

 , Ryuji Hojo 1, Kai Machida 1, Eiichi Teshima 1, Ryuji Tominaga 1
, Ryuji Hojo 1, Kai Machida 1, Eiichi Teshima 1, Ryuji Tominaga 11 Department of Cardiovascular Surgery, Fukuoka Wajiro Hospital, 811-0212 Higashi-ku, Fukuoka, Japan
Abstract
The optimal cannulation strategy for acute type A aortic dissection (ATAAD) remains controversial. Femoral artery, axillary artery, ascending aorta, or apical cannulation is used depending on the clinical scenario; however, no consensus on use has currently been established. Thus, this study aimed to compare the outcomes of femoral artery and central aortic cannulation.
This study retrospectively analyzed 92 patients who underwent emergency surgery for ATAAD between April 2023 and March 2025. Femoral artery cannulation was performed in 71 patients (77%), ascending aortic cannulation in 11 (12%), brachiocephalic in 6 (7%), and apical in 4 (4.3%).
Baseline characteristics did not differ significantly between the femoral and central aortic groups. Total arch replacement was performed more frequently in the femoral group (32%) than in the central aortic cannulation group (0%; p = 0.029). Postoperative stroke occurred in 2.8% of the individuals in the femoral group and 0% of the central aortic cannulation group. Similarly, 30-day mortality did not differ between the groups. The multivariate analysis did not identify any significant predictors of postoperative stroke. However, prolonged operative time was associated with 30-day mortality (odds ratio, 1.01; p = 0.00467). The time from skin incision to cardiopulmonary bypass initiation did not significantly affect patient outcomes.
Excluding cases at high risk of embolization due to retrograde perfusion, both ascending aortic and femoral cannulations can be safely utilized as arterial inflow sites. Therefore, tailoring the cannulation strategy to each patient is essential.
Keywords
- acute type A aortic dissection
- cannulation strategy
- femoral artery cannulation
- cerebral infarction
In surgery for acute type A aortic dissection (ATAAD), arterial cannulation is typically performed through the right axillary or femoral artery, or occasionally both [1, 2, 3]. The 2014 European Society of Cardiology Guidelines recommend the axillary artery as the first-choice cannulation site for ATAAD procedures [4]. Indeed, total aortic arch replacement (TAR) is widely regarded as a recommended option for ATAAD, with the right axillary and femoral arteries commonly adopted as the preferred arterial cannulation sites in current practice [5]. Several studies have raised concerns about the potentially increased risk of stroke associated with femoral artery cannulation [2, 6, 7]. More recently, direct cannulation of the ascending aorta has been reported as a viable alternative [8, 9]. However, no single cannulation site is ideal for all patients, and the choice remains a topic of ongoing debate.
Although several studies have compared the outcomes of central aortic cannulation (CAC), axillary artery cannulation (AXC), femoral artery cannulation (FAC), and apical cannulation (AC), postoperative complications such as stroke, death, and malperfusion of the abdomen or lower limbs have been reported across all strategies [2, 6, 7, 8, 10]. At our institution, we primarily use FAC. However, in patients with unfavorable distal aortic anatomy, including a mural thrombus, aneurysmal changes, or extensive calcification, brachiocephalic artery cannulation (BCAC), AXC, CAC, or AC is performed to avoid retrograde embolization. In emergency settings, the rapid initiation of cardiopulmonary bypass (CPB) is also critical, as delays may increase the risk of aortic rupture [11, 12].
We retrospectively analyzed 92 consecutive patients who underwent surgical treatment for ATAAD between April 2023 and March 2025. Emergency surgery was performed immediately after the diagnosis was confirmed using contrast-enhanced computed tomography (CT) of the chest and abdomen. Intraoperatively, arterial cannulation was guided by transesophageal echocardiography (TEE) or epiaortic ultrasonography. The cannulation sites included the femoral artery, brachiocephalic artery, ascending aorta, and apex of the left ventricle.
The primary aim of this study was to compare the outcomes of antegrade perfusion via CAC and retrograde perfusion via FAC. Due to the small number of cases, patients who underwent BCAC or AC were excluded from the comparative analysis.
The primary outcomes were 30-day mortality and incidence of postoperative
stroke. Organ malperfusion was defined on the basis of clinical symptoms and
preoperative contrast-enhanced CT findings indicating compromised blood flow.
Shock was defined as hypotension (systolic blood pressure
Stroke was categorized as dissection- or procedure-related. Dissection-related strokes were defined as preoperative neurological deficits such as impaired consciousness or hemiparesis. Procedure-related stroke was defined as new-onset stroke in patients without preoperative neurological symptoms. Stroke was included in both categories. When neurological abnormalities were observed, brain CT or magnetic resonance imaging was performed to diagnose cerebral infarction. However, asymptomatic cerebral infarctions cannot be diagnosed.
A standardized surgical protocol was applied to all patients, including rapid transfer to the operating room and immediate initiation of surgical repair [13, 14].
In all cases, except those involving apical cannulation, the ascending aorta was clamped before circulatory arrest and proximal anastomosis was performed. In patients undergoing hemiarch replacement (HAR) or TAR, the aorta was transected at the sinotubular junction level. The false lumen was obliterated using BioGlue® (CryoLife Inc, GA, USA), and the aortic wall was reinforced with inner and outer felt strips of polytetrafluoroethylene, secured with four 4-0 Prolene mattress sutures.
Aortic root replacement was performed in patients presenting annuloaortic ectasia or aortic root-entry tears. Patients with moderate to high aortic stenosis or regurgitation due to leaflet degeneration underwent valve replacement.
Distal aortic management was guided by preoperative CT or intraoperative findings. HAR was performed in cases where entry tears were confined to the ascending aorta, whereas TAR with a frozen elephant trunk (FET) was used in cases presenting arch or distal entry tears [15, 16]. In HAR, the aorta is transected just distal to the brachiocephalic artery and is reinforced with felt strips. In TAR, the aorta is divided into zone 2 just distal to the left common carotid artery. An FET was deployed, the outer layer was reinforced with felt, and the anastomosis was completed using a four-branch graft and continuous suturing with 4-0 polypropylene. The branches of the aortic arch were reconstructed using continuous 5-0 polypropylene continuous sutures.
Cerebral protection was achieved using deep hypothermic circulatory arrest (25 °C) and was monitored via bladder, rectal, and venous blood temperatures. In HAR procedures, retrograde cerebral perfusion was performed through the superior vena cava. In TAR procedures, selective antegrade cerebral perfusion was established after the aortic arch branches were transected.
The cannulation sites were selected based on the preoperative CT findings. Generally, FAC was the first choice. However, antegrade strategies (BCAC, CAC, or AC) have been used to minimize the embolic risk in patients with mural thrombus, aneurysmal changes, circumferential calcification, or a thrombosed false lumen descending to the abdominal aorta. Femoral cannulation was performed using the Seldinger technique with guidewire placement in the true lumen, as confirmed by TEE. For patients exhibiting limb malperfusion, perfusion was initiated on the ischemic side.
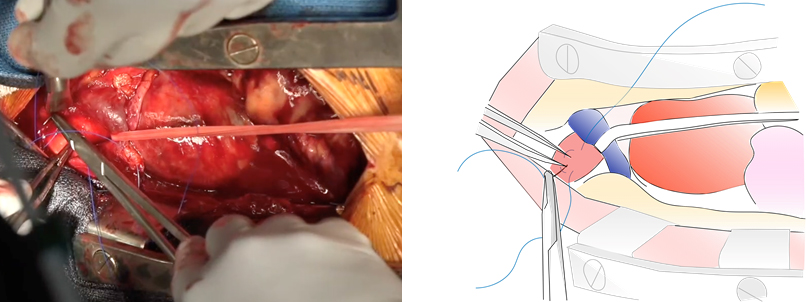
For BCAC procedures, the brachiocephalic artery was not dissected and direct cannulation (the so-called “Harutaro” technique) was performed after median sternotomy (Fig. 1, Ref. [17]). For CAC procedures, cannulation was performed at a site where the false lumen was thrombosed, and the aortic wall was sufficiently thick using the Seldinger technique under epiaortic echocardiographic guidance [18]. If no cannulation site was deemed safe, or in cases of preoperative cardiac arrest, apical cannulation was used. A purse-string suture with 4-0 polypropylene was placed at the apex, which was incised, and a cannula was inserted beyond the aortic valve.
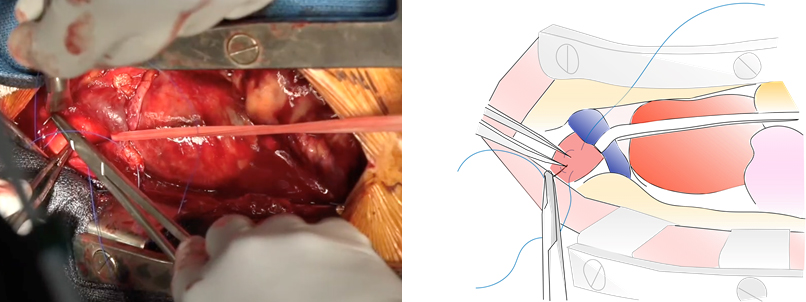 Fig. 1.
Fig. 1.
Direct cannulation of the brachiocephalic artery (Harutaro technique). The innominate vein is taped and retracted caudally, followed by a purse-string suture applied in one or two layers using 4-0 polypropylene [17].
In all cases, the absence of upper extremity hypotension and regional cerebral or lower limb oxygen desaturation was confirmed at the initiation of CPB. In one patient undergoing FAC, however, upper-extremity hypotension and cerebral desaturation developed after aortic cross-clamping and were resolved with supplementary inflow through the brachiocephalic artery.
All data were retrospectively collected from medical records. Categorical
variables were compared using the chi-square test or Fisher’s exact test, and
continuous variables were analyzed using the Student’s t-test. Data were
expressed as medians and interquartile ranges and were compared using the
Mann–Whitney U test. Multivariate logistic regression was used to identify
independent predictors of 30-day mortality and postoperative stroke. Statistical
significance was set at p
All statistical analyses were performed using EZR v4.4.2 (Saitama Medical Center, Jichi Medical University, Saitama, Japan), a graphical user interface for R 4.0 (R Foundation for Statistical Computing, Vienna, Austria) [19].
Of the 92 patients who underwent surgery for ATAAD, FAC was performed in 71 patients (77%), CAC in 11 patients (12%), BCAC in six patients (7%), and AC in four patients (4%). The baseline characteristics of the patients are summarized in Table 1.
| Cannulation site | ||||
| Femoral (n = 71) | Aortic (n = 11) | Brachiocephalic (n = 6) | Apex (n = 4) | |
| Age, year | 70 |
76 |
74 |
66 |
| Male sex | 26 (37) | 4 (36) | 3 (50) | 4 (100) |
| Hypertension | 51 (72) | 11 (100) | 4 (67) | 4 (100) |
| Hyperlipidemia | 10 (14) | 4 (36) | 2 (33) | 1 (25) |
| Diabetes mellitus | 6 (8) | 0 (0) | 2 (33) | 0 (0) |
| Chronic renal failure | 3 (4) | 0 (0) | 0 (0) | 0 (0) |
| COPD | 4 (6) | 0 (0) | 1 (17) | 0 (0) |
| Coronary artery disease | 4 (6) | 0 (0) | 0 (0) | 0 (0) |
Values are n (%) or mean
The preoperative clinical characteristics of the patients are shown in Table 2. In patients presenting with cardiopulmonary arrest, direct cannulation via the BCAC or the apex (AC) was preferred over Seldinger-based techniques such as FAC or CAC. A moderate or high aortic regurgitation (AR) was significantly more common in the CAC group than in the FAC group (Table 3).
| Cannulation site | |||||
| Femoral (n = 71) | Aortic (n = 11) | Brachiocephalic (n = 6) | Apex (n = 4) | ||
| CPA | 0 (0) | 0 (0) | 1 (17) | 1 (25) | |
| Shock | 13 (18) | 3 (27) | 0 (0) | 0 (0) | |
| Tamponade | 14 (20) | 5 (45) | 3 (50) | 0 (0) | |
| Moderate to severe AR | 10 (14) | 5 (45) | 2 (33) | 1 (25) | |
| Any organ malperfusion | 29 (41) | 3 (27) | 1 (17) | 2 (50) | |
| Stroke with vessel involvement | 14 (19) | 1 (9) | 0 (0) | 1 (25) | |
| Dissection extension | |||||
| Limited, proximal dissection | 13 (18) | 4 (36) | 2 (33) | 0 (0) | |
| Arch vessels dissection | 42 (59) | 5 (45) | 2 (33) | 4 (100) | |
| One iliac artery | 18 (25) | 1 (9) | 1 (17) | 0 (0) | |
| Both iliac arteries | 14 (20) | 2 (18) | 0 (0) | 0 (0) | |
| Entry site | |||||
| Ascending aorta | 50 (70) | 9 (82) | 4 (67) | 1 (25) | |
| Aortic arch | 13 (18) | 0 (0) | 2 (33) | 3 (75) | |
Values are n (%) except where otherwise noted. CPA, Cardiopulmonary arrest; AR, aortic regurgitation.
| Cannulation site | ||||
| Femoral (n = 71) | Aortic (n = 11) | p value | ||
| CPA | 0 (0) | 0 (0) | - | |
| Shock | 13 (18.31) | 3 (27.27) | 0.442 | |
| Tamponade | 14 (19.72) | 5 (45.45) | 0.116 | |
| Moderate to severe AR | 10 (14.08) | 5 (45.45) | 0.025 | |
| Any organ malperfusion | 29 (40.84) | 3 (27.27) | 0.390 | |
| Stroke with vessel involvement | 14 (19.72) | 1 (9.09) | 0.680 | |
| Dissection extension | ||||
| Limited, proximal dissection | 13 (18.31) | 4 (36.36) | 0.169 | |
| Arch vessels dissection | 42 (59.15) | 5 (45.45) | 0.392 | |
| One iliac artery | 18 (25.35) | 1 (9.09) | 0.234 | |
| Both iliac arteries | 14 (19.72) | 2 (18.18) | 0.904 | |
| Entry site | ||||
| Ascending aorta | 50 (70.42) | 9 (81.82) | 0.433 | |
| Aortic arch | 13 (18.31) | 0 (0) | 0.198 | |
Values are n (%) except where otherwise noted. CPA, Cardiopulmonary arrest; AR, aortic regurgitation.
All interventions performed on 82 patients included in the FAC vs. CAC analysis were performed by a single surgeon at the Fukuoka Wajiro Hospital. The operative data are summarized in Table 4. There were no significant differences in the proximal aortic procedures between the groups. However, TAR was significantly more frequent in the FAC group, likely accounting for the longer operative time observed in this group. Importantly, no significant difference in the time from skin incision to CPB establishment was observed between the two groups. The duration of circulatory arrest was also comparable between the groups.
| Cannulation site | ||||
| Femoral (n = 71) | Aortic (n = 11) | p value | ||
| Operative times | ||||
| Skin incision time, min | 173 (140–237) | 147 (116–166) | 0.018 | |
| Time to CPB, min | 16 (13–18) | 16 (14–18) | 0.748 | |
| CPB time, min | 93 (77–149) | 80 (70–98) | 0.074 | |
| ACC time, min | 78 (58–116) | 65 (53–73) | 0.034 | |
| HCA time, min | 25 (20–36) | 21 (19–30) | 0.198 | |
| Proximal repair | ||||
| Root replacement* | 5 (7) | 0 (0) | 1.000 | |
| AVR | 5 (7) | 1 (9) | 1.000 | |
| Distal repair | ||||
| Hemiarch replacement | 48 (68) | 11 (100) | 0.029 | |
| Total arch replacement | 23 (32) | 0 (0) | ||
Values are n (%) or median (first quartile-third quartile) except where
otherwise noted. Bold indicates significant results (p
CPB, Cardiopulmonary bypass; ACC, Aortic cross clamp; HCA, hypothermic circulatory arrest; AVR, aortic valve replacement.
*root replacement includes Bentall procedure or valve sparing root replacement.
The postoperative complications, including procedure-related stroke and 30-day mortality, are shown in Table 5. No statistically significant differences were observed between the groups for either outcome. The median postoperative hospital stay was 22 days in both groups.
| Cannulation site | ||||
| Femoral (n = 71) | Aortic (n = 11) | p value | ||
| Overall stroke | 13 (18.31) | 1 (9.09) | 0.680 | |
| Dissection-related stroke | 11 (15.49) | 1 (9.09) | 0.919 | |
| Procedure-related stroke | 2 (2.82) | 0 (0) | 1.000 | |
| In-hospital stay, day | 22 (14–32) | 22 (18–29) | 0.723 | |
| 30 days mortality | 10 (14.08) | 0 (0) | 0.404 | |
Values are n (%) or median (first quartile-third quartile) except where
otherwise noted. Bold indicates significant results (p
Multivariate logistic regression analyses were performed to identify factors associated with procedure-related stroke and 30-day mortality. The factors related to procedure-related stroke are listed in Table 6. Variables such as age, sex, surgical procedure, presence of aortic arch branch dissection, FAC, CPB time, and circulatory arrest time were also examined. Dissection involving the aortic arch branches may pose a risk for procedure-related stroke; however, femoral artery cannulation was not associated with a significant increase in this risk.
| Variable | OR (95% CI) | p value |
| Male sex | 0.33 (0.063–1.73) | 0.190 |
| Age | 1.00 (0.940–1.73) | 0.917 |
| Arch vessel dissection | 15.8 (1.690–148.00) | 0.016 |
| Femoral artery cannulation | 1.06 (0.096–11.60) | 0.964 |
| Total arch replacement | 1.02 (0.097–10.80) | 0.985 |
| CPB time | 1.01 (0.980–1.03) | 0.623 |
| HCA time | 1.02 (0.890–1.16) | 0.793 |
Bold indicates significant results (p
As shown in Table 7, no significant associations were found between age, sex, preoperative malperfusion, and 30-day mortality. However, longer operative time was a significant predictor of 30-day mortality (odds ratio, 1.01; p = 0.00467).
| Variable | OR (95% CI) | p value |
| Male sex | 0.16 (0.142–1.79) | 0.137 |
| Age | 0.94 (0.845–1.05) | 0.263 |
| Any organ malperfusion | 0.26 (0.264–24.90) | 0.417 |
| Time to CPB | 1.00 (0.899–1.12) | 0.944 |
| ACC time | 1.01 (0.996–1.03) | 0.130 |
| Skin incision time | 1.01 (1.000–1.03) | 0.00467 |
Bold indicates significant results (p
The primary objective of this study was to investigate the impact of antegrade and retrograde perfusion on postoperative stroke and mortality rates during the surgical management of ATAAD. Retrograde perfusion via FAC carries theoretical risks such as distal embolization from atherosclerotic plaques in the descending aorta, increased false lumen pressure through re-entries leading to true lumen collapse, and dislodgement of mural thrombi into arch vessels or entry sites [20]. These risks are particularly concerning in patients requiring a TAR, in which the primary entry point is located distal to the aortic arch. Nonetheless, our study did not show a higher incidence of stroke or mortality in the FAC group compared to the CAC group. This may be because we avoid FAC in patients with high-risk descending aortic conditions, such as mural thrombus, aneurysm, circumferential calcification, or thrombosed false lumen, and instead prefer antegrade approaches like CAC, BCAC, or AC.
The benefits of antegrade perfusion provided by CAC include prompt establishment of CPB after sternotomy, prevention of dissection propagation, avoidance of retrograde cerebral embolization and peripheral arterial injury, as well as improved neurological outcomes [21, 22]. However, few studies have concluded that CAC is associated with better outcomes in terms of stroke and mortality than FAC. Klotz et al. [7] compared 127 cases of CAC with 108 cases of FAC and reported new postoperative stroke rates of 8.7% in the central group and 5.6% in the femoral groups (p = 0.449). The 30-day mortality rates were 20.2% and 16.9%, respectively (p = 0.699). In the study by Klotz et al. [7], the cannulation site was selected at the discretion of the surgeon without any defined criteria.
Wang et al. [23] investigated cannulation strategies in DeBakey type I
dissections, including AXC, FAC, and dual-arterial cannulation (DAC: a
combination of AXC and FAC). The incidence of postoperative stroke was 6.0% in
the FAC group and 2.7% in the AXC group (p = 0.02). Notably, DAC was
associated with a higher stroke rate (6.9%) than AXC alone (2.5%; p
Recent studies have reported postoperative stroke rates ranging from 2.2% to 6% when an optimal cannulation strategy is employed [7, 18, 20, 23, 24]. In our study, the new-onset stroke rate in the FAC group was 2.8%, which compares favorably to previous reports. This may reflect our institutional practice of avoiding FAC in patients with poor distal aortic morphology or in those who are at a high risk of thromboembolism.
Liang et al. [24] also found no significant reduction in stroke or
30-day mortality between DAC and single-site cannulation. However, in a subgroup
analysis of patients with CPB times exceeding 180 min, DAC was associated with
improved survival compared to both axillary (HR: 0.35, 95% CI: 0.14–0.90,
p = 0.029) and femoral cannulation (HR: 0.38, 95% CI: 0.14–1.03,
p = 0.058). Although DAC interventions are considered to provide
adequate systemic perfusion, reports on their effectiveness are limited [25, 26].
In our study, none of the patients experienced a CPB time of
Axillary or brachiocephalic cannulation often involves graft interposition, which can delay the initiation of CPB. This delay may increase the risk of malperfusion and aortic rupture. Norton et al. [27] reported median times from skin incision to CPB of 41 min for CAC and 85 min for arch vessel cannulation, with similar stroke (5.6% vs. 5.2 %) and mortality rates.
Patients with cardiac tamponade more often required arch vessel cannulation, likely because CAC is difficult to perform during hemodynamic instability. In these cases, gradual tamponade decompression followed by FAC or AXC is usually preferred. In our cohort, 45% of patients undergoing CAC presented with cardiac tamponade, and cardiopulmonary bypass was not started via peripheral cannulation beforehand. Instead, careful blood pressure control by the anesthesiologist and close teamwork with the surgical staff were crucial. At our institution, direct brachiocephalic cannulation, referred to as ‘Harutaro’ cannulation, is performed in selected cases where the arch vessels are free of dissection [17]. Additionally, recent reports have described the “Samurai” technique, in which the ascending aorta is directly incised and cannulated into the true lumen. However, this approach did not demonstrate significant improvements in mortality or stroke rates [28, 29].
Postoperative stroke risk is influenced by a complex interplay of anatomical and procedural factors, including vessel morphology, entry and re-entry sites, and the presence of a thrombosed false lumen. A more detailed understanding of these elements may help to refine cannulation strategies to improve patient-specific outcomes.
This study has some limitations that should be acknowledged. First, as a retrospective analysis, the lack of randomization may have introduced selection bias. Although propensity score matching may have reduced confounding factors, the sample size was insufficient to allow meaningful post-matching comparisons. Furthermore, in acute aortic dissection, numerous immeasurable factors, such as intraoperative hemodynamics or subtle anatomical variations, may influence outcomes beyond those captured by baseline characteristics. Second, this was a single-center study, which may limit the generalizability of the findings. All surgical interventions were performed by a single surgeon and operator-specific techniques may have affected the outcomes. Third, as previously noted, neurological assessments in retrospective studies are often incomplete [30]. In our study, postoperative brain imaging was not routinely performed, and stroke was diagnosed only in patients with overt neurological deficits. Additionally, the study period was relatively recent, so long-term follow-up data were unavailable.
No universally optimal cannulation strategy is currently available for ATAAD. In many cases, this choice must be made quickly, under time constraints, and often with limited available data. When chosen appropriately, femoral artery cannulation does not inherently worsen the prognosis. The cannulation strategy should be tailored to each patient, taking into account the relative advantages and disadvantages of each method and the experience of the surgical team.
Data to support the findings of this study are available on reasonable requests from the corresponding author.
YM designed the research study and wrote the manuscript. YM and ET performed the research and analyzed the data. Data collection and coordination were handled by RH and KM. Final guidance and designwas provided by RT. All authors participated in the critical revision of the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was carried out in accordance with the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Fukuoka Wajiro Hospital (Protocol No. 00245). All informed consent was obtained through an opt-out procedure with the IRB approval. We followed all relevant guidelines and regulations during the study.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.