
 , Tae Hong Yoon 1, Jae Seok Jang 1, Jun Woo Cho 1,*
, Tae Hong Yoon 1, Jae Seok Jang 1, Jun Woo Cho 1,*
1 Department of Thoracic and Cardiovascular Surgery, Daegu Catholic University School of Medicine, 42472 Daegu, Republic of Korea
Abstract
Spontaneous coronary artery dissection (SCAD) is a rare, non-atherosclerotic cause of acute coronary syndrome, typically confined to the coronary arteries and managed conservatively.
We report a unique case of a 45-year-old man who presented with chest pain and syncope. Initial electrocardiography revealed ST-segment elevation, and imaging suggested aortic dissection. Emergency surgery revealed a hematoma in the sinus of Valsalva compressing the right coronary artery (RCA) ostium, caused by a SCAD extending beyond the coronary artery. The affected segment was resected, and coronary artery bypass grafting was performed. To our knowledge, this is the first reported case of SCAD extending into the sinus of Valsalva, mimicking an ascending aortic dissection. Although the angiographic appearance resembled type 1 SCAD, the anatomical pattern challenges existing classification.
This case highlights the need for heightened awareness of atypical SCAD presentations, consideration of conservative management when appropriate, and the importance of interdisciplinary collaboration in diagnosis and surgical planning.
Keywords
- spontaneous coronary artery dissection
- aortic dissection
- coronary artery bypass graft
Myocardial infarction is most commonly caused by atherosclerotic coronary artery disease. However, in rare cases, it can occur in the absence of significant atherosclerotic lesions [1, 2, 3], such as in spontaneous coronary artery dissection (SCAD)—a non-atherosclerotic, non-traumatic tear of the coronary artery wall [4, 5]. SCAD accounts for less than 1% of all myocardial infarctions and is typically diagnosed via coronary angiography [1, 4, 6], although intravascular ultrasonography (IVUS) or optical coherence tomography (OCT) may be necessary to confirm the diagnosis [5, 7].
Most SCAD cases are confined to the coronary arteries and can be successfully managed conservatively [7]. We present a rare case of SCAD that extended into the sinus of Valsalva and was initially misdiagnosed as an aortic dissection. This report discusses the diagnostic challenges and surgical management considerations based on our experience.
A 45-year-old man with no known medical history was referred to the emergency department with chest pain and a syncopal episode. The patient experienced a sudden onset of chest pain while playing badminton, radiating to both shoulders and the posterior neck. Approximately 30 minutes later, he developed dizziness and subsequently lost consciousness. He presented to a local hospital where electrocardiography (ECG) revealed ST-segment elevation, prompting his transfer for further evaluation.
His family history was significant for a paternal myocardial infarction. On
arrival, his vital signs were stable: blood pressure 130/70 mmHg, pulse rate 64
bpm, and body temperature 36 °C. He was alert and oriented. Laboratory
results showed normal cardiac enzyme levels (creatine kinase–myocardial band
(CK-MB)
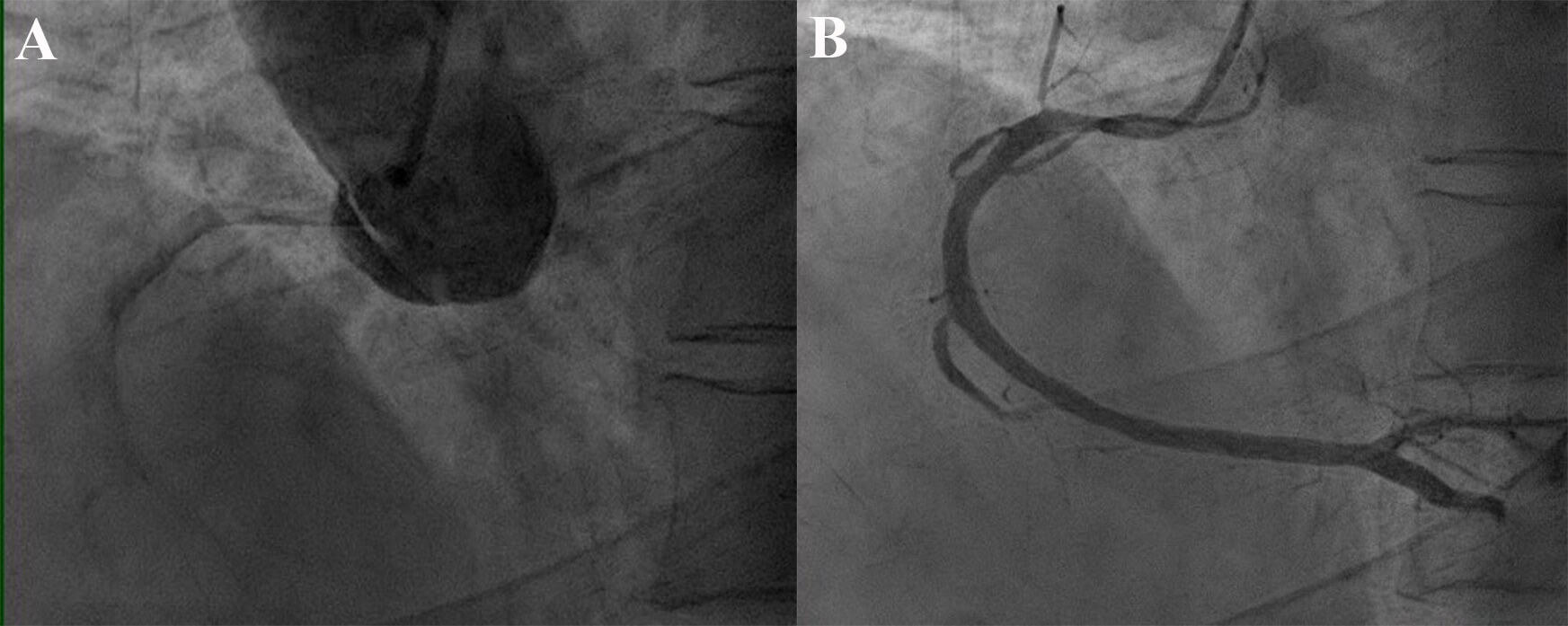
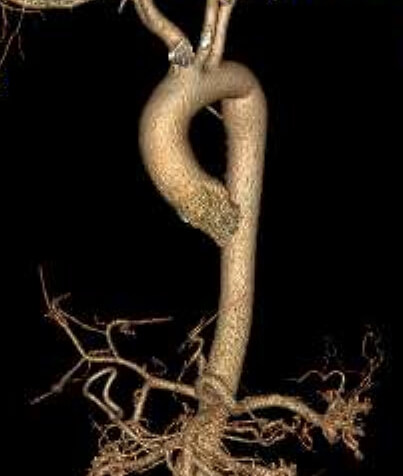
After administration of sublingual nitroglycerin, the patient’s chest pain resolved. However, persistent ST-segment elevation in the inferior leads on ECG necessitated emergent coronary angiography (CAG). The angiogram demonstrated a suspicious focal dissection of the ascending aorta (Fig. 1). Subsequent chest computed tomography (CT) did not provide definitive evidence of an aortic lesion (Fig. 2), although the possibility of aortic injury could not be completely excluded. Given the clinical suspicion, emergent thoracic aortic surgery was recommended.
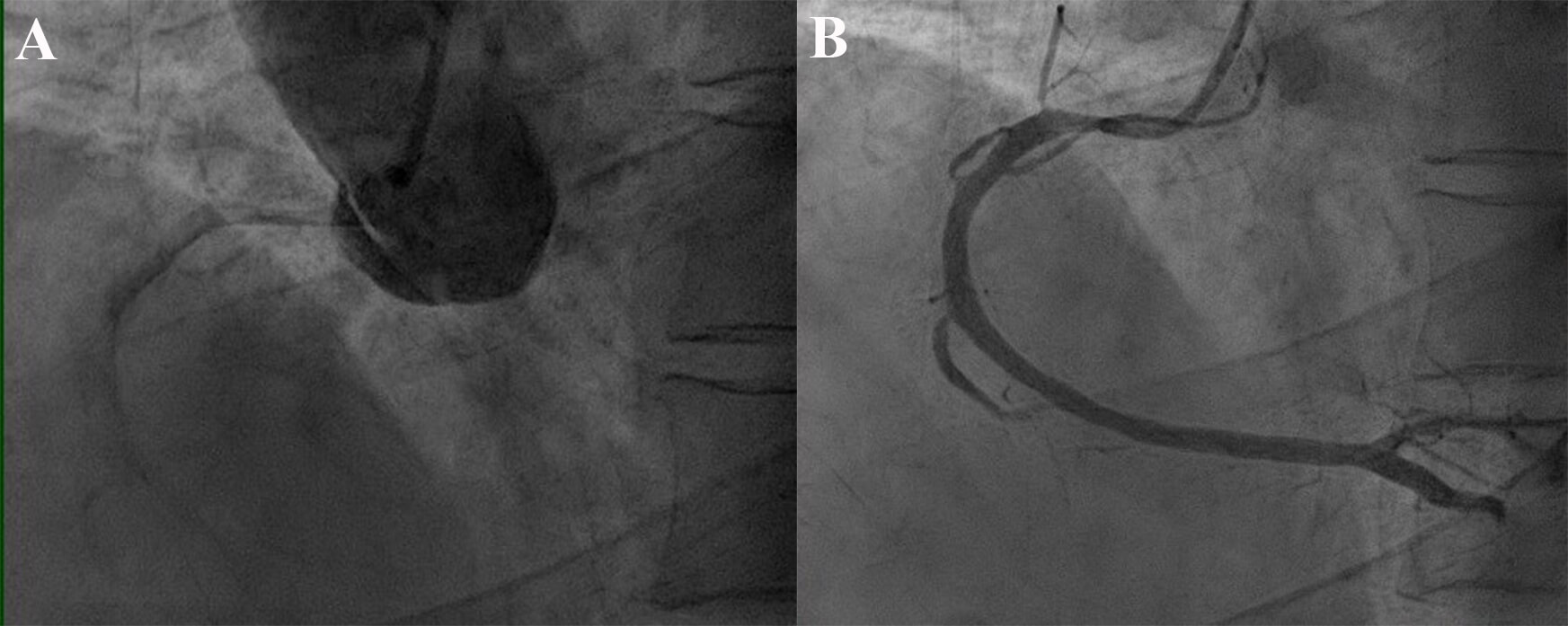 Fig. 1.
Fig. 1.
Coronary angiographic findings. (A) Preoperative coronary angiography showing a suspicious lesion at the sinus of Valsalva, suggestive of an aortic dissection. (B) Selective contrast injection into the right coronary artery (RCA) demonstrating narrowing at the RCA ostium with limited opacification, consistent with external compression.
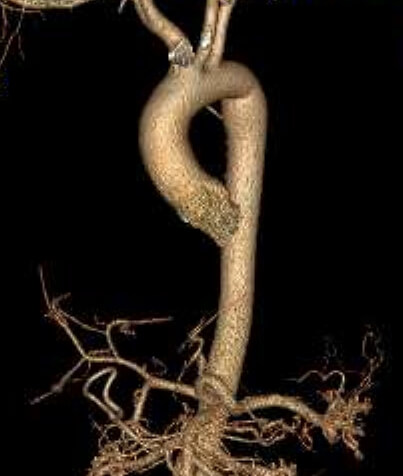 Fig. 2.
Fig. 2.
Three-dimensional computed tomography image showing no definitive lesion in the ascending aorta.
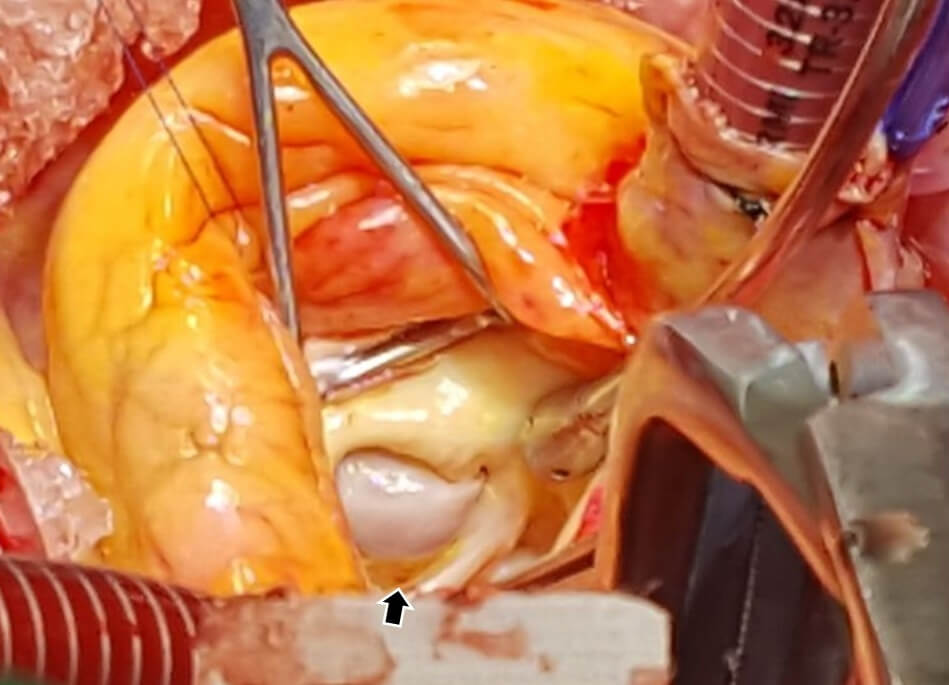
Through a median sternotomy, arterial cannulation was performed via the distal ascending aorta and right atrial appendage. Aortotomy revealed a large hematoma within the right coronary sinus of Valsalva, causing significant external compression of the right coronary artery (RCA) ostium (Fig. 3). The hematoma appeared to originate from a dissection of the proximal RCA that had extended into the aortic wall. This extension obliterated the RCA orifice, mimicking an ascending aortic dissection.
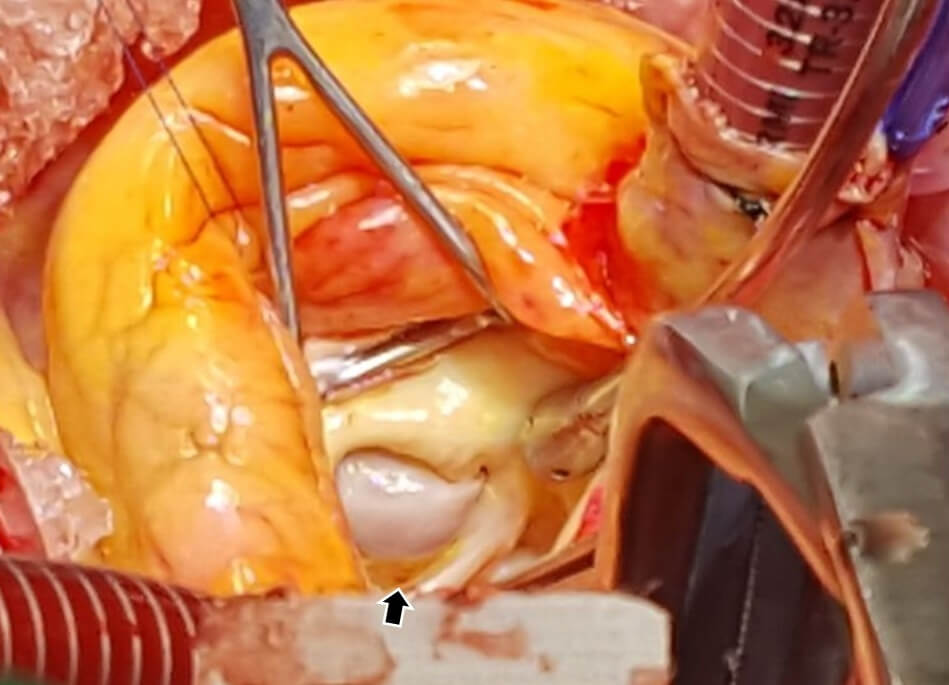 Fig. 3.
Fig. 3.
Intraoperative findings. Intraoperative findings: No intimal tear was observed in the aorta; however, a hematoma was identified within the wall of the sinus of Valsalva (black arrow).
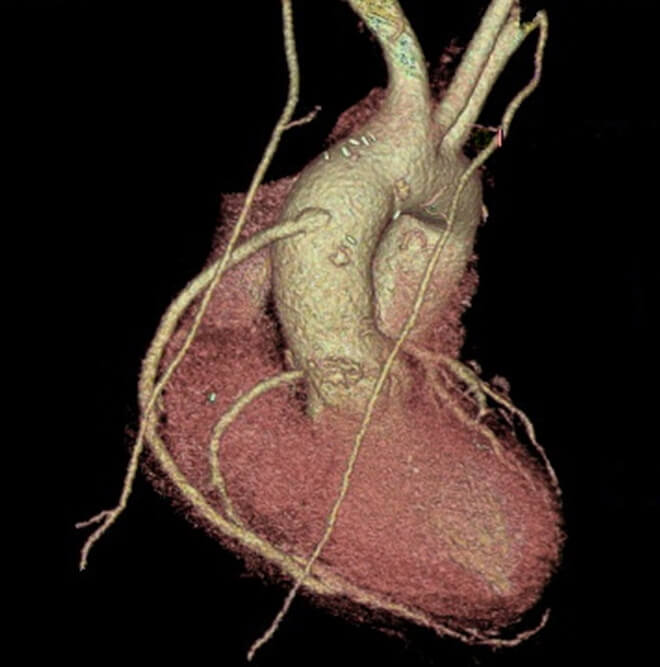
Further inspection revealed a clear intimal tear in the proximal RCA. The affected segment was resected at its proximal stump, and the wall defect was closed primarily. As the dissection extended to the mid-RCA, coronary artery bypass grafting (CABG) was performed using a saphenous vein graft to the intact posterior descending artery (Fig. 4).
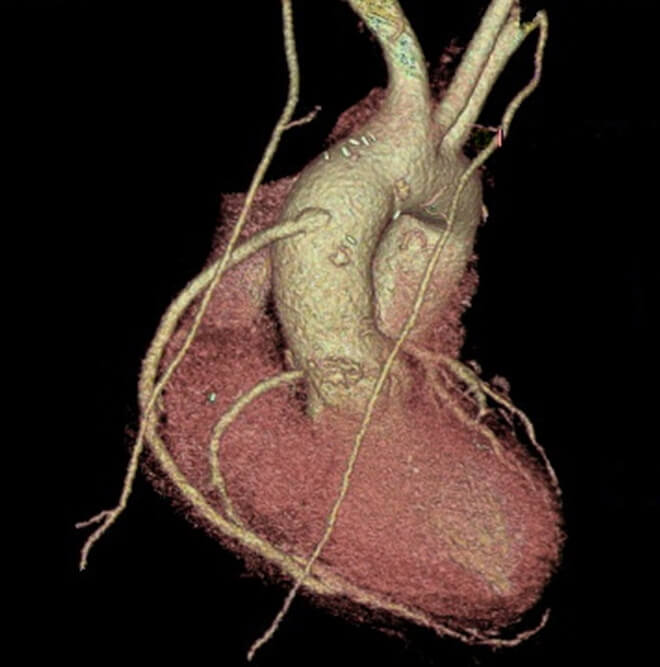 Fig. 4.
Fig. 4.
Postoperative cardiac computed tomography showing a patent saphenous vein graft to the RCA territory.
Postoperatively, the patient developed hypoxemia consistent with procedure-related acute respiratory distress syndrome, which was managed with high positive end-expiratory pressure. He was extubated on postoperative Day 3 and discharged on Day 12 without complications. Histopathological analysis of the resected coronary segment showed degenerative changes without features suggestive of vasculitis or connective tissue disease. The patient maintained wellness according to outpatient follow-ups.
SCAD is an increasingly recognized but often underdiagnosed cause of acute coronary syndrome, particularly in younger individuals without traditional cardiovascular risk factors [4, 5, 7]. Although most SCAD cases are confined to the coronary arteries [7, 8, 9, 10], this report describes an exceptionally rare anatomical presentation, and to the best of our knowledge, it is the first documented case of SCAD extending into the sinus of Valsalva. This extension led to angiographic and radiologic findings that mimicked ascending aortic dissection, necessitating emergent surgical intervention.
This unusual anatomical trajectory underscores a significant diagnostic challenge. When coronary angiography revealed a lesion localized to, or involving, the sinus of Valsalva—especially in the absence of classic features of aortic dissection—SCAD should be strongly considered in the differential diagnosis. In such cases, adjunctive imaging modalities such as OCT or IVUS may be crucial for confirming the diagnosis and differentiating SCAD from true aortic dissection. These advanced techniques provide high-resolution visualization of the coronary vessel wall and can detect intramural hematoma or false lumen formation—features that may be missed on conventional angiography or CT.
SCAD most frequently affects the left anterior descending artery, followed by the left circumflex artery, and less commonly the right coronary artery. Large observational studies have shown that the left anterior descending artery is involved in over 40% of cases, whereas only in 10–20% the right coronary artery is affected [2, 4, 5, 7]. Furthermore, SCAD exhibits a strong female predominance, with up to 90% of cases occurring in women—particularly during the peripartum period or in association with fibromuscular dysplasia [5].
SCAD pathogenesis is considered multifactorial, involving both predisposing arteriopathies and acute physical or emotional triggers. Two primary mechanisms have been proposed: (1) an intimal tear that allows blood to enter the vessel wall and form a false lumen; and (2) spontaneous hemorrhage from the vasa vasorum within the media, leading to an intramural hematoma that compresses the true lumen. Contributing factors such as fibromuscular dysplasia, connective tissue disorders, hormonal fluctuations, and systemic inflammatory diseases may compromise arterial wall integrity. Physical exertion or emotional stress may exacerbate shear forces, precipitating dissection in susceptible individuals [2, 4, 5, 7, 11].
In our case, although the patient was male and lacked identifiable connective tissue disease or hormonal risk factors, the dissection occurred during intense physical activity—a recognized precipitating factor due to its effect on coronary shear stress. The atypical extension of the dissection into the sinus of Valsalva may reflect structural vulnerability at the coronary–aortic junction, where the proximal right coronary artery merges into the aortic wall and is anchored by perivascular connective tissue at the aortic root. Mechanical stress, such as exertion or transient hypertension, may have propagated the intramural hematoma across this anatomical interface.
This lesion—exhibiting both coronary dissection and extramural hematoma—does not neatly conform to the existing Saw classification. Although a single case is insufficient to propose a new classification subtype, it raises the need to recognize such anatomical variants and consider refinements to current SCAD typologies to better encompass lesions that extend beyond the coronary arteries.
Despite the unusual extension into the aortic root, the angiographic appearance in our case resembled Type 1 SCAD per the Saw classification [12]. Type 1 SCAD is characterized by a pathognomonic angiographic appearance, including multiple radiolucent lumens resulting from an intimal tear that permits contrast flow into separate channels. However, given the dissection’s progression into the sinus of Valsalva and associated extramural hematoma formation, the lesion does not fully align with the existing classification criteria. This case represents an anatomically and pathophysiologically atypical variant that challenges the conventional typology of SCAD.
Although emergency surgery was undertaken to exclude a potentially fatal aortic dissection, this decision was made under considerable diagnostic uncertainty. Several clinical features—such as hemodynamic stability, resolution of chest pain following nitroglycerin administration, normal cardiac enzyme levels, and the absence of definitive aortic pathology on CT—could have supported a more conservative approach. However, the angiographic findings closely resembled an ascending aortic dissection. Given the potentially catastrophic consequences of a missed diagnosis, the multidisciplinary team proceeded with surgical exploration after careful deliberation.
In retrospect, greater recognition of the patient’s stability and the possibility of SCAD in the differential diagnosis might have supported a more conservative initial strategy. This underscores the importance of diagnostic vigilance in similar presentations.
A notable limitation in this case was the absence of intravascular imaging with IVUS or OCT, which precluded definitive characterization of the dissection plane. Due to the urgent clinical scenario and angiographic features suggestive of an ascending aortic dissection, there was insufficient time to perform intracoronary imaging prior to surgery. Histopathological examination later revealed nonspecific myxoid degeneration, with no evidence of vasculitis or connective tissue disease. Although these findings did not confirm a secondary etiology, they were also insufficient to definitively exclude one.
Comprehensive CT imaging of the carotid, thoracic, and abdominal arteries revealed no signs of fibromuscular dysplasia or other vascular abnormalities, and there were no phenotypic features suggestive of a heritable connective tissue disorder. Although further genetic testing was considered, the patient declined chromosomal studies due to cost constraints.
The surgical strategy also warrants reflection. When surgical revascularization is required in SCAD, saphenous vein grafts are generally preferred, as spontaneous healing of the native artery can result in competitive flow and subsequent graft failure [10, 11]. In this case, however, the RCA ostium was surgically obliterated, eliminating the risk of competitive flow. While the saphenous vein graft was chosen due to intraoperative urgency and availability, the use of the right internal mammary artery may have offered superior long-term patency. This case highlights the importance of individualized conduit selection in SCAD, particularly when the native anatomy is surgically modified.
Finally, this case underscores the critical role of interdisciplinary collaboration. SCAD remains underrecognized among both cardiologists [7, 13] and cardiovascular surgeons. Given its clinical overlap with emergent conditions such as aortic dissection, timely and effective communication among cardiology, cardiovascular surgery, and radiology teams is essential. Shared interpretation of imaging studies and a consensus-based assessment of diagnostic certainty are key to determining appropriate management.
We recommend considering conservative management in hemodynamically stable patients without ongoing ischemia, left main involvement, or radiologic evidence of dissection progression. Conversely, surgical intervention may be necessary in cases involving hemodynamic instability, refractory ischemia, left main dissection, or suspected extension into the ascending aorta. In stable patients, observation may be feasible, but the potential for rapid clinical deterioration necessitates close, collaborative decision-making. Ultimately, coordinated interdisciplinary care can prevent unnecessary surgical intervention while ensuring timely treatment when warranted, thereby improving patient outcomes.
Herein, we report the first documented case of spontaneous coronary artery dissection extending into the sinus of Valsalva, mimicking an aortic dissection. This case illustrates the diagnostic and therapeutic challenges posed by atypical SCAD, the value of intracoronary imaging before definitive surgery, and the need for thoughtful surgical planning—especially in selecting revascularization conduits. This experience may guide the management of similar cases and foster improved collaboration between cardiologists and cardiovascular surgeons.
Data sharing is not applicable to this article as no datasets were generated or analyzed.
CHL and JWC contributed to the conception and design of the work, and were involved in the patient’s clinical management and drafting of the manuscript. THY and JSJ assisted in data collection, literature review, and manuscript revision. JWC supervised the overall work and approved the final version of the manuscript. All authors read and approved the final manuscript and agreed to be accountable for all aspects of the work.
This study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was obtained from the Institutional Review Board of Daegu Catholic University Medical Center (DCUMC 2025-05-007). Informed consent was waived due to the retrospective nature of the study and the use of anonymized data.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/HSF49415.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.