

 , Jieyu Cao 2, Wenkui Gao 1, Yong Xie 1, Yi Luo 1, Wenguang Zeng 1, Zhe Zhang 1, Jun Hu 1,*
, Jieyu Cao 2, Wenkui Gao 1, Yong Xie 1, Yi Luo 1, Wenguang Zeng 1, Zhe Zhang 1, Jun Hu 1,*
1 Department of Cardiothoracic Surgery, The Second Affiliated Hospital, Hengyang Medical School, University of South China, 421001 Hengyang, Hunan, China
2 Department of Cardiothoracic Surgery, The First Affiliated Hospital, Hengyang Medical School, University of South China, 421001 Hengyang, Hunan, China
Abstract
This study aimed to explore the clinical advantages of the non-free left subclavian artery and single-branch stent graft technique in treating acute DeBakey Type I aortic dissection, with a focus on evaluating the impact of the technique on intraoperative efficiency, postoperative complications, and prognosis.
This study retrospectively analyzed 58 patients with acute DeBakey type I aortic dissection admitted between August 2023 and October 2024. All enrolled patients underwent ascending aorta replacement in combination with total aortic arch replacement and descending aortic stent graft implantation. In the experimental group (n = 28), the left subclavian artery (LSA) was reconstructed using branched stent grafts for distal descending aortic repair, maintaining the anatomical integrity of the vessel and deliberately preserving the thoracic duct and recurrent laryngeal nerve. In the control group (n = 30), conventional minimally invasive stent reconstruction was employed for distal descending aortic repair with anatomical isolation of the LSA. Statistical analyses were conducted on intraoperative parameters (total operative time, heparinization duration), complications (chylothorax, hoarseness), and prognostic indicators (duration of tracheal intubation, mortality rate) using SPSS, version 26.0.0.0 (IBM Corp., Armonk, NY, USA), after controlling for preoperative baseline characteristics between groups.
The total surgical time in the experimental group was significantly shorter than that in the control group (256.21 ± 53.08 minutes vs. 298.97 ± 51.09 minutes; p = 0.003). The intensive care unit (ICU) length of stay (159.50 minutes vs. 257.00 minutes; p < 0.001) and postoperative hospital stay duration (14.00 days vs. 21.00 days; p = 0.001) were also shorter in the experimental group. There was no significant difference in mortality (28.57% vs. 10.00%; p = 0.071) and rethoracotomy rates (10.71% vs. 10.00%; p = 0.732) between the two groups. No cases of recurrent laryngeal nerve injury or chylothorax occurred in the experimental group, whereas the control group reported a 6.67% incidence of chylothorax and 10.00% noted hoarseness.
The non-free left subclavian artery and single-branch stent graft technique can significantly shorten surgical time and reduce postoperative drainage volume and ICU stay duration. Additionally, no recurrent laryngeal nerve injury or chylothorax was observed in this group. Thus, this technique represents a safe and effective surgical approach for acute DeBakey Type I aortic dissection.
Keywords
- acute DeBakey type I aortic dissection
- non-free left subclavian artery
- branched covered stent
- intraoperative parameters
- chylothorax
- recurrent laryngeal nerve injury
Acute DeBakey Type I aortic dissection (Acute type A aortic dissection, ATAAD) is one of the most perilous emergencies in cardiovascular surgery, characterized by its acute onset, rapid progression, and high mortality rate [1]. For patients diagnosed with acute Stanford Type A aortic dissection, the European Association for Cardio-Thoracic Surgery (Class Ib recommendation) in 2014 advised early surgical intervention [2]. Among them, DeBakey Type I dissection, which involves the ascending aorta, aortic arch, and the entire descending aorta, often requires ascending aorta and total aortic arch replacement combined with descending aorta stent grafting (i.e., Sun’s procedure) to completely remove the primary intimal tear and diseased vessels, replace them with artificial vessels, and restore true lumen blood flow to meet the perfusion needs of various organs. The left subclavian artery (LSA) is located deep with abundant surrounding structures; its dissection carries inherent risks of damaging the thoracic duct and recurrent laryngeal nerve, potentially leading to chylothorax or hoarseness [3, 4] that critically impact postoperative recovery.
In recent years, with the development of hybrid techniques for the aortic arch and advancements in materials science, the application of branched covered stents (Shanghai MicroPort) (Castor stent) has provided new solutions for the repair of aortic arch lesions [5, 6]. By implanting a branched covered stent intraoperatively to preserve the anatomical structure of the LSA, this approach can not only simplify surgical steps and shorten operative time but also potentially avoid the risks of nerve, surrounding branch vessel, and lymphatic system injuries associated with traditional surgery that requires LSA dissection [7]. However, existing studies have mostly focused on complex aortic dissection lesions involving the aortic arch branches. The clinical application value of non-dissection LSA technique combined with single-branch stent in acute DeBakey Type I dissection is still in the exploratory stage. In particular, the potential advantages of this technique in shortening operative time, reducing postoperative complications, and improving patient prognosis still need to be verified through multicenter clinical studies and evidence-based medicine.
During LSA dissection, the risk of bleeding increases, and surgical field exposure is challenging. Additionally, traction injury to the recurrent laryngeal nerve may cause vocal cord paralysis, leading to postoperative hoarseness [8, 9]. Moreover, the thoracic duct and its branches have a complex course behind the aortic arch, mostly located on the medial side of the LSA. Intraoperative injury may trigger chylothorax [10], increasing the risk of reoperation [11]. The use of branched covered stent technology, which anchors the LSA orifice directly with the stent branch without LSA dissection, theoretically avoids the aforementioned risks while reducing bleeding and operative time.
On the other hand, patients with acute DeBakey Type I dissection often suffer from poor perfusion of multiple organs. Rapid completion of blood flow reconstruction is positively correlated with patient prognosis [12]. These patients experience massive consumption of coagulation factors and coagulation dysfunction. After undergoing hypothermia and cardiopulmonary bypass during surgery, their coagulation function is on the brink of collapse [13, 14]. Simplifying surgical steps and reducing intraoperative cardiopulmonary bypass time can help salvage coagulation function and reduce ischemia-reperfusion injury [15]. The application of branched covered stents may optimize the surgical process through the following mechanisms: First, the precise docking of the stent branch with the LSA can simplify aortic arch vessel reconstruction steps. Second, the non-dissection technique avoids extensive separation of the left subclavian artery, reducing surgical trauma and potentially shortening cardiopulmonary bypass time. Third, the radial support force of the stent helps stabilize the distal anastomosis, reducing the risk of postoperative anastomotic stenosis and distal endoleak. However, existing literature still lacks systematic evidence on whether this technique can truly improve intraoperative efficiency and postoperative recovery indicators.
Based on the above background, this study aims to explore the clinical application value of non-dissection LSA combined with single-branch intraoperative stent grafting in the surgical treatment of acute DeBakey Type I dissection. By comparing the traditional LSA dissection technique, this study focuses on evaluating the following core issues: (1) Whether this technique can shorten aortic cross-clamp time and overall operative duration by simplifying aortic arch operations; (2) Whether it can effectively reduce the incidence of recurrent laryngeal nerve injury and chylothorax without LSA dissection; (3) Its impact on postoperative drainage volume, blood transfusion requirements, and the intensive care unit (ICU) stay duration. The study results will provide evidence-based support for optimizing surgical techniques in acute aortic dissection and promote the practical transformation of minimally invasive concepts in emergency great vessel surgery.
This study integrates anatomical protection concepts with endovascular techniques, proposing a dual optimization strategy of “structural preservation - functional reconstruction”: On the one hand, it achieves physiological reconstruction of LSA blood flow through a single-branch covered stent, avoiding damage from vessel dissection. On the other hand, it simplifies the aortic arch operation process using the modular design of the single-branch covered stent. Thus, while ensuring long-term prognosis, it reduces trauma and postoperative complications. We hypothesize that, compared with traditional techniques, this approach can significantly shorten key surgical time points, reduce the incidence of specific complications, and accelerate patient postoperative recovery. Through rigorous cohort comparison and multidimensional outcome analysis, this study attempts to establish a safer and more efficient technical pathway for the surgical treatment of acute DeBakey Type I dissection.
This study is a single-center retrospective cohort analysis, consecutively collected 58 patients with acute DeBakey Type I aortic dissection who underwent emergency surgery in the Department of Cardiovascular Surgery of our hospital from August 2023 to October 2024. All data were extracted from the electronic medical record system and surgical records. All patients received ascending aorta replacement, total aortic arch replacement, and descending aorta stent grafting (Sun’s procedure). Patients were divided into two groups based on whether the LSA was dissected during surgery: the experimental group (n = 28, using non-dissection LSA combined with single-branch intraoperative stent grafting technique) and the control group (n = 30, traditional LSA dissection technique). The study was approved by the Ethics Committee of our hospital (Approval number 2025050). Due to the retrospective nature of the analysis, patient informed consent was waived, and all data were anonymized.
Inclusion Criteria: ① Patients diagnosed with acute Stanford Type A
aortic dissection (symptom onset to surgery time
In the control group, the surgical procedure was conducted as follows: (1) After
satisfactory anesthesia, the patient was placed in the supine position followed
by routine disinfection and draping; a femoral artery incision and median
sternotomy were performed to expose the vessels and establish cardiopulmonary
bypass (CPB) with systemic heparinization (3 mg/kg, ACT
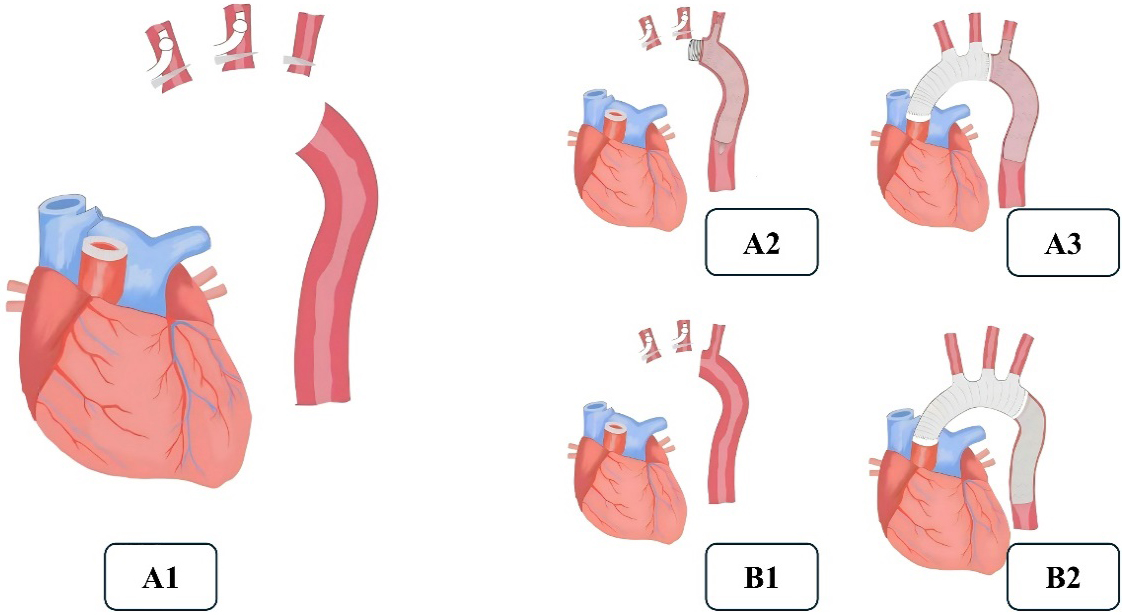 Fig. 1.
Fig. 1.
Application of non-mobilized left subclavian artery (LSA) with single-branched intraoperative stent graft technique in acute DeBakey type I aortic dissection surgery versus classical Sun’s procedure. (A1) Intraoperative mobilization of the brachiocephalic trunk and left common carotid artery. (A2) Intraoperative deployment of the single-branched stent graft. (A3) Schematic demonstrating aortic arch replacement with a four-branched artificial graft and concurrent descending aortic single-branched stent graft implantation for vascular remodeling. (B1, B2) Classical Sun’s procedure schematic, illustrating aortic arch replacement with a four-branched artificial graft and concurrent elephant trunk stent implantation in the descending aorta for vascular remodeling. LSA, left subclavian artery.
Statistical analysis was performed using SPSS 26.0.0.0. (IBM-SPSS Statistics,
Chicago, IL, USA). Normally distributed continuous variables were expressed as
mean
The two groups were comparable in terms of preoperative baseline
characteristics. As shown in Table 1, there were no statistically significant
differences between the experimental group (n = 28) and the control group (n =
30) in terms of age (54.93
| Variable | Experimental group (n = 28) | Control group (n = 30) | χ2/t | p |
| Age (years) | 54.93 |
54.13 |
0.289 | 0.774 |
| Hypertension | 25 (89.29%) | 26 (86.67%) | 1.000 | |
| Diabetes mellitus | 1 (3.57%) | 2 (6.67%) | 1.000 | |
| Coronary artery disease | 4 (14.29%) | 5 (16.67%) | 1.000 | |
| Renal insufficiency | 6 (21.43%) | 6 (20.00%) | 0.018 | 0.893 |
| Hyperlipidemia | 0 (0.00%) | 1 (3.33%) | 1.000 | |
| COPD | 0 (0.00%) | 2 (6.67%) | 0.492 | |
| Cerebral infarction | 7 (25.00%) | 4 (13.34%) | 1.283 | 0.257 |
| Amputation | 1 (3.57%) | 1 (3.34%) | 1.000 | |
| Smoking | 12 (42.86%) | 20 (66.67%) | 3.320 | 0.068 |
| Alcohol consumption | 7 (25.00%) | 9 (30.00%) | 0.181 | 0.670 |
COPD, Chronic obstructive pulmonary disease.
The experimental group demonstrated significantly better intraoperative time
efficiency compared to the control group. The total operative time was
significantly shorter in the experimental group (256.21
| Variable | Experimental group (n = 28) | Control group (n = 30) | Z/t | p |
| Total surgery time (min) | 256.21 |
298.97 |
–3.125 | 0.003 |
| CPB time (min) | 103.00 (91.00, 131.00) | 117.50 (100.00, 163.50) | –1.914 | 0.056 |
| Aortic cross-clamp time (min) | 37.00 (24.25, 68.00) | 46.50 (38.50, 105.00) | –2.296 | 0.022 |
| Circulatory arrest time (min) | 10.00 (9.00, 12.00) | 8.50 (8.00, 9.00) | –3.476 | 0.001 |
| Heparinization time (min) | 500.00 (405.00, 630.00) | 495.00 (450.00, 567.50) | –0.062 | 0.950 |
CPB time, cardiopulmonary bypass time.
The experimental group showed better performance in postoperative recovery and
complication control. The drainage volume on the first postoperative d ay was
significantly lower in the experimental group (median 843.00 mL vs. 1099.00 mL, Z
= –2.303, p = 0.021), and the total amount of red blood cell
transfusion was also lower (median 6.00 U vs. 7.00 U, Z = –2.085, p =
0.037). The experimental group had significantly shorter tracheal intubation time
(median 87.50 hours vs. 140.00 hours, Z = –2.723, p = 0.006), ICU stay
duration (median 159.50 minutes vs. 257.00 minutes, Z = –3.649, p
| Variable | Experimental group (n = 28) | Control group (n = 30) | χ2/Z | p |
| Re-thoracotomy | 3 (10.71%) | 3 (10.00%) | 0.117 | 0.732 |
| Paraplegia | 1 (3.57%) | 1 (3.33%) | 1.000 | |
| CRRT | 1 (3.57%) | 1 (3.33%) | 1.000 | |
| Mortality | 8 (28.57%) | 3 (10.00%) | 3.250 | 0.071 |
| Stroke | 0 (0.00%) | 0 (0.00%) | 1.000 | |
| Chylothorax | 0 (0.00%) | 2 (6.67%) | 0.492 | |
| Hoarseness | 0 (0.00%) | 3 (10.00%) | 0.238 | |
| Day 1 drainage (mL) | 843.00 (453.25, 1266.50) | 1099.00 (784.00, 1671.50) | –2.303 | 0.021 |
| Total RBC transfusion (U) | 6.00 (4.63, 7.38) | 7.00 (5.50, 11.00) | –2.085 | 0.037 |
| Drain removal time (h) | 13.50 (11.00, 17.00) | 16.00 (14.00, 17.25) | –2.144 | 0.032 |
| Ventilator duration (min) | 87.50 (50.50, 144.50) | 140.00 (117.75, 192.50) | –2.723 | 0.006 |
| ICU length of stay (min) | 159.50 (88.50, 199.13) | 257.00 (206.63, 332.25) | –3.649 | |
| Hospitalization duration (d) | 14.00 (3.25, 19.00) | 21.00 (17.75, 30.25) | –3.412 | 0.001 |
CRRT, continuous renal replacement therapy; RBC, red blood cell; ICU, intensive care unit.
For patients with acute DeBakey Type I aortic dissection, Sun’s procedure (total aortic arch replacement combined with the frozen elephant trunk technique) is a classic surgical approach in Mainland China [16]. Total aortic arch replacement, as the core of Sun’s procedure, requires adequate dissection of the three supra-aortic branches (brachiocephalic trunk, left common carotid artery, and left subclavian artery) during surgery. The LSA, compared to the brachiocephalic trunk and left common carotid artery, is located lower and surrounded by more structures. Therefore, there is a risk of damaging the recurrent laryngeal nerve and thoracic duct during LSA dissection, leading to corresponding postoperative complications (such as hoarseness and chylothorax) [17], which affect patients’ postoperative recovery and quality of life. The single-branch covered stent system is mainly used for aortic dissection patients with lesions involving the aortic arch, especially the left subclavian artery [18, 19]. It has achieved precise minimally invasive treatment for aortic arch lesions, simplified operations, reduced the risk of endoleak, and preserved blood flow to important branches [20]. To ensure the intraoperative safety and postoperative recovery of patients with acute DeBakey Type I aortic dissection, we have repeatedly reviewed films, consulted literature, and based on our understanding of aortic dissection and Sun’s procedure, we have applied the non-dissection LSA combined with single-branch covered stent technique within the scope of Sun’s procedure for acute DeBakey Type I aortic dissection surgery. We discuss this application from the following aspects.
This study systematically validated the significant advantages of the non-dissection LSA combined with single-branch stent grafting technique in the surgical treatment of acute DeBakey Type I aortic dissection. The total operative time in the experimental group was reduced by approximately 43 minutes compared to the traditional technique (p = 0.003), primarily due to the simplification of the dissection of the posterior wall of the aortic arch. In the traditional technique, dissection of the LSA requires extensive separation of the posterior wall of the aortic arch to expose the recurrent laryngeal nerve and the course of the thoracic duct, which is not only time-consuming but also prone to nerve injury or lymphatic rupture due to traction [21]. In contrast, the single-branch stent grafting technique achieves precise anchoring of the stent branch to the LSA orifice, directly reconstructing blood flow without the need for LSA dissection and anastomosis [22]. Additionally, the experimental group had a 23% reduction in postoperative drainage volume (p = 0.021) and a 14% decrease in red blood cell transfusion (p = 0.037), which may be related to the reduced intraoperative injury to the lymphatic system [23]. Injury to the thoracic duct in the traditional technique can lead to chyle leakage, while no chylothorax occurred in the experimental group, further confirming the protective effect of the non-dissection technique on lymphatic structures [24]. It is noteworthy that although the circulatory arrest time was slightly longer in the experimental group (10.0 minutes vs. 8.5 minutes), the aortic cross-clamp time was significantly shorter (37.0 minutes vs. 46.5 minutes, p = 0.022). The slightly prolonged circulatory arrest time in the experimental group (10.0 minutes vs. 8.5 minutes) reflects the deliberate intraoperative verification of true lumen guidewire positioning and precise deployment of the branched stent graft under direct vision; however, this necessary technical step crucially ensured accurate LSA branch anchoring without increasing neurological complications or compromising overall surgical efficiency gains. This suggests that the technique optimizes the aortic arch operation process, reducing the organ ischemic burden during deep hypothermic circulatory arrest (DHCA), which may have potential value in improving neurological prognosis [25].
Chylothorax and hoarseness are common complications associated with traditional
Sun’s procedure. In this study, the incidence of these complications was 0% in
the experimental group, while the control group had incidences of 6.67% and
10%. This can be largely attributed to the unique anatomical structure of the
LSA [26, 27]: the recurrent laryngeal nerve loops beneath the aortic arch and is
susceptible to thermal or traction injury during traditional LSA dissection.
Meanwhile, the thoracic duct, which drains into the venous system between the
left common carotid artery and the LSA, can be inadvertently severed during
surgery, leading to chylothorax. The single-branch stent grafting technique
circumvents these risks by avoiding dissection of the posterior aortic arch wall
[28]. Previous studies have reported postoperative hoarseness rates of 5%–15%
with traditional methods. The zero incidence in our experimental group
significantly outperforms these figures, suggesting that this technique could be
a great strategy for reducing nerve injury. Moreover, the experimental group
experienced a 38% reduction in ICU stay duration (p
The application of single-branch stent grafting not only simplifies surgical procedures but also enhances the stability of the distal anastomosis with its radial support force. In traditional techniques, the anastomosis between the descending aorta stent graft and the artificial vessel relies on suture techniques, which are prone to endoleak or anastomotic tear due to tissue fragility. In contrast, the branched stent graft used in the experimental group, by anchoring the true lumen, can evenly distribute the hemodynamic shear forces, thereby reducing the risk of late endoleak [29]. Moreover, preserving the anatomical continuity of the LSA helps maintain blood flow perfusion to the left upper limb and the vertebrobasilar artery, potentially reducing the incidence of postoperative spinal cord ischemia [30]. However, it is necessary to be vigilant about the potential risks of branched stent grafting. First, the true lumen of an acute dissection is often compressed and narrowed, and any deviation in stent deployment may result in incomplete coverage of important branches. Second, the mobility of the distal intimal flap of the dissection may affect the stent apposition. In this study, the rethoracotomy rate in the experimental group was comparable to that in the control group (10.71% vs. 10.00%), indicating the need for further optimization of stent deployment techniques, such as combining intraoperative ultrasound or angiography to confirm the position of the true lumen guidewire.
Although no statistical difference was found in mortality rates between the experimental and control groups (28.57% vs. 10.71%, p = 0.071), the causes of death detailed in Table 3 reveal that among the 8 deaths in the experimental group, 5 were due to coagulation disorders, 2 resulted from unrecoverable malignant arrhythmia (ventricular fibrillation), and 1 was caused by multiple organ failure; the 3 deaths in the control group were attributed to multiple organ failure, coagulation disorders, and acute respiratory distress syndrome (1 case each). The primary causes of mortality were associated with the critical nature of acute Debakey type I aortic dissection itself, preoperative malperfusion of multiple organs, and postoperative coagulation dysfunction, rather than being directly related to the technical approach for managing the left subclavian artery. The higher proportion of coagulation disorders in the experimental group may indicate a worse preoperative coagulation status or a more severe surgical stress response in these patients, though the difference was not significant likely due to the limited sample size; cases of ARDS and multiple organ failure in the control group might be related to intraoperative ischemia-reperfusion injury and postoperative inflammatory responses. These results suggest that the two techniques did not significantly differ in their impact on ultimate patient survival, which was primarily determined by the severity of the primary disease and the patients’ systemic condition; further studies with larger samples are needed to better identify high-risk factors and clarify their relationship with technical selection.
The current study has the following limitations: First, the retrospective design makes it difficult to completely eliminate selection bias. Although the baseline data are well matched, the lower proportion of smoking history in the experimental group (42.86% vs. 71.43%) may affect the interpretation of postoperative recovery indicators. Second, the small sample size (n = 58) may reduce statistical power, especially in the analysis of hard endpoints such as mortality (28.57% vs. 10.71%, p = 0.142), which requires cautious interpretation. Third, the lack of long-term follow-up data means that the durability of the branch stent and long-term complications (such as stent migration or new entry tear) cannot be assessed. In the future, multicenter randomized controlled trials should be conducted, combined with intraoperative imaging navigation technology, to further verify the safety of this surgical procedure. In addition, the application of the new type of four-branch stent may achieve anatomical reconstruction of the entire aortic arch vessels, but its feasibility in acute dissection still needs to be explored [31].
The non-free LSA combined with single-branch stent graft technique, through the synergistic effect of anatomical protection and blood flow reconstruction, provides a safer and more efficient surgical option for acute DeBakey type I aortic dissection. Its significant advantages in reducing operative time and postoperative complications meet the timeliness requirements of emergency aortic surgery and have broad clinical application value.
The datasets used in this study are available from the corresponding author upon reasonable request.
SXH contributed greatly to this work. SXH was primarily responsible for data collection, data analysis, result interpretation, and manuscript writing. JYC, WKG, YX, YL, ZZ, and WGZ were mainly responsible for the conception and design of the study, as well as drafting the manuscript. JH was primarily responsible for the overall conceptualization and design of the study. All authors contributed to editorial revisions of the manuscript. All authors read and approved the final manuscript. Each author has participated sufficiently in the work to assume public responsibility for relevant portions of the content and agreed to be accountable for all aspects of the work, ensuring questions related to its accuracy or integrity are appropriately addressed.
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Second Affiliated Hospital of the University of South China (Protocol No. 2025050). Informed consent for participation in this study and for the publication of its findings was secured in written form from the legally authorized representative of each participant.
This study was supported by colleagues from the Department of Cardiothoracic and Great Vascular Surgery, the Department of Radiology, and the Medical Records Room of the Second Affiliated Hospital of the University of South China. We sincerely appreciate their valuable contributions to the conduct of this research.
This study was supported by the Hunan Provincial Department of Science and Technology (Project No. C202304027603).
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/HSF49262.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.