






 , Takashi Yoshinaga 1, Chih-Hsien Wang 2, Nai-Hsin Chi 2, Hsi-Yu Yu 2
, Takashi Yoshinaga 1, Chih-Hsien Wang 2, Nai-Hsin Chi 2, Hsi-Yu Yu 21 Department of Cardiovascular Surgery, Kumamoto University, 8608556 Kumamoto, Japan
2 Department of Cardiovascular Surgery, National Taiwan University, 10002 Taipei, Taiwan
Abstract
Mitral valve repair has emerged as the gold standard treatment for mitral regurgitation, offering superior long-term outcomes compared with valve replacement. However, the repair process remains one of the most technically demanding and clinically complex procedures in cardiac surgery. Moreover, despite significant advances in surgical techniques, imaging modalities, and transcatheter interventions, the complexity of mitral valve anatomy and pathophysiology continues to present formidable obstacles to clinicians worldwide. The complexity of mitral repair encompasses both technical surgical skills and a sophisticated understanding of valve mechanics, advanced interpretation of imaging, and multidisciplinary team coordination. Thus, as we advance into an era of precision medicine and personalized cardiac interventions, addressing these difficulties becomes increasingly critical for optimizing patient outcomes and advancing the field of structural heart disease. This comprehensive review describes the multifaceted challenges encountered in contemporary mitral valve repair, including anatomical complexity, pathological heterogeneity, technical limitations, patient selection difficulties, and concerns about long-term durability. Moreover, we analyze the outcomes of various repair strategies, discuss the limitations of current approaches, and explore future directions in this rapidly evolving field. This review provides a strategic vision to advance personalized mitral valve interventions and optimize patient outcomes by bridging current limitations and actionable priorities for the future.
Keywords
- cardiac surgery
- computed tomography
- mitral regurgitation
- mitral valve repair
- systolic anterior motion
The mitral valve represents one of the most complex and mechanically sophisticated structures within the human cardiovascular system. Comprising anterior and posterior leaflets, chordae tendineae, papillary muscles, and the mitral annulus, this intricate apparatus functions as a unidirectional valve, preventing retrograde flow from the left ventricle to the left atrium during systole [1]. The challenge of mitral repair has captivated cardiac surgeons and interventional cardiologists for decades, driven by the recognition that successful repair, when achievable, offers superior long-term outcomes compared with valve replacement [2, 3].
The complexity of mitral valve pathology extends far beyond simple structural abnormalities. Functional mitral regurgitation (MR), often associated with left ventricular dysfunction and geometric distortion, presents unique therapeutic challenges that require a comprehensive understanding of ventricular–valvular interactions [4]. Primary MR, resulting from intrinsic valve pathology such as degenerative disease, rheumatic involvement, or congenital abnormalities, demands precise anatomical reconstruction to restore normal valve function [5].
Contemporary mitral repair strategies have evolved significantly from the pioneering work of Alain Carpentier [6], who established the fundamental principles of valve reconstruction based on systematic analysis of leaflet motion abnormalities. The introduction of standardized repair techniques, including annuloplasty ring implantation, leaflet resection and repair, chordal replacement, and papillary muscle procedures, has dramatically improved repair rates and durability [7].
Despite these advances, significant challenges persist in achieving optimal repair outcomes across diverse patient populations and pathological conditions. The heterogeneity of mitral valve disease, ranging from simple posterior leaflet prolapse to complex multisegment involvement with severe annular calcification, requires individualized surgical approaches and sophisticated decision-making algorithms [8]. The advent of transcatheter mitral interventions has transformed the field of mitral repair, providing therapeutic options for patient populations previously considered inoperable while simultaneously introducing novel technical and procedural complexities that warrant further clinical and investigative evaluation [9].
This comprehensive review aims to systematically analyze the multifaceted challenges encountered in contemporary mitral valve repair across anatomical, technical, and clinical domains, and to critically evaluate current surgical and transcatheter repair strategies, with emphasis on outcomes and limitations.
Understanding the three-dimensional (3D) anatomy of the mitral valve apparatus is fundamental to successful repair strategies. The mitral valve consists of two primary leaflets with distinct anatomical characteristics that influence repair techniques and outcomes [10]. The anterior leaflet, larger and more mobile, extends from the anterolateral to the posteromedial commissure and plays a crucial role in left ventricular outflow tract geometry. The posterior leaflet, typically divided into three scallops (P1, P2, P3), demonstrates greater anatomical variability and represents the most common site of degenerative pathology [11].
The subvalvular apparatus, comprising primary, secondary, and tertiary chordae tendineae, provides essential structural support and maintains leaflet coaptation during systole [12]. Primary chordae attach directly to leaflet free edges and are critical for preventing leaflet prolapse, whereas secondary chordae attach to the ventricular side of the leaflets and contribute to overall valve competency. Tertiary chordae, connecting the posterior leaflet to the ventricular wall, help maintain mitral–ventricular continuity and left ventricular geometry.
Papillary muscle anatomy and function significantly influence repair outcomes, particularly in patients with functional MR secondary to ischemic cardiomyopathy [13]. The anterolateral and posteromedial papillary muscles demonstrate distinct blood supply patterns, with the posteromedial muscle being more susceptible to ischemic injury because of its single-vessel blood supply from the posterior descending artery. Moreover, the annulus was significantly dilated and flattened in ischemic MR and is further deformed in anterior compared with inferior myocardial infarction [14].
The mitral annulus, traditionally considered a simple fibrous ring, actually represents a complex 3D structure with dynamic properties throughout the cardiac cycle [15]. The anterior annulus, continuous with the aortic root fibrous skeleton, remains relatively fixed, whereas the posterior annulus demonstrates significant mobility and is prone to dilatation in pathological states. This asymmetric behavior has important implications for annuloplasty ring selection and sizing strategies [16].
Degenerative mitral valve disease, the most common indication for repair in developed countries, typically involves myxomatous degeneration of leaflet tissue and chordal structures [17]. This process leads to leaflet thickening, chordal elongation or rupture, and progressive MR. The pathological changes often follow predictable patterns, with posterior leaflet middle scallop (P2) involvement being most frequent, followed by anterior leaflet middle segment (A2) pathology.
Functional MR presents distinct pathophysiological challenges related to left ventricular remodeling and geometric distortion [18]. Papillary muscle displacement, annular dilatation, and tethering of leaflet edges create complex 3D alterations in valve geometry that must be addressed through comprehensive repair strategies [19]. The interplay between ventricular function, mitral geometry, and regurgitation severity creates a challenging therapeutic paradigm requiring individualized treatment approaches.
Contemporary mitral repair surgery has evolved into a highly specialized field requiring mastery of diverse techniques tailored to specific pathological conditions [20]. The fundamental principle of mitral repair involves restoring normal leaflet coaptation while maintaining physiological valve area and minimizing stenotic gradients. This requires systematic analysis of valve pathology using standardized nomenclature and repair algorithms (Fig. 1).
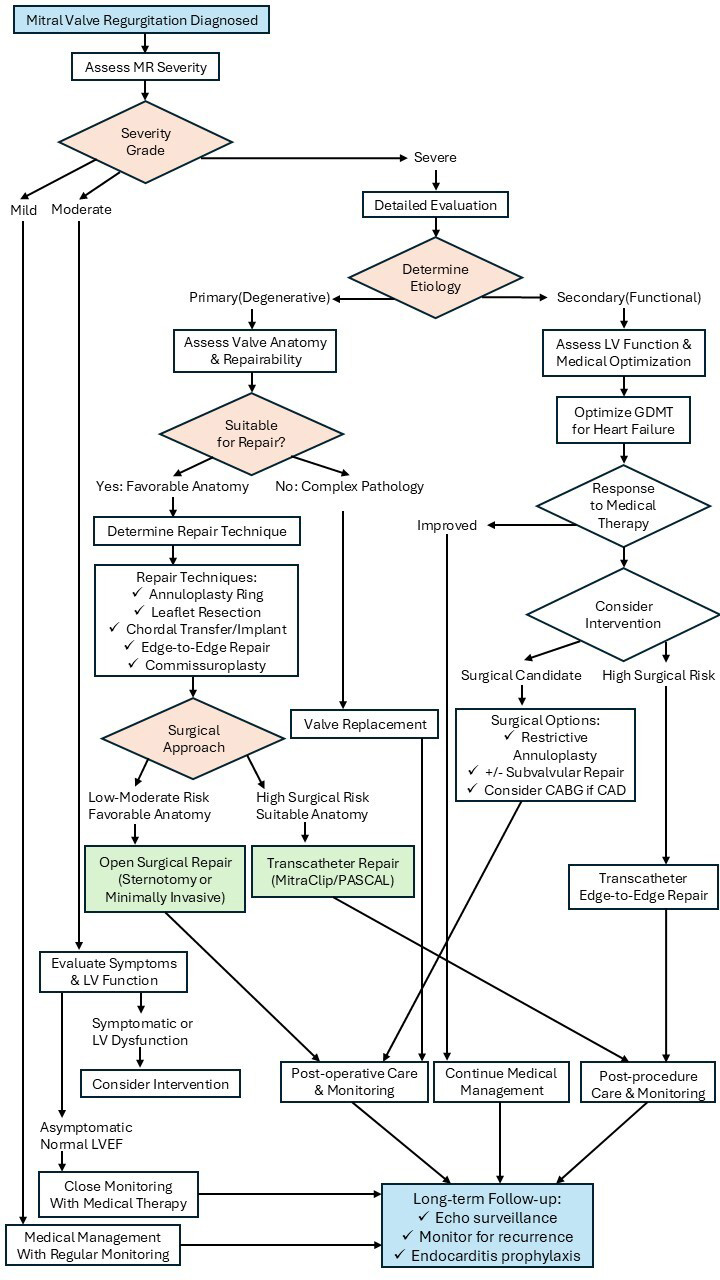 Fig. 1.
Fig. 1.
Flow chart of mitral valve repair. CAD, coronary artery disease; CABG, coronary artery bypass grafting; GDMT, guideline-directed medical therapy; LV, left ventricular; LVEF, left ventricular ejection fraction; MR, mitral regurgitation.
In degenerative mitral valve disease, particularly myxomatous degeneration with leaflet prolapse, several techniques have been established by multiple institutions with excellent long-term durability and freedom from recurrent regurgitation. Posterior leaflet repair remains the most straightforward and successful mitral repair procedure, with excellent long-term durability when performed for isolated P2 prolapse [21]. Quadrangular resection with leaflet reconstruction represents the gold standard technique, involving precise excision of prolapsed tissue followed by reapproximation of leaflet edges. Alternative approaches include triangular resection for smaller lesions and sliding plasty techniques for extensive posterior leaflet involvement. Anterior leaflet repair presents significantly greater technical challenges because of the leaflet’s larger size and complex geometry [21]. Chordal replacement using polytetrafluoroethylene sutures has become the preferred technique for anterior leaflet prolapse, allowing preservation of leaflet tissue while restoring normal coaptation geometry. The technique requires precise measurement of chordal length and optimal positioning to avoid systolic anterior motion (SAM) or residual regurgitation [22]. Annuloplasty ring implantation has become an integral component of most mitral repair procedures, providing annular stabilization and reducing long-term failure rates [23]. The selection between complete rigid rings, partial bands, and flexible rings depends on specific patient factors and pathological conditions. Recent innovations in annuloplasty technology include 3D rings designed to restore physiological annular geometry and saddle-shaped configuration [24, 25]. Complex repair scenarios involving bileaflet pathology, extensive calcification, or commissural involvement require advanced techniques and careful preoperative planning [26]. Patch reconstruction, commissural repair, and combined procedures often become necessary to achieve adequate repair in these challenging cases. The development of standardized protocols and decision-making algorithms has improved outcomes in complex repair scenarios.
For patients presenting with significant ischemic secondary MR accompanied by coronary artery disease necessitating revascularization, concurrent mitral valve intervention during coronary artery bypass grafting (CABG) represents the recommended therapeutic approach, except when elevated perioperative risk or anatomical characteristics favorable for percutaneous coronary intervention are present [27]. Although restrictive annuloplasty using undersized rings constitutes the predominant repair strategy, randomized controlled trial data have demonstrated substantial rates of regurgitation recurrence with this method [28], and beneficial left ventricular reverse remodeling remains modest, particularly among individuals exhibiting an enlarged tenting area exceeding 1.35 cm2/m2 body surface area [29], who frequently require valve replacement rather than repair [30]. Augmenting annuloplasty with subvalvular apparatus procedures in the setting of ventricular chamber enlargement and marked leaflet tethering may enhance repair outcomes [31]; however, the long-term sustainability of such modifications and their effect on heart failure (HF) symptomatology await more comprehensive evaluation.
In patients with atrial secondary MR, recent evidence from matched cohort analyses demonstrates that surgical intervention for MR of atrial origin correlates with reduced HF–related hospital admissions and improved survival compared with optimal medical management alone, even though surgically treated patients presented with more unfavorable baseline clinical characteristics [32]. Multiple nonrandomized investigations additionally indicate that ring annuloplasty procedures yield favorable and sustained results in this patient population, as the technique directly addresses the fundamental pathophysiological process driving regurgitation severity over time [33, 34].
The development of right anterior minithoracotomy and, subsequently, robotic-assisted techniques has transformed mitral valve surgery by enabling complex repairs through small incisions while maintaining the excellent outcomes achieved with conventional approaches [35, 36, 37, 38]. These advances have been driven by patient preference for less invasive procedures, improved visualization technologies, and the development of specialized instruments designed for limited-access surgery. Right anterior minithoracotomy has become the standard minimally invasive approach for mitral valve repair, performed through a 4–6 cm incision in the right fourth or fifth intercostal space. The technique utilizes peripheral cannulation via the femoral vessels for cardiopulmonary bypass, with direct or video-assisted visualization of the mitral valve through the left atrium [39]. Specialized long-shaft instruments and angled retractors provide adequate exposure for leaflet resection, artificial chordae implantation, and annuloplasty ring placement. The learning curve for this approach is significant, with most surgeons requiring 20–100 cases to achieve proficiency [40], though operative times decrease substantially with experience. Modi et al. [36] demonstrated in a systematic review that right minithoracotomy mitral valve surgery resulted in reduced blood transfusions, shorter hospital stays, and lower infection rates compared with sternotomy, with equivalent repair durability. Moreover, repair success rates at experienced centers using the minithoracotomy approach were comparable to those of the sternotomy approach [41].
Robotic-assisted mitral valve repair represents the most technologically advanced minimally invasive approach, first performed by Carpentier et al. in 1998 [42]. The da Vinci Surgical System provides 3D high-definition visualization, articulated instruments with seven degrees of freedom exceeding natural wrist motion, and tremor filtration that enables precise surgical manipulation. The procedure is performed through three-to-four small ports in the right chest, with the surgeon operating from a remote console controlling the robotic arms. Cardiopulmonary bypass is established via femoral cannulation, and the mitral valve is approached through the interatrial groove or transseptal route [43, 44]. Robotic assistance facilitates complex repairs, including posterior and anterior leaflet pathology, commissural lesions, and multiple chordal replacements, with excellent visualization and precision. Although limited literature is available so far, robot-assisted mitral valve repair is comparable to other approaches in terms of safety and early postoperative outcomes, despite being associated with longer operative times.
The future of minimally invasive mitral valve repair continues to evolve with technological advances and expanding experience. Next-generation robotic platforms entering the market may improve competition, reduce costs, and enhance capabilities through better haptic feedback and improved instrument design. Standardized training programs incorporating simulation and structured mentorship are improving the efficiency and safety of the learning curve.
Despite high repair success rates exceeding 95% at experienced centers, postoperative complications can occur that may compromise surgical outcomes. Among these, SAM of the mitral valve, prosthetic ring dehiscence, and iatrogenic mitral stenosis represent three distinct but clinically significant complications that warrant careful attention.
SAM refers to the abnormal anterior displacement of the mitral leaflets toward
the left ventricular outflow tract during systole. This phenomenon results in two
major hemodynamic consequences: left ventricular outflow tract obstruction and
residual MR resulting from incomplete leaflet coaptation. The underlying
mechanism involves complex interactions between altered mitral valve geometry and
abnormal flow dynamics [45]. According to the drag effect theory, increased flow
velocity through a narrowed outflow tract creates a negative pressure gradient
that pulls the mitral leaflets anteriorly. Excess leaflet tissue, particularly in
the anterior leaflet, contributes to SAM by increasing the surface area exposed
to these hemodynamic forces. SAM occurs in approximately 1–15% of patients
following mitral valve repair, with higher rates reported in myxomatous disease
[46, 47]. Several anatomic factors predispose to SAM development, including a
small left ventricular cavity, a narrow aorto-mitral angle (
Prosthetic ring dehiscence refers to partial or complete detachment of the annuloplasty ring from the mitral annulus. Although relatively uncommon, occurring in 1–3% of repairs, it can have devastating consequences, including severe MR, HF, and hemolysis [51, 52]. Dehiscence typically occurs at specific anatomic sites of vulnerability, most commonly the posterior annulus, trigone regions (where tissue quality may be compromised), calcified areas with reduced suture-holding capacity, or sites of previous surgery or endocarditis [52, 53]. Technical factors contributing to dehiscence include inadequate suture spacing or number, excessive suture tension during ring implantation, placement of sutures through calcified or diseased tissue, and inappropriate ring size or type [52, 53]. Echocardiography is the primary diagnostic modality. Transthoracic echocardiography may reveal abnormal rocking motion of the prosthetic ring and worsening MR. TEE provides superior spatial resolution for precise localization of dehiscence, assessment of its extent, evaluation of surrounding tissue quality, and detection of associated complications such as abscess or pseudoaneurysm. 3D echocardiography offers comprehensive visualization of dehiscence location, ring geometry, and stability, aiding surgical planning. Medical management is reserved for minor dehiscence with mild regurgitation and focuses on HF optimization, treatment of hemolysis if present, and close monitoring for progression. Surgical intervention is required in most cases, involving complete reoperation with ring removal, debridement of fibrous tissue around the previous ring, and re-repair with a new annuloplasty ring ensuring adequate tissue quality for suture placement, with possible patch augmentation in areas of deficiency [52]. Mitral valve replacement may be necessary if tissue integrity precludes re-repair. Prevention relies on meticulous surgical technique, including adequate annular exposure, complete decalcification when possible (or reinforcement when not), use of pledgeted sutures in friable or calcified tissue, avoidance of excessive tension during ring seating, and appropriate ring size selection [52].
Functional mitral stenosis following repair represents obstruction to diastolic
flow from the left atrium to the left ventricle. Unlike SAM, which causes
systolic obstruction, post-repair stenosis impairs diastolic filling and can
significantly affect cardiac output and pulmonary pressures. Several mechanisms
contribute to post-repair stenosis, including annular restriction from undersized
annuloplasty rings, reduced leaflet mobility from excessive chordal shortening or
anterior leaflet procedures, altered leaflet geometry from excessive tissue
resection or aggressive sliding plasty, restricted leaflet excursion resulting
from overly short artificial chordae, small native annular size (particularly in
rheumatic disease), and anterior displacement of the posterior leaflet creating
functional stenosis despite adequate anatomic area [54, 55, 56]. Clinically
significant mitral stenosis occurs in approximately 6% of repairs [56], although
mild gradient increases are more common. Surgical factors predisposing to
stenosis include the use of undersized complete rigid rings, excessive posterior
leaflet resection, edge-to-edge technique, and short artificial chordae that
restrict leaflet excursion [54, 55, 56]. Diagnosis requires comprehensive Doppler
echocardiographic evaluation. A mean diastolic gradient
The landscape of mitral valve intervention has been revolutionized by the development of transcatheter repair and replacement technologies, offering treatment options for patients with prohibitive surgical risk [9] or extensive mitral annular calcification [57]. Transcatheter edge-to-edge repair using the MitraClip system is currently the most widely adopted transcatheter mitral intervention. It has demonstrated favorable procedural safety and early clinical outcomes in degenerative and functional MR, although long-term efficacy and durability remain areas of ongoing investigation [58, 59].
The mechanism of transcatheter edge-to-edge repair involves grasping opposing leaflet edges to create a double-orifice configuration, thereby reducing the regurgitant jet area while maintaining sufficient orifice area for forward flow [60]. Patient selection criteria have evolved based on trial data, with optimal candidates demonstrating adequate leaflet length, central regurgitant jets, and favorable valve morphology. The cardiovascular outcomes assessment of the MitraClip percutaneous therapy for heart failure patients with functional mitral regurgitation (COAPT) and percutaneous repair with the MitraClip device for severe functional/secondary mitral regurgitation (MITRA-FR) trials have provided pivotal insights into patient selection for functional MR, highlighting the importance of distinguishing proportionate from disproportionate regurgitation [61, 62] (Table 1, Ref. [9, 61, 62, 63, 64, 65, 66]).
| Trial (year) | Design | Population | Primary endpoint(s) | Outcomes/Key findings |
| EVEREST II (2011 [9], 2015 [63]) | Randomized trial: TEER (MitraClip) vs surgical repair/replacement | Symptomatic severe MR (predominantly degenerative; some functional); patients suitable for either strategy | All-cause death, repeat mitral surgery, or |
Efficacy at 12 months: 55% (TEER) vs 73% (surgery) (p = 0.007). |
| Safety (30-day major adverse events): 15% vs 48%, favoring TEER (p | ||||
| Repeat surgery (12 months): 20% vs 2%, p | ||||
| No significant difference in death or | ||||
| Five-year data: freedom from death, mitral valve surgery, or | ||||
| COAPT (2018 [61], 2021 [64], 2023 [65]) | Randomized trial: TEER + GDMT vs GDMT alone | Symptomatic secondary (functional) MR despite maximized GDMT; LVEF 20–50%, LVESD |
All-cause death, HF hospitalization | HF hospitalizations (24 months): 35.8% (TEER + GDMT) vs 67.9% (GDMT), HR 0.53 (95% CI 0.40–0.70), p |
| All-cause death (24 months): 29.1% vs 46.1%, HR 0.62 (95% CI 0.46–0.82), p | ||||
| Three-year data: mortality 42.8% vs 55.5%, HR 0.67 (95% CI 0.52–0.85), p = 0.001. | ||||
| Five-year data: annualized HF hospitalization 33.1%/year vs 57.2%/year, HR 0.53 (95% CI 0.41–0.68); all-cause mortality 57.3% vs 67.2%, HR 0.72 (95% CI 0.58–0.89); composite of death or HF hospitalization 73.6% vs 91.5%, HR 0.53 (95% CI 0.44–0.64). | ||||
| MITRA-FR (2018 [62]) | Randomized trial: TEER (MitraClip) + medical therapy vs medical therapy alone | Symptomatic secondary MR with larger LV volumes (“less disproportionate” MR); broad inclusion criteria | All-cause death, unplanned HF hospitalization | No significant difference between groups. |
| RESHAPE-HF2 (2024 [66]) | Randomized trial: Transcatheter repair + GDMT vs GDMT | Symptomatic secondary MR on optimized GDMT | Cardiovascular death, HF hospitalization | Primary composite: rate ratio 0.64 (95% CI 0.48–0.85), p = 0.002 (37.0 vs 58.9 events per 100 patient-years). |
GDMT, guideline-directed medical therapy; HF, heart failure; LV, left ventricular; LVEF, left ventricular ejection fraction; LVESD, left ventricular end-systolic diameter; MR, mitral regurgitation; TEER, transcatheter edge-to-edge repair; CI, confidence interval; HR, hazard ratio.
Transcatheter annuloplasty represents another promising approach for functional MR, targeting annular dilatation through mechanisms such as direct annular cinching or indirect reshaping via the coronary sinus [67]. The Cardioband system enables direct annular repair through implantation of a flexible, adjustable device that allows precise control of annular dimensions [68]. However, technical challenges related to device positioning, anchoring stability, and long-term durability remain significant concerns.
Transcatheter chordal replacement technologies offer an additional option for repairing limited leaflet prolapse, potentially expanding treatment strategies for degenerative MR [69]. The NeoChord system facilitates transapical implantation of artificial chordae under echocardiographic guidance, providing leaflet support without the need for cardiopulmonary bypass. Early clinical experience has demonstrated feasibility and procedural safety, though evidence on long-term durability and recurrence rates remains limited.
Transcatheter mitral valve replacement (TMVR) represents the most ambitious frontier in transcatheter mitral intervention, offering complete valve replacement via catheter-based approaches [70]. Multiple device platforms are in various stages of development, each addressing unique challenges such as valve anchoring, paravalvular leak prevention, and avoidance of left ventricular outflow tract obstruction [71]. The complex and variable anatomy of the mitral apparatus, including asymmetrical annular geometry, frequent annular dilatation, proximity to the aortic valve and left ventricular outflow tract, substantial differences between degenerative and functional MR, and frequent absence of annular calcification, creates formidable technical challenges for TMVR deployment and stabilization.
The widespread adoption of these technologies will depend on several factors: demonstration of long-term durability comparable to surgical repair (currently unproven beyond 5 years), cost-effectiveness to justify earlier intervention, and establishment of robust training programs to ensure technical proficiency across diverse centers. The most likely trajectory is a complementary treatment paradigm, in which transcatheter and surgical therapies occupy overlapping yet distinct roles. Transcatheter approaches will likely dominate high-risk and older patient populations, whereas surgery will remain the gold standard for younger, low-risk patients with complex anatomical pathology. The next decade will determine whether transcatheter mitral repair follows the transformative trajectory of transcatheter aortic valve replacement or instead establishes a more modest role as an adjunct to conventional surgery.
Advanced cardiovascular imaging has become indispensable for successful mitral repair, providing detailed anatomical and functional information essential for patient selection and procedural planning [72]. TEE remains the gold standard for intraoperative assessment, offering real-time evaluation of repair quality and immediate detection of complications. 3D TEE has significantly enhanced visualization of mitral valve anatomy and pathology, providing a comprehensive view of leaflet morphology and coaptation patterns [73] (Fig. 2).
 Fig. 2.
Fig. 2.
Three-dimensional transesophageal echocardiography of the mitral valve.
Computed tomography (CT) has emerged as an important adjunctive imaging modality for mitral valve surgery, offering precise anatomical measurements and 3D reconstruction capabilities [74]. CT enables detailed assessment of mitral annular dimensions, leaflet thickness, and spatial relationships with adjacent cardiac structures (Fig. 3).
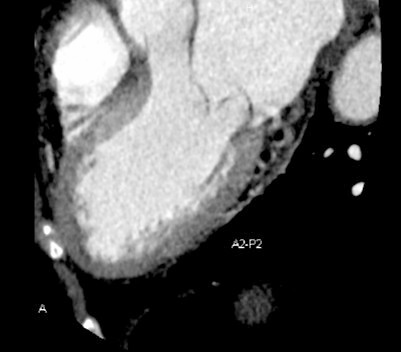 Fig. 3.
Fig. 3.
Computed tomography imaging of mitral valve prolapse (P2) and annular dimensions.
Integration of CT and echocardiographic data through fusion imaging technologies has further improved procedural planning, device sizing, and intraprocedural navigation.
Cardiac magnetic resonance imaging (MRI) provides complementary data regarding left ventricular function, regurgitant volume quantification, and myocardial tissue characterization [75]. MRI-derived metrics, including regurgitant fraction and left ventricular remodeling indices, help guide timing of intervention and predict postoperative outcomes. The ability of MRI to assess myocardial viability and scar distribution is particularly valuable in patients with functional MR secondary to ischemic cardiomyopathy.
Patient selection algorithms now incorporate a combination of clinical, anatomical, and functional parameters to optimize procedural outcomes [76]. Risk stratification models consider variables such as age, comorbidities, ventricular function, pulmonary hypertension, and valve morphology. The heart team approach, integrating cardiac surgeons, interventional cardiologists, and imaging specialists, has become central to decision-making, improving patient selection and overall outcomes [77].
Timing of intervention remains a critical determinant of outcomes, particularly in asymptomatic patients with severe MR [78]. Current guidelines advocate for early referral for mitral repair when feasible, recognizing the superior long-term outcomes associated with valve preservation compared with replacement. However, the optimal timing of intervention in functional MR remains controversial, requiring individualized assessment of ventricular function, symptom burden, and probability of durable repair success.
The assessment of mitral repair outcomes requires a comprehensive evaluation of procedural success, operative mortality, freedom from reoperation, and long-term functional status. Contemporary surgical series demonstrate excellent early outcomes, with operative mortality rates typically below 2% for isolated repairs in low-risk patients [79]. However, outcomes vary considerably depending on patient characteristics, pathological complexity, and institutional experience.
Long-term durability of mitral repair depends critically on the underlying pathology and the quality of the initial repair [7]. Posterior leaflet repairs for isolated P2 prolapse demonstrate excellent 10-year freedom from reoperation, often exceeding 90% in experienced centers. In contrast, repairs involving anterior leaflet pathology, bileaflet disease, or functional MR exhibit higher failure rates of late failure and require more intensive surveillance [80].
The durability of transcatheter mitral interventions is still under investigation. Follow-up data from major clinical trials continue to refine understanding of long-term outcomes [81]. Five-year results from MitraClip studies demonstrate sustained reductions in MR severity and improved functional status, although reoperation rates remain higher than after surgical repair [63]. The long-term performance of newer transcatheter technologies requires further evaluation as clinical experience expands.
Factors associated with repair failure include residual regurgitation at hospital discharge, progressive ventricular dysfunction, and the development of new pathological processes [82]. The importance of achieving complete or near-complete elimination of MR has been demonstrated across multiple studies. Even mild residual regurgitation following repair is associated with an increased risk of late failure and adverse outcomes. Quality metrics have been established for mitral repair programs to standardize outcome reporting and facilitate institutional benchmarking [83]. These include repair rates among appropriate candidates, operative mortality, length of hospital stay, and freedom from reoperation at specified intervals.
Echocardiographic parameters, particularly those reflecting mitral geometry and
left ventricular remodeling, are essential predictors of repair durability in
secondary MR. Unlike degenerative disease, outcomes in functional MR are largely
determined by the degree of leaflet tethering and ventricular remodeling.
Coaptation height (also termed tenting height), representing the distance from
the annular plane to the coaptation point, reflects the extent of leaflet
tethering. Studies have demonstrated that a coaptation height of
Despite significant advances in mitral repair techniques and technologies, substantial challenges and limitations persist that impact clinical outcomes and restrict therapeutic options for certain patient populations [89]. Technical complexity remains one of the greatest challenges in mitral repair, requiring extensive training, experience, and institutional commitment to achieve optimal results. The learning curve for complex repair procedures is steep, and outcomes are highly dependent on surgeon experience and case volume. Heart team collaboration is essential for ensuring procedural quality and achieving favorable clinical outcomes.
Anatomical limitations significantly constrain repair feasibility, particularly in patients with extensive calcification, previous cardiac surgery, or complex congenital abnormalities [90]. Severe mitral annular calcification presents formidable technical challenges that may preclude successful repair and necessitate innovative surgical approaches or alternative treatment strategies [91]. The development of specialized techniques for calcified valve repair remains an active area of investigation.
Patient selection challenges arise from the heterogeneity of mitral valve disease and the complexity of risk-benefit assessment across diverse populations [92]. Older patients with multiple comorbidities present particular difficulties in determining optimal treatment strategies, requiring careful consideration of life expectancy, functional status, and procedural risk. The development of frailty assessment tools and geriatric-specific outcome measures has improved decision-making in this group [93].
Functional MR represents a particularly challenging subset of patients for whom the optimal treatment approach remains controversial [94]. The underlying ventricular pathology driving regurgitation may not be adequately addressed by valve repair alone, leading to high recurrence rates and limited durability. Combined strategies that address ventricular and valvular pathology have become increasingly recognized as necessary for optimal outcomes.
Resource and cost considerations present additional challenges in delivering optimal mitral repair services, particularly in healthcare systems with limited resources [95]. The high cost of advanced imaging, specialized equipment, and prolonged training requirements can create barriers to establishing comprehensive mitral repair programs. Economic analyses demonstrate that mitral valve repair is generally more cost-effective than replacement when repair is successful, supporting continued investment in repair programs to optimize long-term value and patient outcomes [96].
In primary MR, current European guidelines recommend surgical intervention for
symptomatic patients with severe MR or asymptomatic patients with evidence of
left ventricular dysfunction (left ventricular ejection fraction
Secondary MR presents an entirely different timing paradigm because the valve leaflets are structurally normal and MR results from left ventricular dysfunction and geometric distortion. Here, the fundamental question is not “when to operate”, but “whether to operate at all”. The mitral valve is often an “innocent bystander” in a disease process driven by myocardial dysfunction, and correcting the MR alone does not address the underlying cardiomyopathy. Current guidelines recommend considering surgical mitral repair in patients with chronic severe secondary MR undergoing CABG [27]. However, adding mitral valve surgery in patients with moderate secondary MR plus CABG remains controversial [27]. The addition of mitral repair to CABG theoretically reduces MR-related volume overload and may prevent progression of HF, but randomized trials have produced mixed results. Landmark studies comparing CABG alone versus CABG plus mitral repair have inconsistently demonstrated a survival benefit, although some show improved functional status and reduced HF hospitalizations [102, 103]. For isolated severe secondary MR without a concomitant surgical indication, the role of surgical repair remains uncertain. Medical optimization, including guideline-directed HF therapy and cardiac resynchronization therapy when indicated, remains the first-line approach. The durability of repair in secondary MR is significantly inferior to primary MR, with recurrence rates approaching 30% at 2–3 years as a result of ongoing ventricular remodeling [104, 105].
The divergent timing considerations for primary versus secondary MR reflect fundamental differences in pathophysiology and natural history. In primary MR, the weight of evidence increasingly favors earlier surgical intervention in appropriate candidates at experienced centers, before irreversible ventricular remodeling occurs. In secondary MR, a more conservative, highly selective approach is warranted, with surgery reserved for patients most likely to benefit. Future research must address several critical gaps: defining biomarkers or imaging parameters that define the optimal intervention window in asymptomatic primary MR, developing reliable predictors of repair durability in secondary MR, and determining which patients with secondary MR derive meaningful benefit from surgical correction beyond medical therapy alone.
The future of mitral repair is being shaped by rapid advancements in technology, imaging modalities, and a deeper understanding of valve pathophysiology. Artificial intelligence and machine learning applications are beginning to transform patient selection, procedural planning, and outcome prediction in mitral valve disease [106]. Deep learning algorithms are now being developed to automatically quantify and classify cardiac structure, function, and disease severity from echocardiographic images with greater accuracy than traditional assessment methods [107, 108]. Machine learning models that integrate multimodal data, including 3D TEE, cardiac CT, clinical variables, and biomarkers, are being trained to identify optimal candidates for specific repair techniques, whether transcatheter edge-to-edge repair, surgical annuloplasty, or chordal replacement [109]. Advanced algorithms capable of analyzing complex imaging data and clinical data may improve decision-making and optimize treatment strategies.
Novel repair techniques, including robotic surgery, continue to emerge, addressing previously challenging anatomical scenarios and expanding repair options [110]. The integration of robotics and artificial intelligence in cardiac surgery is poised to significantly improve the precision and clinical outcomes of mitral valve repair procedures [111]. Robotic platforms with haptic feedback and autonomous capabilities may reduce variability in repair techniques and improve learning curves for complex procedures. Virtual and augmented reality applications provide new training paradigms and intraoperative guidance systems. Recent studies have shown that robotic mitral valve repair yields durable results with low reoperation rates, even in cases involving complex degenerative disease and multisegment prolapse [112].
Tissue engineering approaches using biocompatible materials and cellular therapies offer potential for creating living valve substitutes that can grow and remodel with the patients themselves [67]. Regenerative medicine applications in mitral repair may represent an exciting frontier with potential for fundamental advances in valve biology and repair durability. Current research focuses on tissue engineering strategies utilizing biodegradable scaffolds seeded with autologous or allogeneic cells to promote valve regeneration and remodeling [113, 114, 115, 116, 117]. Studies have demonstrated that mesenchymal stem cells, endothelial progenitor cells, and induced pluripotent stem cells can differentiate into valve interstitial and endothelial cells under appropriate biomechanical and biochemical stimulation, suggesting their potential for creating functional valve tissue [113, 114, 115, 116, 117]. The application of growth factors such as transforming growth factor-beta and vascular endothelial growth factor has shown promise in enhancing cellular proliferation and extracellular matrix production within engineered valve constructs [113, 114, 115, 116, 117]. Clinical translation of these regenerative techniques faces significant challenges, including achieving appropriate mechanical properties capable of withstanding hemodynamic forces in the mitral position, preventing calcification and thrombosis, and ensuring long-term durability of regenerated tissue. The combination of cellular therapies with conventional repair techniques may enhance healing and improve long-term outcomes.
3D printing technologies now enable creation of patient-specific models for surgical planning and the development of customized repair devices [118]. Using CT or MRI data, surgeons can fabricate anatomically accurate 3D-printed models of individual patients’ mitral valve apparatus, allowing for preoperative simulation and optimization of repair strategies. These physical models enhance understanding of complex pathology, facilitate communication within surgical teams, and have been shown to reduce operative time and improve procedural confidence [119]. However, widespread adoption of 3D printing is currently limited by a lack of robust evidence demonstrating clinical effectiveness, as well as by high costs and workflow complexity [120].
The complexity of mitral repair necessitates comprehensive training programs that address technical skills and theoretical knowledge [121]. Traditional surgical training models are being supplemented with simulation-based learning, virtual reality platforms, and structured mentorship programs. The development of standardized curricula and competency-based assessment tools ensures consistent training quality across institutions. Minimally invasive and robotic approaches require additional specialized training beyond conventional open surgical techniques [122]. Dedicated fellowship programs and proctoring systems have been developed to facilitate safe adoption of these technologies. The learning curve for complex minimally invasive procedures remains substantial, requiring careful case selection during the training period. Continuing education and skill maintenance are essential given the rapid evolution of mitral repair techniques and technologies. Professional societies, such as The Mitral Foundation, have established certification programs and continuing education requirements to ensure practitioner competency. The development of standardized outcome metrics and quality assurance programs facilitates ongoing assessment and improvement of clinical practice, exemplified by initiatives such as The Mitral Valve Repair Reference Center Award.
Multidisciplinary team training has become increasingly important as mitral repair involves collaboration between cardiac surgeons, interventional cardiologists, anesthesiologists, and imaging specialists [123]. Team-based training programs that simulate real clinical scenarios improve communication and coordination during complex procedures. The establishment of heart team approaches has been shown to improve patient outcomes and reduce complications.
Access to advanced mitral repair services varies significantly worldwide, with disparities related to healthcare infrastructure, economic resources, and availability of trained specialists [124]. Developed countries usually have well-established programs with excellent outcomes, whereas developing nations face substantial challenges in providing optimal care. Vervoort et al. [125] reported the current global state of access to cardiac surgery. They found large disparities existed between regions, ranging from 0.12 adult cardiac surgeons per million population in sub-Saharan Africa to 11.12 per million in North America. International collaboration and knowledge transfer programs are essential for addressing these disparities. Training exchange programs and international fellowships play a crucial role in capacity building and skill dissemination. Experienced centers can provide training opportunities for specialists from developing countries while also benefiting from exposure to different approaches and perspectives. The establishment of regional centers of excellence can serve as hubs for training and referral within geographic regions. Task-sharing models and regional training centers have emerged as potential solutions to the workforce shortage, enabling local healthcare providers to develop proficiency in surgical and percutaneous mitral valve interventions. Moreover, partnerships between institutions in high-income and resource-limited settings have facilitated knowledge transfer and capacity building, although sustainable models require long-term commitment and adequate funding.
The cost-effectiveness of mitral repair programs must also be considered in resource-limited settings where healthcare budgets are constrained. Economic analyses demonstrate the long-term benefits of repair over replacement, supporting investment in training and infrastructure. However, the initial costs and learning curves required to establish effective repair programs may pose substantial challenges for some healthcare systems [96].
Telemedicine and remote consultation platforms are emerging as valuable tools to expand access to expert opinion and guidance in mitral valve surgery [126]. These technologies enable collaboration between specialists across different regions and facilitate case discussions and treatment planning. The development of standardized protocols and decision-making algorithms can further improve outcomes, even in centers with limited experience.
Mitral valve repair involves complex technical, anatomical, and clinical challenges that continue to evolve with advances in surgical and transcatheter techniques (Fig. 4). Despite considerable progress, achieving optimal outcomes remains difficult because of the wide spectrum of valve pathologies and patient variability. Repair usually yields excellent results in straightforward cases such as isolated posterior leaflet disease but is less durable and successful for complex lesions involving the anterior leaflet or functional regurgitation.
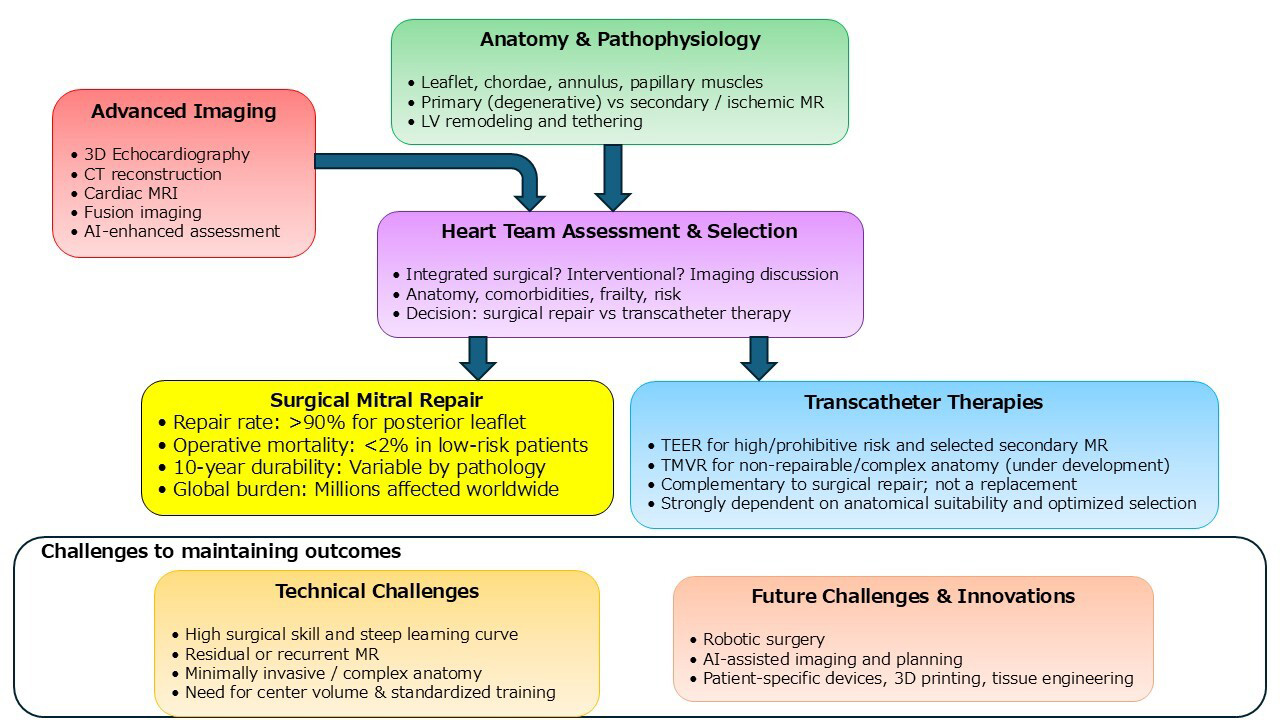 Fig. 4.
Fig. 4.
Central illustration of this review article. AI, artificial intelligence; CT, computed tomography; LV, left ventricular; MR, mitral regurgitation; MRI, magnetic resonance imaging; TEER, transcatheter edge-to-edge repair; TMVR, transcatheter mitral valve replacement; 3D, three-dimensional.
Transcatheter approaches have expanded treatment options for high-risk patients but have introduced new technical and durability concerns. Advances in multimodal imaging and artificial intelligence have improved patient selection and procedural guidance, although expertise in image interpretation remains essential.
The future of mitral repair lies in personalized treatment strategies that incorporate genetic and biomarker data while leveraging innovations such as robotics, artificial intelligence, and regenerative medicine. Ongoing development of new surgical and device technologies aims to improve repair durability and broaden applicability across patient populations.
Success will depend on sustained investment in research, multidisciplinary training programs, and the establishment of centers of excellence. Regional and global collaboration, along with equitable access to education and cost-effective therapies, will be critical for advancing care worldwide. The focus remains on the evidence-based optimization of repair techniques to preserve the advantages of valve repair over replacement by delivering durable, safe, and effective mitral valve treatment for diverse patient populations.
TF contributed to the design of this work and drafted the manuscript. JT and TY drafted and analysed the work. CHW, NHC, and HYY analysed the manuscript and revised it critically for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest. Toshihiro Fukui is serving as one of the Editorial Board members of this journal. We declare that Toshihiro Fukui had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Isaac George.
During the preparation of this manuscript, the author used Claude in order to assist with the writing of the manuscript.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.