




 , Brandon E Ferrell 1, Tadahisa Sugiura 1, Stephen M Spindel 1,*
, Brandon E Ferrell 1, Tadahisa Sugiura 1, Stephen M Spindel 1,*
1 Department of Cardiothoracic and Vascular Surgery, Montefiore Medical Center, Bronx, NY 10467, USA
Abstract
The Ross procedure is ideal for children and young adults that require an aortic valve replacement; However, long-term autograft durability remains a concern. Numerous techniques revolving around supporting the autograft have been developed with the goal of preventing dysfunction and subsequent reoperation. Short- and long-term results of various supported Ross techniques are promising and demonstrate significant autograft preservation. Further work is needed to determine the optimal surgical approach.
Keywords
- Ross procedure
- aortic valve replacement
- pulmonary autograft
- Florida Sleeve
Introduced over a half century ago, the Ross procedure is an excellent option for aortic valve replacement in pediatric patients and young adults [1]. It has gained significant popularity in the recent years with literature demonstrating longevity, low reintervention rates, and improved survival. Although the autograft is durable, significant concern remains for dilatation of the neoaortic root and subsequent insufficiency [2]. Risk factors including preoperative aortic regurgitation and aortic root dilatation, as well as bicuspid aortic valve, all contribute to the likelihood of reintervention. Patients with the aforementioned risk factors would typically not be ideal candidates for the Ross, however modifications to limit reintervention were developed [3, 4]. Since then, further techniques have been described all with one common goal—to eliminate neoaortic root dilation and subsequent insufficiency [5, 6]. This review will discuss various techniques of the “supported” Ross as well as long-term data.
A main concern with the Ross procedure is the long-term stability of the pulmonary autograft, especially in those with aortic insufficiency which increases risk of recurrent dilation and regurgitation [7]. The procedure was initially described using the sub-coronary technique. However, it became apparently challenging in those with bicuspid aortic valves, especially those with sinus and commissure asymmetry.
Initially created to reinforce the aortic root, particularly in patients with aortic insufficiency when the aortic valve could be spared, the Florida sleeve technique involves placing sub annular sutures and then placing a graft over the aortic root to downsize it [8]. When long term outcomes were analyzed, results were promising and revealed safe and durable treatment with long term survival at 93% in 8 years and freedom from reoperation at 98% [9]. A modified technique was then used for Ross procedure, providing reinforcement to the annulus, sinus, and sinotubular junction when implanting the pulmonary autograft (Fig. 1, Ref. [10]). The initial root reinforcement steps are similar to the David procedure where the aortic root base is dissected and sub-annular sutures are placed. The Valsalva aortic root graft is sized based on the diameter of the autograft. The autograft proximal anastomosis is completed and the subannular sutures are passed through the Valsalva graft, stabilizing the annulus. Tear-drop slits are created in the graft for coronary buttons which are then implanted. The ascending aorta is replaced with a straight graft and the components of the Valsalva graft are brought back together, encompassing the autograft. This support system reinforces the annulus, Sinus of Valsalva, and sinotubular junction. The Seattle Shawl is a near identical technique which was created at the same time as this Florida Sleeve Ross approach [10, 11].
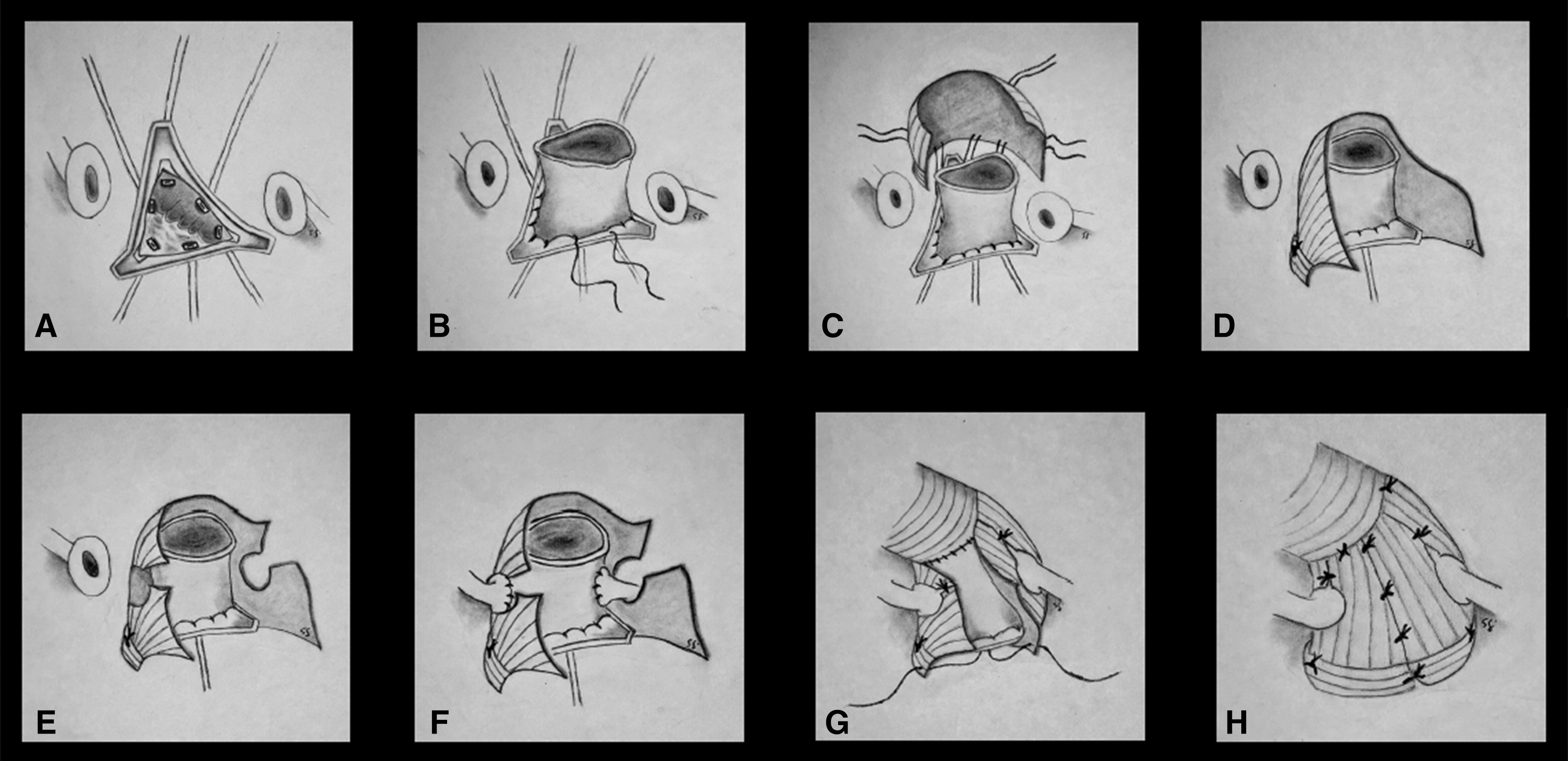 Fig. 1.
Fig. 1.
Stepwise root reinforcement method for the Florida Sleeve Ross procedure. (A) Subannular sutures are placed in the left ventricular outflow tract. (B) The autograft proximal anastomosis is completed. (C) Five of the 6 subannular sutures are passed through the bulged root graft. (D) These 5 annular support sutures are tied. (E) Slits with apertures are created in the bulged root graft for the coronary buttons. (F) The coronaries are reimplanted. (G) The ascending aorta is replaced and after cross clamp removal the sixth subannular suture is passed through the root graft and tied. (H) The divided components of the root graft are loosely approximated with interrupted sutures and the distal portions are tacked to the ascending aortic graft. Reprinted from A simplified reinforcement: The Florida sleeve Ross procedure, Spindel, Stephen M. et al. [10]. JCTVS Techniques, Volume 25, 24–27. Copyright 2024 with permission from Elsevier.
Sir Yacoub went on to describe the Ross as a total root replacement which now exposed the pulmonary autograft to systemic pressure [7, 12]. However, the freestanding autograft root replacement technique became the technique of choice because of a lower risk of early autograft insufficiency and failure. There are some long-term results that have revealed that the freestanding autograft root replacement technique is associated with a higher risk of autograft dilatation and insufficiency [13].
In 1994, Pacifico and colleagues [14] partially or completely wrapped the autograft with glutaraldehyde-fixed bovine pericardium with hopes of stabilizing the neoaortic root. With the goal of preventing post operative aortic insufficiency, Mortiz et al. [15], reduced the diameter of the aortic annulus and wrapped the pulmonary autograft with absorbable mesh. Similarly, Skillington et al. [16, 17], described methods of inserting the autograft as a root replacement, with the native aorta enclosed around it, eventually to be known as the inclusion cylinder technique (Fig. 2, Ref. [7]). In 2000, David and colleagues [18] supported an inclusion cylinder technique over the aortic root replacement technique in patients with a bicuspid aortic valve, a proven risk factor associated with increased dilation of sinuses of Valsava and sinotubular junction.
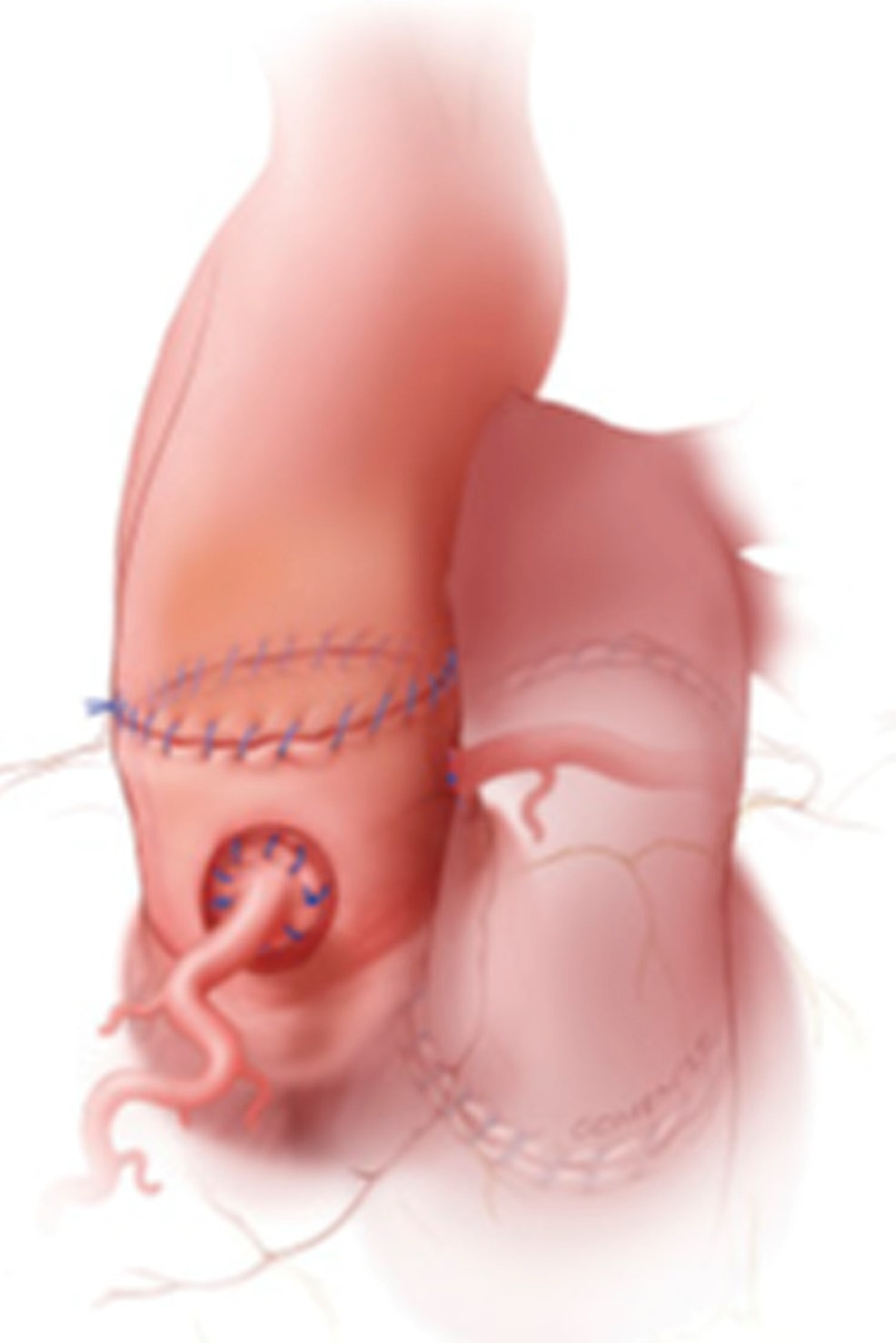 Fig. 2.
Fig. 2.
Full root replacement – autologous inclusion technique. Reprinted from Late Pulmonary Autograft Dilation: Can We Make a Good Operation Great? The Tailored Approach, El-Hamamsy, Ismail et al. [7], Seminars in Thoracic & Cardiovascular Surgery: Pediatric Cardiac Surgery Annual, Volume 27, 42–46. Copyright 2024 with permission from Elsevier.
One of the most widely used modifications was described by Slater et al. [3], where the autograft was encased in a woven polyester tube graft with the coronaries sewn to all layers which demonstrated excellent short term valve function without annular or sinotubular dilatation. Data revealed that patients who underwent supported Ross were less likely to have neoaortic root dilatation compared to unsupported Ross patients [19]. Similarly, Carrel et al. [20], inserted the autograft in a vascular prosthesis with an artificial Valsalva (Fig. 3, Ref. [7]). The purpose of this is to allow for physiologic flows and pressures. The coronaries are re-implanted with suture between coronaries and autograft only with the goal of avoiding blood accumulation between the autograft and vascular graft in the early postoperative period. In 12 patients, short term follow-up revealed 100% freedom from reoperation and absence of aortic insufficiency in 11 patients after a mean follow up of 11 months [20].
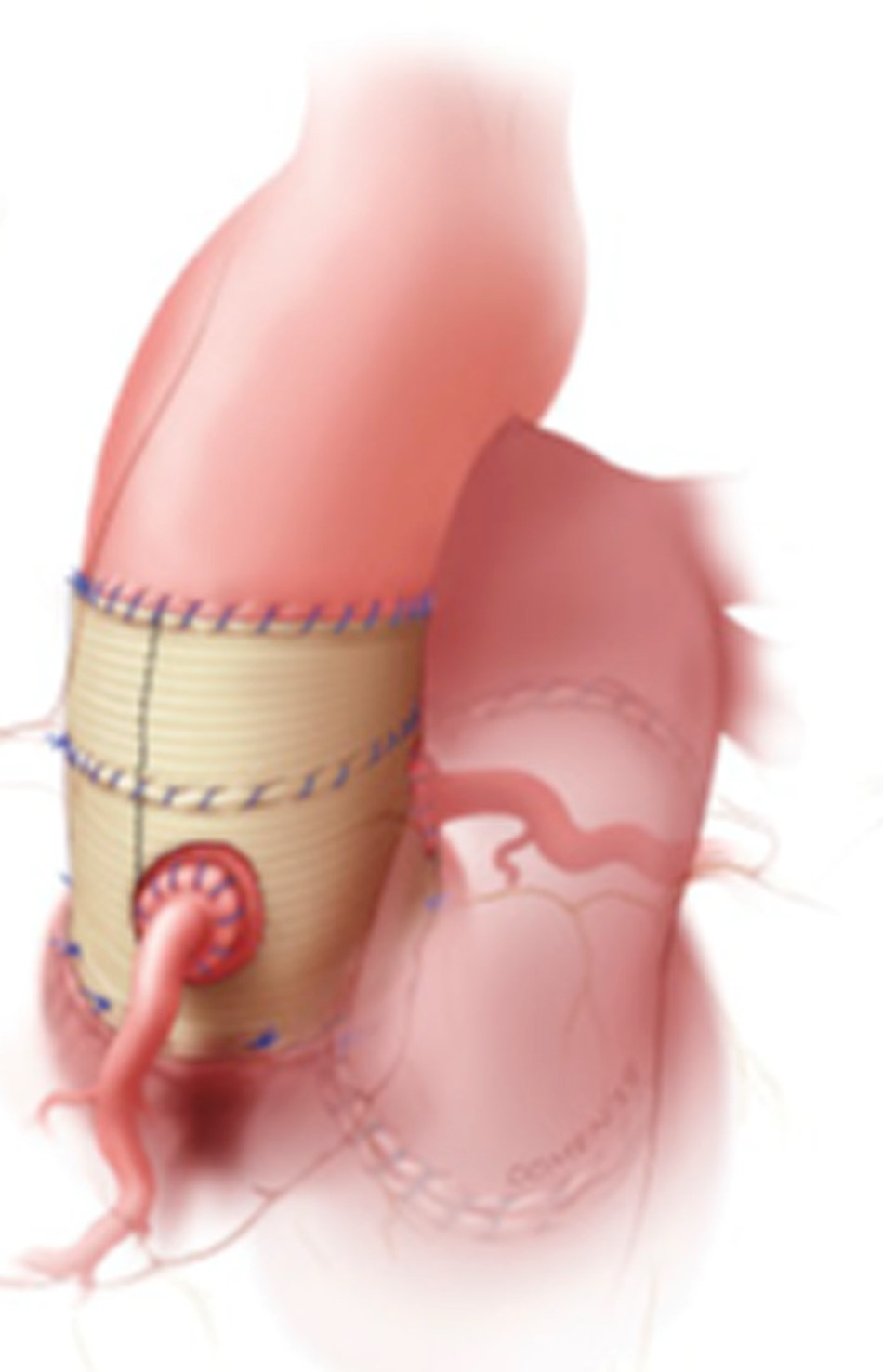 Fig. 3.
Fig. 3.
Dacron inclusion technique, with complete external support by a dacron graft. Reprinted from Late Pulmonary Autograft Dilation: Can We Make a Good Operation Great? The Tailored Approach, El-Hamamsy, Ismail et al. [7], Seminars in Thoracic & Cardiovascular Surgery: Pediatric Cardiac Surgery Annual, Volume 27, 42–46. Copyright 2024 with permission from Elsevier.
The idea of a tailored surgical approach was further supported by Bouhout
et al. [21], which appeared to mitigate early dilatation of the
autograft root in patients with aortic insufficiency by stabilizing the annulus,
sinus of Valsalva, STJ, and ascending aorta to a short interposition woven
polyester graft (Fig. 4, Ref. [7]). Ross procedures were performed with a total
root replacement technique. Surgical technique detailed in their paper revealed
that during autograft harvesting, infundibular muscle was trimmed to 2–3 mm
below the cusp insertion line, and the pulmonary root was cut 2–3 mm above the
commissural level to limit pulmonary artery exposure to systemic pressures. The
distal autograft anastomosis was performed 1–2 mm above the STJ to avoid late
dilatation. If the native ascending aorta was
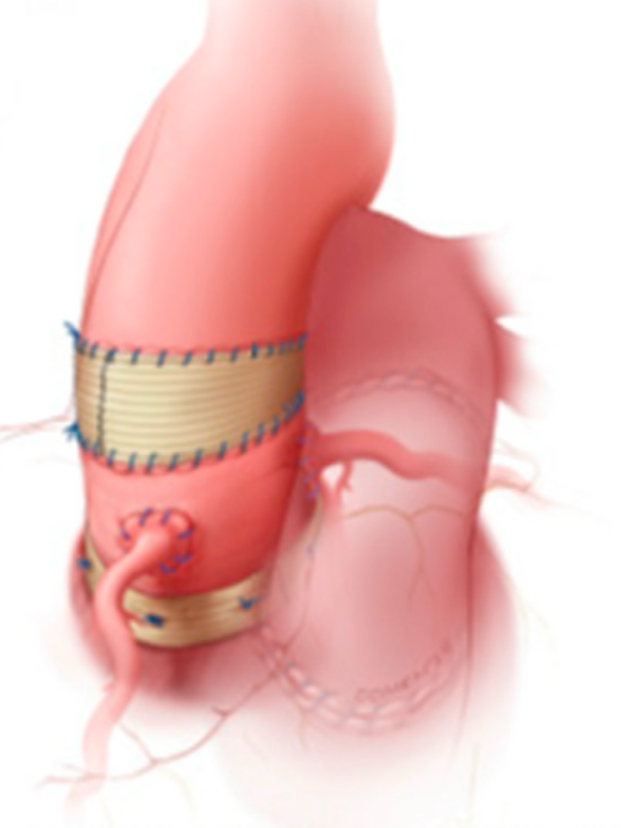 Fig. 4.
Fig. 4.
Tailoring support technique. Extra aortic annuloplasty and interposition graft to support the sinotubular junction and match the distal ascending aorta (sinus support by aortic sinus remnants is not seen). Reprinted from Late Pulmonary Autograft Dilation: Can We Make a Good Operation Great? The Tailored Approach, El-Hamamsy, Ismail et al. [7], Seminars in Thoracic & Cardiovascular Surgery: Pediatric Cardiac Surgery Annual, Volume 27, 42–46. Copyright 2024 with permission from Elsevier.
There have been various supported Ross techniques published for the adult population, and there are also variations in the pediatric population [6]. Redondo and Austin described a technique supporting the Ross autograft with an ExoVasc® personalized external aortic root support [PEARS] (manufactured by Exstent Ltd, UK). It is manufactured from pulmonary artery measurements obtained from computed tomography. In 50 patients with mean follow up of 17 months, there was no evidence of autograft dilation and no significant changes in aortic root and ascending aorta dimensions [22].
It is known in patients with the Ross procedure that neo-aortic root dilatation and neoaortic insufficiency can occur [4, 13]. As mentioned above, multiple techniques have been developed to support the autograft, and in some instances, data has shown that the supported Ross techniques were less likely to have subsequent neoaortic root dilatation when compared to the standard unsupported Ross [13]. Furthermore, unsupported patients or patients who later had support removed in reoperation demonstrated higher rates of autograft dysfunction [2, 23].
Skillington et al. [17] published data on 310 patients who underwent Ross. They adjusted the size of the aortic root to match the pulmonary autograft which was inserted as a root replacement. The aorta was then closed around the graft to provide autologous support with subsequent external ring annuloplasty fashioned from woven polyester graft for further support. The mean follow-up period was 9.4 years. At 16 years, the actuarial survival rate was 97%. Freedom from composite of all reoperations on the aortic valve and late aortic regurgitation greater than mild was 95% at 5 years, 94% at 10 years and 93% at 15 years [17]. Patients presenting with predominant aortic stenosis had better results when compared to those with aortic regurgitation which has been shown to be a risk factor for post-Ross aortic insufficiency [2]. When examining long-term freedom from reoperation, Charitos et al. [12], found that those undergoing a supported Ross with root replacement or subcoronary technique had significantly improved freedom from reoperation at 10 years compared to an unsupported root replacement Ross technique. When specifically examining patients who underwent a root replacement technique, the annulus supported group remained stable for the first ten years in contrast to the unsupported group where aortic insufficiency increased at a 6-fold rate [12].
Carrel and Kadner [24] utilized a technique first introduced by Slater and colleagues which included external reinforcement of the autograft by inserting it into a prosthetic woven polyester graft. Since 2006, 22 patients underwent Ross, the majority with aortic stenosis and one patient requiring aortic valve replacement in the early postoperative period. The remaining 21 patients did not require reoperation. There was no evidence of more than trivial aortic regurgitation in 15 patients after a mean of 70 months and no autograft dilatation was observed during follow up. These results were encouraging, proving that the autograft valve was well functioning in all cases many years after the index operation [24]. Similarly, another group’s technique included pulmonary autograft reimplantation in a woven polyester conduit using David’s valve sparing root replacement technique in patients with preoperative aortic insufficiency and ascending aortic dilation. At a mean of 90 months, survival was 100%. 5- and 10-year survival rates with no repeat procedures were 84% and 82%. Survival from aortic reintervention was 95% at 5 years and similar at 10 years. Ultimately, long-term follow-up data showed stable neo-aortic valve function [25].
de Kerchove et al. [26] examined 218 patients that underwent the Ross
procedure. 68% had a root replacement and 32% underwent the inclusion
technique, in which the autograft root is incorporated as a cylinder within the
native aortic root. At 10 years, freedom from autograft reoperation was 81% in
the root group and 84% in those that underwent the inclusion technique. Ten-year
freedom from proximal aorta dilatation greater than 40 mm were 57% and 80%
respectively. Ten-year freedom from moderate or greater regurgitation was 73%
In a single surgeon study, 129 adults with bicuspid aortic valves underwent the Ross procedure and were divided into those without autograft inclusion (unwrapped) and those with autograft inclusion (autograft within vascular conduit). The pulmonary autograft was mounted inside a tubular woven polyester graft before implantation eliminating the need to alter the anatomy of the aortic root to match that of the pulmonary autograft [27, 28]. With a median follow-up of 10.3 years, ten-year survival was 95.6% and 100% in unwrapped versus wrapped cohorts. Autograft valve failure occurred in 35% and 5% of the respective cohorts. At 10 years, reintervention occurred in 26.8% of the unwrapped cohort and 4.0% of the wrapped cohort [27]. In patients that underwent the supported Ross procedure with a Valsalva graft, freedom from root dilation longer than10 years was observed [29].
In children undergoing Ross operation, Donald et al. [6], placed a poly-p-dioxanone filament around the STJ to match the diameter of the aortic annulus. With a mean follow-up time of 8.9 years, freedom from moderate or greater aortic insufficiency was 100% at 10 years, compared to 83.1% in the unbanded cohort [6]. Similarly, in another study, fifteen adolescent patients underwent a modified Ross procedure where the autograft was wrapped using 0.1 mm Gore Preclude. The mean follow-up period was 15 years. During the follow-up, one patient required aortic valve reoperation due to prolapsed cusps. At follow-up echocardiography, thirteen patients had mild aortic valve insufficiency, and two patients had moderate homograft stenosis. There were no significant differences STJ, aortic root diameter, or annulus [5].
The Ross procedure provides excellent functional results in young and middle-aged adults requiring an aortic valve replacement. The pulmonary autograft is the sole aortic valve substitute that ensures long-term viability of the aortic root, however, there remains a concern for postoperative autograft dilatation and aortic insufficiency and ultimately reoperation.
There have been many studies showing the success of the unsupported Ross
procedure with various techniques of autograft implantation [30, 31, 32, 33, 34]. Kumar
et al. [35], used the root replacement technique with coronary artery
implantation and did not appreciate autograft dilation in patients with bicuspid
aortic valve or in older patients with rheumatic disease and isolated aortic
valve pathology. At 10 years, freedom from reoperation overall was 80% and over
95% in non-rheumatics, highlighting proper patient selection is crucial for
minimizing reoperation. Their team did not perform Ross on those with aortic
annulus larger than 30mm on transesophageal echo, young (
Two years later, Brown and colleagues [37] further examined their Ross patients and found that freedom from autograft reoperation at 15 years was significantly improved for patients undergoing Ross AVR after 2000 compared with patients operated on before 2000 (99% vs 87%; p = 0.001). Regarding autograft root dilation, the group was routinely fixing the sinotubular junction and autograft annulus or replacing dilated aorta if larger than 35 mm. Of note, 80% of patients had bicuspid aortic valve which was not associated with the small patient population that developed long term complications. Their data suggested that long-term complications such as autograft regurgitation or sinus/ascending aortic dilatation can be prevented with a myriad of techniques including replacing the dilated ascending aorta at the time of the initial Ross procedure, external fixation of the autograft annulus or sinotubular junction, and treatment of postoperative hypertension.
Although reoperation is a possibility due to a variety of factors such as technique, preoperative and progressive AI, or size mismatch of pulmonary autograft, the aforementioned studies reflect excellent unsupported Ross outcomes revealing the importance of identifying appropriate Ross candidates, surgical technique and medical management impacting the patient long-term. However, the need for reoperation remains a true possibility for patients undergoing the Ross procedure. Literature suggests that patients with preoperative aortic insufficiency are at higher risk of autograft dilatation and reintervention than those with aortic stenosis, even with annular and STJ reinforcement and replacement of the dilated ascending aorta [38, 39]. David et al. [38] found that in a population aged 16–63, regardless of technique (subcoronary implantation or root replacement) there was a cumulative incidence of Ross-related reoperations 16.8% at 20 years. Patient selection and factors such as preoperative aortic root dilation and AI more than AS are all contributing factors and markers for long term failure. Although various techniques have significantly reduced Ross reintervention for some institutions, others have found success with variations of the supported Ross.
When comparing root replacement versus inclusion cylinder technique, de Kerchove and colleagues [26] found that in the root group, dilatations were more likely in the autograft sinuses or STJ, whereas in the inclusion group, dilatations more likely affect the ascending aorta. For root replacement, autograft dilatation was the main cause of failure and interestingly for the inclusion group, autograft valve prolapse was the main cause of failure [26]. Long-term autograft failure in some supported Ross patients has caused some groups to advocate for a more tailored approach with the goal of maintaining the natural physiology and relationship between autograft components [7, 21]. A multitude of surgical techniques encompassing the supported Ross detailed in this review all play a role in reducing long-term autograft failure and ultimately reoperation. The data and literature suggest that the supported Ross could be one more tool in the toolbox for Ross surgeons. It is important to consider that the long-term supported versus unsupported Ross data reflects single-center experiences which may suggest that surgeon experience, technique and/or small variations in patient selection may heavily affect these outcomes. The Ross is an intimate procedure that has evolved over time, driven by a deeper understanding of the anatomical and physiological factors. Further data is requisite to determine the optimal approach to minimize reoperation and long-term dysfunction of the autograft.
The Ross procedure is an excellent option in children and young adults requiring aortic valve replacement. Although various implantation techniques and modifications have been developed, there is no universal method to reducing long-term autograft failure and Ross reintervention. The supported Ross techniques discussed reveal promising long-term outcomes. However, it is likely that patients would benefit from a tailored approach, with supported Ross being one of many techniques that can be utilized to minimize long-term autograft dysfunction.
AC, BF, TS, and SS were involved in conception and design of the review. All authors drafted the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest. Tadahisa Sugiura is serving as one of the Editorial Board members of this journal. We declare that Tadahisa Sugiura was not involved in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Ferdinand Aurel Vogt and Curtis G Tribble.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.