





1 Center for Invasive Cardiology, Electrotherapy, and Angiology, 33-300 Nowy Sącz, Poland
2 Clinical Research Center Intercard, 30-514 Kraków, Poland
Abstract
Thrombus burden in patients with ST-segment elevation myocardial infarction (STEMI) facilitates distal embolization and microvascular obstruction (MVO), jeopardizing tissue reperfusion despite an open epicardial artery. Early single-center randomized trials (Thrombus Aspiration during Percutaneous Coronary Intervention in Acute Myocardial Infarction Study (TAPAS), Thrombectomy With Export Catheter in Infarct-Related Artery During Primary Percutaneous Coronary Intervention (EXPIRA)) have exhibited improved microvascular surrogates and suggested clinical benefit; however, pragmatic multicenter trials did not confirm efficacy for a routine aspiration strategy, i.e., Thrombus Aspiration in ST-Elevation Myocardial Infarction in Scandinavia (TASTE) and Trial of Routine Aspiration Thrombectomy with PCI versus PCI Alone in Patients with STEMI (TOTAL) did not demonstrate a reduction in death, reinfarction, or heart failure with aspiration plus percutaneous coronary intervention (PCI) versus PCI alone. In TOTAL, routine aspiration intake increased stroke: 0.7% versus 0.3% at 30 days (hazard ratio (HR) 2.06; 95% confidence interval (CI) 1.13–3.75), while the excess was evident within 48 hours and the signal was sustained to 180 days (1.0% versus 0.5%, HR 2.00, 95% CI 1.25–3.20); meanwhile, disabling or fatal strokes were also more frequent (HR 2.69). Accordingly, the current European Society of Cardiology (ESC) 2023 and American College of Cardiology/American Heart Association (ACC/AHA) 2025 guidelines dissuade routine manual aspiration (Class III, Level A) while supporting selective bailout application when large residual thrombus or refractory no-reflow exists despite standard measures. Device-based alternatives (rheolytic thrombectomy, distal protection) have failed to improve hard outcomes in native vessel primary PCI; meanwhile, newer continuous aspiration and coronary stent-retriever systems remain practical but unproven in outcomes trials. This narrative review appraises randomized and mechanistic evidence and proposes a practical, safety-first algorithm. This approach includes performing primary PCI rapidly with guideline-directed antithrombotic therapy; considering thrombectomy only in rare cases of very large thrombus burden when it is likely to improve flow; if aspiration is utilized, careful purging must be ensured to prevent air embolism, continuous negative pressure must be maintained, and a single slow pass performed with sustained suction to minimize embolization. Currently, in practice, the evidence overwhelmingly argues against routine aspiration. However, a selective and technically disciplined bailout approach may still be warranted in carefully chosen patients.
Keywords
- ST-segment elevation myocardial infarction
- primary PCI
- thrombectomy
- thrombus aspiration
- microvascular obstruction
- stroke
- safety
- bailout aspiration
- guidelines
Acute ST-segment elevation myocardial infarction (STEMI) is usually caused by abrupt thrombotic occlusion of a coronary artery. Primary percutaneous coronary intervention (PCI) restores epicardial patency in most cases, but distal embolization of thrombus and plaque debris may continue to sustain microvascular obstruction (MVO), increase infarct size, and adversely affect outcomes. As a result, mechanical thrombus retrieval during primary PCI emerged to mitigate distal embolization. Early randomized studies conducted in single-centers demonstrated improvement in surrogate endpoints, including myocardial blush grade (MBG) and ST-segment resolution (STR), as well as a reduction in 1-year cardiac mortality in patients routinely treated with aspiration [1, 2, 3]. These signals called for a more extensive adoption of thrombectomy as a routine adjunct to PCI. Subsequent large multicenter trials tempered this initial enthusiasm; the Thrombus Aspiration in ST-Elevation Myocardial Infarction in Scandinavia (TASTE) and Trial of Routine Aspiration Thrombectomy with PCI versus PCI Alone in Patients with STEMI (TOTAL) trials demonstrated that, in unselected populations of STEMI patients, routine aspiration yielded no clinical benefit [4, 5, 6, 7, 8]. In TOTAL, routine manual thrombectomy increased 30-day stroke (0.7% vs 0.3%; hazard ratio (HR) 2.06; 95% confidence interval (CI) 1.13–3.75), with the excess apparent within 48 hours, and the signal persisted at 180 days [9]. By contrast, TASTE reported no early difference in “neurological complications” at discharge, a discrepancy plausibly related to registry-based ascertainment using administrative codes and lower sensitivity to non-fatal events. Device-based thrombus retrieval techniques—rheolytic thrombectomy and distal embolic protection—have also failed to demonstrate a beneficial effect on clinical outcomes [10, 11, 12]. Ultimately, the 2023 European Society of Cardiology (ESC) guidelines and the 2025 American College of Cardiology/American Heart Association (ACC/AHA) guidelines are in agreement, both indicating Class III (Level of Evidence A) recommendations against routine aspiration. However, they acknowledge an important, albeit still selective and rare, bailout role in select cases of STEMI with a large thrombus burden, or in cases with known thrombus burden who have refractory no-reflow [13, 14].
For reference, Fig. 1 (Ref. [15]) illustrates the Thrombolysis in Myocardial Infarction (TIMI) Thrombus Scale used to classify coronary thrombus burden angiographically. This grading ranges from grade 0 (no visible thrombus) to grade 5 (total occlusion by thrombus) and helps identify cases of “large thrombus burden” relevant to patient selection for bailout thrombectomy.
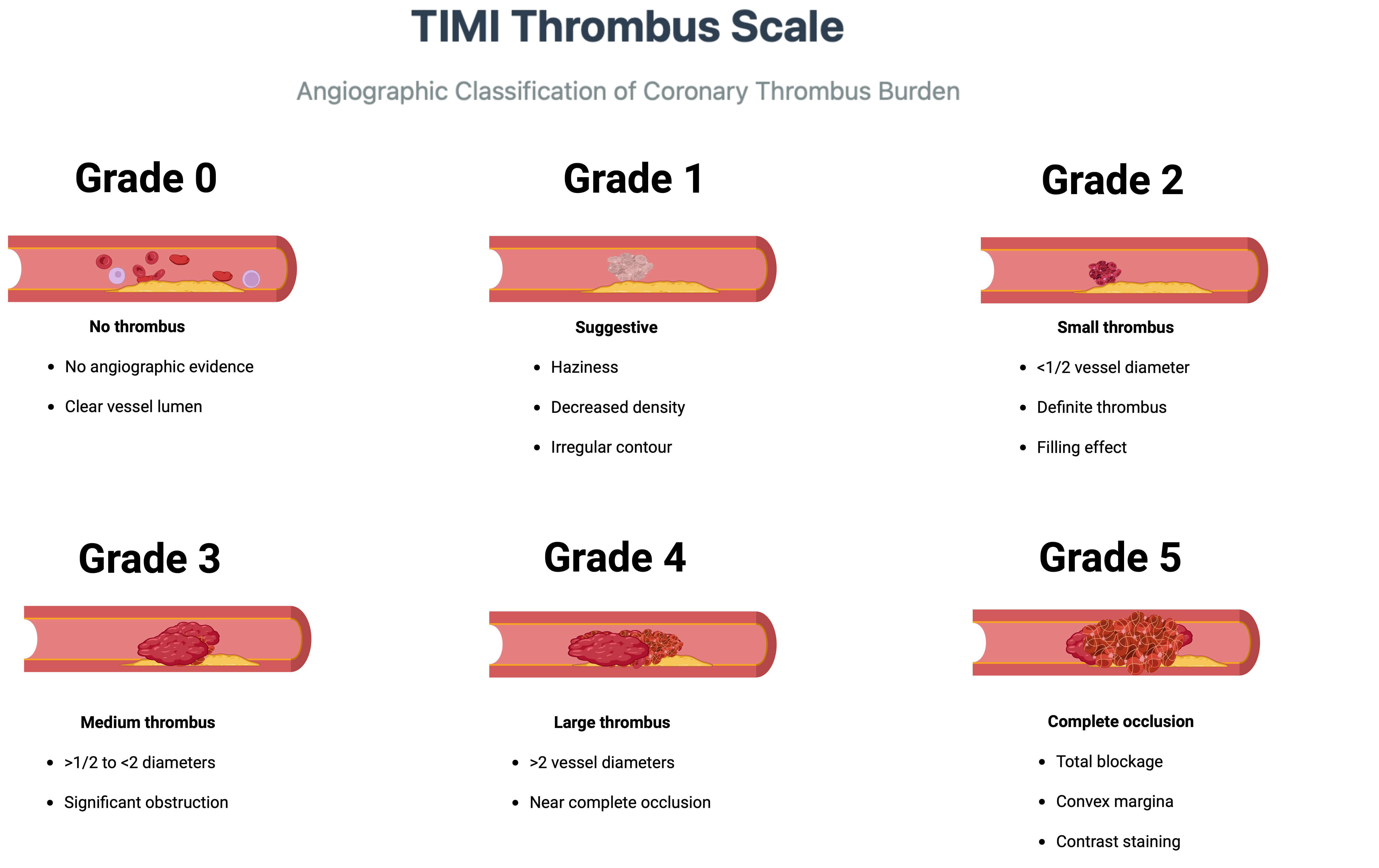 Fig. 1.
Fig. 1.
TIMI Thrombus Scale—Angiographic classification of coronary thrombus burden. Grades 0 through 5 correspond to progressively increasing intracoronary clot burden on angiography (grade 0: no thrombus; grade 5: occlusive thrombus). This standardized scale is used to gauge thrombus size and guide management decisions in STEMI. TIMI, Thrombolysis in Myocardial Infarction; STEMI, ST-segment elevation myocardial infarction. Adapted from Gibson CM et al. [15]. Figure created with BioRender.
This narrative review followed Scale for the Assessment of Narrative Review Articles (SANRA) (scope, literature search, referencing, scientific reasoning, and presentation) quality domains. We conducted a structured search of MEDLINE/PubMed and Embase from January 2005 to May 31, 2025, using combinations of STEMI, aspiration thrombus, thrombectomy, microvascular obstruction, distal protection, and stent-retriever. We selected English language randomized controlled trials (RCTs), prespecified substudies, large investigator-level meta-analyses, and, most importantly, current guidelines. Inclusion criteria were as follows: adult STEMI undergoing primary PCI; randomized comparisons (or prespecified substudies) of aspiration/thrombectomy versus PCI alone of comparative device strategies; clinically relevant outcomes (death, MI, heart failure (HF), stroke) and/or mechanistic endpoints (e.g., cardiac magnetic resonance (CMR), optical coherence tomography (OCT)). Exclusion criteria were as follows: non-STEMI populations, pure case series, non-comparative device reports, and non native-vessel protection except where explicitly mentioned (SVG). Study selection and data extraction were as follows: two reviewers independently screened the titles/abstracts and full text articles; discrepancies were settled by consensus. Data was extracted by one reviewer and independently verified by a second reviewer. In terms of study methods and outcomes, we deemed there to be enough heterogeneity to preclude quantitative meta-analysis; we synthesized the results, in collective agreement and explicitly stating where the ascertainment was register-based (e.g., neurological outcomes in TASTE).
Early single-center trials suggested microvascular and possible clinical
benefits. In TAPAS (n = 1071), routine aspiration improved Myocardial Blush Grade
3 and ST-segment resolution, with fewer 1-year cardiac deaths and cardiac
death/reinfarction events in prespecified analysis [1, 2]. In EXPIRA (n = 175,
anterior STEMI), aspiration increased STR
In TOTAL, 30-day stroke was higher with routine thrombectomy vs PCI alone
(33/5033 [0.7%] vs 16/5030 [0.3%]; HR 2.06; 95% CI 1.13–3.75), with an early
excess within 48 hours (0.30% vs 0.10%; HR 3.00; 95% CI 1.09–8.25).
The absolute risk increase at 30 days was 0.34% (number needed to harm
(NNH)
Data imply that newer thrombectomy technologies could provide improved safety. In the multicenter, single-arm CHEETAH study of continuous aspiration (n = 400; 389 with 30-day follow-up), the rate of stroke within 30 days was 0.77% (3/389), and no device-related serious adverse events were reported. As CHEETAH was non-randomized, any cross-trial comparisons with TOTAL should be interpreted cautiously [20]. In the RETRIEVE AMI trial, there were zero cerebrovascular events with the stent-retriever arm [21, 22].
Mechanistically, improved safety could be explained: (1) in aspiration with continuous negative pressure, less air entrainment occurs compared to intermittent, syringe systems, (2) en-bloc thrombus removal prevents fragmentation/thrombus embolism, and (3) fewer manipulations with the catheter minimize disturbance of aortic plaque. Still, these safety signals await verification in large randomized trials before the validity of newer aspiration techniques is determined to be better than manual aspiration.
Factors that are center-defined appear to be important in stroke prevention. Centers that use defined protocols in thrombectomy, areas solely for catheter preparation, and deliberate monitoring for ACT (anticoagulation time) will have lower complication rates regardless of the device used. Complete neurologic evaluation before and after any mechanical thrombectomy should be mandatory.
Both ESC 2023 and ACC/AHA 2025 discourage routine aspiration (Class III, LOEA). Yet, they permit case-by-case aspiration when large residual thrombus remains after initial flow restoration or when refractory no-reflow hampers reperfusion—generally a Class IIb scenario [13, 14]. Post-hoc analysis of high-thrombus subgroups within large RCTs did not show a clear outcome benefit for planned upfront aspiration [6, 7, 8].
AIMI (AngioJet rheolytic thrombectomy) found larger 30-day infarcts and more early adverse events with AngioJet than with PCI alone, raising concerns about the indiscriminate use of rheolytic energy and potential harm from worse distal embolization [10]. JETSTENT demonstrated better STR and lower 6-month major adverse cardiac events (MACE) rates with AngioJet before direct stenting, but no consistent infarct-size benefit, and was in tension with AIMI; overall, the evidence base is not consistent enough to support a case for routine use. Given inconsistent evidence and potential harm signals, rheolytic thrombectomy should not be used routinely in primary PCI [12].
In Enhanced Myocardial Efficacy and Recovery by Aspiration of Liberated Debris (EMERALD) (n = 501), distal protection captured debris but did not improve STR, infarct size, or 6-month outcomes; distal protection is not recommended in routine native-vessel primary PCI. Protection devices remain indicated in selected saphenous vein graft interventions but are not recommended for native-vessel primary PCI in STEMI [11].
Trials comparing intracoronary (IC) versus intravenous (IV) glycoprotein IIb/IIIa inhibition and testing low-dose IC fibrinolysis aimed to mitigate MVO. AIDA-STEMI showed no reduction in the composite of death, reinfarction, or new heart failure with IC abciximab versus IV [23]. In INFUSE-AMI (large anterior STEMI), lesion-directed IC abciximab reduced infarct size by MRI, whereas manual aspiration did not confer infarct-size benefit [24]. T-TIME found that low-dose IC alteplase did not reduce MVO overall and raised safety concerns among late presenters [25].
Deferring stent implantation to allow thrombus dissolution has intuitive appeal but has not been shown to translate into clinical benefit. In DANAMI-3–DEFER, deferred stenting did not reduce the composite of all-cause mortality, heart failure, or reinfarction compared with immediate stenting [26]. The strategy has therefore not been widely adopted. Accordingly, deferred stenting has not translated into reductions in mortality, recurrent MI, or HF, and should not be used routinely.
The Indigo System CAT RX comprises three components: the CAT RX aspiration catheter (5.3F outer diameter, 140 cm length, rapid exchange design compatible with 0.014″ guidewires and 6F guide catheters), the Penumbra ENGINE aspiration pump, and specialized aspiration tubing with integrated flow switch. This system represents adaptation of neurovascular thrombectomy technology proven over a decade in stroke intervention. The critical innovation is sustained mechanical vacuum at –29 inches of mercury (inHg) (nearly pure vacuum at 98.2 kPa absolute pressure). The Penumbra ENGINE maintains this constant aspiration force throughout the entire procedure.
In contrast, manual aspiration systems use syringes, and the initial negative pressure drops off rapidly over seconds. The technical benefits of continuous aspiration over manual aspiration include continuous suction without catheter changes, reduced risk of thrombus fragmentation through en bloc removal, trackability with neuro-tracking technology, and compatibility with 6F guide catheters with a 5.3F profile. The sustained mechanical aspiration approach solves the shortcomings of manual systems by alleviating variation with an operator-dependent technique and incomplete extraction of thrombus.
The CHEETAH study (prospective, multicenter, non-randomized) (n = 400) has tested the safety and efficacy of CAT RX used in high thrombus burden acute coronary syndrome patients. The study reported favorable primary outcomes (30-day MACE 3.6% [14/389]), very high final TIMI 3 flow (97.5%), and TIMI thrombus grade 0 (99.5%). Stroke within 30 days occurred in 0.77% (3/389); no device-related serious adverse events were observed [20]. The study was non-randomized and therefore hypothesis-generating. A new AVIS protocol (Aspiration, Vasodilators, Imaging, Stenting) was developed to highlight the systematic approach of continuous aspiration thrombectomy [27].
A different innovative approach involves stent-retrievers, self-expanding mesh
devices delivered via a microcatheter and deployed directly into the thrombus,
where they entangle and capture the clot for removal. Widely used in stroke
interventions, these devices demonstrated high rates of vessel recanalization and
favorable clinical outcomes by physically extracting the thrombus rather than
just pushing it aside. The RETRIEVE AMI trial is the first randomized trial to
examine stent-retriever thrombectomy (SRT) using the Solitaire X device in STEMI
patients with substantial thrombus burden. This single-center study randomized 81
patients with TIMI thrombus grade
Relevant outcomes indicate: SRT extracted significantly larger thrombus volumes than manual aspiration (three-fold difference), with efficacy proportional to baseline thrombus burden. The pre-stent thrombus volume remaining after intervention did not differ significantly between the SRT-assisted group and the manual aspiration group; however, both thrombectomy methods significantly reduced thrombus burden compared to no thrombectomy. Additionally, there were no device-related arterial complications or cerebrovascular events noted in the SRT treatment arm; significantly, thrombus modification was associated with superior myocardial perfusion [21, 22].
Clinical implications: RETRIEVE AMI demonstrates the feasibility and safety of coronary stent-retriever thrombectomy, with an emphasis on OCT-based patient selection, and states that device selection should be tailored to each patient’s actual thrombus burden rather than solely on the angiographic appearance of the thrombus at the time of intervention. RETRIEVE AMI suggests an individualized approach to mechanical thrombectomy.
The above-mentioned large-lumen continuous-aspiration systems, as well as coronary stent-retriever techniques, are investigational. The aim behind developing new thrombectomy technologies is to overcome the limitations of previous devices. Manual aspiration was operator-dependent and often removed only part of the clot; rheolytic thrombectomy carried risks like hemolysis and distal embolization; and distal protection filters could not entirely prevent embolization. Although none of the new devices have yet shown a significant improvement in hard clinical outcomes when used routinely, they may be helpful in selective cases (high thrombus burden, refractory no-reflow). There is a paradigm shift towards choosing a device based on anatomy, thrombus composition, and individual patient scenario, rather than relying on a single technology for all cases. Since no single device has been validated for routine use, these approaches should be restricted to research protocols or exceptional bailout scenarios
Recent data have raised doubts over the reliability of angiographic thrombus
assessment, showing that there were considerable differences between TIMI
thrombus grading and actual thrombus burden when assessed by OCT. The RETRIEVE
AMI trial (2025) showed that in patients with a TIMI thrombus grade
This observation brings into question the patient selection or exclusion processes used by larger randomized trials. A systematic approach using baseline OCT may be beneficial in determining which STEMI cases would genuinely benefit from thrombus modification approaches.
Corrected sentence: “In the TOTAL-OCT sub-study, the median pre-stent thrombus burden was just 2.36%, significantly less than the 12.96% in the RETRIEVE AMI cohort, which might explain the neutral result of routine manual aspiration [8].”
OCT-guided techniques have shown encouraging clinical outcomes. An extensive prospective registry of 3897 STEMI patients demonstrated that OCT-guided primary PCI (69.2% of cases) was associated with significantly lower 5-year all-cause and cardiovascular mortality rates compared to angiography-guided interventions [28]; the benefits were confirmed after propensity scoring. The oct-guided cohort of patients had a greater proportion of patients who underwent thrombus aspiration, as the strategy was tailored using imaging.
Clinical Implementation: OCT performance should be contemplated in STEMI cases where there is a suspicion of high thrombus burden for multiple reasons: (1) accurately assessing and quantifying accurate thrombosis volume, (2) to help select devices used, i.e., between manual aspiration, continuous aspiration systems, or stent-retrievers, (3) to assess standardized procedural success after thrombus modification. A personalized approach to patient selection may optimize outcomes and improve the risk-benefit of mechanical thrombectomy.
Fig. 2 illustrates how imaging-guided decision-making translates into procedural strategy during primary PCI for STEMI. The schematic highlights the transition from an occluded, thrombus-filled artery to restored flow through three main techniques—standard balloon–stent implantation, aspiration-based thrombectomy, and stent-retriever extraction. Integrating OCT-derived thrombus characteristics enables operators to choose devices purposefully, adjust procedural sequencing, and implement deferred stenting when distal embolization risk is high. This visualization underscores the shift toward precision-guided reperfusion rather than uniform device application.
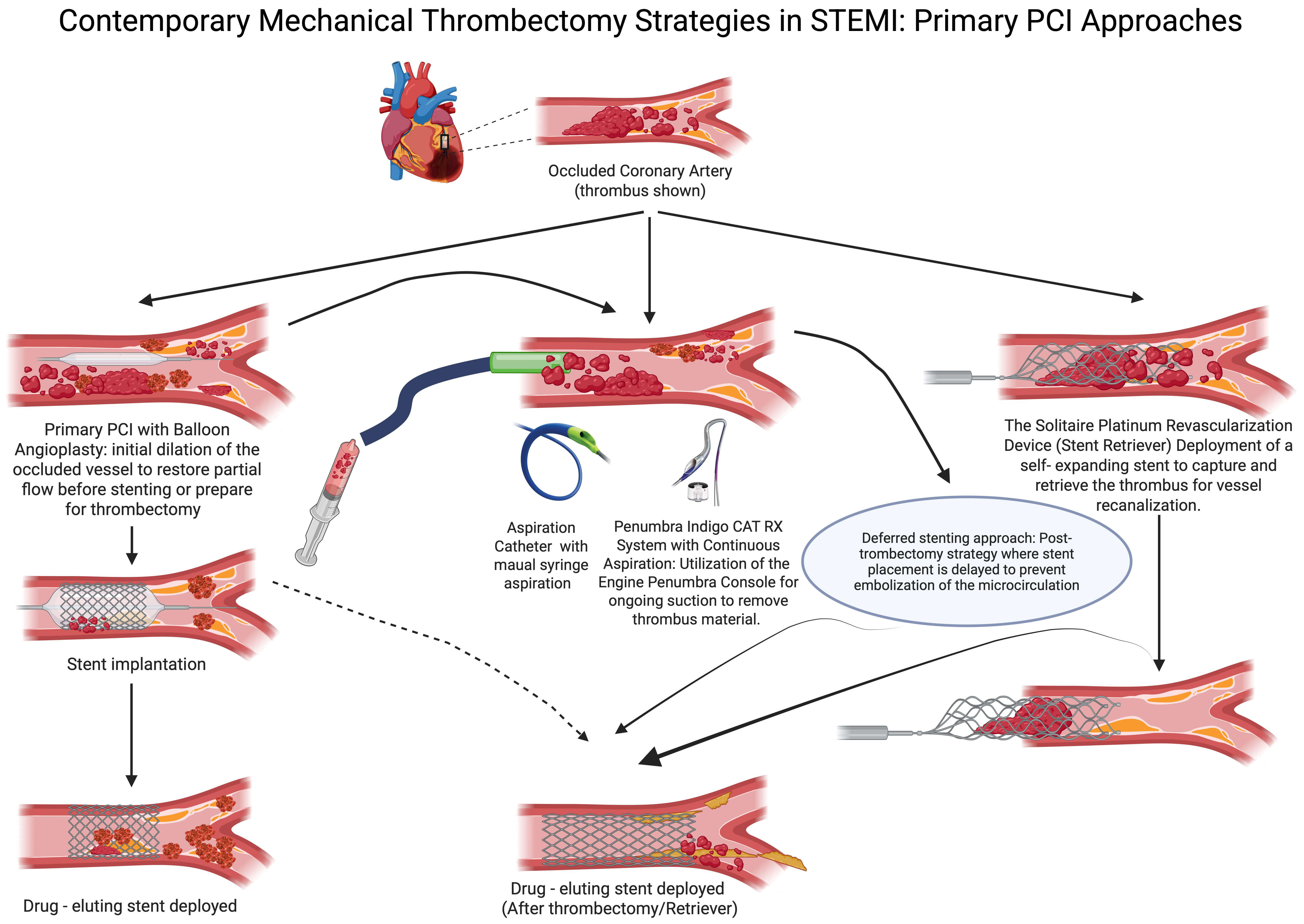 Fig. 2.
Fig. 2.
Contemporary mechanical thrombectomy strategies in STEMI—primary PCI approaches. The schematic illustrates the primary mechanical thrombectomy techniques used during primary percutaneous coronary intervention for ST-elevation myocardial infarction. Starting from an occluded coronary artery containing thrombus, three principal approaches are depicted: (1) Standard primary PCI pathway with balloon angioplasty for initial vessel dilation, followed by drug-eluting stent implantation; (2) Aspiration-based thrombectomy (manual syringe catheters or large-lumen continuous aspiration systems, e.g., CAT RX type); and (3) Stent retriever for mechanical extraction. A deferred stenting strategy is highlighted, wherein stent placement is delayed following thrombectomy to minimize the risk of distal embolization. Although these devices offer theoretical benefits for thrombus management, routine use has not demonstrated improved clinical outcomes in randomized trials, and current guidelines do not support their routine deployment in patients with STEMI undergoing primary PCI. Created with BioRender. PCI, percutaneous coronary intervention.
Current European and American guidelines converge that routine manual aspiration during primary PCI in STEMI is not recommended, whereas selective bailout use may be considered in cases of large residual thrombus or refractory no-reflow despite standard measures [13, 14]. These recommendations reflect consistent neutral results across large, randomized trials and the observed stroke signal with aspiration [6]. Accordingly, both ESC 2023 and ACC/AHA 2025 discourage routine manual aspiration (Class III, Level A) while allowing strictly selective bailout use in the presence of large residual thrombus and refractory no-reflow, aligning the guidance with the neutral large-scale evidence and the stroke signal.
Persistently large thrombus burden after wiring and gentle lesion preparation, e.g., TIMI thrombus grade 4–5 with a long, laminated tail that is unlikely to be jailed safely by a stent.
Refractory no-reflow or slow-flow (TIMI flow
Recurrent distal embolization observed angiographically during minimal manipulation, suggesting high embolic potential of residual thrombus.
Proximal, large-caliber culprit vessel with high thrombus load, where limited, controlled aspiration could plausibly restore laminar flow before definitive stenting.
Contra-indicators to routine use (favor conservative PCI): very tortuous/angulated segments, heavy calcification with poor catheter support, ostial lesions with high risk of aortic plaque disruption, severely delayed presentation with organized thrombus.
Preparation and purging: Prime the aspiration system meticulously to avoid air entrainment; maintain continuous negative pressure before entering the coronary ostium.
Guide support and coaxiality: Use a stable guide and keep the aspiration catheter coaxial to minimize plaque/arch scraping; avoid deep intubation in atherosclerotic ostia.
Limit passes: Prefer one slow, deliberate pass across the thrombus; reassess flow and perfusion markers (TIMI/MBG/STR) before considering a second pass.
Flow-protective technique: Maintain suction while withdrawing the catheter into the guide to reduce embolic spill; allow controlled back-bleeding and vigorous saline flushes.
Anticoagulation: Maintain activated clotting time (ACT)
Avoid fragmentation: Minimize pre-dilation in very large thrombus; if needed, use small, short inflations to preserve thrombus integrity before a single aspiration pass.
Post-aspiration strategy: If TIMI-3 is restored with an acceptable angiographic result, proceed to definitive stenting with careful sizing; if no-reflow persists, treat pharmacologically and reassess the need for further device passes versus conservative completion.
When to stop: Abort further aspiration if there is no incremental flow improvement, catheter instability, suspected air or athero-embolization, or vessel trauma.
Fig. 3 distills the evidence into a pragmatic, imaging-informed algorithm for thrombus clearance during primary PCI in STEMI. It prioritizes a no-routine-thrombectomy default, defines selective bailout pathways for high thrombus burden or impaired flow, integrates OCT-based assessment, and annotates class-of-recommendation and the stroke-risk signal from TOTAL to guide real-time decisions.
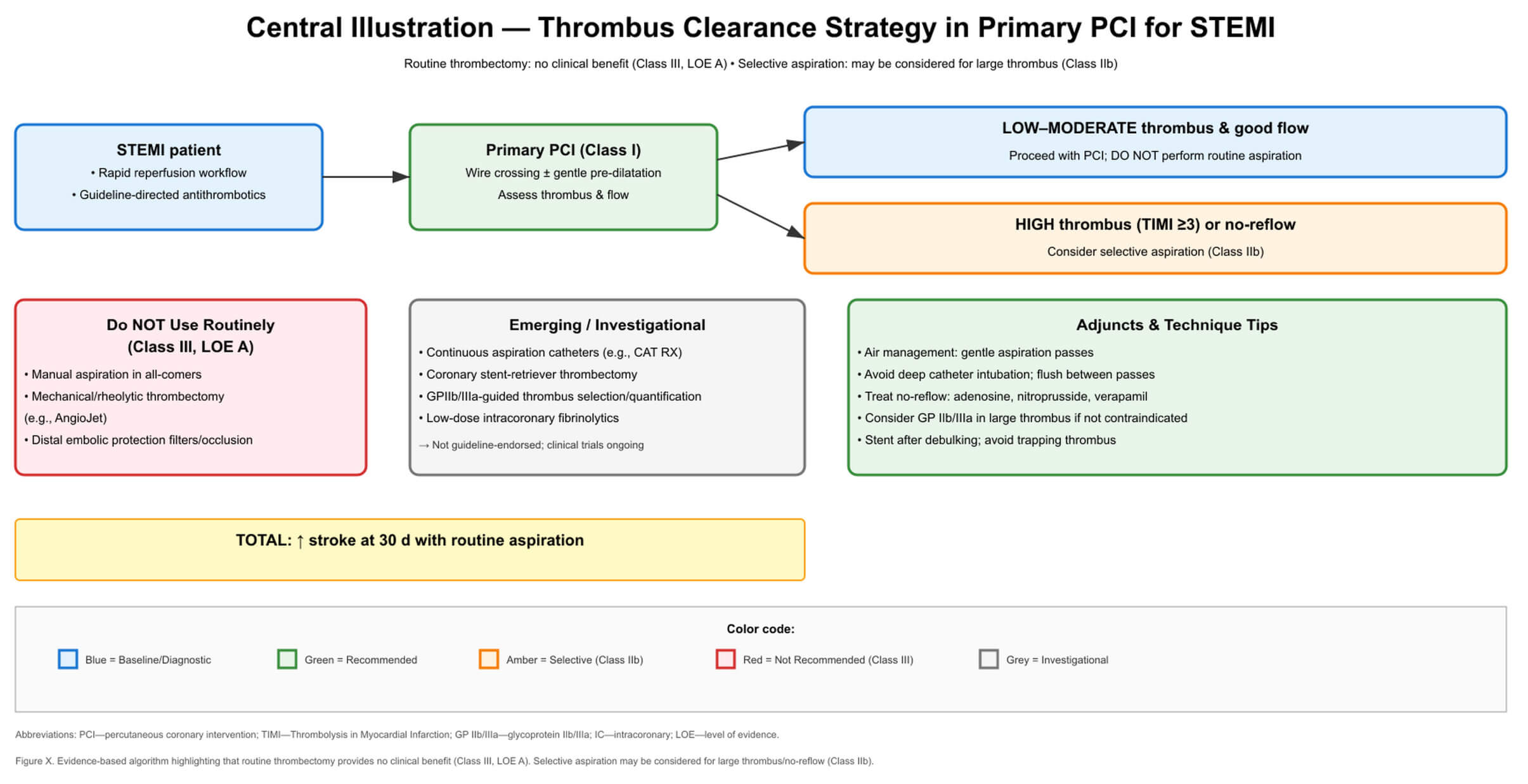 Fig. 3.
Fig. 3.
Central illustration—thrombus clearance strategy in primary PCI for STEMI.
This evidence-based algorithm guides clinical decision-making for thrombus management during primary percutaneous coronary intervention. Following initial wire crossing and flow assessment, patients are stratified by thrombus burden (TIMI thrombus grade) and flow status. The algorithm emphasizes that routine thrombectomy provides no clinical benefit (Class III, Level of Evidence A) while allowing for selective aspiration in cases of high thrombus burden with impaired flow (Class IIb). The schema incorporates current ESC 2023 [14] and ACC/AHA 2025 [13] guideline recommendations, highlights interventions to avoid, presents emerging investigational approaches, and provides practical technique tips for selective thrombectomy when indicated. The key safety finding from the TOTAL trial [9], regarding an increased stroke risk associated with routine aspiration, is prominently displayed.
The Table 1 (Ref. [10, 11, 12, 13, 14]) summarizes the current position of both ESC 2023 and ACC/AHA 2025 on the various thrombectomy techniques available for the management of STEMI. The table presents a comparison of the recommendations regarding routine, selective and device based approaches to the thrombectomy techniques for STEMI; the table shows that there is agreement among the two organizations to recommend against the routine aspiration strategy and very little support for bailout use. The table will provide a quick reference guide to allow the clinician to make an informed decision about their procedural approach to STEMI based on current clinical evidence and class of recommendation.
| Intervention | ESC 2023 Recommendation | ACC/AHA 2025 Recommendation |
| Routine manual aspiration | Class III, Level A—Not recommended (“Routine thrombus aspiration is not recommended”) [14]. | Class III (No Benefit), Level A—Not beneficial (manual aspiration thrombectomy should not be performed routinely) [13]. |
| Selective (“bail‑out”) manual aspiration | Class IIb, Level C—May be considered in selected patients with large/persistent thrombus burden (bail‑out use) [14]. | Formal Class/Level not assigned for bailout in the 2025 text [13]. |
| Rheolytic thrombectomy (AngioJet) | Not recommended routinely (no proven outcome benefit over conventional PPCI; evidence from RCTs is neutral/negative) [10, 12, 14]. | Not recommended routinely (no benefit)—contemporary guidance does not endorse routine mechanical/rheolytic thrombectomy in STEMI; evidence has not shown benefit vs standard [10, 12, 13]. |
| Distal embolic protection | Not recommended in primary PCI for native‑vessel STEMI (no benefit) [11, 14]. | Not endorsed for STEMI (no benefit) — not recommended for native‑vessel primary PCI; use of protection devices is confined to selected SVG settings in revascularization guidance [13]. |
Note: In the ACC/AHA 2025 document, only the prohibition of routine manual aspiration carries a formal Class/Level. Bailout aspiration is allowed in narrative text (no separate class).
STEMI, ST-segment elevation myocardial infarction; ESC, European Society of Cardiology; ACC/AHA, American College of Cardiology/American Heart Association; PPCI, Primary percutaneous coronary intervention; RCTs, randomized controlled trials; SVG, Saphenous vein graft.
The Cochrane Risk-of-Bias 2 (RoB 2) assessment for the pivotal thrombectomy trials is summarized in Table 2 (Ref. [1, 2, 3, 4, 5, 6, 10, 12]). This table evaluates the reliability of trial results based on randomization integrity, blinding, and data completeness as well as how reliable the measured outcomes were to evaluate reliability of study results. A uniform “low” or “some concerns” rating suggests that these landmark studies have moderate to high internal validity and thus support current practices.
| Trial (Year) | Randomization | Deviations/Blinding | Missing data | Outcome measurement | Overall bias |
| TAPAS (2008) [1, 2] | Low | Some concerns | Low | Low | Some concerns |
| TASTE (2013–14) [4, 5] | Low | Some concerns | Low | Low | Low |
| TOTAL (2015) [6] | Low | Some concerns | Low | Low | Low |
| EXPIRA (2009) [3] | Low | Some concerns | Low | Low | Some concerns |
| JETSTENT (2010) [12] | Low | Some concerns | Low | Low | Some concerns |
| AIMI (2006) [10] | Low | Some concerns | Low | Low | Some concerns |
TAPAS, Thrombus Aspiration during Percutaneous Coronary Intervention in Acute Myocardial Infarction Study; TASTE, Thrombus Aspiration in ST-Elevation Myocardial Infarction in Scandinavia; TOTAL, Trial of Routine Aspiration Thrombectomy with PCI versus PCI Alone in Patients with STEMI; EXPIRA, Thrombectomy With Export Catheter in Infarct-Related Artery During Primary Percutaneous Coronary Intervention; JETSTENT, AngioJet rheolytic thrombectomy before direct Infarct artery stenting in patients with acute Myocardial Infarction.
Table 2 shows judgments follow Cochrane RoB 2 (Risk of Bias 2) domains and refer to effects of assignment (intentiontotreat). Where risk varies by outcome (e.g., mortality vs stroke).
The information in Table 3 (Ref. [9, 10, 12, 20, 21]) synthesizes both comparative effectiveness and mechanistic information on current thrombectomy technology and compares these by the first generation’s manual aspiration with continuous vacuum, stent retrievers, and rheolytics as well as how each relates to procedural success and cerebrovascular safety. The results show a clear progression in technology from manual aspiration and stent retrievers toward continuous aspiration and mechanical retrieval; however, it also shows that although there is an improvement in flow metrics, there is no evidence of consistent clinical benefits from this progression.
| Device category | Representative system | Mechanism | Key study | TIMI 3 flow | Stroke rate | Evidence level* |
| Manual Aspiration | Export/Pronto | Syringe-based negative pressure | TOTAL (n = 10,732) [9] | 0.7% (HR 2.06) | Strong (negative) | |
| Continuous Aspiration | CAT RX (Penumbra) | Sustained vacuum (–29 inHg) | CHEETAH (n = 400) [20] | 97.5% | 0.77% (30 days); no device-related SAEs | Moderate (positive) |
| Stent-Retriever | Solitaire X | Mechanical entrapment/extraction | RETRIEVE AMI (n = 81) [21] | 0% | Limited (promising) | |
| Rheolytic | AngioJet | High-pressure saline jets | AIMI [10]/JETSTENT [12] | Variable | Not specified | Moderate (negative) |
*Evidence levels: Strong = Large multicenter RCTs; Moderate = Single-center RCTs or large registries; Limited = Small studies or registries. HR, Hazard ratio; SAEs, Serious Adverse Events.
Table 3 compares current thrombectomy modalities—manual aspiration, continuous vacuum aspiration, stent retrievers, and rheolytic systems—together with mechanisms.
The management of intracoronary thrombus during primary PCI requires a systematic approach that balances potential benefits against demonstrated risks. Current evidence supports a selective rather than routine thrombectomy strategy, with clear differentiation between patients who may benefit from mechanical intervention and those who should proceed with standard PCI alone. The decision to employ thrombectomy devices should be individualized based on angiographic thrombus burden, flow characteristics, and response to initial interventions. This algorithmic approach integrates the latest guideline recommendations with practical considerations for optimal patient selection. TASTE was registry-randomized; neurological outcomes were obtained from administrative sources without central adjudication.
“Default pathway: Immediate reperfusion with primary PCI under guideline-directed anticoagulation/antiplatelets; do not use routine aspiration (Class III, LOE A; ESC 2023; ACC/AHA 2025) [13, 14]”.
After wiring and gentle lesion preparation:
If TIMI-3 flow and low thrombus burden
If large thrombus (e.g., TIMI 4–5) or refractory no-reflow/slow-flow despite
vasodilators
Perform aspiration (if chosen): one slow pass; maintain suction during withdrawal; reassess TIMI/MBG/STR.
Evaluate response:
If flow improves to TIMI-3 and the angiographic result is acceptable
If no-reflow persists
Avoid routine rheolytic thrombectomy or distal protection (no proven outcome benefit bailout criteria [10, 11, 12].
Consider single-pass bailout aspiration when:
TIMI thrombus grade 4–5 persists after wiring/gentle lesion preparation;
Refractory noreflow/slowflow despite vasodilators and careful ballooning; or
Recurrent distal embolization despite minimal manipulation. Favor large-caliber, proximal culprit anatomy; avoid highly tortuous/ostial disease with aortic plaque”.
Adjunct imaging (optional): Post-flow OCT/IVUS to assess residual thrombus/plaque and optimize stent sizing/expansion in selected cases.
Expanded Patient Selection Criteria for Bailout Thrombectomy
Anatomical Considerations:
Vessel diameter
Proximal to mid-segment location (avoiding distal vessels).
Absence of severe tortuosity (
Non-ostial location or ostial with minimal aortic atheroma on angiography.
Thrombus Characteristics:
TIMI thrombus grade
Fresh thrombus appearance (hazy, mobile, with contrast penetration).
Persistent after gentle wire manipulation and/or small balloon inflation.
Evidence of distal embolization during initial wire crossing.
Clinical Scenarios:
Acute presentation (
Hemodynamic instability with a large thrombus potentially contributing.
High-risk anatomy (left main, proximal left anterior descending artery (LAD) with large myocardial territory).
Failed pharmacological intervention (persistent TIMI
Contraindications to Consider:
Presentation
Severe calcification is visible on angiography.
Vessel diameter
Extreme tortuosity requiring excessive catheter manipulation.
Heavy aortic arch atheroma (if transfemoral approach).
Technical Requirements:
Operator experience with
Availability of multiple aspiration catheter sizes.
ACT confirmed ACT
Cardiac surgical backup available (though rarely needed).
Device selection for modern bailout techniques.
OCT-guided evaluation: When available, always perform OCT in the initial wire
crossing to help quantify the actual thrombus burden. Thrombus volume
Continuously aspirating systems (CAT RX): There are many considerations for use:
Large proximal vessel thrombus (
Fresh thrombus characterized by high mobility on angiography.
Cases requiring a more extended aspiration time.
Operators with limited manual aspiration techniques.
The technique involves a single pass with continuous –29 inHg suction, advancing and crossing the lesion slowly, maintaining negative suction during the withdrawal phase, and allowing for controlled back bleeding.
Stent retriever systems (Solitaire X): There are many considerations for use:
Very large, organized thrombus (
Has previously failed manual or continuous aspiration.
A thrombus that appears laminated or resilient on imaging.
The technique: nets should be deployed distal to the thrombus; allow 2–3 minutes of integration; retrieve under continuous aspiration vacuum.
Maintain anticoagulation, ACT
Device proficiency and availability: We suggest that institutions optimize
health care by standardizing on a single advanced system (either continuous
aspiration OR stent-retriever), rather than attempting to remain proficient in
multiple devices. Operators with
The trajectory of aspiration thrombectomy—from early promise to routine
adoption and then to decisive downgrading—illustrates the difference between
improving surrogate measures and improving patient outcomes. Initial published
single-center investigations TAPAS [1, 2] and EXPIRA [3] had improvements in
microvascular surrogates and some possible signals of survival; however, the
following pragmatic multicenter studies TASTE [4, 5] and TOTAL [6, 7] found no
reduction in death, reinfarction, or heart failure with a routine aspiration
strategy (TOTAL also identified an early and sustained increase in stroke [9].
Device-based strategies—rheolytic thrombectomy in AIMI [10] and JETSTENT [12],
and distal protection in EMERALD [11]—were no better for hard outcomes;
intracoronary pharmacology in AIDA STEMI [23] and INFUSE AMI [24] identified
mechanistic benefits but no reduction in clinical events; and deferring four
weeks to stenting with a high hemorrhagic risk in DANAMI 3 DEFER [26] did not
improve outcomes. Investigator-level meta-analyses (
Several non-mutually exclusive mechanisms could explain why aspiration may be harmful in an all-comer STEMI strategy:
Aortic/ostial plaque disturbance and air embolization: Catheter exchanges at the coronary ostia and in the aortic root may dislodge atheroma or introduce microbubbles if the system is not perfectly purged, providing a plausible pathway for cerebral emboli (consistent with the stroke signal in TOTAL) [6].
Thrombus fragmentation with distal embolization: Negative pressure applied to laminated thrombus can shear and disperse clot fragments into the microcirculation when engagement is suboptimal, paradoxically worsening MVO despite epicardial patency.
Pressure-gradient and flow-field effects: Rapid aspiration can transiently alter local hemodynamics, potentially collapsing fragile channels or dislodging debris downstream.
Device-specific concerns (rheolytic): High-velocity jets can cause hemolysis and endothelial trauma. In AIMI, a larger infarct size raised the possibility that indiscriminate rheolysis exacerbates distal embolization [10].
PCI procedure time was modestly longer with routine thrombectomy in TOTAL (median 39 vs 35 min), and more aggressive guide manipulation or catheter exchanges may predispose to aortic plaque disturbance and paradoxical systemic embolization [9].
These mechanisms underscore why a selective, carefully executed bailout approach—rather than routine use—is more defensible.
Progress likely depends on smarter selection and better tools:
Enriched RCTs in very-high thrombus burden: Randomize after initial wiring/flow restoration, using standardized TIMI thrombus grading and core-lab adjudication. Hard outcomes plus mechanistic endpoints (CMR infarct size, MVO) should be co-primary.
Imaging-guided selection: Evaluate OCT- or IVUS-confirmed large thrombus and plaque morphology to identify phenotypes most likely to benefit from mechanical extraction.
Device innovation and technique: Test single-pass, continuous-vacuum protocols; compare modern large-lumen aspiration vs stent-retriever approaches in prespecified high-risk anatomies; build in systematic stroke surveillance with neurological assessment.
Therapy integration: Optimize combinations with potent antithrombotics and vasodilators; pre-specify rescue pharmacology for no-reflow to minimize repeated device passes.
Without proven clinical benefit in unselected populations, with a small but non-zero stroke risk, routine aspiration is unlikely to be cost-effective. Device costs, additional procedure time, and potential downstream costs of periprocedural stroke may outweigh any theoretical gains in surrogate markers. A selective bailout strategy concentrates device use in patients with the highest pretest probability of net benefit, which is economically and clinically rational pending definitive randomized evidence.
Routine manual aspiration thrombectomy during primary PCI in STEMI does not improve clinical outcomes and carries a small but significant stroke risk; it is not recommended (Class III, LOE A) [4, 5, 8, 13, 14]. Selective aspiration may be considered when a large thrombus or refractory no-reflow jeopardizes reperfusion (Class IIb) [13, 14]. Rheolytic thrombectomy and distal protection offer no proven benefit [10, 11, 12]. Emerging continuous aspiration and stent-retriever technologies are promising but unproven [20, 21, 22]. The cornerstone remains rapid PCI with optimized pharmacotherapy. In unselected STEMI, the net clinical signal disfavors routine aspiration because an early and persisting stroke hazard offsets any theoretical microvascular benefits. Selective, single-pass bailout may be reasonable in very high thrombus burden with refractory no-reflow, provided meticulous technique and anticoagulation are ensured [4, 5, 6, 7, 8, 9, 13, 14, 18].
STEMI, ST-segment elevation myocardial infarction; MVO, Microvascular obstruction; PCI, Percutaneous coronary intervention; TAPAS, Thrombus Aspiration during Percutaneous Coronary Intervention in Acute Myocardial Infarction Study; EXPIRA, Thrombectomy With Export Catheter in Infarct-Related Artery During Primary Percutaneous Coronary Intervention; TASTE, Thrombus Aspiration in ST-Elevation Myocardial Infarction in Scandinavia; TOTAL, Trial of Routine Aspiration Thrombectomy with PCI versus PCI Alone in Patients with STEMI; HR, Hazard ratio; CI, Confidence interval; ESC, European Society of Cardiology; ACC/AHA, American College of Cardiology/American Heart Association; TIMI, Thrombolysis in Myocardial Infarction; MBG, Myocardial blush grade; STR, ST-segment resolution; SANRA, Scale for the Assessment of Narrative Review Articles; RCT, Randomized controlled trial; HF, Heart failure; CMR, Cardiac magnetic resonance; NYHA, New York Heart Association; OCT, Optical coherence tomography; NNH, Number needed to harm; ARI, Absolute risk increase; AIMI, AngioJet rheolytic thrombectomy before direct Infarct artery stenting in patients with acute Myocardial Infarction; JETSTENT, AngioJet Rheolytic Thrombectomy Before Direct Infarct Artery Stenting; MACE, Major adverse cardiac events; EMERALD, Enhanced Myocardial Efficacy and Recovery by Aspiration of Liberated Debris; IC, Intracoronary; IV, Intravenous; AIDA-STEMI, Abciximab Intracoronary versus Intravenous Drug Application in STEMI; INFUSE-AMI, Intracoronary Abciximab and Aspiration Thrombectomy in Patients With Large Anterior Myocardial Infarction; T-TIME, A Trial of Low-Dose Adjunctive Alteplase During Primary PCI; DANAMI, Danish Study of Optimal Acute Treatment of Patients with STEMI; ACT, Activated clotting time; IVUS, Intravascular ultrasound; SVG, Saphenous vein graft; PPCI, Primary percutaneous coronary intervention; LAD, Left anterior descending artery; OR, Odds ratio; RR, Relative risk; TIA, Transient ischemic attack; LOE, Level of evidence.
MT designed the research study, performed the research, analyzed the data, and drafted the manuscript. MT has read and approved the final manuscript and has participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
The author acknowledges the use of BioRender for creating Figs. 1,2, and the use of Claude (Anthropic) to assist with the layout of Fig. 3. The author takes full responsibility for the content of this manuscript.
This research received no external funding.
The author declares no conflict of interest. Marek Tomala has a financial relationship with the Clinical Research Center Intercard. However, the company had no role in the handling or conduct of the study. The author had full access to all data in the study and take full responsibility for the integrity of the data and the accuracy of the data analysis.
Language editing assistance was provided using AI-based tools. After using this tool, the author reviewed and edited the content as needed and takes full responsibility for the content of the publication.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.