







 , François-Adrien Duvauchelle 2, Amale Ghandour 3,4, Oliver Lee 5, Dominique Shum-Tim 6,*
, François-Adrien Duvauchelle 2, Amale Ghandour 3,4, Oliver Lee 5, Dominique Shum-Tim 6,*
1 Faculty of Medicine, University of Montreal, Montreal, QC H3T 1J4, Canada
2 Division of Cardiology, Montreal University Hospital Centre, Montreal, QC H2X 0C1, Canada
3 Division of Cardiac Surgery, McGill University Health Centre, Montreal, QC H4A 3J1, Canada
4 Research Institute of the McGill University Health Centre, Montreal, QC H4A 3J1, Canada
5 UCL Medical School, University College London, WC1E 6BT London, UK
6 Department of Surgery, Division of Cardiac Surgery, McGill University Health Centre (MUHC), Montreal, QC H4A 3J1, Canada
Abstract
Postoperative atrial fibrillation (POAF) is the most common complication following cardiac surgery. While often considered a transient and expected complication, recent evidence suggests that POAF is associated with an increased risk of recurrence, thromboembolic events, and long-term morbidity. Moreover, the management of POAF remains debated, particularly regarding the choice between rate- and rhythm-control strategies and the use of anticoagulation. A narrative literature review was conducted using the PubMed, the Cochrane Library, and Google Scholar databases. Studies that focused on adult patients who developed POAF after coronary artery bypass grafting or valve surgery and addressed at least one of the following were included: recurrence patterns, treatment strategies (rate vs. rhythm control), stroke risk stratification, or anticoagulation. Studies focusing on nonsurgical atrial fibrillation (AF), pediatric populations, or animal models were excluded. A total of 45 articles were included for the final analysis. A total of 8 studies evaluated the recurrence of POAF after discharge. Across these studies, recurrence ranged between 30% and 60%, with many episodes occurring within the first month and remaining asymptomatic. Continuous monitoring tools, such as implantable loop recorders and handheld electriocardiogram (ECGs), showed a significantly higher detection rate than usual care. Seven studies compared rate- and rhythm-control strategies; in most patients, sinus rhythm was maintained regardless of the approach. Rate control, typically with beta-blockers, was favored as a safer first-line option. However, rhythm control, particularly through catheter ablation, showed improved outcomes in patients with heart failure or persistent symptoms. Nine studies examined stroke risk. The risk score for stroke in atrial fibrillation (CHA2DS2-VASc) score, although widely used in the general atrial fibrillation population, was validated primarily in the nonsurgical and transient AF population and may underestimate short-term thromboembolic risk in the postoperative setting. Some studies reported that stroke risk increased significantly once the CHA2DS2-VASc score reached ≥4, highlighting the potential for early postoperative thromboembolism. Several articles explored whether tools designed for subclinical AF, such as the risk stratification tools for subclinical atrial fibrillation (SCAF) score, could better stratify POAF risk. Notably, stroke risk increased significantly when episodes of atrial fibrillation exceeded 48 hours, suggesting that both duration and timing post-surgery are important considerations. Nine studies addressed anticoagulation. Oral anticoagulants, particularly apixaban, were associated with modest reductions in thromboembolic events but also with increased bleeding complications. Meanwhile, despite eligibility, fewer than 30% of patients received anticoagulation upon discharge. POAF is a common but underrecognized complication of cardiac surgery that carries a significant risk. Individualized management strategies guided by early rhythm monitoring and refined risk assessment tools are essential for optimizing outcomes.
Graphical Abstract

Keywords
- postoperative atrial fibrillation
- rate control
- rhythm control
- anticoagulation
- stroke risk
- POAF recurrence
- atrial fibrillation management
Postoperative atrial fibrillation (POAF) is a common complication of cardiac surgery, with reported incidence rates ranging from 25% to over 40% [1]. While frequently considered a benign and expected postoperative event, mounting evidence suggests that POAF can lead to serious short- and long-term consequences. It is associated with an increased risk of ischemic stroke, prolonged hospitalization, heart failure exacerbation, and long-term mortality [2, 3].
Despite its high incidence and well-documented risks, the management of POAF remains a clinical gray zone. Multiple treatment strategies exist, ranging from rate control to aggressive heart rhythm restoration. The use of anticoagulation remains debated, with significant variability in clinical practice. Current guidelines from leading cardiovascular societies offer divergent recommendations, largely based on data derived from patients with non-surgical atrial fibrillation [4, 5]. As a result, clinical practice varies widely, and therapeutic decisions are often based on institutional preferences rather than robust, targeted evidence.
Additionally, increasing attention has been directed toward the recurrence of POAF and its association with thromboembolic events. Although most patients are discharged from the hospital in sinus rhythm, continuous postoperative heart monitoring has revealed that atrial fibrillation frequently recurs in the weeks following surgery, often without any clinical symptoms [3, 6]. These episodes present a challenge for stroke risk stratification and have raised ongoing uncertainty regarding the need for anticoagulation in this population. While the CHADS2 score remains the standard tool for assessing stroke risk in atrial fibrillation, its applicability in the context of transient POAF is not well established [7]. It is important to note bleeding risks associated with anticoagulation such as gastric bleeding, hemorrhagic stroke, and cardiac tamponade.
The optimal management of POAF remains uncertain, and a review of current evidence is important to guide clinical practice. This article aims to critically evaluate four key aspects of postoperative atrial fibrillation in the literature: (1) recurrence of atrial fibrillation and its temporal patterns after cardiac surgery; (2) the effectiveness of rate versus rhythm control strategies; (3) stroke risk stratification in the POAF population; and (4) the effectiveness of anticoagulation. By synthesizing recent findings from randomized trials, observational studies, and expert guidelines, we seek to clarify unresolved questions and support a more individualized, evidence-informed approach to the management of POAF.
A narrative literature review was conducted to synthesize current evidence on POAF. Searches were performed in PubMed, the Cochrane Library, and Google Scholar for articles published between January 2015 and March 2024 using the following Boolean combinations: (“postoperative atrial fibrillation” OR “POAF”) AND (“cardiac surgery” OR “CABG” OR “valve surgery”) AND (“management” OR “recurrence” OR “stroke risk” OR “anticoagulation”). The most recent studies published in the last five years were prioritized to ensure that the review reflects the most current evidence and contemporary clinical practice. Only English-language studies involving adult patients were included. Eligible studies reported POAF following coronary artery bypass grafting (CABG), valve, or combined cardiac procedures and addressed at least one of the following domains: recurrence, management strategies, stroke risk, or anticoagulation. Non-surgical atrial fibrillation (AF), pediatric, animal, and case-report studies were excluded. Reference lists of included articles were also screened manually to ensure completeness. The study identification and selection process is summarized in Table 1, which outlines the number of records identified, screened, and included in accordance with a PRISMA-style approach.
| Steps | Description | Number of articles found (n) |
| 1 | Records identified through database searching (PubMed, Cochrane Library, Google Scholar) | 412 |
| 2 | Records after duplicates removed | 334 |
| 3 | Full-text articles assessed for eligibility | 81 |
| 4 | Full-text articles excluded (non-surgical AF, pediatric, animal, case-reports) | 36 |
| 5 | Studies included in the final review | 45 |
AF, atrial fibrillation.
A total of three reviewers independently screened the titles and abstracts for relevance. Studies were included if they focused on adult patients who developed POAF after CABG or valve surgery, and if they addressed one or more of the following key topics: (1) the recurrence and timing of POAF, (2) comparison between rate and rhythm control strategies, (3) stroke risk stratification, and (4) the role of anticoagulation. Studies limited to nonsurgical atrial fibrillation, animal models, or pediatric populations were excluded.
Forty-five articles were ultimately included. From each study, data were extracted regarding sample size, study design, outcomes of interest, and type of intervention. The emphasis was placed on synthesizing clinically relevant findings and their potential implications in real-life practice. Given the narrative nature of this review, no formal risk of bias assessment was applied. Emphasis was instead placed on clinical relevance and consistency across studies. This review did not involve human or animal subjects and thus did not require any ethical approval.
As shown in Fig. 1, a total of 45 studies were included in this review, covering four primary areas: recurrence of POAF, comparison of rate versus rhythm control strategies, stroke risk stratification and anticoagulation. Table 2 (Ref. [1, 2, 6, 8, 9, 10]) summarizes all key research papers used in each subsection.
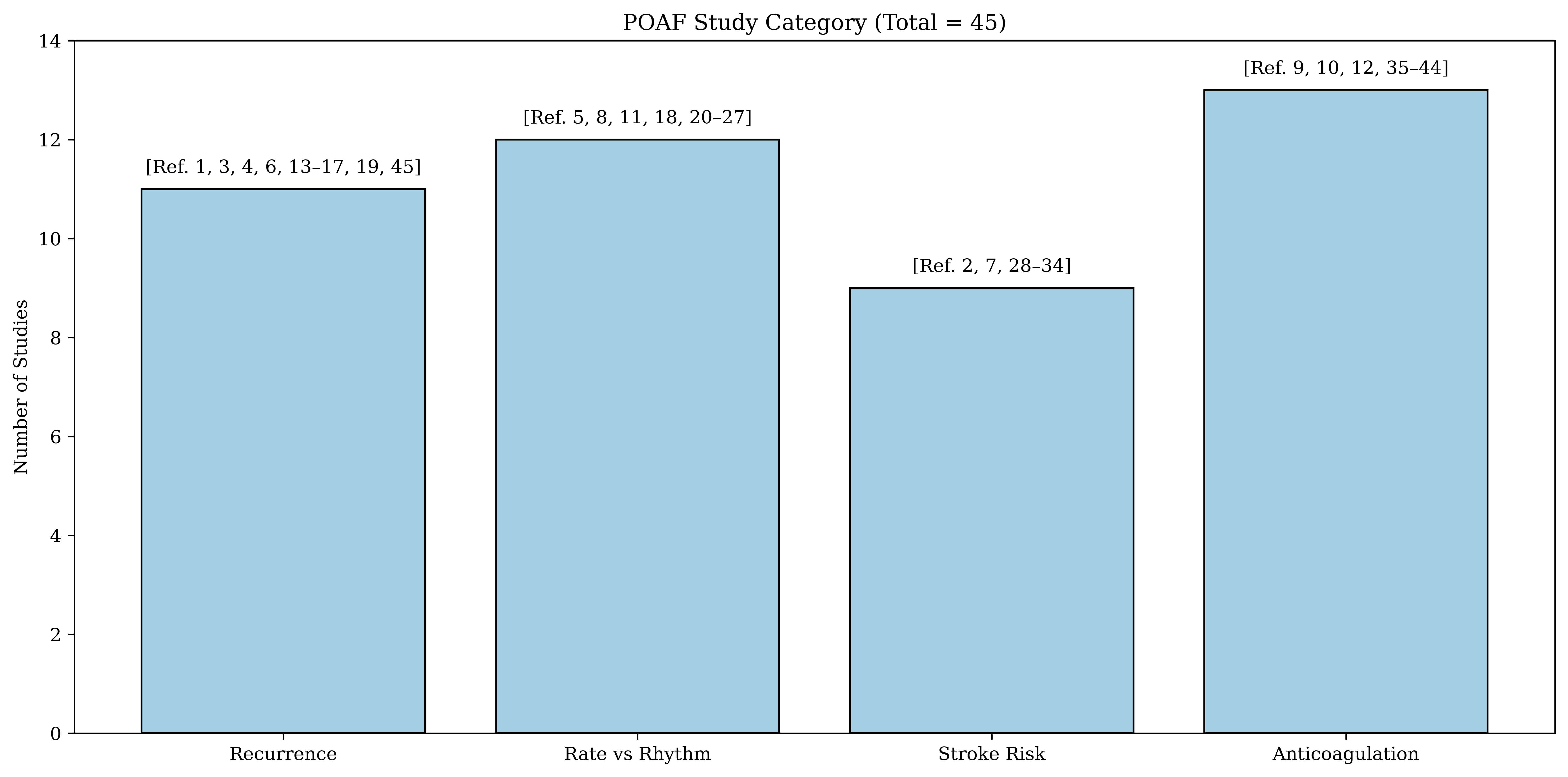 Fig. 1.
Fig. 1.
Distribution of studies by clinical key domain. Overview of the 45 studies included in this narrative review, organized into four key domains of POAF: recurrence patterns, rate vs rhythm control strategies, stroke risk stratification, and anticoagulation. POAF, postoperative atrial fibrillation.
| Author (Year) | Design | Population | N | Focus/intervention | Key findings | Domain |
| Sandgren et al. (2021) [6] | Prospective cohort | CABG | 40 | ILR + handheld ECG | 68% incident AF; 42% recurrence; ILR detected more asymptomatic AF than usual care | Recurrence |
| Abdelmoneim et al. (2021) [1] | Cohort (ILR) | CABG/Valve | 42 | ILR monitoring | High recurrence beyond discharge; many episodes asymptomatic | Recurrence |
| Wang et al. (2022) [2] | Systematic review & meta-analysis | CABG + Valve | 540,209 | Registry/meta-analysis | POAF associated with ↑ short- and long-term stroke risk | Stroke Risk |
| Gillinov et al. (2016) [8] | RCT | CABG/Valve | 2109 | Rate vs Rhythm | 95.9% sinus rhythm at 60 days; no difference in recurrence nor mortality | Rate vs Rhythm |
| Fragão-Marques et al. (2021) [9] | Systematic review & meta-analysis | CABG + Valve | 15,000+ | Anticoagulation | No significant stroke reduction with OAC; bleeding inconsistently reported | Anticoagulation |
| Matos et al. (2021) [10] | Registry | CABG | 160,000 | Amiodarone |
Combo therapy ↓ stroke by 35% without ↑ bleeding | Anticoagulation |
CABG, coronary artery bypass grafting; IRL, implantable loop recorder; RCT, randomized control trial; ECG, electrocardiogram; OAC, oral anticoagulation; Arrow up: increased; Arrow down: decreased.
Eight studies evaluated the recurrence patterns of POAF following discharge after cardiac surgery [1, 6]. These studies primarily aimed to assess the time interval between the surgery and the recurrence of atrial fibrillation, as well as the presence of any associated symptoms. A variety of rhythm monitoring strategies were employed, including 24-hour Holter monitors, handheld ECG devices (such as iECG) and implantable loop recorders. These monitors enabled continuous rhythm surveillance in the weeks to months following hospital discharge. Across the studies, there was considerable variability in the timing of recurrence, with some AF episodes occurring within days of discharge and others occurring weeks later. A significant proportion of these recurrences were asymptomatic, emphasizing the importance of continuous rhythm monitoring even in patients who are clinically stable at hospital discharge.
Seven studies assessed rate versus rhythm treatment strategies in the management of POAF [8, 11]. Rate control commonly involved beta-blockers while rhythm control strategies included two types of cardioversions: electrical cardioversion and pharmacological cardioversion. Among antiarrhythmic pharmacological options, amiodarone and sotalol are the most widely used. One study specifically compared the safety and effectiveness of sotalol versus amiodarone in the postoperative setting, which is further explored in the discussion section. Moreover, two studies compared catheter ablation to medical therapy in patients with heart failure, and the remaining four evaluated rate versus rhythm treatment strategies.
A total of nine studies explored the relationship between POAF and thromboembolic risk [2]. These studies assessed the temporal relationship between POAF and a thromboembolic event, its associated risk factors and any short- and long-term consequences. Moreover, several articles focused on how to prevent such ischemic events using stroke-risk predictor models such as the CHA2DS2-VASc score. Others examined whether tools developed for subclinical atrial fibrillation, such as the subclinical atrial fibrillation (SCAF) score, could better capture the risk profile for POAF patients specifically. Overall, this shows the importance of having effective tools to accurately assess stroke risk in patients with POAF.
A total of nine studies explored anticoagulation strategies in POAF, focusing on identifying the appropriate timing for its initiation and determining which type of anticoagulation provides optimal stroke protection while minimizing bleeding-related complications [9, 10, 12]. Across these studies, multiple subjects were addressed including whether transient episodes of POAF require anticoagulation treatment and how the timing of initiation influences its outcomes. Also, various types of agents were evaluated including warfarin and direct oral anticoagulants such as apixaban, rivaroxaban, and dabigatran to try to highlight differences in safety profiles and bleeding complications among the various agents. Additionally, several studies reported the outcomes related to ischemic stroke prevention, while also documenting complications associated with anticoagulation treatments such as gastrointestinal bleeding, hemorrhagic stroke, and pericardial complications (tamponade). Together, these studies provided important insight into the decision-making process for anticoagulation, helping define when treatment is beneficial and when it may pose unnecessary risk.
Despite decades of research, the optimal management of POAF remains unclear. While often dismissed as a transient arrhythmia, accumulating evidence suggests that POAF is not a completely benign condition. This review discusses the variability in its recurrence and stroke risk, as well as the conflicting data around treatment strategies, particularly regarding rhythm/rate control and anticoagulation.
POAF remains one of the most frequent complications post-cardiac surgery. Despite patients being discharged in sinus rhythm and frequently receiving antiarrhythmic therapies such as amiodarone and sotalol, recurrence rates within the first month ranged between 30% and 60% across studies [6, 13, 14, 15, 16, 17, 18]. Continuous monitoring tools, including implantable loop recorders and handheld ECGs, revealed that many episodes were asymptomatic and would have gone entirely undetected if monitoring devices were not used [6, 19].
The surveillance for early atrial fibrillation recurrence after cardiac surgery (SEARCH-AF) trial demonstrated that nearly 20% of patients had atrial fibrillation recurrences lasting over 6 minutes when monitored continuously with a wearable ECG patch, compared to only 1.7% detection in those followed through usual care [20]. These findings show that relying only on symptoms is not enough and that early rhythm monitoring can be very useful, especially for high-risk patients. Without this, silent recurrences with potential thromboembolic consequences may be missed. Several studies reported that AF episodes tended to recur within the first 30 days, although late recurrences (up to a year) were also observed [1, 14]. While these later episodes were often shorter in duration, their clinical significance remains under debate. Even more concerning is that although approximately 80% of postoperative patients met the criteria for anticoagulation, only 20% were treated [19], suggesting a major gap in post-surgical stroke prevention. Altogether, these findings show that AF requires closer, long-term surveillance. Integrating continuous monitoring into routine post-discharge care may be essential to identify silent recurrences and adapt treatment strategies accordingly.
Although the distinction between rate and rhythm control is clinically less significant in cardiac surgery patients due to the high rates of spontaneous conversion to sinus rhythm, the management of POAF often still involves a decision between both options. Rate control (beta-blockers) is generally favored as a first-line strategy due to their safety profile. In fact, beta-blockers reduce atrial ectopy by decreasing automaticity, which directly lowers the incidence of atrial fibrillation. However, this choice is not always straightforward. Most patients spontaneously convert to sinus rhythm post-op, making rate control sufficient in most cases. However, this assumption does not universally hold, especially in those with structural heart disease, recurrent symptoms, or prolonged AF episodes [21, 22, 23].
Several trials support a rate-first approach, emphasizing that rhythm control does not significantly improve short-term outcomes such as recurrence rates, length of stay, or mortality in the average postoperative patient [8, 11, 22]. 95.9% of patients, regardless of treatment strategy, maintained sinus rhythm 60 days post-operation, suggesting that spontaneous recovery is common and aggressive rhythm control is often unnecessary [8].
That being said, a few special cases still need to be considered. In high-risk patients, particularly those with left ventricular heart failure, rhythm control through catheter ablation accompanied by medical therapy has demonstrated substantial benefits, including reduced mortality and hospitalizations compared to rate control alone [21, 24]. These findings, although not exclusive to surgical patients, suggest that rhythm control may be the main choice in some populations, such as patients with paroxysmal AF as well as patients at risk of cognitive decline. When rhythm control is prioritized medically, the choice often lies between amiodarone and sotalol. Although no randomized controlled trial has directly compared these two drugs in POAF, the sotalol amiodarone atrial fibrillation efficacy trial (SAFE-T) trial in patients with prevalent AF (non-surgical population) showed that amiodarone was more effective than sotalol in maintaining sinus rhythm [16, 25, 26]. However, its use still requires vigilance due to potential hepatic, thyroid, and pulmonary toxicity. Sotalol, while in terms of drug interactions is cleaner and metabolized renally, is also contraindicated in patients with reduced left ventricular ejection fraction (LVEF) or with left ventricular hypertrophy (LVH) and carries a five percent risk of torsades de pointes with corrected QT interval (QTc) prolongation. This explains sotalol’s disappearance from most recent guidelines. The primary differences between amiodarone and sotalol are shown in Fig. 2 (Ref. [5, 25, 27]). Some evidence suggests that early rhythm intervention, particularly in symptomatic or persistent cases, may prevent long-term complications and reduce the frequency of arrhythmia [28].
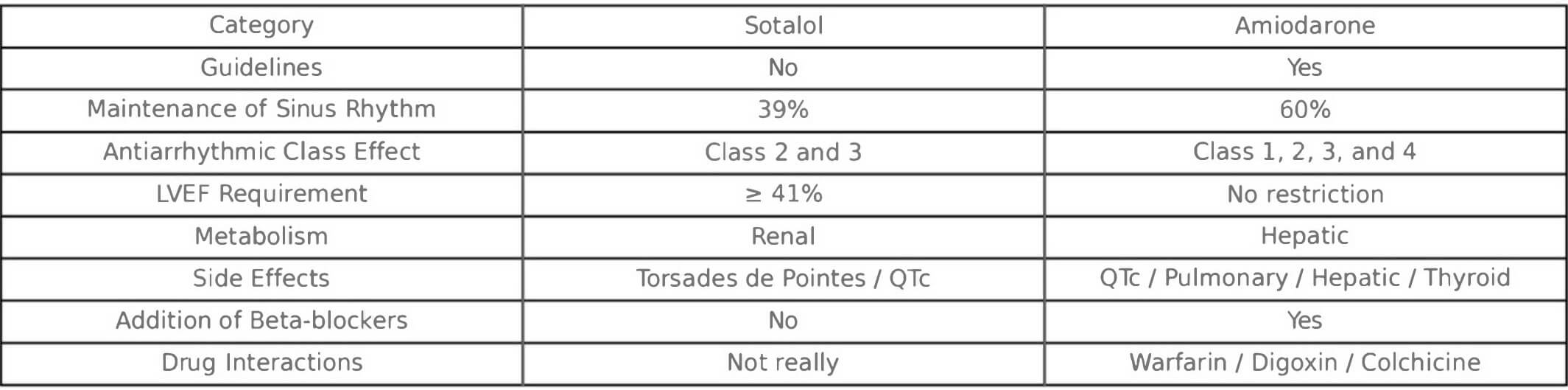 Fig. 2.
Fig. 2.
Comparison of sotalol and amiodarone for rhythm control in postoperative atrial fibrillation. Data adapted from SAFE-T trial [25] and subsequent guideline summaries [5, 27]. The table contrasts key clinical features, efficacy, contraindications, and safety considerations relevant to the postoperative context. SAFE-T, sotalol amiodarone atrial fibrillation efficacy trial; QTc, corrected QT interval.
Finally, it is worth considering additional strategies that may help reduce the burden of postoperative AF in select patients. Mineralocorticoid receptor antagonists like spironolactone can be valuable in supporting atrial remodeling and hemodynamic stability, especially in patients with underlying hypertension or renal dysfunction. When it comes to beta-blockers, tailoring their choice and dosing schedule is crucial. Metoprolol, though commonly used, may not offer consistent coverage throughout the day, particularly in patients with rapid metabolism. In contrast, bisoprolol, when given twice daily, seems to provide more stable rate control with less hypotension, making it a practical option in the early postoperative period. Some surgical teams have also integrated left atrial appendage exclusion as a preventive measure, recognizing its potential to reduce thromboembolic risk even in patients without pre-existing AF. These approaches reflect a shift toward more individualized, physiology-based prevention strategies.
Ultimately, the decision between rate and rhythm control should not be rigid but flexible according to patient-specific factors. In reality, the decision is often shaped by chance and how the clinical course unfolds. A 3-month period can act as a blinding phase, after which a strategy can be defined. This highlights the importance of 3-month follow-up and clear communication between surgery, cardiology, and primary care.
Effective stroke prevention is essential in POAF, which has been linked to higher rates of late stroke and subsequent long-term mortality [29]. Preventing stroke in the context of POAF requires careful risk stratification rather than a one-size-fits-all approach. Short-term stroke rates are significantly elevated in patients with POAF compared to those in sinus rhythm, with the risk particularly pronounced after valve surgery or combined procedures [2]. As illustrated in Fig. 3 (Ref. [2]), the absolute risk of stroke in the POAF group reached 4.5%, nearly doubling that of the non-POAF population at 2.5%. Although the long-term absolute stroke risk is lower, it remains elevated compared to non-POAF patients, suggesting that the risk extends beyond hospitalization [30, 31].
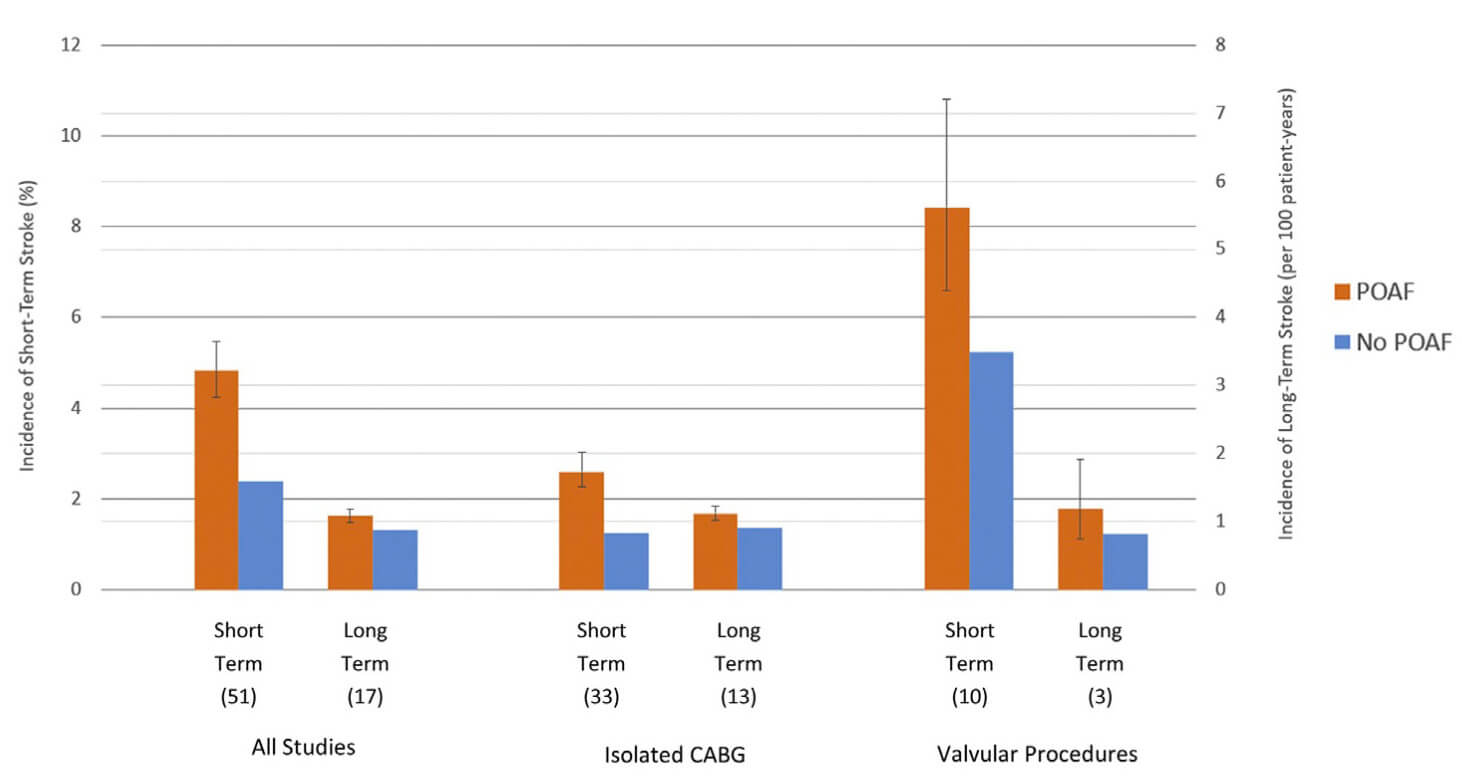 Fig. 3.
Fig. 3.
Incidence of stroke incidence in patients with and without POAF
after CABG and valvular surgery. Data adapted from Wang et al. [2].
Short-term refers to
Risk stratification in POAF is far from straightforward. While the CHA2DS2-VASc score remains a cornerstone in guiding anticoagulation for general atrial fibrillation, its reliability in the postoperative context is less certain. Although stroke risk increases significantly once the CHA2DS2-VASc score reaches 4 or more [7], this threshold may carry a different significance in surgical patients. For example, a postoperative cardiac surgery patient with a CHA2DS2-VASc of 4 has an estimated annual stroke risk of only 2.3%, which corresponds to a score of 2 in the general AF population where anticoagulation is usually recommended. This suggests that postoperative patients may require a higher score to derive a similar net benefit from anticoagulation, and relying on the same cutoffs used in the general population may underestimate thromboembolic risk in this setting.
Adding to this complexity is the presence of SCAF, often detected only through implantable monitors or pacemakers. As shown in Fig. 4 (Ref. [32]), only SCAF episodes exceeding 24 hours clearly raise the risk of stroke [32, 33, 34], while shorter episodes appear less concerning. However, the apixaban for the reduction of thrombo-embolism in patients with device-detected subclinical atrial fibrillation (ARTESiA) trial showed that in high-risk patients, even briefer episodes might justify anticoagulation if the bleeding risk is acceptable. This aligns with findings from the SEARCH-AF study, previously discussed in the section Recurrence Patterns of POAF, which revealed that a substantial number of patients develop subclinical AF after cardiac surgery. In practice, there is a growing trend to anticoagulate SCAF based on increasingly shorter episodes. These findings demonstrate that CHA2DS2-VASc alone is not enough; it must be interpreted within a broader clinical context [35].
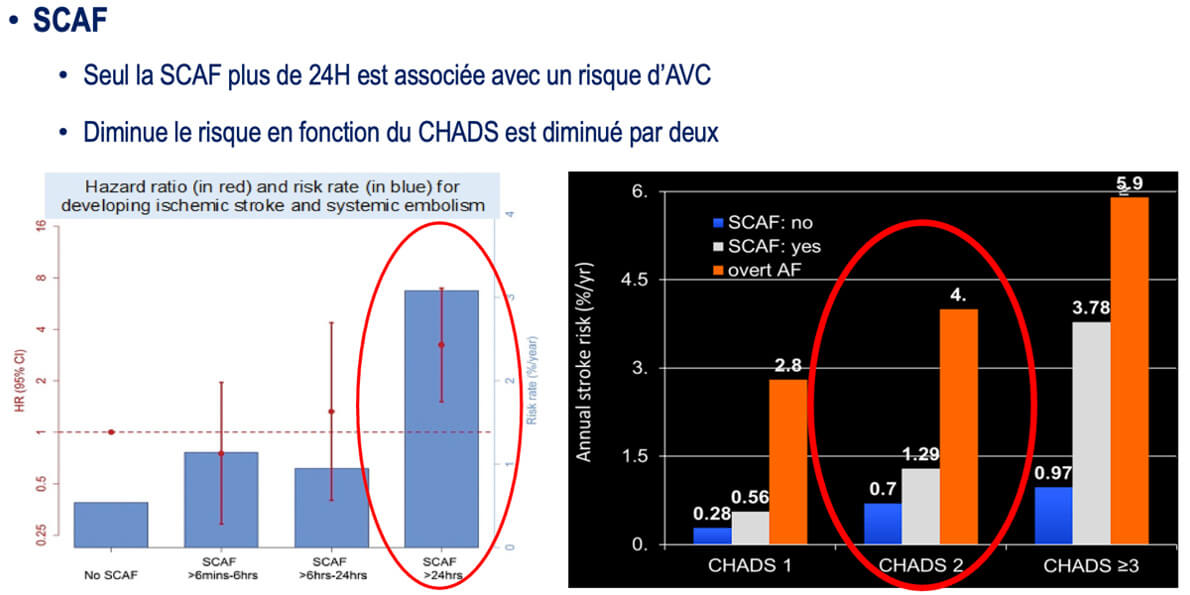 Fig. 4.
Fig. 4.
Stroke risk in subclinical atrial fibrillation (SCAF) by episode
duration and CHADS2 score. Stroke risk associated with SCAF, showing that
only episodes lasting
Moreover, anticoagulation is underused. Fewer than 30% of eligible patients receive treatment within the first 30 days, even with evidence of increased stroke risk and a low number needed to harm (NNH) [36]. Clinicians remain caught between minimizing bleeding and preventing embolic complications [37].
Large observational studies report that only 25% to 30% of patients receive oral anticoagulation after cardiac surgery, a rate that is strikingly low given the perceived stroke risk in this population [9, 38]. This cautious approach reflects the ongoing uncertainty regarding the true benefit of anticoagulation in POAF, especially when weighed against its potential bleeding harms. In clinical practice, the decision to initiate anticoagulation is often influenced by the surgeon, who may be particularly hesitant due to the risk of complications such as tamponade, which can lead to reoperation and may be viewed as a failure of the surgery itself. In addition, variability arises from differences between surgical centers, surgeon preference, patient comorbidities, and the absence of POAF-specific recommendations in major guidelines.
As shown in Fig. 5 (Ref. [39]), the role of anticoagulation in POAF is anything but clear-cut. In cardiac surgery patients, a meta-analysis of ten retrospective studies showed that oral anticoagulation lowered the risk of thromboembolic events by 32% (OR 0.68, 95% CI: 0.47–0.96), which seems promising on the surface. But that benefit came with a trade-off: a significantly higher risk of major bleeding, nearly four times as high as those not anticoagulated (OR 4.30, 95% CI: 3.69–5.02). And when it came to overall survival, there was no meaningful improvement (OR 0.93, 95% CI: 0.70–1.22). In non-cardiac surgical patients, the picture was even less reassuring. There was not even a statistically significant reduction in thromboembolic events, despite the same elevated bleeding risk.
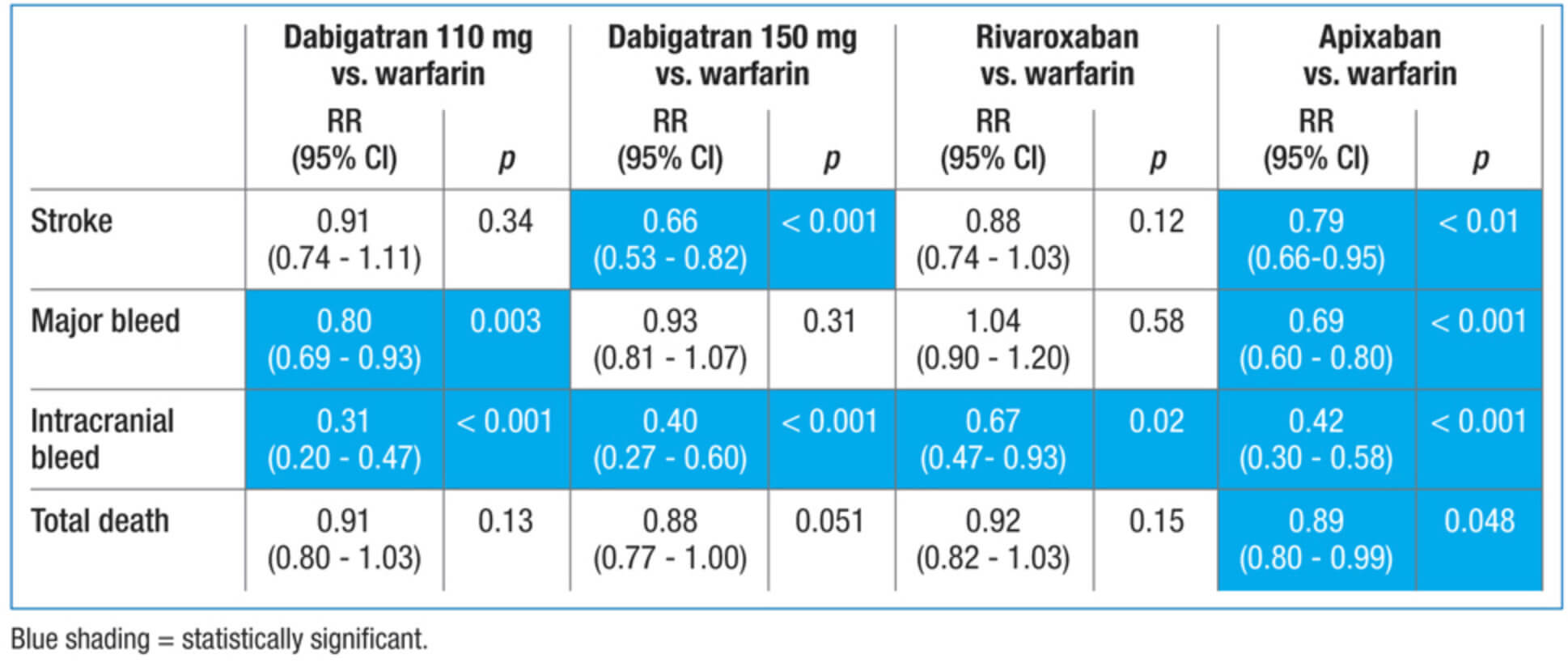 Fig. 5.
Fig. 5.
Major outcomes in anticoagulated patients with atrial fibrillation (general AF population). Comparison of dabigatran, rivaroxaban, and apixaban versus warfarin in randomized trials of the general AF population (not POAF-specific). Outcomes include stroke, major bleeding, intracranial bleeding, and total mortality. Results are provided as relative risk (RR) with 95% confidence intervals. Blue shading indicates statistical significance. Adapted from [39]. This figure is included to provide contextual evidence, as large-scale randomized trials specifically in POAF are lacking.
The inconsistency across studies and the absence of randomized trials show the limitations of current evidence. While a few studies hint at the benefit of anticoagulation, the overall picture remains mixed. For instance, a large retrospective study of over 254,000 patients with POAF found that anticoagulation led to a 0.8% absolute reduction in thromboembolic events, translating to eight strokes prevented per 1000 patients. However, it also reported an additional five bleeding events per 1000 patients [38]. Similarly, in the Fragão-Marques meta-analysis of over 15,000 POAF patients, anticoagulation did not significantly reduce stroke rates and only showed a non-significant trend toward reduced mortality [9]. Bleeding risks were inconsistently reported, adding further uncertainty.
Interestingly, among patients not anticoagulated but discharged on amiodarone alone, the stroke and bleeding rates remained low, suggesting that short-term anticoagulation may not always be necessary when rhythm control is used. Even more compelling, those discharged on both amiodarone and anticoagulation experienced a 35% reduction in early stroke without an increase in bleeding, pointing to a potential synergistic benefit when the two therapies are combined [10].
When anticoagulation is initiated in POAF, the choice of agent requires careful consideration. Warfarin, while historically the standard anticoagulant agent, is less favorable in a cardiac postoperative setting due to challenges maintaining therapeutic International Normalized Ratio (INR) and its association with early tamponade events [40, 41]. Direct oral anticoagulants (DOACs) have increasingly replaced it, offering more predictable pharmacokinetics and fewer monitoring requirements [26, 42]. Among them, apixaban consistently shows the most favorable safety profile, significantly reducing both major and intracranial bleeding compared to warfarin, while preserving stroke protection as seen in Fig. 6 (Ref. [39]). However, apixaban’s antidote (andexanet alfa) can interfere with anticoagulation monitoring during surgery, which presents a challenge if urgent reoperation is needed. In contrast, dabigatran’s antidote (idarucizumab) can be used safely in surgical settings, as recognized by European anesthesiology guidelines. It is important to note that the comparative data presented in Fig. 5 and Fig. 6 are derived from a non-specific POAF population and thus should be interpreted as contextual rather than direct evidence for the postoperative setting. In addition, patients with mechanical valves require lifelong warfarin therapy, limiting the applicability of DOACs to CABG or bioprosthetic valve patients.
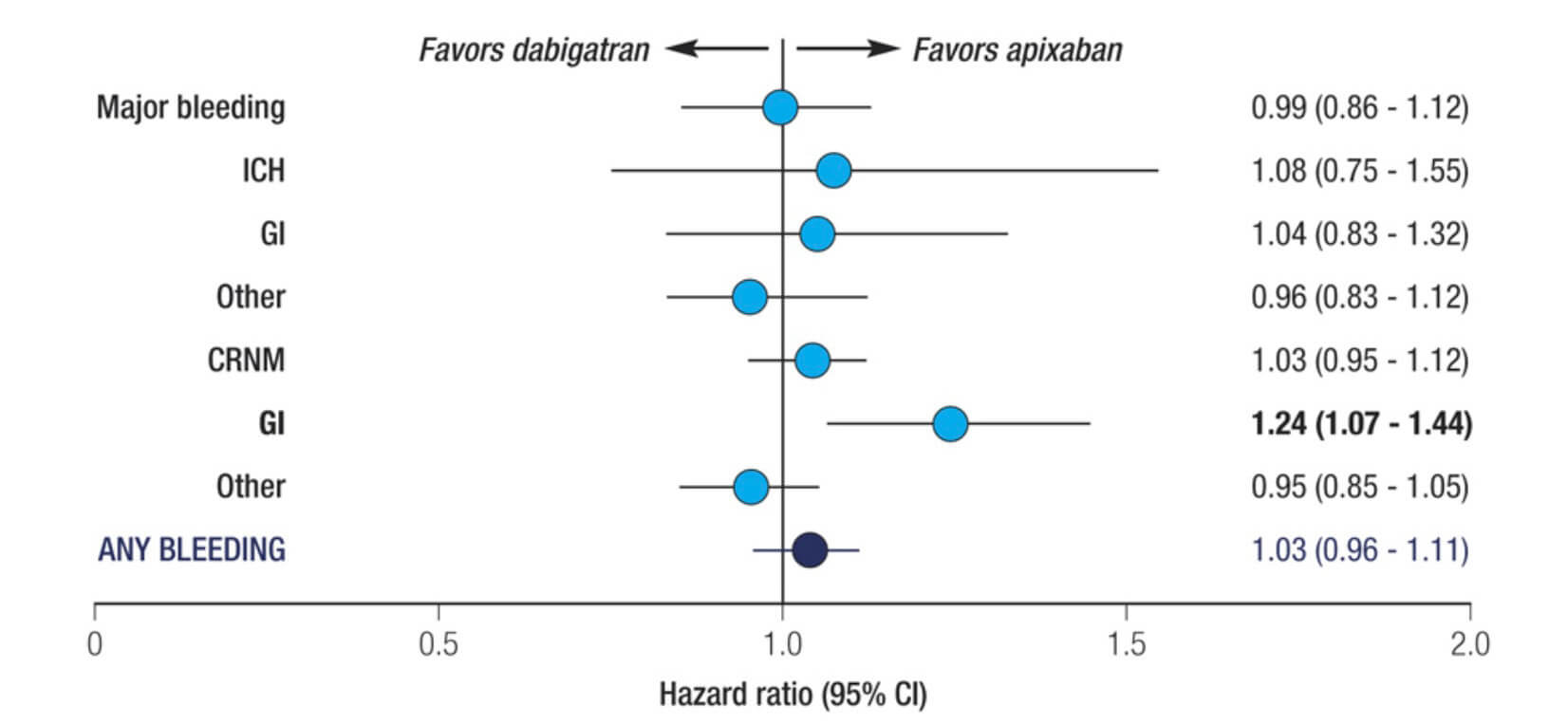 Fig. 6.
Fig. 6.
Adjusted bleeding risks in dabigatran vs apixaban (general AF population, real-world data). Forest plot comparing adjusted bleeding risks between dabigatran and apixaban in the general AF population. Outcomes include major bleeding, intracranial hemorrhage (ICH), gastrointestinal bleeding (GI), clinically relevant non-major bleeding (CRNM), and overall bleeding events. Data adapted from registry-based real-world evidence [39]. This analysis provides contextual safety insights relevant to anticoagulant selection but should not be interpreted as POAF-specific evidence.
Dabigatran, on the other hand, provides even stronger stroke prevention, but at a cost: it significantly increases the risk of gastrointestinal bleeding, with a number needed to harm (NNH) of approximately 200 over two years. In real-world studies, as shown in Fig. 6, patients on dabigatran experienced 24% more gastrointestinal bleeding (GI) bleeds compared to those on apixaban. Additionally, some data suggest that apixaban may carry a slightly higher risk of venous or arterial thrombosis compared to dabigatran, particularly in the early postoperative period.
Cardiac tamponade is a serious but under-recognized complication of anticoagulation therapy following cardiac surgery. It typically presents in two forms: early tamponade and late tamponade. Early tamponade is bleeding-related and often triggered by anticoagulation, while late tamponade, also called post pericardiotomy syndrome, is inflammatory in nature and may also involve pericardial effusions [43]. The risk is particularly relevant in the first month postoperatively. Recent data suggest that early use of DOACs, particularly apixaban, may lower bleeding-related complications compared to warfarin and thereby reduce tamponade risk [12]. Beyond anticoagulant selection, anti-inflammatory strategies may offer additional protection. The COPPS-2 trial demonstrated that colchicine reduced the incidence of postpericardiotomy syndrome with a number needed to treat (NNT) of 10, although its effect on postoperative atrial fibrillation and effusions was more modest [44]. While gastrointestinal intolerance was more frequent, serious adverse events were rare, reinforcing colchicine’s role as a potentially useful adjunct in high-risk patients [23, 45].
A limitation of this review is that most included studies pooled CABG, valve surgery patients and mixed surgical populations, with only one [2] reporting the outcomes separately. This heterogeneity may limit the generalizability of the findings, as the hemodynamic context and arrhythmogenic mechanisms differ substantially between different surgical subtypes. Furthermore, the included literature encompasses diverse study designs such as randomized controlled trials, registry analyses, and meta-analyses, with varying follow-up durations and endpoint definitions, which may result in some variability in reported outcomes. Finally, several studies did not exclusively focus on POAF, and certain data were derived from broader AF populations to only to provide context. Together, these factors highlight both the current evidence gaps and the need for more uniform, procedure-specific, and prospective investigations dedicated to POAF.
POAF remains one of the most frequent complications of cardiac surgery. While often dismissed as transient, accumulating evidence highlights its recurrence potential, association with stroke, and contribution to long-term morbidity.
This review underscores several key insights. First, recurrence of POAF is common, especially within the first month, and is often asymptomatic. Second, while rate control remains the pragmatic first-line approach for most patients, rhythm control may offer benefits in select subgroups, particularly those with heart failure or persistent symptoms. Third, stroke risk stratification in POAF is inadequately served by current tools like CHA2DS2-VASc, which may not fully capture short-term thromboembolic risk after surgery. Lastly, anticoagulation decisions must carefully weigh bleeding risk, especially in the early postoperative period, but emerging data, particularly favoring DOACs like apixaban, suggest its role for POAF.
Ultimately, the management of POAF should be individualized, guided by patient-specific risk factors, AF burden, and clinical trajectory. A one-size-fits-all approach is no longer defensible. Looking forward, the field urgently requires POAF-specific risk prediction models, randomized trials of anticoagulation, and broader evaluation of early rhythm-monitoring strategies. Bridging these gaps remains essential to improve outcomes for patients undergoing cardiac surgery.
AO conceived and designed the study, conducted the literature review, performed data extraction, analysis, and interpretation, and drafted the manuscript. FAD and AG contributed to data acquisition, organization, and interpretation, and critically reviewed the manuscript. DST contributed to the conceptual framework of the study, provided clinical and methodological oversight, assisted in data interpretation, and critically revised the manuscript. OL contributed to manuscript editing, structural refinement, and critical revision to enhance content clarity. Therefore, all authors contributed to the revision of the manuscript, read and approved the final version. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest. Dominique Shum-Tim is serving as one of the Editorial Board members of this journal. We declare that Dominique Shum-Tim had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Giuseppe Santarpino.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.