




 , Morgan Harloff 2, Alexandros N. Karavas 2,*
, Morgan Harloff 2, Alexandros N. Karavas 2,*
1 Department of Surgery, Boston Medical Center, Boston University Chobanian & Avedisian School of Medicine, Boston, MA 02118, USA
2 Division of Cardiac Surgery, Department of Surgery, Boston Medical Center, Boston University Chobanian & Avedisian School of Medicine, Boston, MA 02118, USA
Abstract
Lipomatous hypertrophy of the interatrial septum is rare, and extension to surrounding structures is extremely uncommon, yet may result in obstructive symptoms requiring surgical resection.
This case report describes a 56-year-old male who had been undergoing an outpatient workup for lightheadedness, palpitations, and chest pain. Computed tomography revealed a large mass extending from the superior vena cava to the atrial septum, resulting in compression of the superior vena cava. Magnetic resonance imaging suggested lipomatous characteristics. Subsequently, the patient was referred for cardiac surgery and underwent an uncomplicated resection of the mass and reconstruction of the superior vena cava, with ensuing resolution of the symptoms.
Lipomatous hypertrophy of the interatrial septum can rarely expand into the superior vena cava, causing obstructive symptoms. Symptomatic relief may be achieved via resection of the entire mass, which can be performed without violating the atrial septum and atrial wall.
Keywords
- cardiac surgery
- lipomatous hypertrophy of the interatrial septum
- benign cardiac tumors
Cardiac tumors are an uncommon pathology, with a prevalence of less than 0.5% [1]. Lipomatous hypertrophy of the interatrial septum (LASH) is a benign cardiac tumor and a rare entity with incidence largely limited to a few hundred case reports over several decades, with very few requiring surgery. LASH is characterized by an unencapsulated fatty infiltration of the interatrial septum that has a thickness of at least two centimeters [2, 3]. It is distinct from lipomas, which are characterized by the presence of a capsule. Characteristically, LASH spares the fossa ovalis, which accounts for the diagnostic dumbbell shape on imaging. LASH has the tendency to extend towards the superior vena cava (SVC) and roof of the atria rather than the inferior vena cava [2, 3, 4]. Extension beyond the interatrial septum is exceedingly rare, with only a few cases reported in the literature, and this may result in compressive symptoms or arrhythmias [2, 5, 6].
A 56-year-old male with no cardiac history and a medical history notable only for a 48-pack-year smoking history underwent a lung screening computed tomography (CT) scan and was found to have a lipomatous mass extrinsically compressing the SVC and extending into the interatrial septum. During further evaluation, he reported a history of palpitations, lightheadedness, and chest pain, exacerbated with activity, particularly bending down. These symptoms had been present for over a year at the time of his evaluation but had not been previously attributed to any specific cause. During the course of his outpatient work-up, he suffered a syncopal episode resulting in a motor vehicle collision. A workup was negative for other causes of syncope. His physical exam during this time was notable for occasional extra beats but was otherwise unremarkable with no jugular venous distention and no facial plethora.
At this point, he was referred for outpatient evaluation by Cardiac Surgery. Additional workup was completed, consisting of a computed tomography angiogram (CTA) and a transesophageal echocardiogram (TEE). CTA revealed the known lipomatous mass at the level of the right atrium and interatrial septum. It measured approximately 5 cm by 4 cm and was associated with severe stenosis of the SVC at the level of the cavoatrial junction (Fig. 1). Coronary protocol CTA was suggestive of coronary artery disease, which was subsequently excluded by left heart catheterization. Notably, his cardiac catheterization revealed a prominent vessel feeding into the mass at the level of the cavoatrial junction. TEE confirmed the mass as described on CTA, with otherwise unremarkable findings; normal biventricular and valve function, no wall motion abnormalities and no intracardiac shunts. Magnetic resonance imaging (MRI) suggested lipomatous characteristics of the mass.
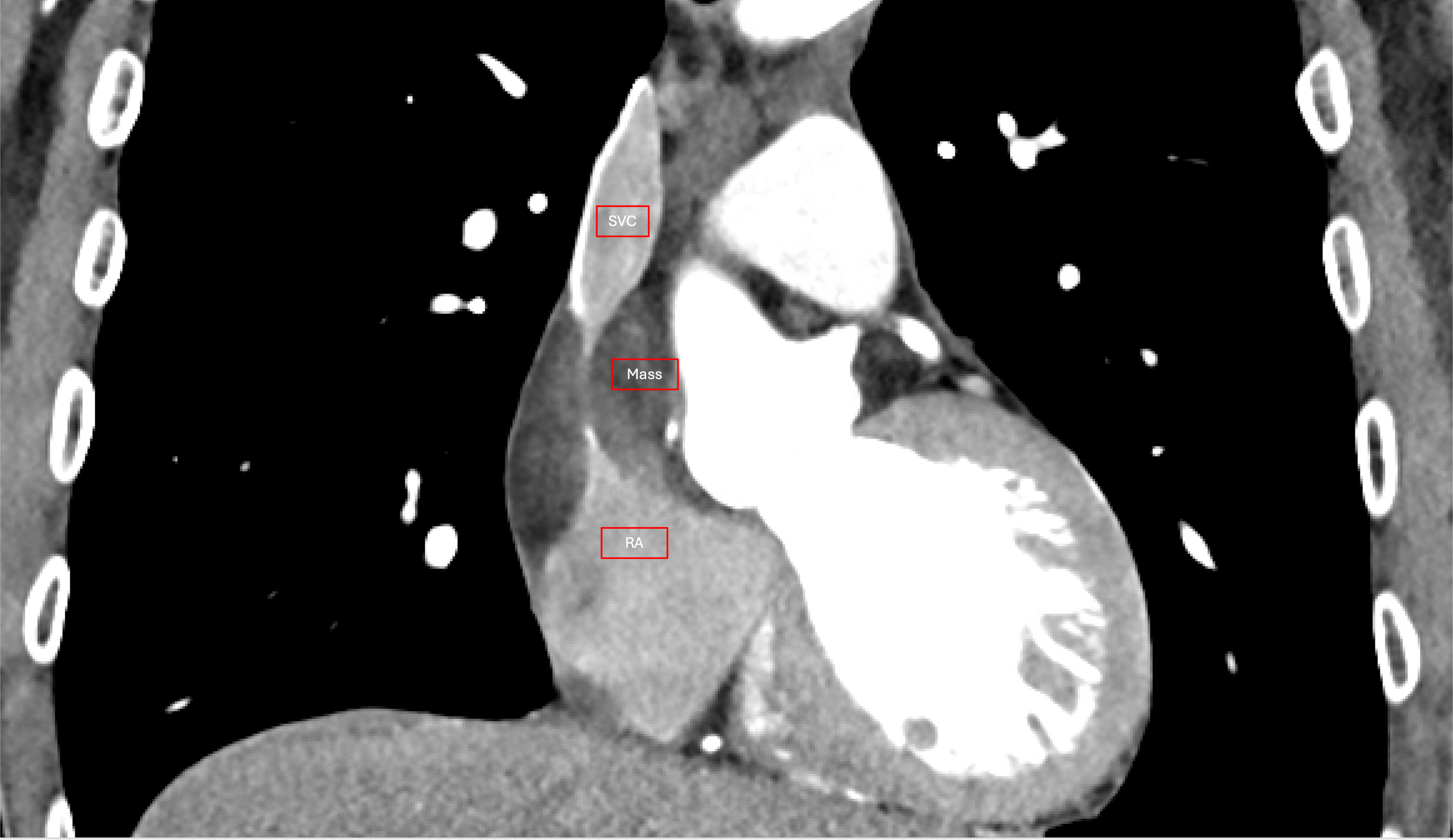 Fig. 1.
Fig. 1.
Computed tomography angiogram demonstrating the mass compressing the cavoatrial junction. SVC, superior vena cava; RA, right atrium.
Given the patient’s non-specific symptoms and recent syncopal episode, all without other clear cause, the mass was presumed to be symptomatic. After a discussion of risks and benefits, the patient elected for operative management for symptomatic relief. Through a median sternotomy approach, the resection was initiated at the SVC level. For the interatrial portion, cardiopulmonary bypass was instituted via high bicaval and aortic cannulation. The heart was arrested using del Nido cardioplegia via an antegrade approach. The mass was mobilized from the SVC, and the dissection extended into the Sondergaards groove to resect the interatrial portion (Fig. 2). A 2 cm by 3 cm atrial septal defect was identified at the level of the SVC. Normal pulmonary venous drainage was confirmed and the atrial septal defect was closed using a bovine pericardial patch. The mass was extending into the dome of the left atrium and resection was accomplished by transecting the SVC one cm above the sinus node. To ensure tensionless reconstruction of the SVC-right atrial junction, the right atrial appendage was mobilized, and a lateral bovine pericardial patch was utilized (Fig. 3).
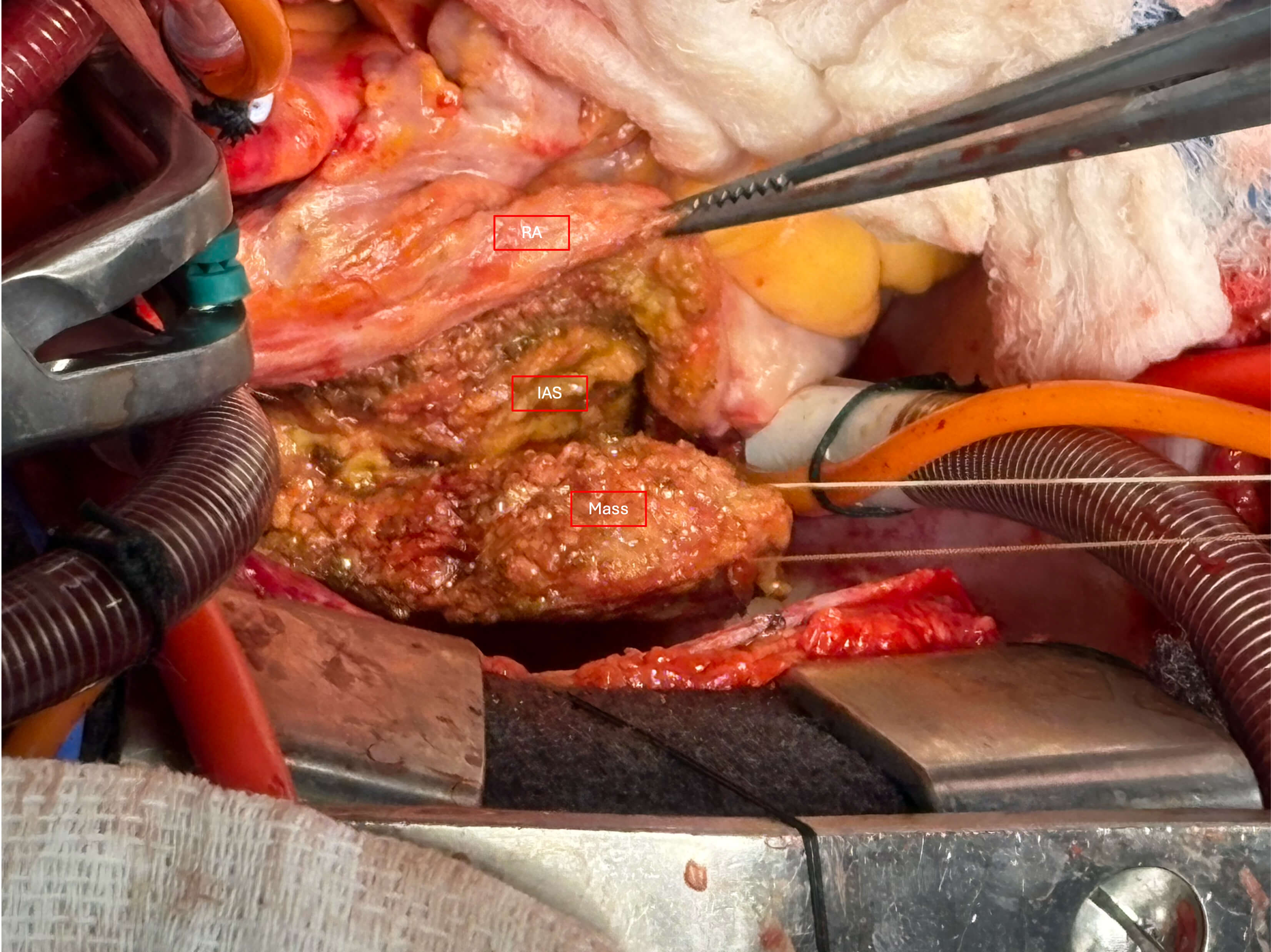 Fig. 2.
Fig. 2.
Intraoperative picture depicting resection of the mass within the Sondergaard’s groove (surgeon’s view from left). RA, right atrium; IAS, interatrial septum.
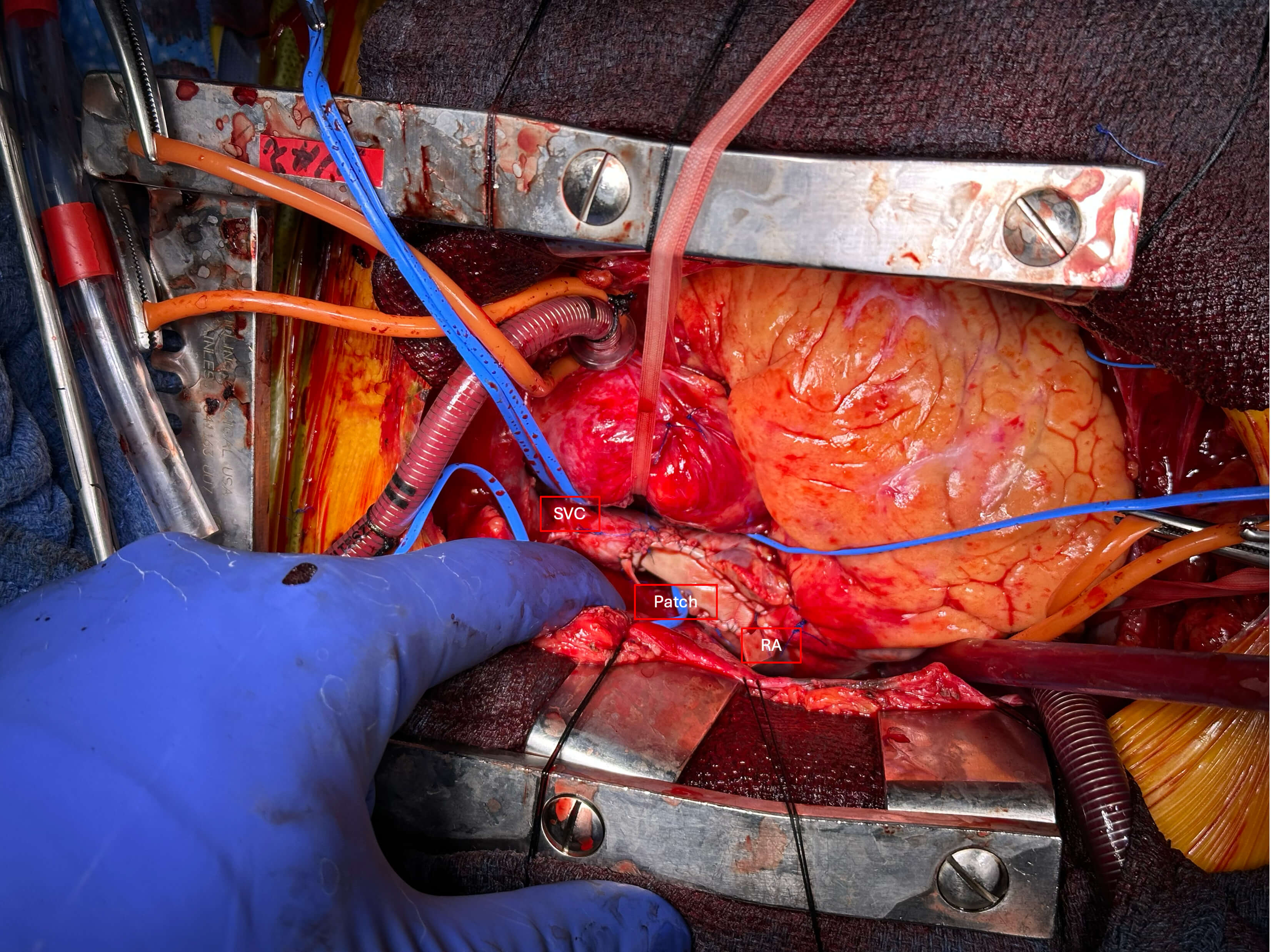 Fig. 3.
Fig. 3.
Intraoperative picture of cavoatrial junction repair after resection of the mass (surgeon’s view from left). SVC, superior vena cava; RA, right atrium; Patch, Bovine pericardial patch.
The patient’s postoperative course was notable for initial junctional rhythm that recovered spontaneously, allowing the patient to be discharged home on the fifth postoperative day. CT prior to discharge revealed resolution of SVC obstruction and no residual mass, but some hematoma within the interatrial septum. Pathology demonstrated an unencapsulated mass comprised of mature and immature adipose tissue infiltrating hypertrophied myocytes and mild interstitial fibrosis. Fluorescence in situ Hybridization (FISH) was negative for MDM2 gene amplification. At outpatient follow up, the patient reported that his symptoms had resolved.
Consistent with previous reports, in this case, LASH was incidentally found on imaging obtained for other reasons [7]. Imaging characteristics, including a dumbbell-shaped, homogenous mass without contrast enhancement, are typically consistent and unique enough to be sufficient for diagnosis without tissue sampling [8]. Overall, the condition most commonly affects older female patients, those of white race, and those with obesity [8]. While most cases are asymptomatic, in retrospect, this patient’s vague symptoms of palpitations, chest pain and dizziness, as well as a syncopal episode, are likely attributable to SVC obstruction associated with the mass, particularly as these symptoms resolved after resection. The palpitations he experienced may have been the result of atrial arrhythmias, due to disrupted atrial conduction systems secondary to stretching or direct infiltration by the mass [8].
While cardiac masses are overall rare, and clinical symptoms are often attributable to other cardiac causes, a broad differential diagnosis remains the core tenet of management. Our patient displayed a vague symptom constellation associated with LASH, with the rare finding of associated SVC compression. With broader use of cardiac and chest imaging, diagnosis of such symptomatic lesions is more likely to occur during the patient’s lifetime than postmortem as early reports had suggested [9]. Failure to identify such rare cases may result in poor outcomes or continued distressing symptoms for the patient.
Surgical resection has been described in the management of symptomatic patients. The surgical approach is not clear and reports have equally described a limited resection as well as complete macroscopic resection, while still other studies have described an atrial approach as opposed to an interatrial approach [2, 10, 11, 12]. Breuer et al. [2] reported partial resection of the mass to alleviate SVC obstruction, without extending the resection into the interatrial septum. While such masses are considered benign and unlikely to invade, they can be symptomatic. Thus, this management is a reasonable approach in patients in whom surgical risk is elevated and may not tolerate well a longer cardiopulmonary bypass run [2]. Oxorn and colleagues [12] reported an aggressive resection approach, similar to ours, which resulted in removal of the majority of the mass. They avoided resection of the portion of the mass that was extending towards the aorta [12]. The approach in our case consisted of complete resection of the mass using an interatrial approach. We encountered an atrial septal defect near the SVC, not seen on preoperative imaging studies, which was repaired with a bovine pericardial patch. Typically, LASH has been described to occur within the infoldings of the atrial walls rather than the true septal tissue, which allows the surgeon to avoid direct access through the atrium [3]. Therefore, we believe that the interatrial approach allows for an easier way to follow and resect the mass, especially as it extends beyond the cardiac structures into the SVC and the dome of the left atrium. This approach requires a longer operative time, and was possible in this case given the patient’s overall excellent functional status. In higher risk patients who may not tolerate a long operation and cardiopulmonary bypass, interventional approaches such as SVC stenting may be considered as a palliative measure.
The patient developed a postoperative junctional rhythm that recovered spontaneously after a few days. This has been previously described in such cases [12]. Postoperative dysrhythmias may be attributed to dissection near the sinus node or disruptions to the vascular supply of the mass. In our case, a large vessel supplying the mass was coursing near the sinus node. The distal portion of this vessel had to be sacrificed along with the mass, which may have accounted for the patient’s temporary sinus node dysfunction.
With increased frequency of chest imaging, identification of LASH with extension into the surrounding structures is likely to rise and may increase diagnosis in the face of non-specific symptoms. Surgical resection may be accomplished via an interatrial approach without having to enter the cardiac chambers, however, SVC mobilization or complete resection may be required.
LASH, lipomatous hypertrophy of the interatrial septum; SVC, superior vena cava; CT, computed tomography; CTA, computed tomography angiography; TEE, transesophageal echocardiogram; MRI, magnetic resonance imaging.
SS: Acquisition of data, drafting of original manuscript, editorial changes and final approval. MH: Interpretation of the data, Critical editing of manuscript, editorial changes and final approval. AK: Conceptualization, acquisition of data, critical editing of the manuscript, editorial changes and final approval. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was carried out in accordance with the guidelines of the Declaration of Helsinki. Patient provided informed written consent for this publication. The Institutional Review Board of Boston Medical Center - Boston University waived full review in the presence of informed written patient consent, as per institutional guidelines.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest. Alexandros N. Karavas is serving as one of the Editorial Board members and Guest Editor of this journal. We declare that Alexandros N. Karavas had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Guowei Tu and Gregory D. Trachiotis.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/HSF52748.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.