




 , Sanjhai Ramdeen 1,†, Matthew Kazaleh 1, Jonathan Eliason 2, Bo Yang 1, David M. Williams 3
, Sanjhai Ramdeen 1,†, Matthew Kazaleh 1, Jonathan Eliason 2, Bo Yang 1, David M. Williams 31 Department of Cardiac Surgery, University of Michigan, Ann Arbor, MI 48109, USA
2 Department of Vascular Surgery, University of Michigan, Ann Arbor, MI 48109, USA
3 Department of Interventional Radiology, University of Michigan, Ann Arbor, MI 48109, USA
†These authors contributed equally.
Abstract
Endovascular therapy provides a new treatment modality for patients with aortic disease. By avoiding the morbidity of open surgery, endovascular approaches make treatment possible for a larger array of patients. However, the durability and long-term survival benefit of endovascular aortic intervention require further discussion and additional follow-up. We believe that the characterization of the role of endovascular therapy involves close risk-benefit analysis based on patient risk, disease presentation, native and pathological anatomy, and long-term outlook. Through review of the randomized prospective literature and relevant retrospective data, we explore the role of catheter-based solutions in abdominal and thoracic aortic disease, with a focus on aortic aneurysm and aortic dissection (AD). For patients with appropriate anatomy, endovascular aortic repair (EVAR) has largely supplanted open aortic repair (OAR) in the treatment of abdominal aortic aneurysm (AAA), both in the elective setting and during rupture. Similarly, thoracic endovascular aortic repair (TEVAR) has gained popularity in treating disease of the descending thoracic aorta, in both aneurysmal degeneration and AD. Similar adoption has been seen in treating other disease states, namely traumatic aortic injury. However, we recognize the current limitations of endovascular therapy and detail the innovations being pursued to advance endovascular therapy in the future.
Keywords
- EVAR
- TEVAR
- aorta
- endovascular therapy
- aortic aneurysm
- aortic dissection
Those afflicted with aortic disease represent a high-risk patient subset with increased mortality risk. In fact, overall global death rates from aortic disease (abdominal aortic aneurysm, thoracic aortic aneurysm, and acute aortic dissection) increased from 2.49 cases per 100,000 people in 1990 to 2.78 cases per 100,000 people in 2010 [1]. Traditionally, open surgery was the only option for patients. However, peri-operative mortality ranged from 2.7 to 7.5% open abdominal aortic repair [2]. Open repair of the distal thoracic aorta has early mortality rates reaching as high as 20% [3, 4]. Hence, ever since approval of the first device in 1999, endovascular therapy for aortic disease has gained popularity for providing treatment without the morbidity of open surgery [5].
However, the efficacy of endovascular therapy in the treatment of various aortic pathologies in different locations is an evolving discussion. This manuscript reviews the current literature on the efficacy of endovascular therapy in the treatment of aneurysmal disease and aortic dissection, both in the abdominal and thoracic aorta. The role of endovascular therapy is dependent on patient risk, disease presentation, and vessel anatomy, both for the management of immediate risk and for the optimization of long-term survivorship. Additionally, we recognize the current limitations of endovascular therapy and the associated innovations being studied to advance therapy in the future (Fig. 1).
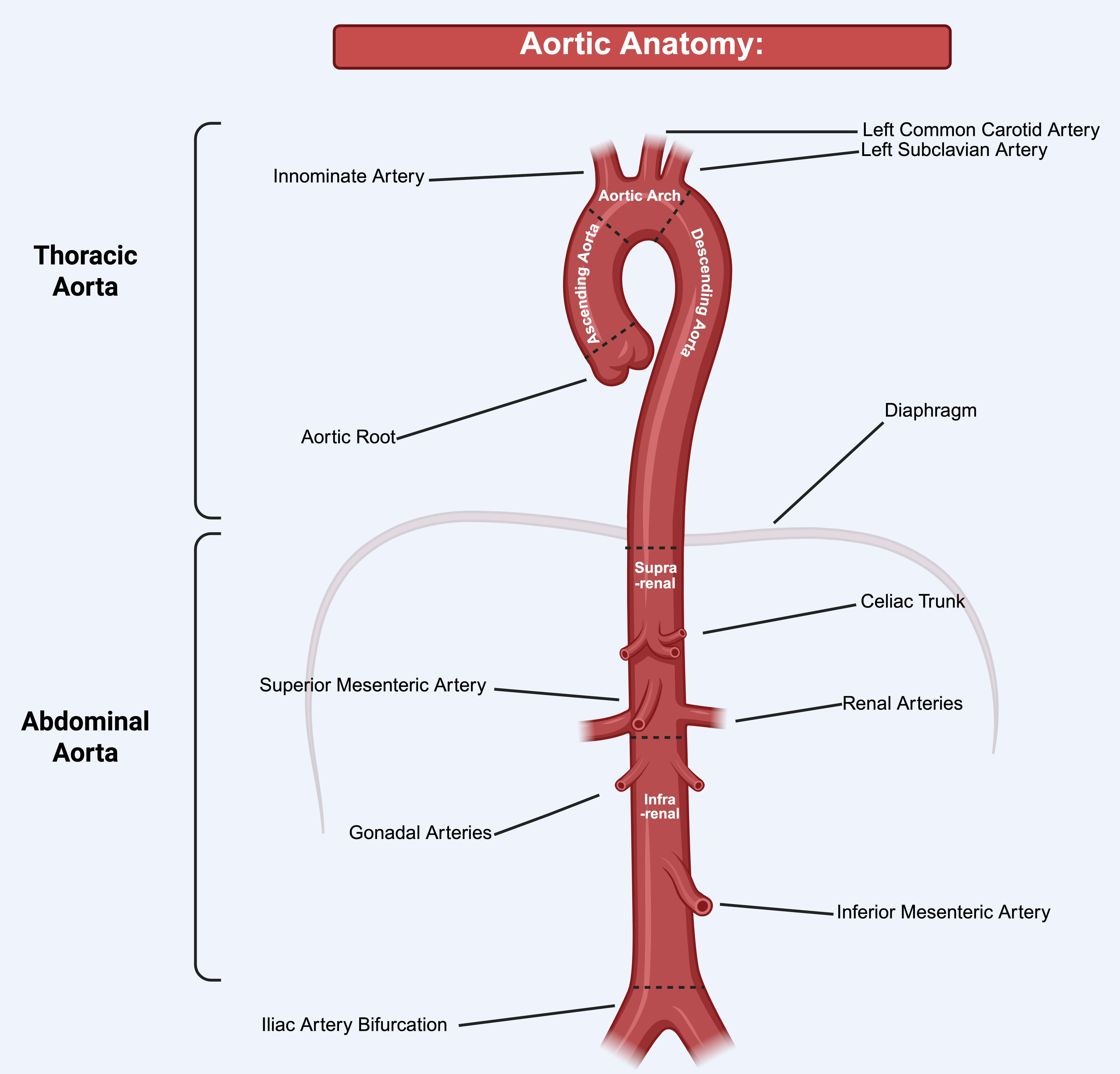
Based on a literature search of the PubMed database, articles related to the outcomes of endovascular surgery of abdominal and thoracic aortic disease were collected. Search terms included, but were not limited to: “aortic aneurysm”, “aortic dissection”, “endovascular aortic repair”, “endovascular aortic repair (EVAR)”, “thoracic endovascular aortic repair (TEVAR)”, “aortic trauma”, “REBOA”, “mesenteric malperfusion syndrome” etc. The literature included, but were not limited to prospective randomized controlled trials, retrospective reviews of population level data, registry data, and single institution series. Systemic reviews and meta-analysis were also included among these studies. Furthermore, expert opinion pieces and other reviews were also included to provide further context and insight. This review references a wide variety of sources. Of note, the Journal of Vascular Surgery was heavily referenced in this text. However, references were selected from a broad subject matter and a variety of authors, thereby enhancing the diversity and objectivity of the manuscript’s academic foundation. Each manuscript was individually reviewed by the authors for relevance and scientific rigor. Years of publication ranged from 2000 to 2024. Fig. 1 illustrates the vascular anatomy referenced in this review.
Endovascular therapy in the treatment of abdominal aortic aneurysm has provided many patients with an effective treatment option without the morbidity of open repair. Abdominal aortic aneurysm (AAA) is the 13th leading cause of death in the United States, with up to 40–70% operative mortality upon rupture [2]. Despite this, improved screening measures and improvements in the management of atherosclerotic risk factors have resulted in a favorable decline in mortality [6, 7]. The increased adoption of endovascular aortic repair (EVAR) therapy in the treatment of AAA may also play a role in improved survival.
Ever since FDA approval in 1999, EVAR has quickly surpassed open aortic repair (OAR) as the primary treatment for elective AAA. The 2022 AHA/ACC guidelines give a level 1 recommendation for shared decision making for AAA in deciding between endovascular and open repair for low- and medium-risk patients when vessel anatomy is suitable for endovascular repair [8].
Prospective data have substantiated the non-inferiority of EVAR to OAR in the
elective treatment of AAA in patients with appropriate vessel anatomy. Namely,
the 2011 ACE Trial demonstrated no significant difference in short- or
medium-term mortality between EVAR (n = 150) and OAR (n = 149) (30-day mortality:
1.3% vs. 0.6%, 3-year survival: 86.3% vs. 86.7%, p = 0.24). EVAR did
demonstrate a shorter length of stay (5.8 days vs. 8.4 days, p
In certain scenarios, OAR may be preferred over EVAR. These scenarios include
prolonged life expectancy (
The use of EVAR in high-risk populations has also been studied. The EVAR-2 Trial, which compared EVAR to isolated medical therapy in patients at too high risk for OAR, showed lower rates of aneurysm-related mortality in EVAR (3.6% vs. 7.3%, p = 0.02), but no difference in all-cause mortality (21% vs. 22.1%, p = 0.97) [14]. This study was limited by a high crossover rate and pre-procedure mortality in the EVAR group [15]. The 2022 AHA/ACC guidelines currently give a 2A recommendation for EVAR in high-risk patients to reduce the risk of 30-day morbidity and mortality [8].
The 2022 AHA/ACC guidelines provide a level 1 recommendation for percutaneous, ultrasound-guided femoral artery access over femoral artery cutdown for vascular access to reduce blood loss, time of wound healing, hospital length of stay, and post-operative pain [8]. The 2014 (Percutaneous Access Versus Open Femoral Exposure in Endovascular Aortic Aneurysm Repair) PEVAR trial and the 2019 Percutaneous Access in Endovascular Repair vs. Open (PiERO) Trial have validated the improved outcomes with a percutaneous access approach [16]. In cases of small, tortuous vessel anatomy or cases of groin scarring, a cut-down approach can be entertained. When iliac disease precludes percutaneous access, iliac stenting or surgical implantation of a conduit to the iliac artery may be required [17].
Most devices require at least a 10–15 mm proximal seal zone with angulation less than 60 degrees, but the instructions for use may vary by device. Ideally, the aortic neck should be parallel and free of heavy thrombus or calcification. Aortic neck diameters up to 32 mm can be accommodated when considering appropriate oversizing and available endograft sizes. Appropriate sizing involves appraisal of aortic neck conicity to prevent endoleak from under sizing and graft pleating from oversizing.
In patients that do not have a 10–15 mm proximal landing zone, partial renal artery coverage or stenting may be required. These limitations can be addressed using techniques such as partial renal artery encroachment with adjunctive renal artery stenting. Additionally, complete renal artery coverage with a parallel “snorkel” stent to the renal artery can be employed. However, enthusiasm for this technique has been tempered by a 9% rate of Type IA endoleak [18].
The 2022 ACC/AHA guidelines also provide a 2A recommendation for the use of a
fenestrated endovascular device (F-EVAR) over open repair for patients with
moderate to high operative risk to reduce risk of perioperative complications
[8]. A 2020 review of 3253 patients with complex AAA pathology from the Vascular
Quality Initiative who underwent OAR, FEVAR, or physical modified endograft
placement showed no significant difference in perioperative mortality (5.7% vs.
3.3%, p = 0.17), but open repair was associated with higher rates of
myocardial infarction (MI), acute kidney injury (AKI) and initiation of new
dialysis. On analysis of propensity-weighted long-term survival, the F-EVAR group
demonstrated higher long-term mortality than the open repair group (p =
0.02). A 2019 study of the American College of Surgeons NSQIP database compared
all patients undergoing elective AAA repair using the Zenith Fenestrated
Endovascular Graft (ZFEN) device to standard infra-renal EVAR and open complex
aortic repair defined as repair of juxtarenal or suprarenal proximal aneurysmal
extent. On univariate analysis, ZFEN demonstrated lower perioperative mortality
(1.8% vs. 8.8%, p = 0.001) and lower overall complication rates (11%
vs. 33%, p
In the case of ruptured AAA (rAAA), the 2022 ACC/AHA guidelines give level 1
recommendations for pre-operative computed tomography angiography (CTA) to assess
endovascular candidacy and usage of endovascular treatment over open repair [8].
The 2014 Immediate Management of Patient with Ruptured Aneurysm: Open Versus
Endovascular Repair (IMPROVE) trial, composed of 613 patients with rAAA
randomized to endovascular or open surgery demonstrated a 36.4% 30-day mortality
with EVAR compared to 40.6% with OAR (p = 0.62). Endovascularly treated
patients were more likely to be discharged home compared to those receiving open
repair (94% vs. 77%, p
rAAA may present with large infra-renal aortic diameters and short neck lengths, which may impact candidacy for endovascular intervention. A sub-analysis of aorta morphology of patients in the IMPROVE trial demonstrated that an aneurysm neck length was inversely related to open and overall mortality (OR: 0.72 for every 16 mm of added aortic neck length). Since patients with shorter aortic necks do not meet the criteria for endovascular treatment, more patients with higher mortality risk end up receiving open repairs. This may explain why an early mortality difference is seen in the retrospective, observational literature, but not in randomized controlled trial data [22]. Overall, rAAA has historically presented a 50% mortality rate with open repair, while endo-first strategies have demonstrated mortality rates as low as 18.5%. The combination of increasing institutional endovascular experience, creation of organized protocols for rAAA patients including early preoperative cross sectional imaging, and early aortic balloon occlusion under fluoroscopy has allowed endovascular therapy to supplant open repair in the treatment of ruptured abdominal aortic aneurysm [8].
The 2022 ACC/AHA guidelines call for repair of intact descending thoracic aortic aneurysm (TAA) at diameters at or above 5.5 cm; repair can be pursued at diameters below 5.5 cm in presence of risk factors for rupture. ACC/AHA guidelines provide a level 1 recommendation for TEVAR over open surgery in the treatment of patients without connective tissue disease, who meet the appropriate size threshold and anatomic criteria for endovascular repair [8].
Safety and feasibility trials of FDA-approved devices demonstrated technical
success in
A 2011 retrospective review of US Medicare claims data compared 12,573 patients
receiving open repair to 2732 patients who underwent TEVAR. TEVAR patients
demonstrated lower crude 30-day all-cause mortality in patients with non-ruptured
(6.1% vs. 7.1%, p = 0.07) and ruptured (28% vs. 46%, p
Another 2013 review of US Medicare claims data compared the results of TEVAR and
open repair based on patient volume. High volume was defined as
In the treatment of ruptured descending TAA (rTAA), endovascular repair is
preferred over open repair because of decreased perioperative death and morbidity
(Grade 1 Recommendation, 2022 ACC/AHA Guidelines). A 2009 study from our group,
looking at single institution data of all patients receiving either open or
endovascular repair for ruptured thoracic aorta from 1993 to 2009, uncovered 35
patients undergoing TEVAR and 34 patients undergoing open repair. This study
included 18 patients with a fusiform aneurysm, 22 patients with a saccular
aneurysm, and 29 patients with aortic dissection. Recipients of TEVAR were those
who had favorable anatomy for endovascular therapy or those who were deemed too
high risk for OAR. TEVAR patients demonstrated a lower 30-day mortality (11.4%
vs. 26.5%, p = 0.13). Multivariate analysis identified hemodynamic
instability (p
A 2011 retrospective review from Yale of rTAA patients from 7 institutions spanning from 1995–2010, compiled 92 patients receiving TEVAR and 69 patients undergoing open repair [26]. TEVAR patients had a significantly lower composite outcome of death, stroke, and permanent paraplegia compared to open repair (21.7% vs. 36.2%, p = 0.044). On multivariate regression analysis, patient age (p = 0.036) and hypovolemic shock (p = 0.03) were independent predictors of death, stroke, or paraplegia. Utilization of TEVAR was noted to be significantly protective in this study (OR: 0.44, 95% CI: 0.20–0.95, p = 0.039). The study also demonstrated a decrease in rTAA-related 30-day mortality, from 32.4% before 2000 down to 15% from 2005–2009. This decrease correlated with a fall in the number of open rTAA repairs from 100% before 2000, to 57.4% between 2000–2004, to 10% after 2005 [26]. Hence, the advent of TEVAR in the management of rTAA may play a role in reducing mortality rates.
A larger 2017 analysis of the National Inpatient Sample between years 1993 and
2012 identified 1622 patients receiving TEVAR (13%), 2808 patients undergoing
open repair (23%), and 7969 undergoing non-operative management (64%) for
isolated rTAA. TEVAR demonstrated an increasing proportion of repairs from 2% of
total admission in 2003–2004 to 43% in 2011–2012 (p
More recently, a 2024 study from the University of Pennsylvania looked at
long-term mortality and re-intervention after TEVAR for both intact and ruptured
thoracic aortic aneurysms. Compared to intact TAA, rTAA had a lower 30-day
survival (69.2% vs. 96.9%, p
Preoperative computed tomography (CT) angiogram for TEVAR patients to evaluate
iliofemoral access and consideration of conduit access in the setting of
inadequate iliac artery anatomy are both grade 1 recommendations from 2022
ACC/AHA guidelines. Choosing total percutaneous access over open femoral cutdown
in patients with favorable anatomy is a 2A recommendation [8]. A retrospective
review of the Gore Global Registry for Endovascular Aortic Treatment (GREAT)
registry identified 944 patients undergoing TEVAR. In this group, 315 (33.4%)
patients received total percutaneous access, 505 patients (53.6%) received
surgical cut-down, and 124 (13.1%) received a hybrid access technique.
Increasing sheath size did not correlate with the risk of access site
complications. In total, 18 patients (1.9%) receiving TEVAR reported an access
site complication. Total percutaneous access was associated with lower rates of
access site complications compared to open cut-down and hybrid techniques (p =
0.03) Interestingly, a linear relationship between access site complications and
body mass index (BMI) was established regardless of access technique (p
As a general rule, proximal and distal landing zones greater than 20 mm are required for an appropriate seal; however, when treating more angulated or longer aortic segments, larger landing zone sizes may be required. This is pertinent to atherosclerotic aneurysms, since the degenerative process may extend past aneurysmal segments leading to higher risks of device migration, wall trauma or endoleak. Additionally, stiffness of the endograft may prevent appropriate apposition of the stent graft with the inner curve of the aorta, resulting in bird beaking and eventual device failure [31].
Celiac artery (CA) coverage is sometimes, albeit uncommonly, required in order to establish a quality distal seal. ACC/AHA guidelines give a grade 2A recommendation to confirm adequate collateralization to mitigate risk [8]. A 2014 retrospective analysis from the University of Alabama identified 18 patients (5%) who received CA coverage out of 366 patients who received a TEVAR over a 9-year period. Only 1 patient in this group required pre-operative superior mesenteric artery (SMA) stenting before the index procedure. At the end of the procedure, 2 patients (11%) demonstrated Type 1A endoleaks, 2 patients (11%) demonstrated Type 1B endoleaks, and 2 (11%) demonstrated Type 2 endoleaks. Post operatively, 30-day mortality of 1 patient (5%) was observed, 2 (11%) developed visceral ischemia, 1 (5%) developed weight loss, and 2 (11%) developed spinal cord ischemia. Four more patients died within the year, of which 1 was an aneurysm-related death. Lastly, 50% survival was reached at 40 months as per survival analysis. The authors recommend preoperative angiographic evaluation of mesenteric collateral flow before CA coverage and assert that new symptoms should not occur unless the SMA is compromised [32]. Hence, preoperative assessment of vessel anatomy and close postoperative surveillance for symptom onset are recommended when CA coverage is considered.
When patients present with inadequate space for an adequate seal zone, branch
vessel encroachment may be necessary. Based on single center reviews, left
subclavian artery (LSA) coverage is required in up to 40% of TEVAR cases in the
treatment of TAA [33]. Review of early feasibility trials for TEVAR with various
devices have shown
Primary revascularization for patients with Zone 2 coverage can be achieved through preoperative carotid-subclavian bypass or subclavian transposition. For Zone 1 coverage with left carotid artery occlusion, additional right-to-left carotid bypass can be employed for revascularization. Endovascular options for arch vessel revascularization have also been described.
A 2009 meta-analysis from the United Kingdom, looking at TEVAR for all
pathologies, found an increase in stroke rates for TEVAR patients with LSA
coverage compared to those without LSA coverage, both without revascularization
(4.7% vs. 2.7%, p = 0.005) and with primary revascularization (4.1%
vs. 2.6%, p = 0.02). There was also a noted increase in spinal cord
ischemia rates for patients without LSA revascularization (2.8% vs. 2.3%,
p = 0.005), but not for those who received revascularization (0.8% vs.
2.7%, p = 0.35) [36]. These findings indicate that revascularization
may not entirely protect against neurological complications. Similarly, a 2016
meta-analysis from the Cedar Sinai group saw a significantly heightened stroke
rate with LSA coverage compared zone 3 and zone 4 TEVARs (7.4% vs. 4%,
p
Currently, AHA/ACC guidelines provide a level 1 recommendation for revascularization before TEVAR to prevent spinal cord ischemia, reduce stroke risk, and risk of other ischemic complications [8]. Hence, thorough consideration of revascularization is advised.
Complete endovascular solutions to aortic arch disease have been sought after due to the risk of mortality and stroke with open and hybrid approaches. Endovascular treatment of the aortic arch is limited due to the high curvature of the vessel, heightened hemodynamic forces, and the presence of great vessels. Parallel stent grafting of branch vessels including chimneys, periscopes, and snorkels has been described, especially in the urgent/emergent setting when encroachment onto great vessel territory is required. Aortic grafts are typically oversized to prevent gutter formation and leakage around parallel grafts. Parallel grafts typically extend 1–2 cm past aortic grafts to prevent branch collapse. However, strong evidence supporting endovascular treatment in aortic arch disease is lacking. Feasibility trials may demonstrate reasonable technical success. However, rates of endoleak, need for conversion to open surgery, and short-term morbidity are barriers to further implementation [39, 40].
In-situ fenestration of endovascular stent grafts has also been proposed as a solution for branch vessel management in the treatment of aortic arch disease. Modalities include needle fenestration, laser fenestration, and radio-frequency fenestration, which are used to puncture the stent graft, followed by balloon dilation and stenting of branch vessels. The proximal aspect of the branch vessel is typically flared to increase the diameter and reduce the number of endoleaks. Stent material, branch vessel angulation, presence of vessel dissection, and proximity to other vessels are important variables to consider when utilizing fenestration [41, 42, 43]. The chances of fabric tears and branch vessel thrombosis increase the risk of these procedures.
Experiences with physician-modified endografts (PMEG) have been described in the literature. The role of back table modified endografts in the treatment of aortic arch disease is unclear. These are typically done under institutional review board (IRB) with investigator device exemption (IDE) approval prior to use. PMEG is the least commonly used branch vessel management strategy. Fenestrations are typically made with an ophthalmic cautery device and then suture-reinforced with radio-opaque markers. After this, the graft is manually replaced into the sheath. Concerns about the long-term durability of home-made fenestrations have limited widespread application of this technique. However, practitioners should still be aware of its use as a bailout maneuver in acute presentations. A 2020 meta-analysis of all PMEGs identified six articles accounting for 239 patients. Aneurysmal disease accounted for 25.9% of patients, while 64.4% had acute or subacute aortic dissection. Technical success was achieved in 93.7%. Thirty-day mortality was 2.9%, cerebrovascular accident (CVA) occurred in 2.1% of patients, and paraplegia occurred in 0.4% of patients. While these early results are encouraging, 70% of cases were done at 4 high volume centers, thus affecting result generalizability [44]. While studies have demonstrated proof of concept in the total endovascular management of aortic arch disease, limitations still exist preventing large scale adoption of these techniques.
The principal role of endovascular therapy in Type B aortic dissection is in the management of complicated disease. Complicated disease is defined by the presence of aortic rupture, static and/or dynamic malperfusion, dissection extension, acute aortic enlargement, intractable pain, uncontrolled hypertension. In theory, stent coverage of the entry tear redirects flow through the true lumen, preventing dynamic malperfusion, and promoting aortic remodelling. However, static malperfusion may remain unresolved and should be treated appropriately.
The 2015 GORE TAG 08-01 study was a prospective, multi-center, non-randomized
study of 50 patients with type B aortic dissection complicated by either
malperfusion or rupture who underwent TEVAR. In total, 4 patients (8%)
experienced operative mortality, and 28 patients (56%) experienced at least one
serious adverse event in the post-procedure period. In particular, 9 patients
(18%) experienced stroke, 5 patients (10%) experienced new aortic dissection
events, and 4 patients (8%) experienced spinal cord ischemia. Regarding
long-term analysis, 4 patients experienced late death, putting 2-year survival at
nearly 85%. For the 2-year follow-up of 41 patients who had successful stent
exclusion of their entry tear, 20 patients demonstrated complete false lumen
thrombosis (74.1%) while 6 patients (22.2%) experienced partial thrombosis.
Lastly, at their 2-year follow-up, 10 patients (38.3%) experienced a greater
than 5 mm decrease in overall aortic diameter, while 3 patients (11.5%)
experienced a greater than 5 mm increase [45]. These findings identify a higher
complication and stroke rate in TEVAR in the setting of the life-threatening
complications of Type B dissection. However, TEVAR did demonstrate acceptable
late survival and positive aortic remodeling compared to previous literature. The
TAG Complex Pathology Trial, an earlier 2009 study from the same author, looked
at 59 patients who received TEVAR deployment for either complicated type B
dissection, traumatic tear, or thoracic aneurysm rupture. Of the 19 patients who
received therapy for complicated type B dissection, 3 patients (16%) experienced
the 30-day composite endpoint of mortality or paraplegia compared to a 24.1%
mortality rate seen in historic controls (n = 800) undergoing open repair
(p
More recently, the 5-year follow-up data from the Dissection Trial were published. This study followed 50 patients who received the Valiant Captivia thoracic stent graft from Medtronic for acute complicated type B aortic dissection. Of note, 94% of patients presented with DeBakey class IIIB dissection. At their 5-year follow up, patients demonstrated 83% freedom from aneurysm-related mortality. Furthermore, 89% of patients demonstrated decreased complete false lumen thrombosis. True lumen diameter was stable or increased in 94% of patients and false lumen diameter was stable or decreased in 77% of patients. These findings indicate that TEVAR in the treatment of complicated type B aortic dissection does promote positive aortic remodeling when assessed at long-term.
Retrospective literature also supports the role of endovascular therapy in Type B dissection. A 2015 meta-analysis from Athens University of 2531 patients undergoing TEVAR for acute complicated type B dissection and 1276 patients undergoing open repair. The TEVAR group demonstrated lower in-hospital mortality (7.3% vs. 19%), lower stroke rates (3.9% vs. 6.8%), and comparable 5-year survival (61%–81% for TEVAR vs. 44–82% for open repair based on the study) [47]. Another 2021 meta-analysis identified 2565 patients receiving TEVAR for acute complicated Type B aortic dissection presenting with either rupture or malperfusion. Actuarial survival analysis adjusted for study quality demonstrates 85.4%, 79.1%, 69.8%, and 63.1% survival at 2, 4, 6, and 8 year-follow up, respectively. Freedom from re-intervention was 73.2%, 67.6%, 63.7%, and 63.7% at the aforementioned time-points. While these findings suggest long-term performance with endovascular intervention, randomized controlled trial data is required to further substantiate these trends [48].
Outside of patients with malperfusion or rupture, acute intractable pain or uncontrolled hypertension may also characterize a subset of patients who would benefit from endovascular repair. A 2010 review of the International Registry of Acute Aortic Dissection (IRAD), identified 69 patients with Type B aortic dissection without classic complications, but with severe pain and/or uncontrolled hypertension. Compared to 296 uncomplicated cases of Type B Aortic Dissection, those with pain or elevated blood pressure had higher in-hospital mortality (17.4% vs. 4%, p = 0.0003). However, with endovascular management, no significant difference in in-hospital mortality was found between groups (3.7% vs. 9.1%, p = 0.5). On multivariate regression analysis, refractory pain or hypertension were identified as predictors of in-hospital mortality (OR: 3.31, p = 0.041) [49]. At the University of Michigan, acute pain and uncontrolled hypertension have been associated with iliofemoral or renal malperfusion, and are therefore sought for and, if indicated, treated in every interventional radiology procedure. Therefore, the definition of complicated disease may extend to hypertensive patients and those with intractable pain.
Current management guidelines dictate that uncomplicated Type B Dissections are treated with anti-impulse therapy. As per the 2022 ACC/AHA guidelines, medical therapy as an initial strategy is a grade 1 recommendation, while endovascular management for those with high-risk characteristics is given a 2B grade [8]. However, emerging evidence may call for a paradigm shift to a more aggressive approach in appropriately selected patients.
The 2014 ADSORB trial, a randomized prospective trial studied 61 patients with
acute uncomplicated type B aortic dissection (
In contrast, the 2009 INSTEAD Trial, another randomized controlled trial
comparing medical management (BMT) versus medical management and endovascular
therapy, focused on cases of uncomplicated Type B dissection of subacute or older
chronicity (
Ascending aortic aneurysm or type A aortic dissection is typically treated with open surgery. Inadequate spacing for quality seal zones as well as the elasticity, curvature, and pulsatile forces of the ascending aorta limit endovascular treatment of the ascending aorta [55]. Feasibility trials have been conducted [56]. However, open surgery remains the gold standard for treatment of the ascending aorta.
Mesenteric malperfusion syndrome (MMS), defined as clinical end-organ dysfunction or necrosis secondary to inadequate bowel perfusion, can result in a five-fold increase in mortality risk for type A aortic dissection (AD) patients [57]. In fact, the in-hospital mortality of MMS has ranged from 65–100% [58, 59, 60, 61, 62, 63, 64]. Hence, the team at the University of Michigan has pioneered a mesenteric reperfusion-first approach in appropriately selected type A aortic dissection patients.
A 2019 review from our group of 597 type A aortic dissection patients treated between the years 1997 and 2017, identified 135 patients with type A aortic dissection with mesenteric malperfusion. In the second decade of the study, the risk of dying from organ ischemia was 6.9 times higher than the risk of death from aortic rupture. However, in-hospital mortality for patients with mesenteric malperfusion who received endovascular revascularization followed by staged aortic repair was only 4%, which was much lower when compared to the projected 33% in-hospital mortality with an upfront open repair approach (p = 0.001) [65]. Hence, for the hemodynamically stable patient with clinical mesenteric malperfusion, endovascular mesenteric reperfusion before open aortic repair may improve survival. At the University of Michigan, unless a patient presents with rupture, wide-open aortic insufficiency, neurovascular malperfusion, or cardiac tamponade, stable patients with clinical mesenteric malperfusion syndrome will undergo mesenteric reperfusion with interventional radiology (IR), with close follow up of bowel and lower extremity perfusion. After this, staged aortic repair is pursued. As per the Michigan Classification System, malperfusion can be dynamic, resulting from dissection flap coverage of the branch vessel orifice by the dissection flap, or static, resulting from primary vessel dissection, or can be a combination of both. Either type can be complicated by true lumen thrombosis. Standard TEVAR can treat dynamic, but not static malperfusion. Hence, primary endovascular dissection flap fenestration and/or stenting is utilized to treat mesenteric malperfusion syndrome. If a thrombus is present in the iliac and superior mesenteric arteries, localized thrombolysis or thrombectomy is used before central aortic flow is restored. If thrombolysis is used, transesophageal echocardiography (TEE) is used to monitor the pericardial sac and cardiac function. A gradient of less than 15 mmHg between the ascending aorta and compromised branch vessel is indicative of successful revascularization. Following revascularization, the patient is closely monitored in the intensive care unit (ICU) setting to confirm resolution of mesenteric or lower extremity malperfusion syndrome. In addition, up-front repair of ischemia and clearance of thrombus also creates reliable transition zones between viable and non-viable tissue for the vascular or general surgeon. Based on clinical and laboratory monitoring of ischemia by the ICU, vascular surgery, and general surgery, exploratory laparotomy and bowel resection and limb fasciotomy are considered and performed as indicated. Only after resolution of ischemia and repair of ischemic damage in stable patients is aortic repair considered. The traditional up-front aortic surgery approach not only delays time till mesenteric reperfusion but also accentuates the ischemic insult through the stressors of surgery. The treatment algorithm at the University of Michigan requires close inter-departmental cooperation between intensivists, aortic surgeons, and interventional radiologists. Integration of surgical and endovascular expertise has allowed practitioners at our institution to innovate and improve patient care (Fig. 2, [65]).
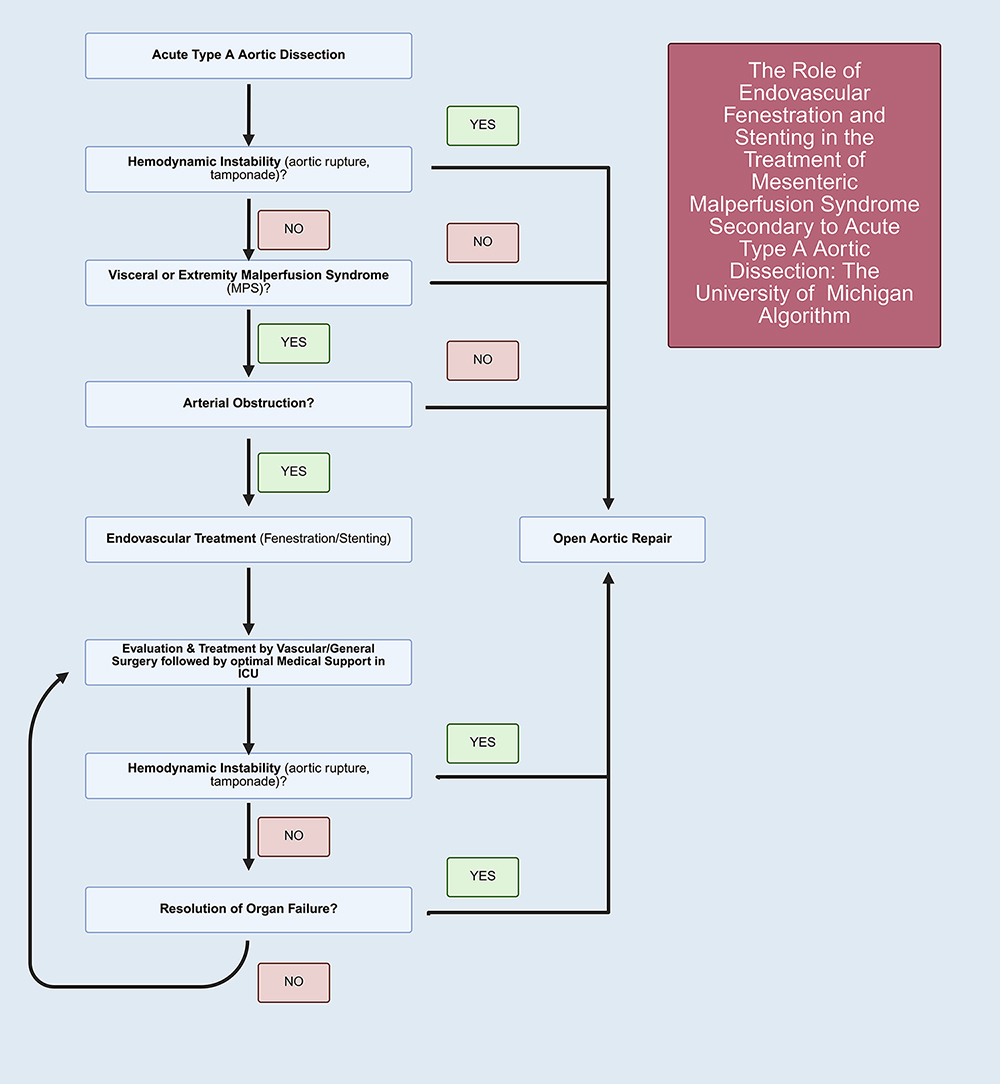 Fig. 2.
Fig. 2.
Algorithm for the treatment of mesenteric malperfusion syndrome during type A dissection at the University of Michigan [65]. At the University of Michigan, patients presenting with type A aortic dissection with mesenteric malperfusion syndrome, but without complications such as cardiac tamponade, aortic rupture, wide-open aortic insufficiency, or neurovascular malperfusion, are treated with upfront endovascular revascularization followed by delayed open aortic repair. This deviates from the traditional approach of upfront aortic repair. Created by BioRender.
Endovascular therapy has greatly improved outcomes in the treatment of traumatic aortic disease. The 2022 ACC/AHA guidelines give a level 1 recommendation in the treatment of traumatic pseudo-aneurysm or rupture and a 2A recommendation for intervening on intramural hematomas with high-risk imaging features. Furthermore, TEVAR is recommended over open repair in the treatment of thoracic aortic injury as a level 1 recommendation [8].
Analysis of the National Trauma Data Bank from 2007–2015 found 14,422 patients
diagnosed with blunt thoracic aortic injury (BTAI), comprising 0.3% of all
patients. Of those with BTAI, 3628 received intervention: 3226 received TEVAR
(87.9%) and 445 (12.1%) received open repair. Rate of open repair procedures
decreased from 7.4% to 1.9% during the study period, while the rate of TEVAR
usage increased from 12.1% to 25.7% during the same timeframe. On multi-variate
analysis, receipt of open repair over TEVAR significantly increased mortality
risk (OR: 1.63, 95% CI: 1.19–2.23, p
Endovascular therapy has also provided benefit in those afflicted with blunt abdominal aortic injury (BAAI). BAAI is a relatively rare occurrence. A retrospective analysis from the Western Trauma Association spanning from 1996 to 2011 identified 113 patients with BAAI (0.03% of all blunt trauma cases) from 12 major trauma centers. Of these, 40 cases (35.4%) underwent non-operative management and 3 cases resulted in failure of non-operative management. Recipients of non-operative management most often presented with lower grade aortic injuries. Forty-nine cases (43.4%), including all 30 patients who presented with aortic rupture, underwent OAR; mortality was 57.1% (28 cases). Recipients of endovascular therapy demonstrated no operative mortality when EVAR was the primary treatment means. While differences in injury grade preclude comparison of OAR and EVAR in the treatment of BAAI, these findings encourage the adoption of endovascular treatment in appropriately selected patients. Other endovascular modalities such as Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) have also been introduced as a means of hemorrhage control in the acute setting [69]. A comprehensive review of REBOA in the treatment of life-threatening hemorrhage from trauma is outside the scope of this overview, but recent data support that in-hospital survival is greater for patients undergoing REBOA than resuscitative thoracotomy for all injury patterns [70].
The application of endovascular therapy for aortic disease continues to evolve with ongoing technological advancements. Catheter-based platforms have revolutionized the treatment of aortic disease by expanding access to life-saving interventions while minimizing the morbidity associated with open surgery. Hence, an ‘endovascular first’ approach is utilized in the current clinical landscape for patients with appropriate anatomy. EVAR has demonstrated improved short-term outcomes across all patient risk strata in the elective setting. Additionally, due to ease of deployment, EVAR provides an expedient solution in the setting of rupture. Similarly, TEVAR has supplanted open repair in the treatment of descending thoracic aortic aneurysm both in the elective setting and during rupture. Lastly, TEVAR is recommended in the treatment of complicated Type B dissection and emerging data demonstrate its utility in improving aortic remodeling, possibly suggesting a benefit of TEVAR in the treatment of uncomplicated Type B AD. Endovascular therapy for the treatment of ascending aortic disease and aortic arch disease remains undefined and further exploration is needed, including more prospective data regarding long-term repair durability and aortic remodeling after endovascular treatment. This is especially true when considering the effect of selection bias on retrospective data comparing endovascular therapies to other treatment modalities. Overall, while more remains to be learned, endovascular therapy to date has been highly encouraging and highlights significant promise for the future.
AAA, abdominal aortic aneurysm; rAAA, ruptured abdominal aortic aneurysm; TAA, thoracic aortic aneurysm; rTAA, ruptured thoracic aortic aneurysm; AD, aortic dissection; EVAR, endovascular aortic repair; TEVAR, thoracic endovascular aortic repair; CA, Celiac Artery; SMA, superior mesenteric artery; REBOA, resuscitative endovascular balloon occlusion of the aorta; OAR, open aortic repair; BAAI, blunt abdominal aortic injury; BTAI, blunt thoracic aortic injury; TEE, transesophageal echocardiography; IR, interventional radiology; MMS, mesenteric malperfusion syndrome; BMT, best medical therapy; PMEG, physician modified endograft; IRB, institutional review board; IDE, investigator device exemption.
RP, SR, MK, JE, BY, and DMW all made substantial contributions to conception and design as well as acquisition and interpretation of data. RP, SR, MK, BY, JE, and DMW were involved in drafting the manuscript or reviewing it critically for important intellectual content. All authors gave final approval of the version to be published and take public responsibility for appropriate portions of the content and are accountable for all aspects of the work.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.