




 , Marcos Nores 1, Sotiris Stamou 2
, Marcos Nores 1, Sotiris Stamou 21 HCA Florida JFK Hospital, Atlantis, FL 33462, USA
2 Lewis Gale Medical Center, Roanoke, VA 24153, USA
Abstract
Cardiac surgery has undergone significant innovation over the past several years. The increased use of robotic surgery and transcatheter therapies has expanded the armamentarium of interventions available to patients. Here, we discuss the recent technological developments in coronary revascularization, structural heart procedures, and the surgical management of atrial fibrillation and heart failure, with particular emphasis on feasibility, clinical applicability, and potential for further innovation.
Keywords
- structural heart
- heart failure
- coronary revascularization
- atrial fibrillation
- transcatheter
- robotic
The surgical treatment of cardiovascular disease continues to evolve as innovative technologies enable increasingly minimally invasive approaches. Conventional sternotomy remains the most commonly performed approach for coronary artery bypass grafting (CABG) and surgical valve procedures. Studies of minimally invasive techniques suggest survival and hemodynamic outcomes comparable to those of traditional sternotomy, while offering a shorter length of stay, reduced intubation time, and lower infection rates. Although these studies continue to present data demonstrating these benefits, the applicability of these approaches to general community practice is limited by the highly selected patient populations studied and the institution-specific protocols involved.
The range of procedures that can be performed robotically depends on the complexity of the surgery and the skill set of the surgeon, which has a significant learning curve. This poses challenges for early-career cardiac surgeons, who must continually adapt to rapidly evolving surgical technologies and operative approaches. Despite the increasing use of robotic technology in other surgical specialties, there is still no consensus on robotic minimally invasive approaches in cardiovascular surgery.
Transcatheter approaches have also gained favor, particularly for use in high-risk surgical patients. As these transcatheter devices are improved and studied with longer follow-up, there is potential for their use as first-line treatment options in lower-risk surgical patients. This would shift the patient population for cardiac surgeons toward managing complications of transcatheter therapies.
The surgical management of heart failure has not yet fully incorporated a minimally invasive approach as surgeon-scientists continue to develop and optimize the total artificial heart (TAH). Nevertheless, it is reasonable to expect artificial heart models that can be implanted using a minimally invasive approach. Indeed, some institutions are already exploring robotic and minimally invasive approaches for donor heart transplants.
In this narrative literature review, we summarize emerging approaches and evolving technologies in coronary revascularization, structural heart surgery, atrial fibrillation, and heart failure. Specifically, we discuss current and emerging technologies and approaches in modern cardiac surgery, as well as the potential for further innovation and incorporation into daily practice and surgical training.
We performed a narrative review of recent advancements in selected fields of cardiac surgery, addressing the following pathologies: coronary artery disease, structural heart disease, atrial fibrillation, and heart failure. Systematic and narrative reviews were identified in PubMed, prioritizing but not limited to publications from 2018 to 2025. Articles relevant to the topics of interest were included, prioritizing the following study types in descending order: meta-analyses, randomized controlled trials, and prospective or retrospective studies.
Coronary artery bypass surgery has undergone considerable innovation toward minimally invasive techniques since the 1990s. Bonatti et al. [1] report the distribution of minimally invasive coronary revascularization procedures in a literature review from 1996 to 2019, identifying minimally invasive direct coronary artery bypass (MIDCAB) as the most common approach, followed by robotic MIDCAB. The evolution of these minimally invasive techniques is summarized in Fig. 1.
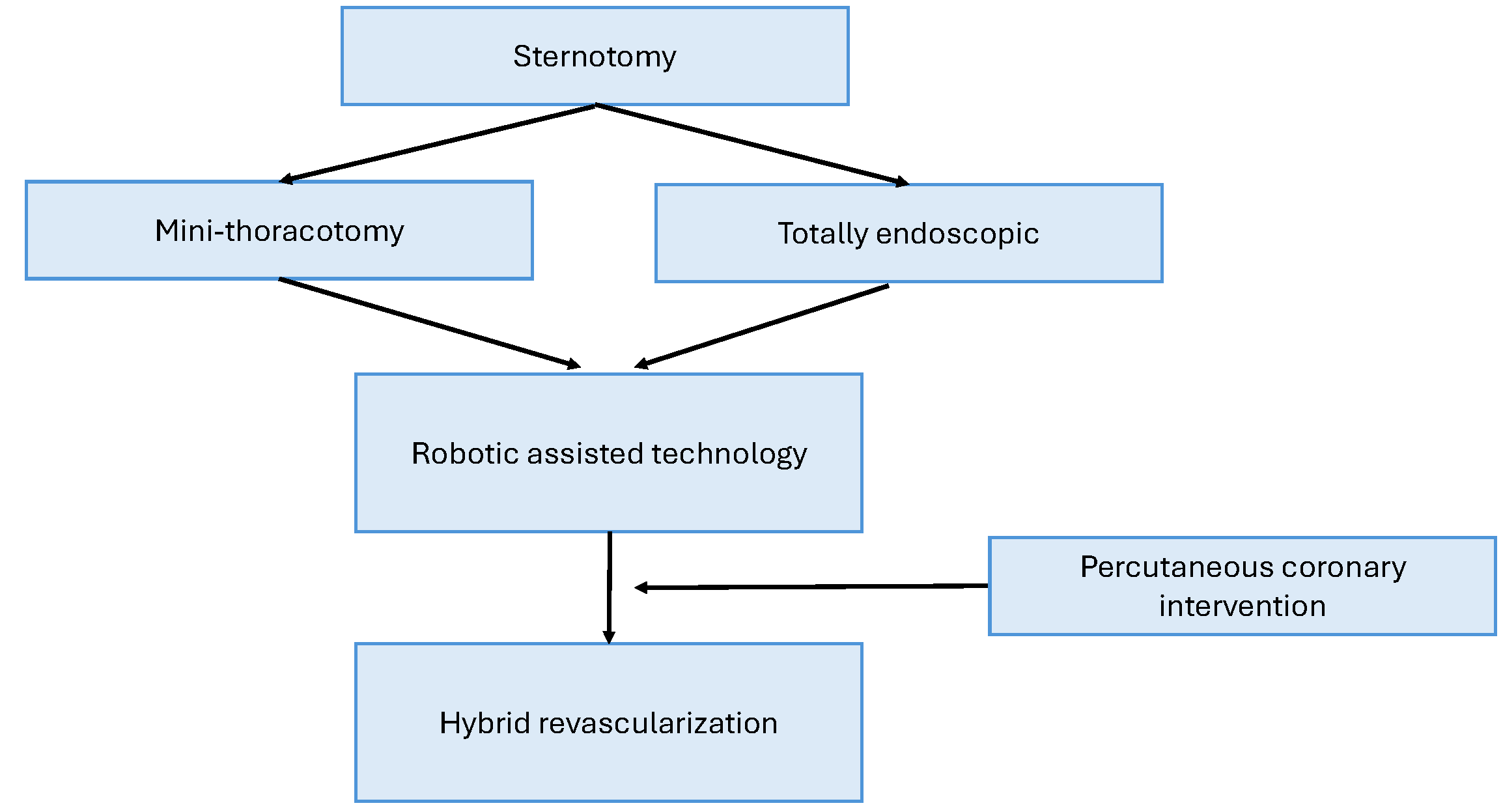 Fig. 1.
Fig. 1.
The evolution of coronary revascularization approaches. Coronary revascularization has progressed from sternotomy to minimally invasive approaches using thoracoscopy and robotics, and is now frequently combined with percutaneous coronary interventions.
There are numerous approaches to minimally invasive CABG, the most common of which is MIDCAB, which accounted for 46.9 percent of minimally invasive procedures performed between 1996 and 2019. Meanwhile, robotic MIDCAB represents 15.8% of these procedures. Other variations of minimally invasive CABG include totally endoscopic CABG (TECAB) and robotic TECAB [1].
MIDCAB typically involves a mini-left thoracotomy with stabilization of the target vessel on the beating heart. The single graft is typically the left internal mammary artery (LIMA); however, the right internal mammary artery (RIMA) can also be harvested, requiring an average of 28.5 minutes compared with 22.2 minutes for LIMA harvesting [1, 2]. The 5-year survival rate was similar at approximately 91% [3]. Video-assisted MIDCAB is performed with the patient in the right lateral decubitus position. The LIMA is then harvested through two thoracoscopic ports, and the anastomosis is completed via a left mini-thoracotomy. LIMA harvesting times are nearly twice those of conventional MIDCAB, adding roughly an hour to the total operating time. Across several studies, operative times ranged from 2 to 5.3 hours [4, 5, 6, 7, 8].
Robotic MIDCAB similarly uses a camera port and two instrumental ports in conjunction with a mini-thoracotomy. It has been reported to require an average of 4 hours per graft, most commonly using the LIMA [1]. Meanwhile, postoperative complication rates are comparable to those of non-robotic MIDCAB, although the conversion rate to a larger incision is higher (6.6% versus 1.7%). Robotic MIDCAB has been associated with a reduction in length of stay by approximately 4 days and a similar 5-year survival rate (94%) compared with sternotomy.
On-pump CABG via a mini-thoracotomy is similar to MIDCAB but uses cardiopulmonary bypass established through peripheral vessels, typically the femoral artery and vein. Although this exposes the patient to cardiopulmonary bypass, the technique eliminates the challenges of beating-heart bypass and provides improved exposure by unloading the heart. Although operative times are similar to MIDCAB, with IMA harvesting times comparable to those of video-assisted MIDCAB, some surgeons were able to perform an average of three bypasses in a single operation [9].
TECAB eliminates the need for a mini-thoracotomy, with camera and instrument ports positioned similarly to those in robotic MIDCAB. TECAB is reportedly technically challenging but the least invasive option, with a reported conversion rate to a larger incision of up to 45.1% and longer LIMA harvesting times (average of 77 minutes) [10, 11]. Robotic TECAB uses a robotic platform similar to that used for MIDCAB but without a sternotomy. Notably, robotic assistance has facilitated the effective application of TECAB by improving IMA harvesting times, 55 minutes for the LIMA and 32 minutes for the RIMA [12]; meanwhile, the mean number of bypass grafts per procedure was 1.4. The conversion rate to a larger incision has been reported at 10.3%, and the 3-year survival approached 96% [13, 14].
Minimally invasive coronary artery bypass has been shown to decrease hospital stay and eliminate the exposure to the potential complications associated with cardiopulmonary bypass. Although patients generally prefer the least invasive approach, there remains significant potential for conversion to a sternotomy, and broader applicability to the general population is limited by the experience of the surgeon with the robot. Existing studies on minimally invasive coronary artery bypass are not randomized for direct comparison with sternotomy. Furthermore, these approaches are generally limited to high-volume, specialized centers that offer a specific approach, which prevents adequate comparison across different types of minimally invasive procedures. Moreover, controlling patient-specific factors that can significantly affect postoperative outcomes, such as the extent of coronary artery disease and the experience of the surgeon using minimally invasive approaches, is challenging. Therefore, these procedures may be more likely to be offered to lower-risk operative candidates.
Given that operative times for robotic MIDCABG are longer than those for
sternotomy, proponents have advocated a hybrid approach combining minimally
invasive coronary bypass with percutaneous coronary intervention (PCI), which can
offer similar postoperative benefits, including reduced hospital length of stay,
infection rates, and ventilator time. The argument for hybrid coronary
revascularization is supported by evidence of superior 1-year patency with the
newest drug-eluting stents compared with saphenous vein grafts (95% versus 80%)
[15]. Hybrid revascularization offers survival rates (99%) and stroke rates
(
However, hybrid revascularization is limited to carefully selected patients, typically those with complex left anterior descending artery disease and focal right coronary and circumflex artery disease suitable for stenting. Although MIDCABG can be performed either before or after PCI, some argue for performing MIDCABG before PCI to avoid the increased risk of bleeding associated with antiplatelet therapy. The HREVS trial compared hybrid revascularization with PCI and traditional CABG, using a protocol in which MIDCABG was performed 3 days before PCI and Plavix was initiated on the day of PCI [17]. Hospital length of stay was similar between the hybrid and sternotomy groups. There was no significant difference in repeat revascularization at 1 year among groups, although the CABG group had the lowest rate of repeat revascularization and a significantly higher bleeding rate. The POLMIDES study compared the hybrid strategy with CABG and found similar 12-month rates of survival, myocardial infarction, and repeat revascularization [18], with comparable bleeding between groups. Ding et al. [19] compared off-pump CABG with PCI and simultaneous hybrid revascularization, and found that hybrid therapy was associated with longer operative times and a higher cumulative 10-year repeat revascularization rate. The authors attributed these findings to higher SYNTAX scores and longer follow-up in their study population.
Although the operative costs of hybrid PCI are higher than those of traditional CABG, decreased ventilation and intensive care unit (ICU) length of stay, along with reduced postoperative length of stay, may offset these costs [20]. Since hybrid PCI and CABG account for only 0.48% of CABG volume, further research on outcomes is needed to clarify the postoperative benefits and cost-effectiveness of robotic and hybrid revascularization, particularly when considering the conversion rate to sternotomy [15]. Despite the significant learning curve and increased operative times associated with MIDCAB, the associated cost–benefit analysis, minimally invasive approach, shorter hospital stay, and avoidance of cardiopulmonary bypass support the continued application and long-term study of MIDCAB. Ultimately, decisions regarding hybrid revascularization, MIDCAB, and traditional CABG should be patient-centered and aim to offer improved benefits without completely replacing traditional sternotomy.
Robotic technology has been adopted for minimally invasive valve replacement and repair, particularly in mitral valve surgery, and is increasingly used for aortic and tricuspid valve procedures. Notably, robotic technology can be combined with concomitant interventions, including ablation and additional valve surgeries. Robotic valve surgery requires peripheral cannulation for cardiopulmonary bypass but has the potential to expand the population of surgical candidates for valvular procedures.
Robotic valvular procedures require peripheral cannulation for cardiopulmonary bypass, typically via the femoral, axillary, or jugular vessels. These procedures are performed via a right transaxillary thoracotomy incision, with additional thoracoscopic ports placed bilaterally.
The first robotic surgical aortic valve replacement (SAVR) was performed in 2020. In a study of 300 cases, SAVR was associated with a lower rate of pacemaker implantation: 2.8% compared with 4–8% for sternotomy–SAVR [21]. The median length of stay was 5 days, and the median cross-clamp time was 120 minutes. In a separate study of sternotomy-SAVR, median aortic cross clamping time was 76 minutes and length of stay was 12.5 days [22]. In both of these studies, median aortic valve implant size was 23 mm [21, 22].
Robotic mitral valve repair also has the potential to reduce the length of stay and postoperative pain. Arghami et al. [23] analyzed outcomes following robotic mitral valve repair over 10 years. Follow-up echocardiography showed improved cardiac function, and reoperation rates and survival were similar to those with open sternotomy approaches. The median ICU stay was 18 hours, and the median hospital length of stay was 3 days. The median cardiopulmonary bypass and cross-clamp times were 79.5 and 53 minutes, respectively. These cardiopulmonary bypass and cross-clamp times were comparable to those reported for open sternotomy mitral valve surgery in one study: 97 minutes and 63.4 minutes, respectively [24]. Although robotic approaches may initially have longer cross-clamp and bypass times, Chou et al. [25] reported declining operative times with increasing surgeon experience, especially after performing 30 procedures. Roach et al. [26] found that improved visualization with the robotic approach offsets the loss of tactile feedback associated with traditional sternotomy.
Noda et al. [27] reported successful robotic tricuspid valve repair with sustained echocardiographic improvement at 1 year. Freedom from recurrent tricuspid regurgitation at 1 year was 98% [27]. The authors argued that the robotic approach allows for a vertical right atriotomy, thereby reducing the risk of injury to the inferior vena cava or sinus node. However, cardiopulmonary bypass and cross-clamp times were 242 and 99 minutes, respectively, which were longer than the 135 and 82 minutes reported in a study of open sternotomy for redo tricuspid valve surgery [28].
Femoral cannulation during robotic procedures carries a risk of lower-extremity ischemia, and further studies are needed to identify complications specific to the robotic approach. Concomitant robotic procedures have been described with valve surgery, and additional research is warranted in higher-risk patients with prior sternotomy and mediastinal adhesions.
Further studies are also needed to assess outcomes in higher-risk populations, as robotic aortic valve replacement may represent a viable alternative to transcatheter therapies in select high-risk patients. With broader adoption of the robotic approach, operative times may decrease while still offering shorter lengths of stay and reduced postoperative pain compared with conventional sternotomy.
Surgeons should continue to remain proficient in the traditional sternotomy approach while also preparing to adopt robotic minimally invasive approaches for valvular surgery. Robotic valvular procedures have a significant learning curve and should be undertaken only after gaining adequate experience with sternotomy approaches. Furthermore, valvular calcification can preclude adequate repair via robotic assistance; if debridement is required, sternotomy is necessary [29]. As with robotic coronary artery bypass approaches, the higher operative costs can be offset by shorter lengths of stay; however, successful implementation usually requires a high-volume center to optimize efficiency and operative times for robotic valve procedures.
Transcatheter valve interventions have expanded the population of patients eligible for treatment of valvular disease. Transcatheter approaches were initially tailored for patients considered high risk for surgery, although these approaches are now increasingly applied in younger patients with a low surgical risk profile.
Transcatheter aortic valve implantation (TAVI) continues to evolve, with ongoing improvements in bioprosthetic design that have facilitated the use of this approach in intermediate- and low-risk surgical patients. TAVI implant modifications have included external cuffs for improved intra-annular seating and anti-calcification treatments. Current TAVI options include balloon-expandable and self-expandable devices, some of which are repositionable or retrievable [30].
The MitraClip system, a form of transcatheter edge-to-edge repair (TEER), received approval from the United States Food and Drug Administration (FDA) for primary mitral regurgitation in 2013 and for secondary mitral regurgitation in 2019. The PASCAL transcatheter device, currently under investigation, uses two clasps and paddles to grasp the mitral leaflets, while a central spacer reduces regurgitation. All transcatheter edge-to-edge repair techniques require specific anatomic criteria to achieve optimal outcomes. Transcatheter mitral valve replacement (TMVR) offers an alternative for high-risk surgical patients who are not candidates for TEER and is deployed via a transapical or transseptal approach. Transcatheter mitral annuloplasty represents another addition to the armamentarium of transcatheter devices.
TEER for the tricuspid valve (T-TEER) has been studied in patients with symptomatic tricuspid regurgitation who are high-risk for cardiac surgery [31]. For patients with large tricuspid annuli, excessive coaptation gaps, complex anatomy, or advanced disease, transcatheter tricuspid valve replacement (TTVR) represents another promising alternative option.
Pibarot et al. [32] reported significantly higher rates of structural valve degeneration in the TAVI cohort of patients with SAPIEN XT valves than in the SAVR cohort; however, this difference was not significant in a propensity-matched analysis of patients with SAPIEN 3 valves. This finding may be attributed to the improved sealing of the SAPIEN 3 transcatheter-implanted valve via an external cuff, which is absent in the SAPIEN XT; however, this design modification may also be associated with increased AV node impingement and higher rates of pacemaker implantation [33]. The PARTNER 3 trial compared TAVR with the SAPIEN 3 valve versus SAVR in low-risk patients over 2 years and found that TAVR was associated with significantly lower rates of all-cause death, stroke, or rehospitalization (11.4% versus 17.4%) [34]. Older SAVR models lacked anti-calcification treatment, which may also have biased earlier studies toward TAVI [35].
More longitudinal studies in low-risk patients treated with modern valve models are needed to assess outcomes. TAVI has the potential to modify the patient population eligible for surgical aortic valve therapy. If a larger population of low-risk patients is eligible for TAVI at a younger age, cardiac surgeons will be expected to manage potential TAVI-related long-term complications surgically. In one meta-analysis, redo SAVR was compared with valve-in-valve TAVI (VIV-TAVI): redo SAVR was associated with a significantly lower risk of cardiovascular death at 1 to 4 years (hazard ratio, 0.35), but with a higher risk of cardiovascular mortality at 30 days (hazard ratio, 2.04) [36]. This may be attributed to postoperative complications associated with redo SAVR and long-term effects of valve thrombosis and patient–prosthesis mismatch in VIV-TAVI. Randomized trials are needed to control for baseline patient characteristics between VIV-TAVI and redo SAVR, as patients selected for redo SAVR in retrospective studies were likely lower-risk surgical candidates.
The EVEREST trial showed a significantly superior combined endpoint of freedom from mortality, surgical reintervention, and grade 3+ or 4+ mitral regurgitation in the surgical cohort compared with the MitraClip cohort at 5 years (64.3% versus 44.2%). However, there was no significant difference in mortality [37]. The MATTERHORN trial demonstrated non-inferiority of transcatheter versus surgical mitral valve intervention in high-risk patients with secondary mitral regurgitation, based on 1-year outcomes of death from any cause, rehospitalization, mitral valve reintervention, stroke, or implantation of a left ventricular assist device (LVAD) [38]. In the United States, the MitraClip continues to be offered to patients deemed high risk for mitral valve surgery, resulting in increased use [39]. Similar to TAVI, further study is needed to assess long-term outcomes, particularly in lower-risk patients. The REPAIR trial will compare outcomes between surgical and transcatheter mitral valve intervention in moderate-risk patients with primary mitral regurgitation [40]. The CLASP IID trial found a significantly higher odds ratio of achieving at most 1+ mitral regurgitation at 6 months in patients with primary mitral regurgitation treated with the PASCAL transcatheter device compared with MitraClip [41].
A systematic review that included several models of TMVR reported no mid-term outcomes of more than mild mitral regurgitation, with a 30-day mortality of 13.6% [42]. TMVR has also been used for valve-in-valve and valve-in-ring replacement, with 30-day mortality rates of 8.1% and 5.0%, respectively, in patients with greater-than-mild mitral regurgitation [43].
The Cardioband system provides a transseptal approach to posterior annuloplasty and achieves less than moderate mitral regurgitation in 65% of patients at 1 year [44]. Multiple devices are currently in development for chordal repair. The RESTORE trial is currently evaluating outcomes with the Harpoon DSD-5 device, which provides off-pump transapical chordal implantation [45]. Another device, the Carillon Mitral Contour System, is anchored in the coronary sinus to provide posterior mitral annuloplasty. In the TITAN II trial, use of the Carillon system reduced moderate mitral regurgitation by 75% and was associated with a 1-year mortality of 23% [46].
In the TRILUMINATE trial, there was no significant difference in 1-year mortality; however, at 30 days, 87% of patients in the T-TEER group had moderate or less tricuspid regurgitation, compared with 4.8% in the medical therapy group [47]. A separate study of 2-year outcomes also showed no significant difference in mortality; however, this study demonstrated a significantly higher rate of moderate or less tricuspid regurgitation (84%) compared with 44% in the medical therapy group [48]. Shimoda et al. [49] compared surgical tricuspid valve repair with T-TEER and found lower in-hospital mortality (2.5% versus 12.5%) and lower pacemaker implantation rates (0% versus 12.7%) with T-TEER. Although there was no significant difference in 2-year mortality, the reintervention hazard ratio was 8.03 for T-TEER.
Similar to TEER, TTVR has been studied in patients with severe, symptomatic tricuspid regurgitation who are at high surgical risk. The TRISCEND II trial compared the EVOQUE TTVR plus optimal medical therapy with optimal medical therapy alone. At 1 year, 99.1% of patients in the TTVR group had moderate or less tricuspid regurgitation, compared with 16.1% in the medical-therapy alone group. TTVR was associated with higher rates of bleeding and permanent pacemaker placement. However, Kaplan–Meier 1-year mortality was lower with TTVR (12.6%) than with medical therapy alone (15.2%) [50].
Transcatheter therapies were initially introduced for patients considered high-risk surgical candidates, but have the potential to be applied to an expanded population. The use of these devices requires that patients meet anatomical and physiologic criteria, while long-term outcome data remain limited in lower-risk and younger patients, who may have concerns about potential complications arising decades later. Transcatheter therapy avoids the need for cardiopulmonary bypass and sternotomy, thereby reducing hospital length of stay and postoperative complications.
Transcatheter therapies are best offered through shared decision-making between patients and the multidisciplinary heart team. These procedures may be performed by either interventional cardiologists or surgeons, with each specialty providing valuable insight regarding the optimal procedural approach for a specific patient. These discussions should also include long-term planning for potential redo transcatheter or surgical procedures following transcatheter therapy, as well as concomitant procedures. Surgeons need to be on standby in case of a failure during device deployment.
The surgical treatment of atrial fibrillation continues to evolve, with innovations in ablation technologies, particularly robotic systems and hybrid thoracoscopic approaches. The evolution of procedures for treating atrial fibrillation is illustrated in Fig. 2.
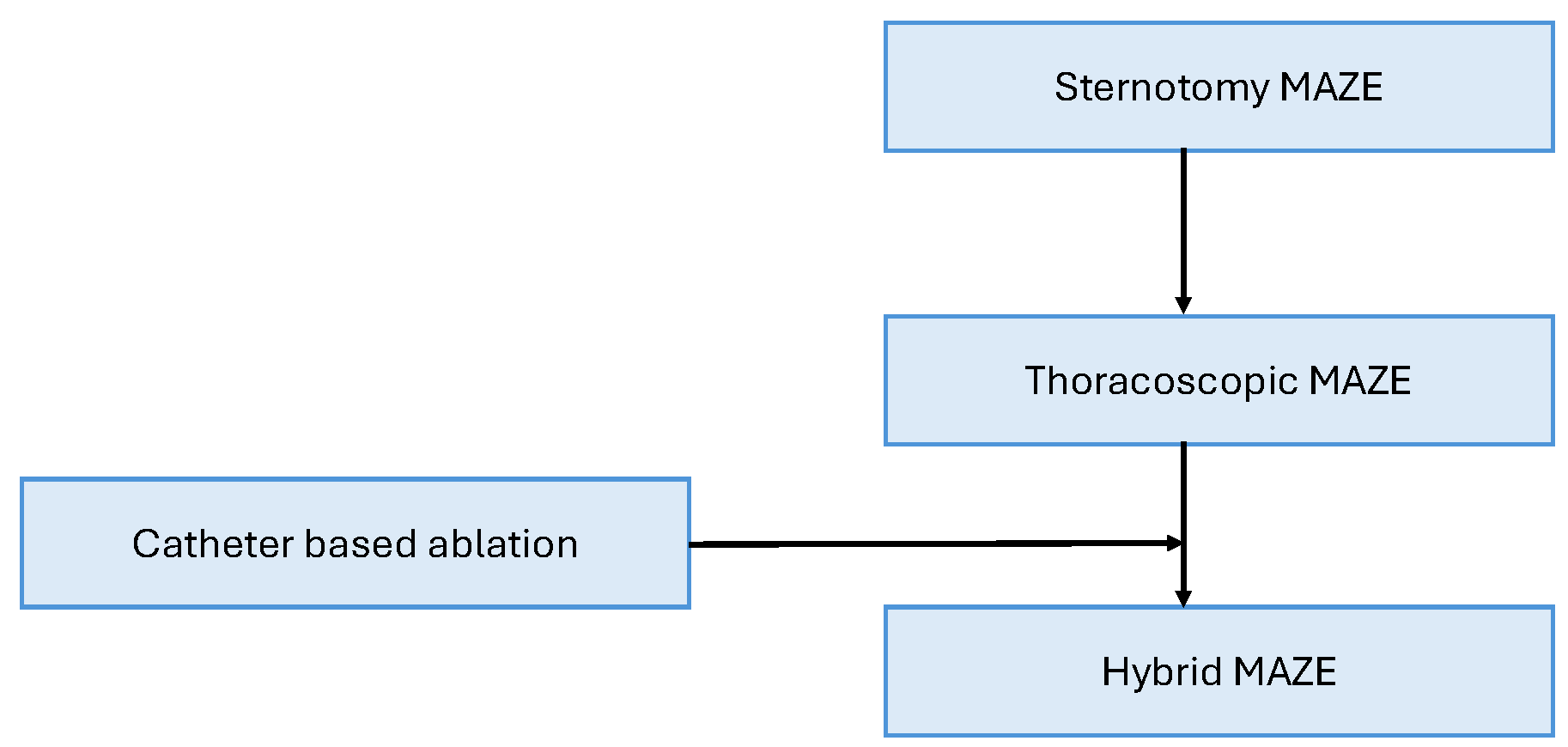 Fig. 2.
Fig. 2.
The evolution of atrial ablation approaches. The hybrid maze enables the combination of endocardial and epicardial ablative approaches in a less invasive modality compared to sternotomy.
Open sternotomy atrial ablation, known as the MAZE procedure, has long been considered the gold standard therapy for persistent atrial fibrillation. However, owing to the invasive nature of open sternotomy atrial ablation, patients who are not undergoing other cardiac surgical procedures commonly elect for catheter-based endocardial ablation. Recent innovations have included complete thoracoscopic ablation and hybrid ablation combining the thoracoscopic and catheter-based approaches.
Catheter ablation is typically not durable, with a reported success rate as low as 28% at 5 years, compared with 97% for surgery in patients with persistent atrial fibrillation [51]. The hybrid approach involves creating thoracoscopic epicardial lesions followed by catheter-based endocardial lesions. This strategy has demonstrated superior 16-month freedom from recurrence of persistent atrial fibrillation compared with a catheter-based approach without antiarrhythmic drugs (86.7% versus 53.3%) [52]. Performing complete thoracoscopic MAZE lesions was reported to be non-inferior to open sternotomy, with shorter ICU length of stay, lower operative mortality, and shorter hospital stay [53]. Almousa et al. [54] reported that complete biatrial lesion creation via a robotic approach achieved freedom from recurrence of persistent atrial fibrillation greater than 90% at 1 year off antiarrhythmic drugs; however, longer follow-up is needed.
With further development and practice of minimally invasive lesion-based approaches for atrial fibrillation, patients may be more amenable to surgical approaches, allowing for more sustained freedom from recurrent atrial fibrillation without antiarrhythmic medications. However, long-term evidence for minimally invasive surgical approaches remains limited, which prevents their widespread adoption. Additionally, patients may also be hesitant to pursue surgical ablation while catheter-based ablation is available. Nevertheless, the hybrid approach may enable more effective treatment of atrial fibrillation in patients who would otherwise choose catheter-only based ablation. Although hybrid approaches and total thoracoscopic MAZE may approach the short-term outcomes of traditional sternotomy MAZE, long-term analysis is necessary to evaluate non-inferiority.
Hybrid thoracoscopic and catheter-based approaches, as well as complete thoracoscopic approaches, have a substantial learning curve and are therefore limited to high-volume centers with adequate infrastructure and surgical experience. Successful implementation of the hybrid approach requires a heart team to manage atrial fibrillation, with collaboration among cardiac electrophysiologists, surgeons, and cardiologists for therapeutic planning and appropriate selection of surgical candidates.
The surgical management of heart failure has undergone immense innovation over the past 20 years. Left ventricular assist devices (LVADs) have undergone significant improvements in durability and function. LVADs have evolved through multiple generations and continue to offer potential for device optimization. Moreover, the increasing use of novel temporary mechanical circulatory support (tMCS) devices offers patients hope for improved survival and a transition to long-term mechanical circulatory support (LT-MCS) therapies.
The Impella has been used as a temporary ventricular assist device. This microaxial pump is placed in the left ventricle, thereby improving cardiac output, increasing coronary perfusion, and decreasing ventricular load. Use of the Impella has increased in the United States, as evidenced by the rising application of this device among patients with Medicare being managed for acute myocardial infarction or cardiogenic shock [55]. The Impella CP can deliver up to 4 L/min of flow and, similar to the Impella 2.5, can be inserted percutaneously. The Impella 5.5 can provide up to 5.0 L/min of flow and requires surgical insertion via the femoral or axillary arteries. The Impella RP Flex provides temporary mechanical circulatory support for right ventricular failure refractory to medical management and may be used as a bridge to recovery or to additional surgical procedures.
The first generation of LVADs provided pulsatile flow and included the HeartMate Extended Vented Electric and Novacor N100 [56]. The HeartMate II and Jarvik 2000 LVADs comprised the second generation of devices providing continuous flow via axial-flow pumps with fewer mechanical components. These devices are smaller and less susceptible to mechanical wear; however, continuous flow is associated with a higher risk of bleeding, attributed to degradation of von Willebrand factor (vWF) multimers. The HeartMate II can be implanted via a thoracoabdominal approach without a percutaneous ventilator, and the Jarvik 2000 axial-flow rotor is implanted into the left ventricle via a left lateral thoracotomy. Third-generation LVADs provide centrifugal flow and use magnetically levitated rotating components (MAGLEV technology) to minimize wear, thrombosis, and hemolysis [56]. The additional sensory and suspensory components require more energy [57]. The HeartMate III incorporates centrifugal flow, while the HeartWare device additionally includes hydrodynamic support, allowing blood flow to provide suspension between components [58].
In a propensity-adjusted analysis of 2156 patients from the Premier Healthcare database, the Impella reduced the risk of myocardial infarction by 71% and cardiogenic shock by 46% when used pre-emptively in patients undergoing high-risk PCI. The reduction in cardiogenic shock was associated most strongly with mortality [59]. Iannaccone et al. [60] reported improved survival among patients receiving the Impella CP for cardiogenic shock; however, the IMPRESS trial showed no significant difference in 30-day or 6-month mortality between Impella CP and IABP [61]. The DANGER trial compared routine Impella CP insertion for cardiogenic shock secondary to myocardial infarction to the standard of care and found significantly lower 180-day mortality with Impella CP (45.8% versus 58.5%) [62].
Outcomes following Impella placement vary significantly, reflecting the diverse applications of this device, including pre-emptive insertion during cardiac procedures and emergent restoration of flow during circulatory collapse. Maigrot et al. [63] reported that patients who received an Impella 5.5 in earlier stages of cardiogenic shock were more likely to be successfully transitioned to permanent circulatory support or heart transplantation than patients with impending circulatory collapse. Further study is warranted regarding the use of Impella 5.5 in high-risk patients undergoing cardiac procedures, particularly in anticipation of decompensation to cardiogenic shock. Eisenga et al. [64] reported in a cohort of 10 patients undergoing high-risk cardiac surgery (median EF 25%) that perioperative use of the Impella 5.5 was associated with a 90% hospital discharge rate and an 80% 30-day survival. Benke et al. [65] reported a 30-day survival of nearly 93% in 14 patients who received Impella 5.0/5.5 support before high-risk CABG.
The RECOVER RIGHT study was a prospective study of 30 patients receiving the Impella RP Flex, 18 of whom developed right ventricular failure after LVAD implantation [66]. Hemodynamic benefits included a statistically significant improvement in cardiac index and a decrease in central venous pressure, with a 30-day survival of 73.3%. In a retrospective study of 22 patients, 15 of whom received left ventricular support, overall survival was 68%, accompanied by a reduction in mean lactate levels post-insertion [67]. Larger clinical studies are needed to develop guidelines that establish criteria and indications for the use of the Impella RP Flex.
Slaughter et al. [68] compared outcomes in patients receiving the HeartMate II versus those receiving the HeartMate I and found significantly higher 2-year survival free from disabling stroke or reoperation to repair or replace the LVAD with the HeartMate II (46% versus 11%). The 2-year mortality rate was also significantly lower with the HeartMate II (33% versus 41%). The MOMENTUM 3 study is a randomized controlled trial comparing outcomes in patients receiving either the HeartMate III or HeartMate II LVAD [69]. Per protocol analysis, the HeartMate III was associated with significantly lower rates of pump thrombosis (1.4% versus 13.9%), stroke (9.9% versus 19.4%), and bleeding (43.7% versus 55.0%) [70]. In a retrospective observational study, no significant differences in mortality or major adverse cardiovascular events were observed between the HeartMate III and HeartWare; however, the HeartWare was associated with a significantly higher malfunction rate of 20%.
tMCS provides patients with a bridge to LT-MCS, which can be used either as destination therapy or a bridge to transplant. Evidence strongly suggests improved survival with the Impella CP in cardiogenic shock, and recently established guidelines for Impella insertion will enable more standardized implementation. A small but significant percentage of patients are candidates for weaning from mechanical circulatory support. In patients with ventricular failure refractory to intensive medical management, mechanical circulatory support devices provide an additional measure to prolong survival and allow for either heart transplant or recovery of cardiac function.
Guidelines for LT-MCS implantation are available but not definitive, and require consideration of anticipated recovery, comorbidities, and the social context of patients. Furthermore, cardiologists and cardiac surgeons must be familiar with the management and surgical implantation of multiple devices, which entails a substantial learning curve in a continually evolving landscape of device therapies. Current efforts to improve LVAD therapy include reducing device size and the number of components, particularly the subcutaneous lines, which are prone to infection. A miniature ventricular assist device has been studied in an ovine preclinical model and has the potential benefit of applicability in smaller patients. Moreover, this device provides a comparable flow rate of up to 7 L/min with acceptable hemocompatibility and biocompatibility [71]. Future improvements may include implementing transcutaneous energy to avoid the need for a subcutaneous line. Although the device has been previously tested, reports of device failure and electromagnetic interference with transcutaneous energy transfer indicate that further improvement is necessary [56].
Heart failure remains a frontier for continued progress in cardiac surgery. Ongoing improvements of the total artificial heart (TAH) and innovations in xenotransplantation and partial heart transplantation have expanded the armamentarium for treating heart failure.
SynCardia/CardioWest were the first devices to be approved for bridge-to-transplantation in patients with biventricular failure, using diaphragm-pneumatically driven pumps [72]. The Carmat TAH, approved in 2020, uses bioprosthetic material and biological valves that come into contact with blood to reduce the risk of thrombosis and is currently being evaluated in human trials. The ReinHeart device is being developed with a transcutaneous battery-charging system, thereby avoiding the potential for power-line infection. One drawback of these devices is the associated large size, which restricts use in patients with small thoracic cavities, particularly women. To address this, the BiVACOR is being developed with a displaceable, rotary magnetic propulsion system that enables implantation of a smaller device in smaller patients [72]. Similarly, the Cleveland Clinic Continuous-Flow TAH is a valveless, pulsatile model under development that aims to increase applicability for smaller patients while avoiding the need for a percutaneous pneumatic cable through the use of a rotary propulsion system [73].
Although robotics has not been as widely adopted in the surgical management of heart failure as in other cardiac procedures, reports have illustrated its potential. Khalpey et al. [74] described a robotic approach to LVAD implantation via bilateral mini-thoracotomy, which was associated with a reduced length of stay. Khaliel et al. [75] describe the first robotic orthotopic heart transplant in a 16-year-old boy, and in the United States, a Baylor robotic heart transplant was performed successfully in an adult [76].
Xenotransplantation remains predominantly in the preclinical stage. Reports of genetically modified porcine hearts implanted into human recipients highlight the feasibility of xenotransplantation; however, the rejection of donor specimens despite porcine donor genetic modification and aggressive immunosuppression shows that further investigation into immunogenic targets is necessary [77].
A partial heart transplant was first performed in 2022 in a 17-day-old patient with truncus arteriosus. Subsequent procedures included partial heart transplants involving the mitral valve and right ventricular-to-pulmonary artery conduit [78].
Currently, Syncardia is the only FDA-approved TAH. In a 20-year retrospective study of 196 patients in Germany, Razumov et al. [79] found 1-month, 6-month, and 1-year mortality rates of 28%, 56%, and 61%, respectively. Overall, 35.2% of patients survived to transplantation, with a median post-transplant survival time of 5.8 years. TAHs are typically indicated for patients with severe biventricular failure or for those with contraindications to bilateral ventricular assist device implantation. In a retrospective study, 90-day post-transplant mortality was significantly higher among patients with TAH compared with those with LVAD or undergoing de novo transplants (12.2% versus 6.4% versus 5.4%, respectively); however, patients with TAH before transplant had higher rates of renal dysfunction, dialysis, and functional limitation [80]. Ferrall et al. [81] found similar post-transplant survival between State as biventricular assist device (BiVAD) and TAH recipients at high-volume centers. In a prospective single-institution study of 100 patients, TAH support was associated with a 1-year mortality of 34%, a transplantation rate of 46%, and a 95.1% survival at 6 months post-transplant [82].
The TAH is a practical alternative to BiVAD because this option enables synchronized operation of the associated components and avoids the need for reoperation to place a right-sided ventricular assist device (VAD) when indicated. However, device availability and experience with TAH remain limited, and this option applies only to patients with thoracic cavities large enough to accommodate a TAH. Xenotransplantation requires continued research into immunogenic targets and immunosuppression regimens before successful long-term application in humans. Benefits of partial heart transplant include the availability of donor hearts that are not otherwise suitable for orthotopic heart transplant and the potential for reduced doses of immunosuppressive therapy; however, further clinical application and research are needed to evaluate outcomes and optimize immunosuppression. Nevertheless, partial heart transplants have the potential for successful outcomes, as cases have shown the growth capacity of transplanted tissue in pediatric recipients [78].
Ferrall et al. [81] reported a higher incidence of multiple organ dysfunction and dialysis in patients with TAH, as well as a higher post-transplant survival in patients with previous BiVAD compared with those with TAH, even when comparing single-organ transplant recipients. These findings suggest that dialysis is not the only factor affecting post-transplant outcomes and that TAH may be better suited for patients with multiple organ dysfunction [81]. The choice between BiVAD and TAH depends on center volume and device availability, in addition to the clinical history unique to each patient. Further development is needed to ensure long-term device functionality and applicability to a wider range of patients, particularly those with smaller thoracic cavities. Partial heart transplantation has the potential to increase the availability of donor tissue, as recipients can have their own tissue donated, and donor hearts can be used to supply tissue to multiple recipients. Ethical considerations include whether orthotopic transplants should take precedence over a partial heart transplant for a specific patient [78].
Impending advances in cardiac surgery are vast and include the application of artificial intelligence (AI), three-dimensional (3D) printing, and individualized cardiac surgery. Three-dimensional printing has predominantly been used to create anatomical models for preoperative planning, which is particularly useful in cases of complex anatomy. Other applications include resident and student education in cardiac surgery [83]. AI has been used for preoperative risk stratification and has the potential to be applied in robotic surgery through intraoperative monitoring and autonomous assistive maneuvers [84]. Individualized cardiac surgery enables preoperative planning and implantable device modeling tailored to the unique anatomy of each patient [85]. Currently, individualized cardiac surgical planning allows the selection of a prosthesis model that best approximates the anatomy of each patient. Individualized surgery, 3D printing, and AI can serve complementary functions. For example, AI can facilitate preoperative planning and anatomical modeling, enabling 3D printing of an implantable construct optimized for an individual patient. Further research and development are required before 3D bioprinting becomes commonplace. AI will inevitably see increased use in cardiac surgery; however, surgeons should ensure that AI is used as a tool to assist in operative planning and procedures rather than as a replacement for human expertise. Although there is concern that AI could eliminate the need for surgical assistants and limit trainee participation in the operating room, AI and 3D modeling can also be useful for surgical training through virtual reality models. This may help overcome the learning curve associated with innovative robotic approaches and enable cardiac surgical trainees to enter the workforce with exposure to both traditional and novel surgical techniques.
Cardiac surgery has remained at the center of innovation and development in minimally invasive approaches. Robotic platforms have been increasingly adopted for minimally invasive thoracoscopic approaches to cardiac revascularization, valve procedures, and ablative therapies, with a few but successful attempts in transplantation.
Conventional approaches of sternotomy remain the predominant modality of performing cardiac surgery. The advent of catheter-based therapies for revascularization, valve replacement, and ablation, commonly performed by interventional cardiologists, narrowed the population of patients selected for cardiac surgery. However, robotic-assisted minimally invasive cardiac surgery can potentially offer the same benefits of catheter-based therapy, such as decreased post-procedural pain and shorter hospital stays, while matching the efficacy of open sternotomy approaches. With further application and experience with the robot, cardiac surgeons may be able to attain the shorter bypass and cross-clamp times of sternotomy while still providing optimal surgical therapy.
Further research on the outcomes and potential complications of robotic-assisted cardiac surgery is necessary before this option can be accepted as a standard therapy. Nevertheless, robotic cardiac surgery should be approached with curiosity and inquiry rather than skepticism, as this approach may expand the population of patients who can benefit from the expertise of cardiac surgeons and may improve clinical outcomes.
Cardiac surgeons have traditionally been innovators and have resisted accepting the status quo. As innovations are evaluated, an unbiased assessment of emerging technologies is essential to ensure patient safety and to confirm that the novelty can reliably produce the desired results without introducing new shortcomings. Industry stands to benefit most from the adoption of novel technologies; however, a new process must be validated with the utmost rigor to ensure that therapy is validated without compromising the safety of patients whom this technology is intended to treat. The pressures exerted by industry and the ambitions of the well-intentioned physicians who wish to advance science and distinguish themselves can sometimes obscure what is most important in medicine: restoring our patients to health. We must pursue advances in medicine—yes—but never at the expense of the safety and well-being of our patients.
CN, MN, and SS contributed to the literature review and drafting of the manuscript. MN and SS contributed to the critical revision of the manuscript for important intellectual content. All authors participated in the design of the study. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare-affiliated entity.
The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities. The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.