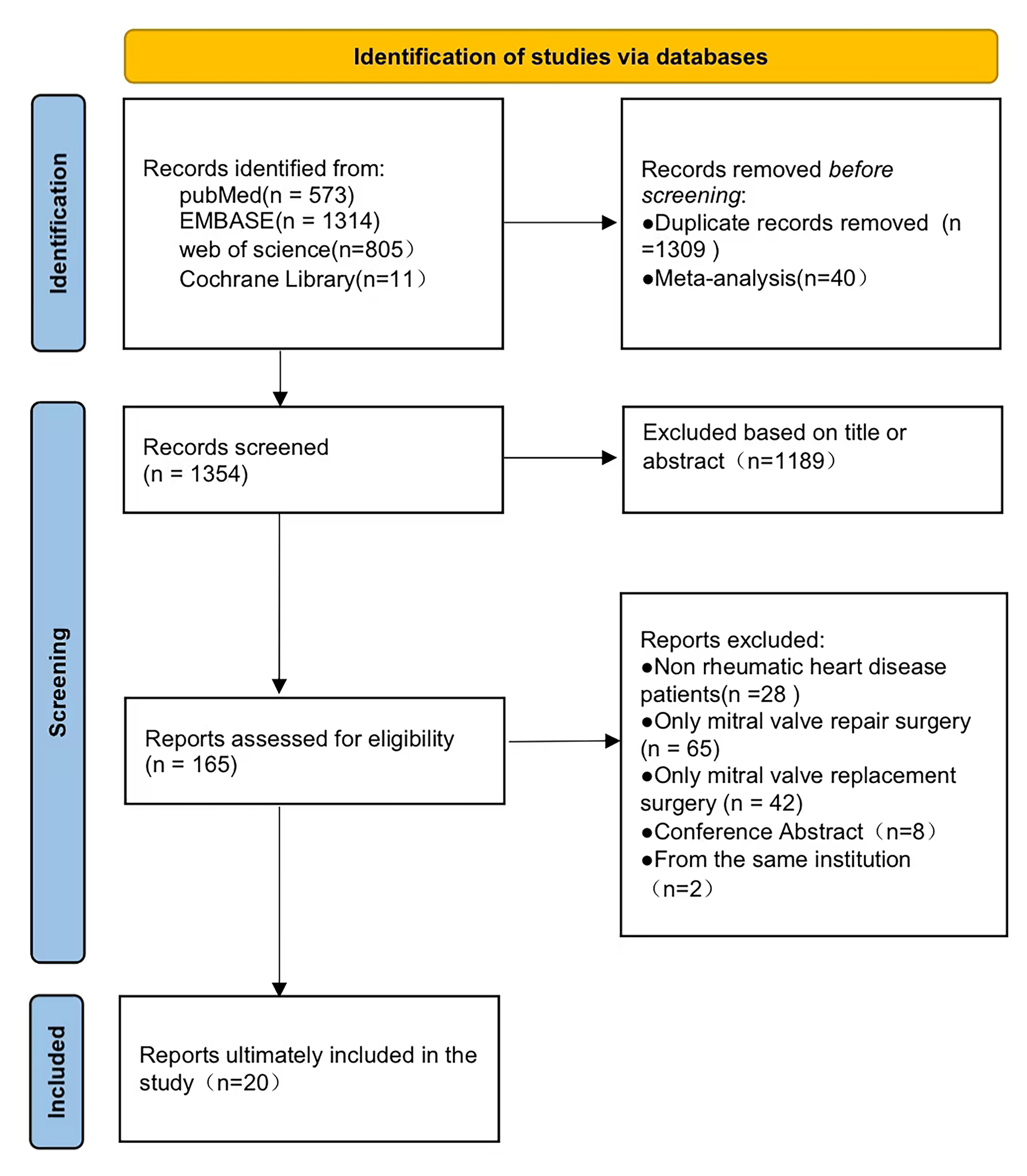 Fig. 1.
Fig. 1.
Findings from the literature search.
| Study | Country | Years of surgery | MVP | MVR | Mean age (years) | Male/female | Mean follow-up years | ||
| MVP | MVR | MVP | MVR | ||||||
| Antunes 1990 [14] | South Africa | 1976–1984 | 241 | 675 | 21.5 | 27.1 | \ | \ | \ |
| Brescia 2022 [15] | USA | 1997–2018 | 80 | 100 | \ | \ | \ | \ | 5.0 |
| Chen 2022 [16] | China (Taiwan) | 2000–2013 | 467 | 467 | 56.8 | 56.7 | 219/248 | 206/261 | 5.9 |
| Cotrufo 1997 [17] | Italy | 1981–1996 | 300 | 240 | 43 | 50 | 34/266 | 66/174 | 6.2 |
| Duran 1991 [18] | Saudi Arabia | 1988–1990 | 136 | 67 | 26.5 | 34 | 65/71 | 32/35 | \ |
| Duran 1994 [19] | Saudi Arabia | 1988–1992 | 306 | 231 | \ | \ | \ | \ | 1.7 |
| Fu 2020 [20] | China | 2011–2019 | 529 | 529 | 54.5 | 54.6 | 147/382 | 147/382 | 4.1 |
| Geldenhuys 2012 [21] | South Africa | 2000–2010 | 69 | 69 | 36.9 | 40.9 | 15/54 | 11/58 | 4.4 |
| Grossi 1998 [22] | USA | 1980–1996 | 725 | 514 | 59.4 | 60.9 | \ | \ | 3.3 |
| Ho 2004 [23] | Vietnam | 1992–2001 | 201 | 408 | 32.2 | 38.7 | 108/93 | 227/181 | 9 |
| Jiao 2019 [24] | China | 2011–2017 | 221 | 700 | 50 | 55.5 | 47/174 | 190/510 | 5.6 |
| Kim 2010 [25] | South Korea | 1997–2007 | 122 | 418 | 41.7 | 51 | 27/95 | 157/261 | 6.0 |
| Kim 2018 [26] | South Korea | 1997–2005 | 294 | 1437 | 43.9 | 54 | 70/224 | 471/966 | \ |
| Kuwaki 2007 [27] | Japan | 1981–2003 | 47 | 81 | 48 | 53 | 14/33 | 34/47 | 8 |
| Krishna Moorthy 2018 [28] | Malaysia | 1992–2015 | 336 | 83 | 12.3 | 13.8 | 133/203 | 36/47 | 3.9 |
| Remenyi 2013 [29] | New Zealand | 1990–2006 | 48 | 33 | 11.7 | 14.4 | 28/20 | 11/22 | 5 |
| Russell 2017 [30] | Australia | 2001–2013 | 119 | 1078 | 57.3 | 62 | 50/69 | 309/769 | \ |
| Talwar 2007 [31] | India | 1995–2005 | 76 | 293 | 30.3 | 32.5 | 53/23 | 211/82 | 5.8 |
| Wang 2008 [32] | China (Taiwan) | 1997–2005 | 33 | 59 | 49.7 | 58.1 | 12/21 | 20/39 | 3.0 |
| Yau 2000 [33] | Canada | 1978–1995 | 142 | 431 | 42 | 57.9 | 21/121 | 88/343 | 5.7 |
MVP, mitral valve repair; MVR, mitral valve replacement.
| Study | MECH (%) | NYHA (II/III/IV%) | AF (%) | MR (%) | MS (%) | MR + MS (%) | CS TVP (%) | CS AVR (%) | |||||||
| MVP | MVR | MVP | MVR | MVP | MVR | MVP | MVR | MVP | MVR | MVP | MVR | MVP | MVR | ||
| Antunes 1990 [14] | 57.2 | \ | \ | \ | \ | 73.0 | 77.6 | \ | \ | \ | \ | \ | \ | \ | \ |
| Brescia 2022 [15] | \ | \ | \ | \ | \ | \ | \ | \ | \ | \ | \ | \ | \ | \ | \ |
| Chen 2022 [16] | \ | \ | \ | 57.4 | 58.0 | 19.3 | 18.8 | 65.1 | 65.5 | 15.6 | 15.6 | 26.3 | 27.2 | 22.1 | 21.0 |
| Cotrufo 1997 [17] | 100 | \ | \ | 36.0 | \ | \ | \ | \ | \ | \ | \ | \ | \ | \ | \ |
| Duran 1991 [18] | 46.2 | 8.1/74.2/16.9 | 4.48/80.6/13.4 | 32.2 | 46.3 | 56.6 | 29.9 | \ | \ | 43.4 | 70.1 | \ | \ | \ | \ |
| Duran 1994 [19] | 38.0 | \ | \ | \ | \ | \ | \ | \ | \ | \ | \ | \ | \ | \ | \ |
| Fu 2020 [20] | \ | \ | \ | 67.9 | 69.6 | 12.7 | 10.2 | 10.4 | 11.9 | 76.9 | 77.9 | 91.1 | 89.2 | 18.9 | 19.8 |
| Geldenhuys 2012 [21] | 91.3 | \ | \ | 29.0 | 39.0 | 56.6 | 18.3 | 4.3 | 10.7 | 39.1 | 71.0 | 5.8 | 2.9 | \ | \ |
| Grossi 1998 [22] | 100 | \ | \ | \ | \ | 49.1 | 27.8 | \ | \ | \ | \ | \ | \ | \ | \ |
| Ho 2004 [23] | 99.0 | 79.6/17.9/1.5 | 83.8/15.2/0.5 | 36.8 | 60.3 | 37.4 | 12.7 | 30.3 | 59.1 | 32.3 | 28.2 | 28.9 | 32.4 | 100 | 100 |
| Jiao 2019 [24] | 72.6 | \ | \ | \ | \ | \ | \ | \ | \ | \ | \ | 90.0 | 89.7 | 13.1 | 27.8 |
| Kim 2010 [25] | 100 | \ | \ | 72.9 | 82.5 | 26.2 | 66.0 | 67.2 | 14.8 | 8.2 | 19.1 | \ | \ | \ | \ |
| Kim 2018 [26] | 78.9 | \ | \ | 56.8 | 75.2 | 61.6 | 17.5 | 24.1 | 46.4 | 14.3 | 36.1 | 33.6 | 43.2 | 17.3 | 34.3 |
| Kuwaki 2007 [27] | 81.5 | -/-/12.7 | -/-/18.1 | \ | \ | 8.5 | 6.2 | 83.0 | 54.3 | 8.5 | 39.5 | 17.0 | 40.7 | 100 | 100 |
| Krishna Moorthy 2018 [28] | 83.1 | II + III + IV: 70.5 | II + III + IV: 66.3 | \ | \ | 93.8 | 90.4 | 0.9 | 4.8 | 5.4 | 4.8 | 31.5 | 14.4 | \ | \ |
| Remenyi 2013 [29] | 100 | 2.79 |
2.81 |
6.0 | 21.0 | 86.0 | 87.9 | 8.0 | 0 | 6.0 | 12.1 | \ | \ | \ | \ |
| Russell 2017 [30] | 100 | III + IV: 42.9 | II + III + IV: 66.3 | 26.1 | 48.9 | 74.8 | 24.7 | 6.7 | 34.2 | 18.5 | 41.1 | \ | \ | \ | \ |
| Talwar 2007 [31] | 100 | II + IV: 48.0 | III + IV: 45.5 | 48.7 | 38.3 | 15.8 | 13.2 | 40.8 | 44.4 | 43.4 | 42.4 | \ | \ | 100 | 100 |
| Wang 2008 [32] | 69.5 | 12.5/66.7/18.2 | 5.1/42.4/8.5 | 93.9 | 96.6 | 14.4 | 14.4 | 15.2 | 15.2 | 70.7 | 70.7 | 45.5 | 61.0 | \ | \ |
| Yau 2000 [33] | 62.4 | 25/63.2/11.8 | 28.1/64.1/7.8 | 31.7 | 64.3 | 16.2 | 14.8 | 67.6 | 48.0 | 16.2 | 37.1 | 7.8 | 18.1 | \ | \ |
MECH, mechanical valves; NYHA, New York Heart Association; AF, atrial fibrillation; MR, mitral regurgitation; MS, mitral stenosis; CS, concomitant surgery; TVP, tricuspid valve; AVR, aortic valve replacement.
The statistical analysis revealed no significant heterogeneity (I2 =
11.2%; p = 0.317); therefore, a fixed-effects model was used for the
meta-analysis. The merger effect was statistically significant. MVP was found to
significantly reduce the risk of early mortality compared with MVR (OR, 0.63;
95% CI: 0.50–0.78; p
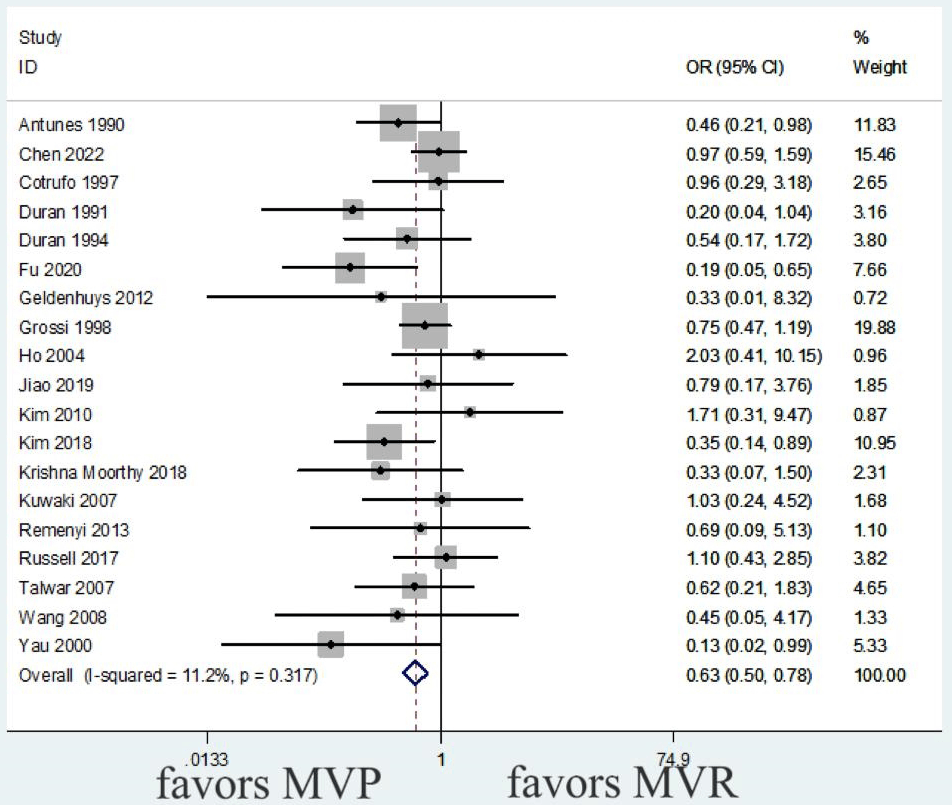 Fig. 2.
Fig. 2.
Meta-analysis of early mortality between MVP and MVR. MVP, mitral valve repair; MVR, mitral valve replacement.
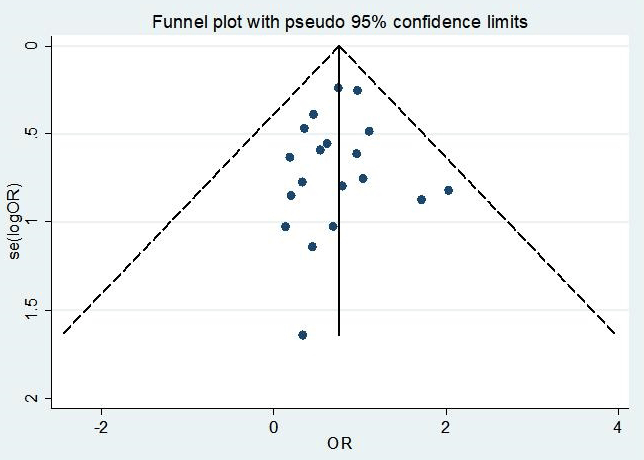 Fig. 3.
Fig. 3.
Funnel plot of early mortality.
| Outcome | Subgroup | N | Heterogeneity test | Z test | OR (95% CI) | Publication bias | |||
| pH | I2 (%) | pZ | Fixed model | Random model | pB | pE | |||
| Early mortality | 19 | 0.317 | 11.2 | 0.63 (0.50–0.78) | 1.000 | 0.662 | |||
| Long-term mortality | 14 | 0.001 | 61.8 | 0.57 (0.42–0.77) | 0.743 | 0.118 | |||
| Reoperation rate | 0.048 | 44.6 | 2.73 (1.86–4.00) | 0.837 | 0.776 | ||||
| Before 2000 | 5 | 0.042 | 59.7 | 3.67 (1.98–6.78) | 0.221 | 0.041 | |||
| 2000–2010 | 5 | 0.090 | 50.3 | 0.040 | 2.16 (1.04–4.50) | 0.806 | 0.541 | ||
| After 2010 | 2 | 0.286 | 12.3 | 0.222 | 1.81 (0.70–4.68) | 1.000 | \ | ||
| Valve-related events | 0.127 | 24.3 | 0.67 (0.57–0.79) | ||||||
| Infective endocarditis | 9 | 0.892 | 0 | 0.786 | 1.07 (0.66–1.73) | 0.076 | 0.035 | ||
| Thromboembolism | 10 | 0.088 | 40.4 | 0.58 (0.46–0.74) | 1.000 | 0.208 | |||
| Bleeding | 8 | 0.098 | 24.3 | 0.004 | 0.70 (0.55–0.89) | 0.536 | 0.058 | ||
| Adverse events | 0.804 | 0 | 0.013 | 0.76 (0.62–0.94) | |||||
| Heart failure | 4 | 0.688 | 0 | 0.004 | 0.28 (0.12–0.67) | 0.734 | 0.363 | ||
| Stroke | 5 | 0.933 | 0 | 0.503 | 0.83 (0.48–1.44) | 0.462 | 0.429 | ||
| Fibrillation | 4 | 0.842 | 0 | 0.180 | 0.85 (0.66–1.08) | 0.734 | 0.808 | ||
N, number; pH, p-value of the heterogeneity test; pZ, p-value of the Z test; OR, odds ratio; 95% CI, 95% confidence interval; pB, p-value of Begg’s test; pE, p-value of Egger’s test.
Moderate heterogeneity was revealed in the statistics (I2 = 61.8%;
p = 0.001). Two studies were combined using HR rather than the OR [15, 20]. In line with our protocol, these HRs were not converted to ORs, and the
studies were excluded from the primary pooled analysis to maintain methodological
consistency. Nonetheless, the studies were considered in a qualitative
sensitivity analysis, which confirmed that the associated findings did not
contradict the direction of the overall pooled effect. A sensitivity analysis of
the heterogeneity source was conducted, and the inclusion studies were eliminated
one by one; the results were relatively stable (Supplementary Content 3).
Therefore, the random-effects model was used to estimate the combined effect. MVP
was associated with a significantly reduced risk of long-term mortality compared
with MVR (OR: 0.57, 95% CI: 0.42–0.77; p
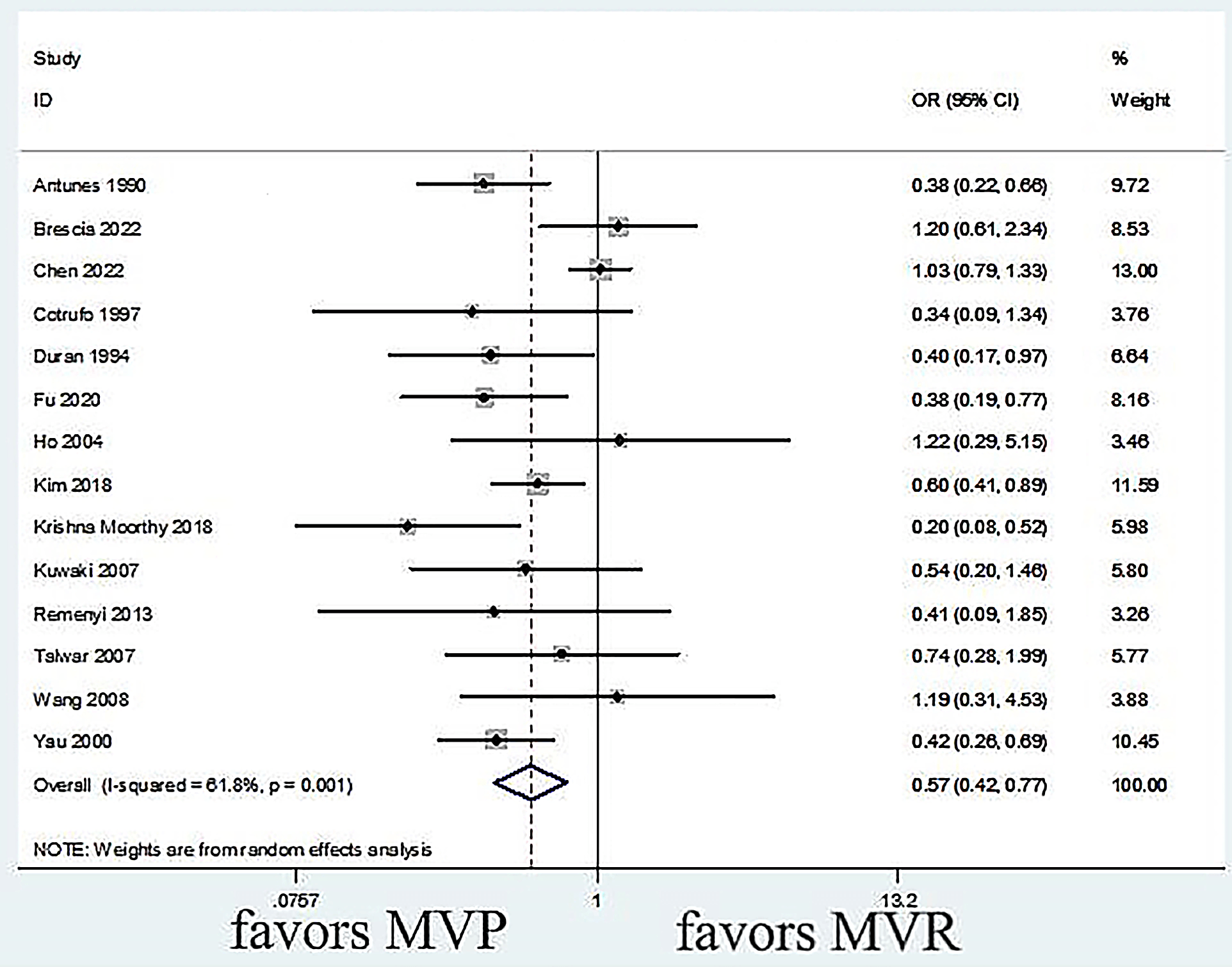 Fig. 4.
Fig. 4.
Meta-analysis of long-term mortality between MVP and MVR. MVP, mitral valve repair; MVR, mitral valve replacement.
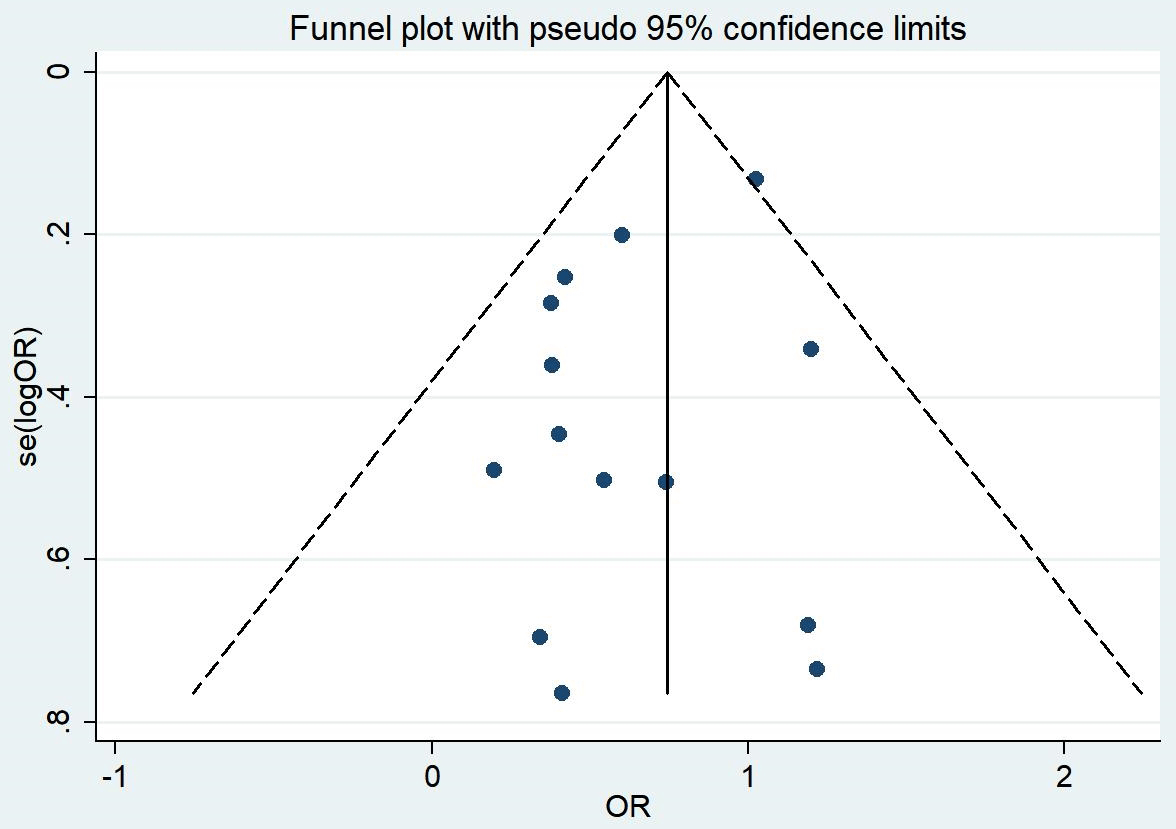 Fig. 5.
Fig. 5.
Funnel plot of long-term mortality.
Statistical analysis indicated mild heterogeneity (I2 = 44.6%; p
= 0.048). Two studies combined HR instead of OR [20, 21]. These studies were
included in a sensitivity analysis to ensure consistency of the overall findings,
but were excluded from the primary pooled OR analysis. A random-effects model was
used, with year of surgery as a subgroup variable. Meanwhile, studies spanning a
wide range of years of surgery were excluded, and those with a narrower span were
retained. Before 2000, MVP was associated with a high risk of reoperation (OR,
3.67; 95% CI: 1.98–6.78; p
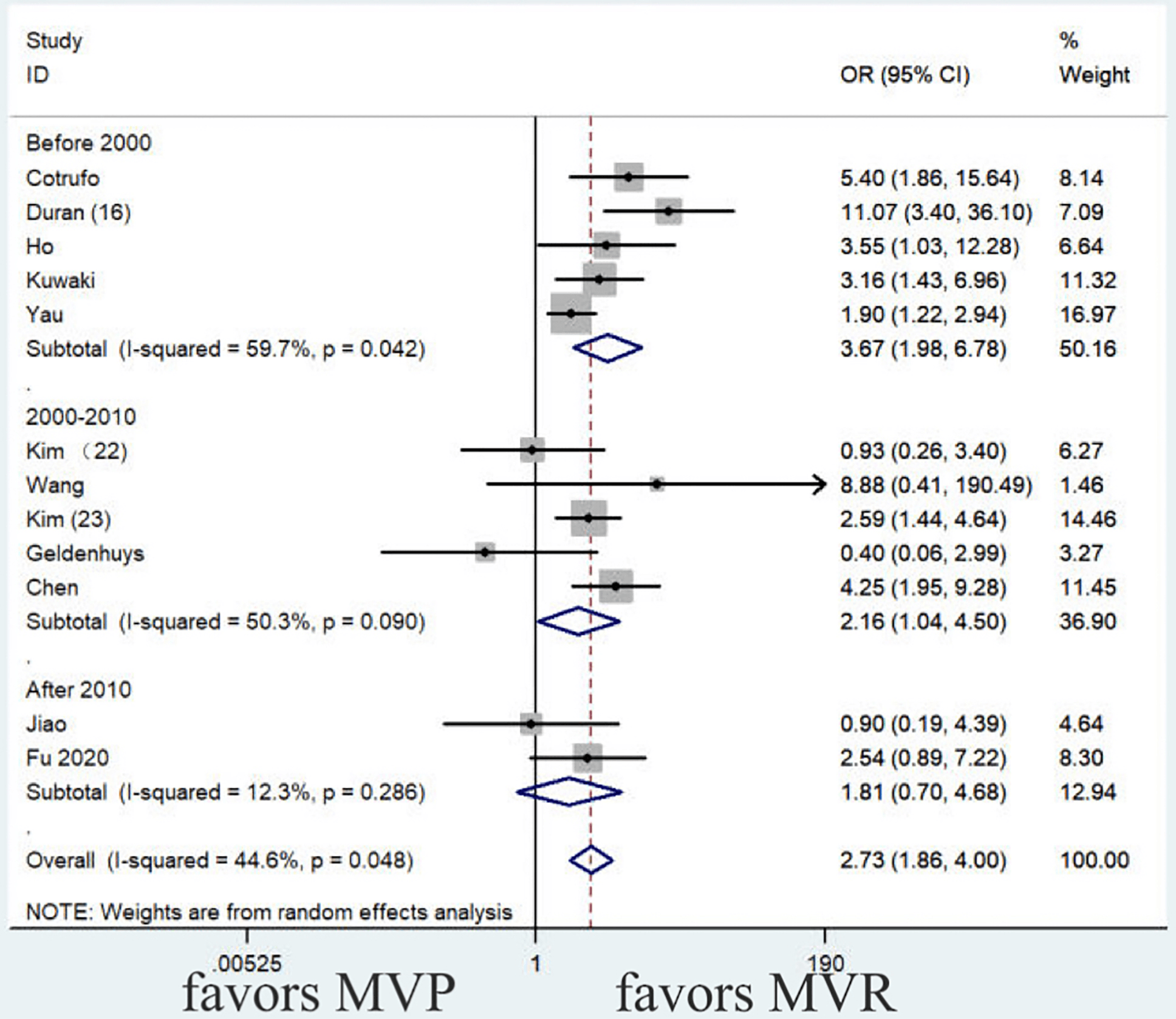 Fig. 6.
Fig. 6.
Meta-analysis of the reoperation rates between MVP and MVR. MVP, mitral valve repair; MVR, mitral valve replacement.
Funnel plots, Begg’s test, and Egger’s test were employed to evaluate
publication bias. The funnel plot was symmetrical (Fig. 7); meanwhile, the
results of the Begg’s test (p
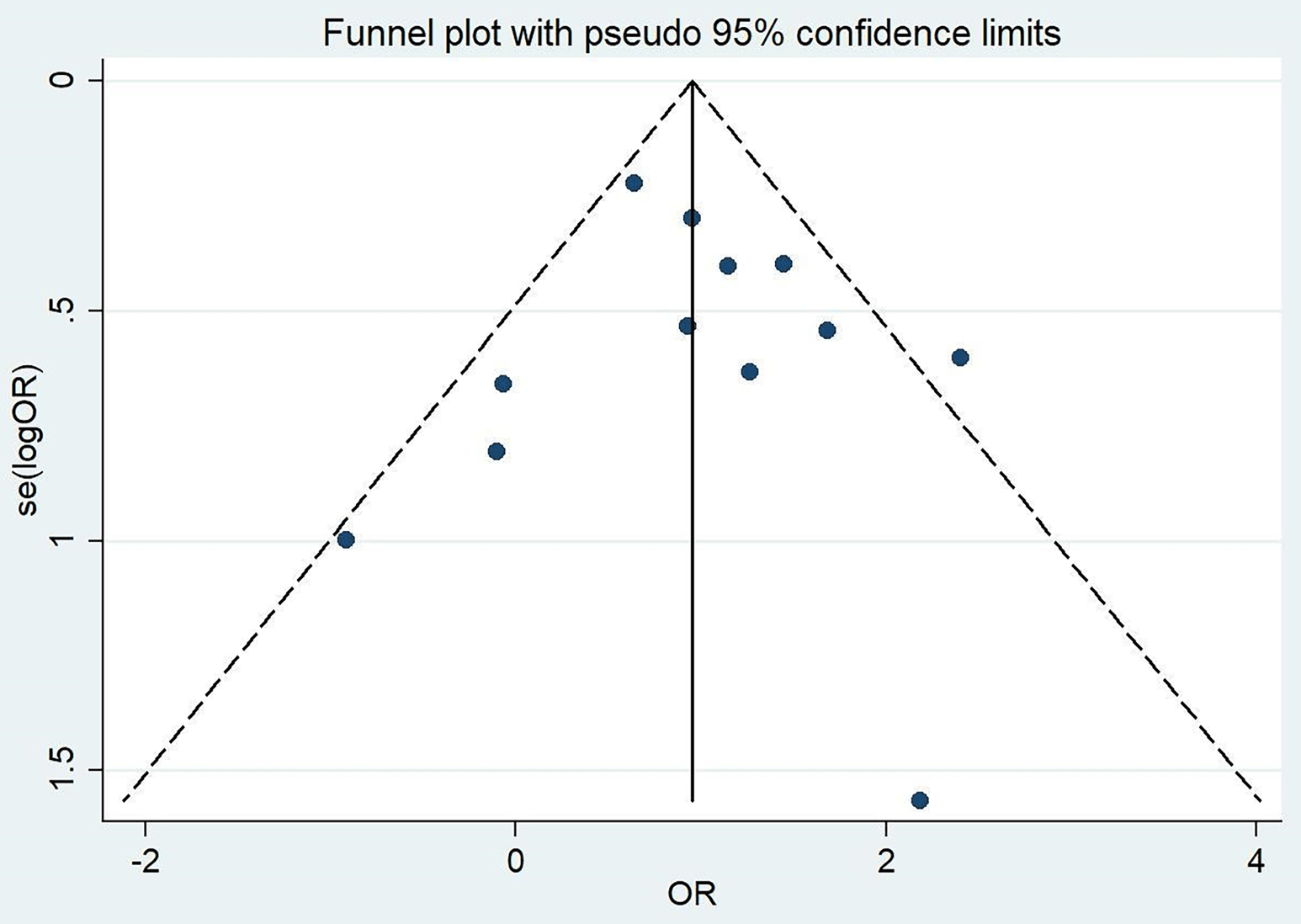 Fig. 7.
Fig. 7.
Funnel plot of reoperation rates.
No heterogeneity was observed across the three subgroups (I2 = 24.3%;
p = 0.127), which were combined using the fixed-effects model. Compared
with MVR, MVP was associated with a reduced risk of thromboembolism (OR: 0.58,
95% CI: 0.46–0.74; p
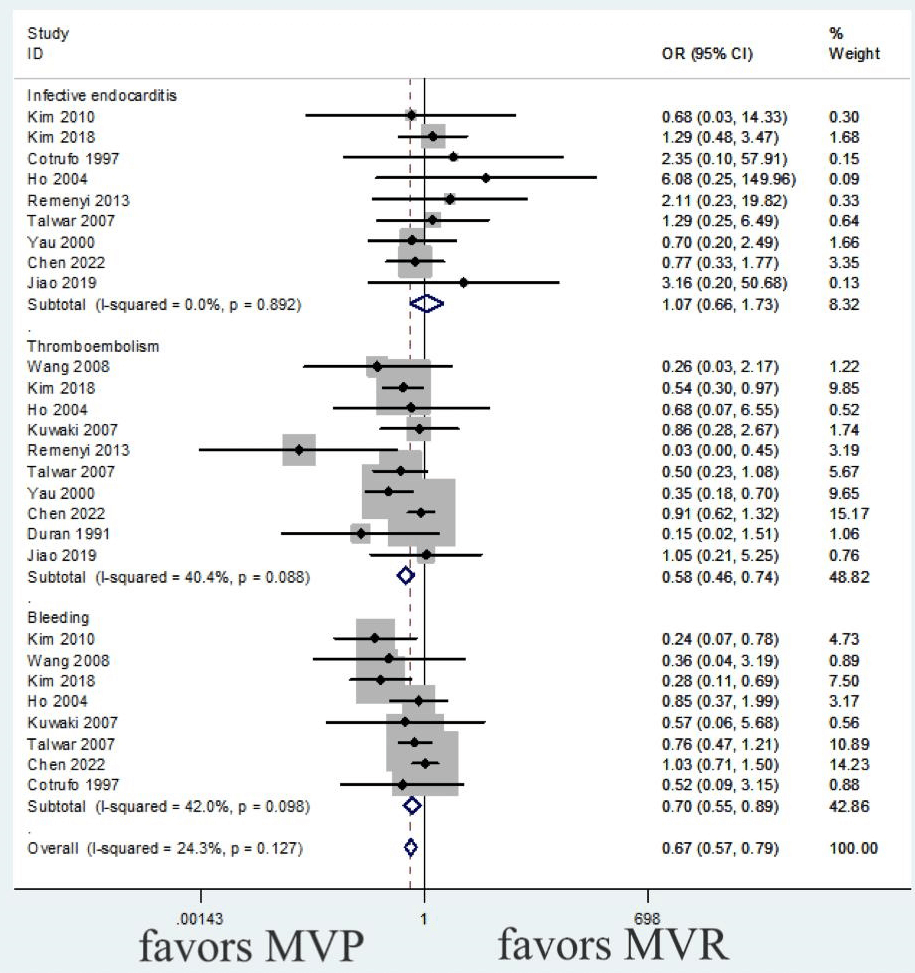 Fig. 8.
Fig. 8.
Meta-analysis of valve-related events between MVP and MVR. Valve-related events include infective endocarditis, thromboembolism, and bleeding. MVP, mitral valve repair; MVR, mitral valve replacement.
No heterogeneity was observed across the three subgroups (I2 = 0.0%; p = 0.779). In the meta-analysis using a fixed-effects model, MVP was more effective than MVR in reducing the risk of heart failure (OR: 0.28, 95% CI: 0.12–0.67; p = 0.004). However, there were no significant differences between the two groups in the risk of stroke (p = 0.503) or atrial fibrillation (p = 0.180) (Fig. 9 and Table 3).
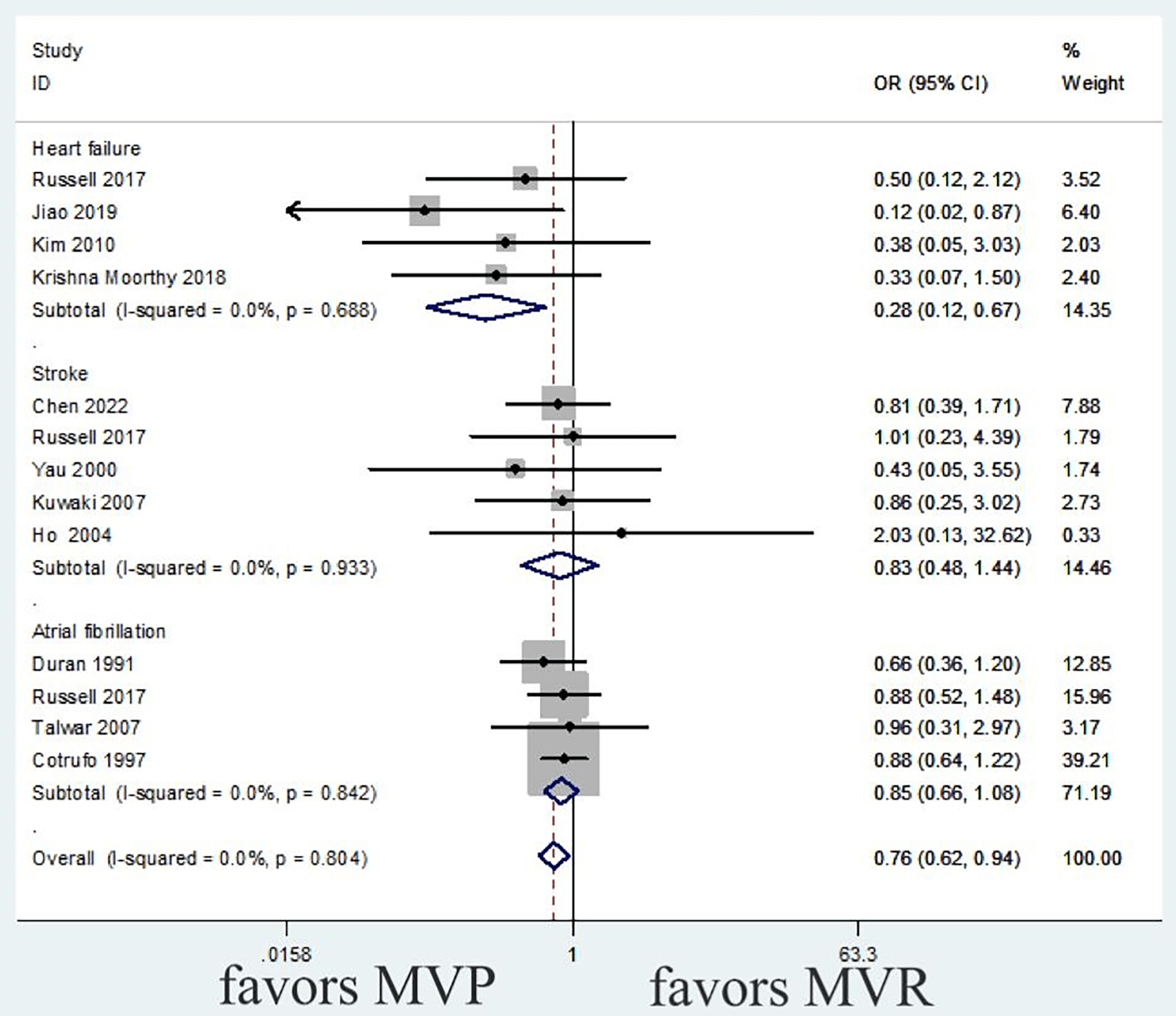 Fig. 9.
Fig. 9.
Meta-analysis of adverse events between MVP and MVR. Adverse events include heart failure, stroke, and atrial fibrillation. MVP, mitral valve repair; MVR, mitral valve replacement.
The overall risk of bias for the included studies, assessed using the ROBINS-I tool, is summarized in Figs. 10,11. Most studies were judged to have a moderate risk of bias, primarily due to potential confounding and selection bias inherent in non-randomized study designs.
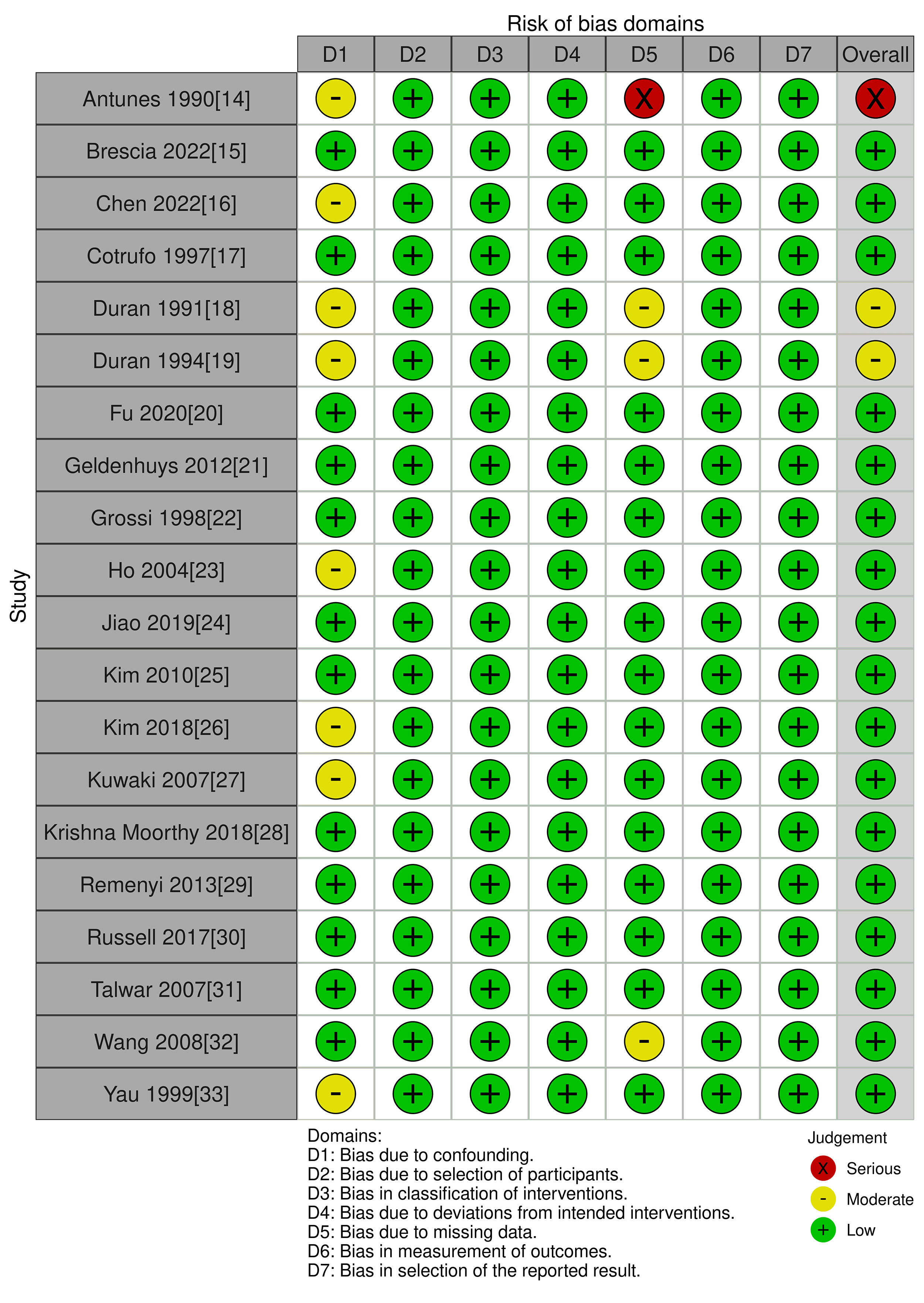 Fig. 10.
Fig. 10.
Risk Of Bias In Non-Randomized Studies - of Interventions (ROBINS-I) tool with traffic lights.
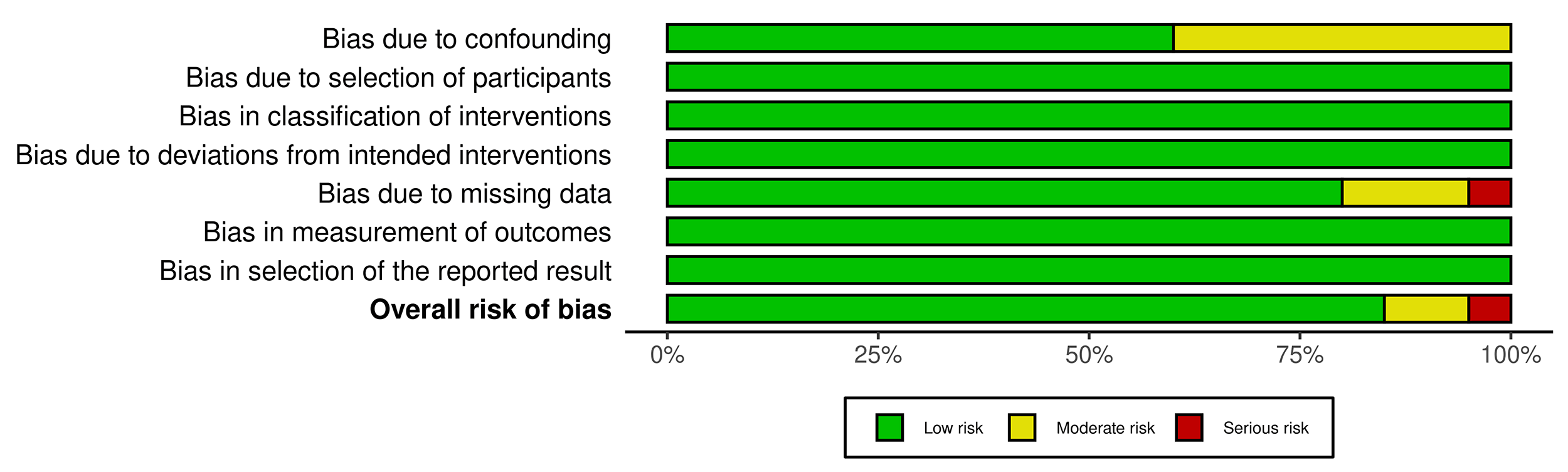 Fig. 11.
Fig. 11.
Risk Of Bias In Non-Randomized Studies - of Interventions (ROBINS-I) tool with summary plot.
In degenerative mitral valve disease, MVP is regarded as the gold standard surgical treatment and is associated with lower early mortality than MVR [34, 35]. The main cause of early postoperative mortality in these patients was cardiac insufficiency. MVP usually avoids the need for resection of subvalvular structures, preserves the integrity of the autologous valve, reduces cardiac damage, and minimizes postoperative recovery time [24, 36]. MVP is also associated with a higher left ventricular ejection fraction [32], reducing the incidence of events such as heart failure due to left ventricular dysfunction [24, 25, 30]. Similarly, in rheumatic mitral valve disease, MVP also achieves superior early survival benefits compared with MVR [37]. This study found that rheumatic MVP significantly reduced early mortality compared with MVR (OR: 0.63), consistent with a previous study [10]. In addition, rheumatic MVP reduces early valve-related complications, including valve detachment and valve thrombosis, which likely contributes to the observed reduction in early mortality [20, 38, 39].
This study found that rheumatic MVP was associated with lower long-term
mortality than MVR (OR, 0.57; 95% CI: 0.42–0.77; p
The most controversial issue is reoperation; however, analyzing all studies together is unreasonable owing to significant changes in case selection and surgical techniques over time. Therefore, the studies were divided into three subgroups and evaluated based on the year of surgery. Studies before 2000 consistently reported a high risk of reoperation for MVP [17, 19, 23, 27, 33]. Degenerative mitral valve lesions are mainly characterized by localized pathological damage. In contrast, RHD affects the entire mitral valve apparatus, including the annulus, valve body, subvalvular tendon cords, and papillary muscles, which may be damaged and altered to varying degrees [44]. The degree of pathologic damage to the rheumatic mitral valve is generally accepted to affect the application of the repair techniques [45, 46]. Furthermore, Yau et al. [33] showed that factors such as significant damage to the mitral valve tissue contribute to a higher rate of repair failure. In patients with RHD, MVP combined with aortic valve replacement, compared with MVR combined with aortic valve replacement, has been reported by Ho et al. [23] to have a significantly higher reoperation rate. This is mainly due to the progression of mitral valve disease and the deterioration of the bioprosthetic aortic valve [10, 47]. Therefore, MVP should be limited to repairing lesions with better durability. The reoperation rates after MVP are also influenced by age [44, 48], and Duran et al. [19] found a higher failure rate among patients under 20 years of age who opted for MVP than among older patients with rheumatic MVP. Therefore, the higher reoperation rates reported in studies prior to 2000 may be partly attributable to inappropriate case selection.
The period from 2000 to 2010 was transitional, and studies have shown that the risk of reoperation has trended downward, although large inter-institutional variations in reoperation rates remain. Chen et al. [16] and Wang et al. [32] showed that MVP had a higher reoperation rate than MVR and identified factors associated with higher mitral valve reoperation rates, including prior percutaneous transvenous mitral commissurotomy and complex valve pathology. Chen et al. [16] also concluded that having an experienced surgeon evaluate mitral calcification and rheumatologic activity in early-stage patients with rheumatic mitral regurgitation is important. Kim et al. [26] showed that MVP has a favorable outcome compared to mechanical valve replacement for RHD in selected patients. MVP has better durability than mechanical valve replacement in RHD, and there was no significant difference in the incidence of reoperation between the two approaches. At this center, MVP is primarily managed with junctional dissection, and valve replacement is more frequently chosen when severe fibrosis or calcification impairs the mobility of the anterior leaflet or involves subvalvular structures. These findings suggest that rational patient selection and advancements in surgical technique have led to improved reoperation rates for rheumatic MVP [25, 26, 49]. Nonetheless, further research is needed to identify specific pathological subtypes of rheumatic mitral disease that derive the most benefit from MVP, as the included studies did not provide sufficient detail for such a subgroup analysis.
Since 2010, two studies have shown that there is no longer a significant difference in reoperation rates between MVP and MVR [20, 24]. The current understanding of rheumatic mitral valve disease is improving, and MVP techniques have also improved significantly. Recently, Gillinov et al. [50] suggested several reasons for reoperation following rheumatic MVP, including suture dehiscence, shortened tendon cable rupture, incorrect selection of the shaped ring size, and lack of valve tissue. Therefore, the operator must have a good understanding of the severity of the valve lesion, choose the appropriate repair method, and demonstrate successful repair experience [37]. Findings from the post-2010 period should be interpreted with caution. This subgroup included only two studies, leading to wide CIs and reduced statistical power. While the trend suggests a convergence of reoperation rates, more contemporary, large-scale studies are needed to confirm this observation definitively.
Important advances in rheumatic MVP have been made in recent years. Some researchers have proposed a three-part clinicopathologic triage of rheumatic mitral valves [51], comprising leaflet thickening, subvalvular structure thickening, and a mixed type. This typing method can help surgeons assess the condition of a patient more accurately and, thus, develop more personalized treatment plans [52]. Building on this foundation, researchers have developed a standardized procedure for rheumatic MVP surgery-the “SCOR” procedure, specifically designed to repair the fused commissure [20, 24, 51, 52]. The four procedures include shaving junctional fibroplaques, checking the natural junctional area, performing junctional commissurotomy, and relaxing adhesions in the subvalvular structures. This approach has yielded significant clinical results in practice, simplifying the procedure and significantly decreasing the reoperation rate [20, 24]. These advances have greatly contributed to the development of rheumatic MVP. Therefore, we believe that rational case selection and continued improvement of repair techniques are key initiatives that have led to optimal results in rheumatic MVP.
This meta-analysis has several limitations. First, the studies included in this review were primarily retrospective cohort studies, with no randomized controlled trials. Second, the sample sizes of some studies were small, which unavoidably increased selection bias in the analysis. Third, the studies were conducted in different countries, which may be heterogeneous; furthermore, several studies did not report baseline parameters for patients, making obtaining complete baseline data for all patients challenging. Fourth, our primary analysis relied on odds ratios for long-term outcomes such as mortality and reoperation. We acknowledge that the hazard ratio (HR) is the preferred and more appropriate measure for time-to-event data, as this measure inherently accounts for varying follow-up durations across studies. However, a primary meta-analysis based on HRs was not feasible due to inconsistent and often absent reporting of time-to-event data (such as log-rank statistics or CIs for HRs) in many of the included publications, particularly older ones. Hence, our choice of an OR-based approach was a pragmatic decision to maximize the inclusion of available evidence and provide a comprehensive overview. This limitation should be considered when interpreting the magnitude of the long-term effects. Furthermore, this meta-analysis was limited by inconsistent reporting of key intraoperative and postoperative variables across the included studies, including operative time, residual mitral regurgitation, and left atrial remodeling. This heterogeneity in reporting precluded a quantitative synthesis of these clinically relevant outcomes. Finally, our analysis of reoperation rates did not formally account for the competing risk of mortality. Since mortality differs between the MVP and MVR groups, this may have influenced the observed reoperation rates, which remain a limitation of the available literature.
In patients with RHD, MVP reduces early and long-term mortality, thromboembolism, bleeding, and heart failure compared with valve replacement. With appropriate patient selection and advances in repair techniques, reoperation rates have significantly decreased, especially after 2010. Currently, there is no significant difference in reoperation rates between repair and replacement. In conclusion, MVP is the preferred treatment option for selected patients with RHD.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
CY: conception, design, materials, data collection, analysis, literature review, and writing. SH: design, materials, data collection, and writing. YW: materials, data collection, and writing. YZ: materials, data collection, and writing. YL: analysis, supervision, and critical review. WH: supervision, materials, data collection, analysis, writing, and critical review. All authors contributed to the editorial revision of the manuscript, read the final version, and gave their approval for publication. All author has participated sufficiently in the work to take public responsibility for relevant parts of the content, and agreed to be accountable for all aspects of the research in upholding its accuracy and integrity.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/HSF47165.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.