

 , Abudar A. Al-Ganadi 1, Mahdi A. Kadry 1, Tarq Noman 2, Naseem Al-Wsabi 1
, Abudar A. Al-Ganadi 1, Mahdi A. Kadry 1, Tarq Noman 2, Naseem Al-Wsabi 11 Department of Cardiovascular Surgery, Cardiovascular and Kidney Transplantation Center, Taiz University Faculty of Medicine, 96704 Taiz, Yemen
2 Department of Cardiovascular Surgery, Sana’a University Faculty of Medicine, 96701 Sana’a, Yemen
Abstract
Atrial fibrillation (AF) is a common complication following cardiac surgery, particularly in populations undergoing complex cardiac procedures. This randomized clinical trial aimed to evaluate the effectiveness of posterior pericardiotomy (PP) in preventing postoperative atrial fibrillation (POAF) in a Yemeni cardiac surgical population.
This prospective, single-center, randomized clinical trial conducted in Yemen enrolled 210 patients undergoing open-heart surgery involving coronary artery bypass grafting (CABG), aortic valve replacement, ascending aortic surgery, or a combination of these procedures. Patients were randomized using sealed opaque envelopes into either the PP group (n = 106), in which a posterior left pericardiotomy was performed, or the control group (n = 104), which received standard care without pericardiotomy.
A total of 436 patients were screened between January 1, 2022, and June 30, 2024, and 210 were randomized. The median age was 60 years (interquartile range (IQR) 50–65), with 165 males (78.5%) and 45 females (21.5%). The incidence of POAF was significantly lower in the PP group compared to the control group (8.5% vs. 22.1%; p = 0.006). Cardiac tamponade occurred exclusively in the control group (n = 10). The PP group also demonstrated significantly shorter mechanical ventilation time (p < 0.001) and intensive care unit (ICU) stay (p = 0.004). In-hospital mortality was significantly lower in the PP group compared to the control group (p = 0.067).
Our findings reinforce the evidence supporting PP as a simple, low-cost adjunct to cardiac surgery. Thus, PP may improve postoperative recovery and resource utilization by reducing POAF, pericardial effusion, and tamponade, particularly in resource-limited settings such as Yemen.
NCT07266935, https://clinicaltrials.gov/study/NCT07266935.
Keywords
- posterior pericardiotomy
- postoperative atrial fibrillation
- cardiac surgery
- cardiac tamponade
- randomized controlled trial
- Yemen
Postoperative atrial fibrillation (POAF) is one of the most frequent arrhythmic complications following cardiac surgery, with an incidence ranging from 30% to 40% depending on procedure type and assessment methodology [1]. POAF has been associated with both early and late adverse outcomes, including increased mortality, heightened risk of stroke, prolonged hospitalization, and elevated healthcare costs [2, 3].
Pericardial effusion, particularly of small to moderate volume, is another common postoperative finding [4]. Echocardiographic studies have demonstrated its occurrence in more than two-thirds of patients after cardiac surgery [4, 5]. In this context, posterior pericardiotomy (PP) represents a simple yet effective surgical technique. By creating a communication between the posterior pericardial sac and the left pleural space, PP facilitates continuous drainage of pericardial fluid and thrombi during the early postoperative period [6].
Several studies have investigated the association between PP and POAF incidence, with some reporting significant reductions in POAF, while others showed inconsistent findings [7, 8, 9]. Nevertheless, multiple randomized controlled trials (RCTs) and recent meta-analyses have confirmed a statistically significant decrease in POAF incidence among patients undergoing PP [10, 11, 12].
Despite its documented benefits and favourable safety profile, PP remains underutilized in routine cardiac surgical practice. To address this gap and provide further evidence, we conducted a randomized controlled trial assessing the efficacy of PP in reducing POAF among patients undergoing coronary artery bypass grafting (CABG), aortic valve replacement (AVR), ascending aortic surgery, or a combination of these procedures. This study also represents the first randomized trial addressing this topic within a Yemeni cardiac surgical population.
This prospective, single-center, randomized controlled trial was conducted in the Department of Cardiovascular Surgery, Cardiovascular and Kidney Transplantation Center, Taiz, Yemen, between January 2022 and June 2024.
The study followed the principles of the Declaration of Helsinki. Approval was obtained from the ethical approval was obtained from the Research Ethics Committee of the Cardiovascular and Kidney Transplantation Centre, Taiz University, Yemen (Approval ID 0030425, dated December 20, 2021), and written informed consent was collected from all participants prior to enrollment. The trial is registered with ClinicalTrials.gov (Identifier: NCT07266935).
Patients aged
Exclusion criteria included: (1) previous cardiac or thoracic surgery, (2)
left-sided pleural adhesions, (3) preoperative atrial fibrillation or other
rhythm disorders, (4) hyperthyroidism, (5) renal failure with plasma creatinine
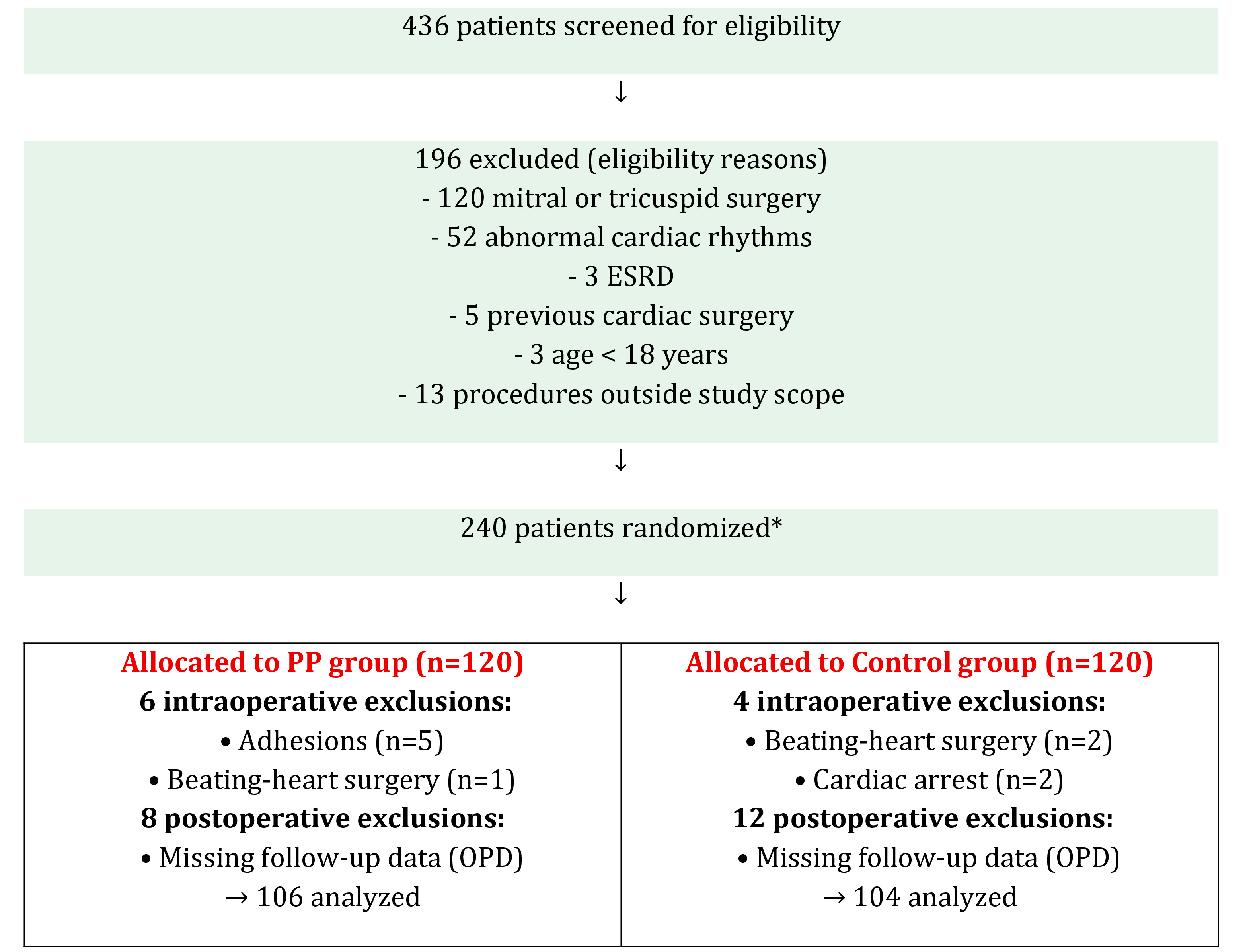
Patients were randomized in a 1:1 ratio to the PP group or the control group using sealed, opaque envelopes prepared by an independent staff member not involved in clinical care. A total of 106 patients were assigned to the PP group, and 104 patients to the control group (Fig. 1).
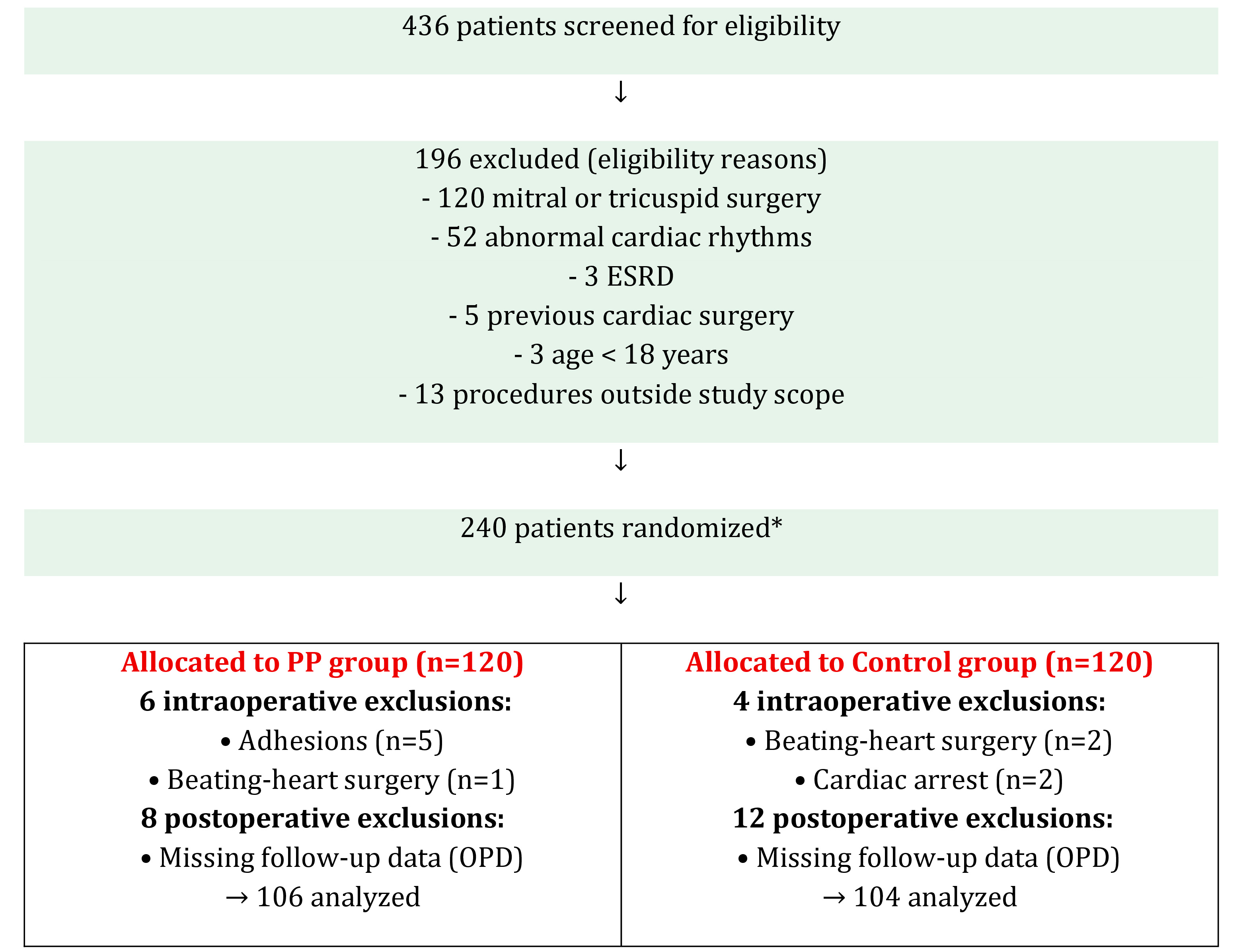 Fig. 1.
Fig. 1.
Trial CONSORT flow diagram. PP, Posterior pericardiotomy; OPD, outpatient clinic; POD, postoperative day. *Randomization: sealed, opaque envelopes prepared by an independent assistant not involved in patient care.
The trial followed a single-blind design: investigators responsible for data collection and outcome assessment were blinded to group allocation throughout the perioperative and postoperative periods.
All procedures were carried out through a median sternotomy. Prior to initiation
of cardiopulmonary bypass (CPB), patients were anticoagulated with intravenous
heparin (3 mg/kg) to achieve an activated clotting time (ACT)
PP was performed according to the operative procedure. In CABG, it was created after completion of distal vein grafts but before the internal mammary artery–LAD anastomosis. In valve or combined surgeries, PP was carried out after valve excision. The incision measured 4–5 cm, oriented longitudinally and positioned parallel and posterior to the left phrenic nerve, extending from the left inferior pulmonary vein to the diaphragm [11, 14]. Any complications during the procedure were recorded.
Chest drainage was standardized in all patients. A 28 Fr tube was inserted into the left pleural cavity and a 32 Fr tube into the anterior mediastinum. The pleural tube was introduced through a separate pleural opening and directed to the lower pleural space. If the right pleura was inadvertently opened, the mediastinal drain was passed through it before being positioned retrosternal. In all cases, the anterior pericardium was left open, and posterior placement of tubes near the heart was avoided to minimize arrhythmic risk.
After surgery, patients were transferred to the intensive care unit (ICU). Chest
drains were regularly milked and stripped to maintain patency, with
low-intermittent suction (–20 cmH2O) applied. Drainage was measured hourly,
and tubes were removed on the second postoperative day once output had fallen
below 100 mL in 24 hours. Standard prophylaxis with
Cardiac rhythm was continuously monitored by electrocardiography for the first
three postoperative days. Monitoring was resumed whenever arrhythmia was
suspected, when heart rate changes were observed, or if patients experienced
palpitations. Electrolytes were corrected as needed, with potassium maintained
above 4.5 mmol/L and magnesium above 1.0 mmol/L. Two-dimensional echocardiography
was performed on days 3 and 5, before discharge, and again during follow-up to
evaluate pericardial effusion. An effusion
• Primary endpoint: occurrence of POAF was defined as atrial fibrillation documented by a 12-lead electrocardiogram or continuous telemetry monitoring, lasting more than 30 seconds, and occurring after cardiac surgery in patients with no prior history of atrial fibrillation [15, 16].
• Secondary endpoints: requirement for antiarrhythmic medications, systemic anticoagulation, or cardioversion; development of pericardial or pleural effusion, cardiac tamponade, or need for reexploration; duration of ventilation (hours under mechanical ventilation until extubation); ICU stay (defined as total time in hours from ICU admission until until transfer to the ward); total hospital stay (days from surgery to discharge); in-hospital mortality; and major adverse cardiovascular events (stroke, myocardial infarction, or all-cause mortality).
• Pulmonary complications included pneumonia, prolonged ventilation (
All analyses followed the intention-to-treat (ITT) principle. A per-protocol (PP) analysis was also performed for sensitivity.
Sample size was calculated assuming a 25% incidence of POAF in controls and a
10% incidence in the PP group, based on prior literature [11, 17]. With
The baseline variables listed in Table 1 (including demographic characteristics, comorbidities, and preoperative laboratory and echocardiographic findings). These variables were chosen based on established predictors of POAF in the literature [1, 2, 3]. Postoperative outcomes, such as pericardial effusion, cardiac tamponade, pleural effusion, re-exploration, hospital mortality, and other adverse events, were screened during hospitalization and 30 days post operative follow-up. Data collection was performed prospectively, with preoperative variables assessed before surgery, intraoperative variables recorded during surgery, and postoperative variables monitored until discharge and at follow-up for 30 days postoperatively.
| Variable | Overall (n = 210) | PP group (n = 106) | Control group (n = 104) | p-value |
| Age, years (median, IQR) | 60 (50–65) | 60 (50–65) | 60 (50–65) | 0.546 |
| Male sex, n (%) | 165 (78.5) | 88 (83.0) | 77 (74.0) | 0.113 |
| Female sex, n (%) | 45 (21.5) | 18 (17.0) | 27 (26.0) | |
| Hypertension, n (%) | 106 (50.5) | 54 (50.9) | 52 (50.0) | 0.891 |
| Diabetes mellitus, n (%) | 89 (42.4) | 49 (46.2) | 40 (38.5) | 0.255 |
| Current/recent smoker, n (%) | 61 (29.0) | 31 (29.2) | 30 (28.8) | 0.949 |
| COPD, n (%) | 13 (6.2) | 6 (5.7) | 7 (6.7) | 0.748 |
| PAD*, n (%) | 4 (1.9) | 2 (1.9) | 2 (1.9) | 1.000 |
| Prior MI, n (%) | 153 (72.9) | 82 (77.4) | 71 (68.3) | 0.139 |
| Prior stroke/TIA, n (%) | 13 (6.2) | 9 (8.5) | 4 (3.8) | 0.163 |
| CHF (NYHA II–IV), n (%) | 89 (42.4) | 48 (45.3) | 41 (39.4) | 0.390 |
| Haematocrit, % (median, IQR) | 38.9 (35.4–40.8) | 38.9 (35.7–41.0) | 38.8 (35.0–40.0) | 0.690 |
| Creatinine, mg/dL (median, IQR) | 1.0 (0.8–1.1) | 0.9 (0.8–1.1) | 1.0 (0.8–1.1) | 0.460 |
| LVEF, % (median, IQR) | 51 (43–60) | 50 (41.7–55.5) | 54 (45–61) | 0.022 |
| LA size, cm (median, IQR) | 4.0 (3.5–4.2) | 4.0 (3.5–4.2) | 3.7 (3.3–4.2) | 0.022 |
| CABG, n (%) | 175 (83.3) | 87 (82.1) | 88 (84.6) | 0.432 |
| Aortic valve/ascending aorta, n (%) | 18 (8.6) | 8 (7.5) | 10 (9.6) | |
| CABG + aortic procedure, n (%) | 17 (8.1) | 11 (10.4) | 6 (5.8) | |
| No. of grafts (mean |
3.23 |
3.30 |
3.14 |
0.125 |
| Cross-clamp time, min (median, IQR) | 68 (55–85) | 69.5 (58–85) | 64 (51–85) | 0.051 |
| CPB time, min (median, IQR) | 100 (89–123) | 98 (89–116) | 104 (89–132) | 0.111 |
| Operative time, min (median, IQR) | 180 (160–210) | 178 (154–195) | 195 (175–228) |
PP, posterior pericardiotomy; COPD, chronic obstructive pulmonary disease; PAD, peripheral arterial disease; MI, myocardial infarction; TIA, transient ischemic attack; CHF, congestive heart failure; NYHA, New York Heart Association; LVEF, left ventricular ejection fraction; LA, left atrium; CABG, coronary artery bypass grafting; CPB, cardiopulmonary bypass. *Fisher’s exact test applied for PAD due to low expected counts. **p-value calculated among all patients who underwent CABG (CABG alone or Combination, N = 192).
All analyses were performed using IBM SPSS Statistics, version 24.0 (IBM Corp.,
Armonk, NY, USA). Continuous variables were summarized as mean
Univariate logistic regression was used to identify risk factors for POAF.
Multivariable logistic regression adjusted for clinically relevant covariates
(e.g., age, sex, hypertension, diabetes, left atrial size, left ventricular
ejection fraction (LVEF)), irrespective of univariate significance. A two-tailed
p-value
Between January 2022 and June 2024, a total of 436 patients were screened for eligibility, of whom 210 were enrolled and randomized: 106 assigned to the PP group and 104 to the control group. The cohort had a median age of 60 years (IQR 50–65), with 78.5% being male. Baseline demographic data and operative characteristics were largely comparable between groups (Table 1).
Overall, baseline demographics and intraoperative variables were well matched between groups, with the exception of minor differences in echocardiographic parameters and operative duration.
The incidence of POAF was significantly reduced in the PP group compared with controls (8.5% vs. 22.1%; OR 0.32, 95% CI 0.14–0.71; p = 0.006) (Table 2).
| Outcome | Overall | PP group (n = 106) | Control group (n = 104) | p-value | |
| Primary outcome | |||||
| POAF, n (%) | 32 (15.2) | 9 (8.5) | 23 (22.1) | 0.006 | |
| Secondary outcomes | |||||
| Antiarrhythmic medication*, n (%) | 31 (14.8) | 8 (7.5) | 23 (22.1) | 0.003 | |
| Systemic anticoagulation*, n (%) | 19 (9.0) | 6 (5.6) | 13 (12.5) | 0.040 | |
| Electrical cardioversion, n (%) | 1 (0.5) | 0 (0.0) | 1 (0.6) | 0.320 | |
| Ventilation time, hr. (median, IQR) | 3.0 (3.0–4.5) | 3.0 (3.0–4.0) | 4.0 (3.0–6.0) | ||
| ICU stay, hr. (median, IQR) | 24.0 (22.0–29.0) | 23.0 (22.0–24.0) | 24.0 (22.2–45.0) | 0.004 | |
| Chest drains output (ICU), mL (median, IQR) | 445 (330–600) | 410 (300–550) | 490 (340–707) | 0.014 | |
| Total chest drainage, mL (median, IQR) | 670 (500–880) | 660 (500–850) | 695 (519–930) | 0.165 | |
| Hospital stays, days (median, IQR) | 6.0 (5.0–7.0) | 6.0 (5.0–7.0) | 6.0 (5.0–7.8) | 0.099 | |
| Readmission, n (%) | 23 (11.0) | 11 (10.4) | 12 (11.5) | 0.788 | |
PP, posterior pericardiotomy; POAF, postoperative atrial fibrillation; ICU, intensive care unit. *Refers to treatment administered for POAF.
Among secondary endpoints, the need for antiarrhythmic therapy was lower in the PP group (7.5% vs. 22.1%; OR 0.28, 95% CI 0.11–0.67; p = 0.003), as was the requirement for systemic anticoagulation (5.6% vs. 12.5%; OR 0.41, 95% CI 0.15–0.97; p = 0.040). Electrical cardioversion was infrequent, with no significant difference between groups (0% vs. 0.6%; p = 0.32).
Patients in the PP group also demonstrated shorter ventilation times and ICU
stays. Median ventilation time was 3.0 hours (IQR 3.0–4.0) versus 4.0 hours (IQR
3.0–6.0) in controls (p
Postoperative chest drainage during ICU stay was significantly lower in the PP group (median 410 mL, IQR 300–550) than in controls (median 490 mL, IQR 340–707; p = 0.014). However, cumulative drainage during hospitalization did not differ significantly (p = 0.165). Median hospital stay was 6 days in both groups (p = 0.099), and readmission rates were comparable (10.4% vs. 11.5%; p = 0.788).
Posterior pericardiotomy was associated with a marked reduction in pericardial
complications compared with the control group. The incidence of pericardial
effusion was significantly lower in the PP group (9.4% vs. 39.4%; OR 0.17, 95%
CI: 0.08–0.36; p
| Outcome | Overall | PP group (n = 106) | Control group (n = 104) | p-value |
| Pericardial effusion, n (%) | 51 (24.3) | 10 (9.4) | 41 (39.4) | |
| Cardiac tamponade, n (%) | 10 (4.8) | 0 (0.0) | 10 (9.6) | 0.003 |
| Left pleural effusion, n (%) | 47 (22.4) | 26 (25.0) | 21 (19.8) | 0.367 |
| Re-exploration, n (%) | 8 (3.8) | 1 (0.9) | 7 (6.7) | 0.067 |
| – for bleeding | 2 (1.0) | 1 (0.9) | 1 (0.9) | 1.000 |
| – for tamponade | 6 (2.9) | 0 (0.0) | 6 (5.8) | 0.036 |
| Hospital mortality, n (%) | 5 (2.4) | 0 (0.0) | 5 (4.8) | 0.067 |
| Adverse events, n (%) | 8 (3.8) | 2 (1.9) | 6 (5.8) | 0.267 |
| Pulmonary complications, n (%) | 15 (7.1) | 4 (3.8) | 11 (10.6) | 0.056 |
| Sternal complications, n (%) | 13 (6.2) | 7 (6.6) | 6 (5.8) | 0.802 |
| Renal impairment, n (%) | 18 (8.6) | 7 (6.6) | 11 (10.6) | 0.304 |
Data are presented as n (%). PP, posterior pericardiotomy. Chisquare test with
continuity correction was used for categorical variables (Fisher’s exact test
applied when expected frequency
Hospital mortality was 0% in the PP group and 4.8% in the control group (p = 0.067). This difference was not statistically significant. Postoperative pulmonary complications were lower in the PP group (3.8% vs. 10.6%; p = 0.056), although this trend did not reach statistical significance. Rates of sternal complications and renal impairment were comparable between the two groups.
On univariate analysis, PP was associated with a reduced risk of POAF (OR 0.48, 95% CI 0.25–0.90; p = 0.022). No other baseline or operative characteristics (age, sex, comorbidities, left atrial size, LVEF, operative times) were significantly associated with POAF (Table 4). In multivariable analysis adjusting for clinically relevant covariates (age, sex, hypertension, diabetes, left atrial size, LVEF, surgical type), PP remained an independent protective factor against POAF (adjusted OR 0.194, 95% CI 0.06–0.62; p = 0.006).
| Variable | POAF (n = 32) | No POAF (n = 178) | OR (95% CI) | p-value |
| Age, years (mean |
58.6 |
56.6 |
1.01 (0.98–1.03) | 0.626 |
| Female sex, n (%) | 5 (15.6) | 40 (22.5) | 1.05 (0.56–1.97) | 0.877 |
| Hypertension, n (%) | 13 (40.6) | 93 (52.2) | 1.55 (0.79–3.07) | 0.204 |
| Diabetes mellitus, n (%) | 13 (40.6) | 76 (42.7) | 1.06 (0.54–2.11) | 0.859 |
| Smoker, n (%) | 6 (18.8) | 55 (30.9) | 1.51 (0.67–3.39) | 0.316 |
| Prior MI, n (%) | 27 (84.4) | 126 (70.8) | 0.67 (0.37–1.24) | 0.201 |
| Prior stroke/TIA, n (%) | 1 (3.1) | 12 (6.7) | 5.95 (0.79–44.7) | 0.083 |
| COPD, n (%) | 3 (9.4) | 10 (5.6) | 0.63 (0.20–2.00) | 0.437 |
| CHF (NYHA II–IV), n (%) | 13 (40.6) | 76 (42.7) | 1.07 (0.58–1.97) | 0.824 |
| LA size, cm (median, IQR) | 3.6 (3.4–4.1) | 4.0 (3.5–4.2) | 1.00 (0.76–1.30) | 0.974 |
| Haematocrit, % (median, IQR) | 39.0 (34.8–40.0) | 38.7 (35.7–41.0) | 0.96 (0.98–1.02) | 0.198 |
| Creatinine, mg/dL (median, IQR) | 1.0 (0.8–1.2) | 0.9 (0.8–1.2) | 0.81 (0.29–2.25) | 0.691 |
| LVEF, % (median, IQR) | 50 (40.3–59.7) | 52 (45–60) | 1.00 (0.97–1.03) | 0.840 |
| Surgical type (CABG vs. others) | — | — | 0.84 (0.50–1.42) | 0.508 |
| No. of grafts (mean |
3.25 |
3.23 |
1.07 (0.61–1.88) | 0.824 |
| Posterior pericardiotomy, n (%) | 9 (28.1) | 97 (54.5) | 0.48 (0.25–0.90) | 0.022 |
| Cross-clamp time, min (median, IQR) | 69 (55–86) | 67 (55–85) | 1.00 (0.98–1.01) | 0.578 |
| CPB time, min (median, IQR) | 100 (90–120) | 100 (89–123) | 1.00 (0.99–1.01) | 0.500 |
| Operative time, min (median, IQR) | 180 (165–223) | 180 (160–210) | 1.00 (0.99–1.01) | 0.904 |
POAF, postoperative atrial fibrillation; MI, myocardial infarction; TIA, transient ischemic attack; COPD, chronic obstructive pulmonary disease; CHF, congestive heart failure; NYHA, New York Heart Association; LA, left atrium; LVEF, left ventricular ejection fraction; CABG, coronary artery bypass grafting; CPB, cardiopulmonary bypass. Odds ratios are from univariate logistic regression.
Our findings are consistent with previous randomized controlled trials and meta-analyses demonstrating the protective effect of posterior pericardiotomy in reducing POAF [18, 19, 20, 21, 22, 23]. Gaudino et al. [24] reported that posterior pericardiotomy significantly reduced the incidence of pericardial effusion and POAF after cardiac surgery. Similarly, Amr and Elkassas [21], Ahmad et al. [25], and Zhao et al. [26], all confirmed that PP is associated with a lower risk of POAF without increasing surgical complications.
Some earlier studies, such as Asimakopoulos et al. [7] and Bakhshandeh et al. [27], did not observe significant benefit, likely due to smaller sample sizes, heterogeneity, or underpowered designs.
Mechanistically, there are at least two plausible explanations for the reduction in POAF with PP. First, even small postoperative collections of pericardial fluid or thrombi can trigger atrial arrhythmias through local inflammation, oxidative stress, or mechanical compression [6, 28]. By providing continuous drainage into the pleural space, PP minimizes these triggers. Second, pericardiotomy itself may subtly alter atrial geometry and hemodynamics, reducing susceptibility to arrhythmic triggers, though this hypothesis requires further echocardiographic validation [24].
In line with earlier reports (e.g., Zhao et al., 2014 [26]; Ebaid
et al., 2021 [29]; Ekim et al., 2006 [23]), we observed
significantly fewer cases of pericardial effusion and cardiac tamponade in the PP
group (p
While some RCTs (e.g., Zhao et al. [26], and Kaygin et al., 2011 [32]) reported a higher incidence of pleural effusion in the PP group, we found no significant difference in pleural effusion rates between groups (p = 0.367), suggesting that with proper chest tube placement, PP does not increase the risk of pleural fluid accumulation.
Importantly, our study also evaluated key secondary outcomes. Patients in the PP group experienced shorter ICU stays (1.16 vs. 1.46 days, p = 0.004), shorter overall hospitalization (6.6 vs. 8.1 days), and lower in-hospital mortality (0% vs. 4.8%, p = 0.067). These improvements mirror findings in trials such as those by Erdil et al. [30] and Kaya et al. [31], which demonstrated better recovery metrics and reduced complication rates. The finding of lower hospital mortality in the PP group (0% vs. 4.8%) is noteworthy but should be interpreted cautiously. The small number of deaths limits the ability to attribute mortality differences directly to PP. However, the reduction in tamponade and re-exploration rates likely contributed to greater hemodynamic stability and fewer complications, which may explain this observation.
This trial has several limitations. First, it was a single-center study performed by a single surgeon, which may limit generalizability. Second, this study did not evaluate the duration of POAF episodes, which may also influence clinical outcomes. Future studies should assess the duration of POAF to clarify whether PP reduces overall arrhythmic burden. Finally, a small proportion of patients were lost to follow-up, which may have introduced bias. In addition, follow-up was limited to 30 days, consistent with the majority of published studies on POAF.
Posterior pericardiotomy was associated with a significantly lower incidence of POAF, pericardial effusion, and cardiac tamponade in patients undergoing CABG, aortic valve, or ascending aortic surgery. These findings, derived from the first randomized trial conducted in Yemen, suggest that PP is a safe and effective adjunct to cardiac surgery. Larger multicenter randomized trials are needed to confirm whether the observed benefits extend to broader populations and translate into consistent reductions in mortality and other major adverse outcomes.
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
IA and AAA designed the research study. IA collected, managed, and analyzed the data. NA prepared the tables. MAK and TN reviewed, edited the manuscript, and interpreted the results. IA drafted the manuscript. All authors contributed to critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was granted by the Research Ethics Committee of the Cardiovascular and Kidney Transplantation Centre, Taiz University, Yemen (Approval ID 0030425, dated December 20, 2021). Written informed consent was obtained from all participants prior to enrollment. The trial is registered on ClinicalTrials.gov under the identifier NCT07266935, https://clinicaltrials.gov/study/NCT07266935 and is registered on Yemen Clinical Research Registry (YCRR) under ID 20210411.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.