



 , Shanshan Lv 1,†, Guixia Li 1, Anzhao Ma 2, Xuying Guo 1, Shuangyan Jiang 1, Jing Zheng 1,*
, Shanshan Lv 1,†, Guixia Li 1, Anzhao Ma 2, Xuying Guo 1, Shuangyan Jiang 1, Jing Zheng 1,*
1 Cardiac Surgery Intensive Care Unit, Shandong Provincial Hospital Affiliated to Shandong First Medical University, 250021 Jinan, Shandong, China
2 Shandong Province Ji Nan Huaiyin District Municipal Center for Disease Control and Prevention, 250022 Jinan, Shandong, China
†These authors contributed equally.
Abstract
This study aimed to investigate the clinical effects of early recruitment maneuver (RM) combined with prone position (PP) in improving acute respiratory distress syndrome (ARDS) after aortic dissection (AD) surgery.
A before-and-after single-arm interventional study was conducted to collect data on patients with Stanford type A aortic dissection (STAAD), who underwent surgical treatment from April 2017 to October 2023 in the Department of Cardiac Major Vascular Surgery, a teaching hospital in China. Comparisons of hemodynamic indices, changes in respiratory parameters, and adverse events were performed at six time points: before the intervention, immediately after early RM combined with PP, and at 30 min, 1 h, 2 h, and 4 h thereafter.
A total of 41 patients (80.49% male; mean age 49.05 ± 11.64 years) were included. Following early lung recruitment combined with prone positioning, PaO2 increased from 66 mmHg at baseline to a peak of 102 mmHg post-intervention at 1 hour, and the PaO2/FiO2 ratio improved from 95 mmHg to 154 mmHg, indicating enhanced oxygenation. PaCO2 remained stable throughout the observation period. FiO2 initially increased from 60% to 70% and returned to baseline levels, while SpO2 improved from 94.5% to 97%, demonstrating a sustained improvement in peripheral oxygen saturation. Hemodynamic parameters, including heart rate and central venous pressure, remained largely stable. All changes in oxygenation indices were statistically significant (p < 0.001 following the Friedman test).
Early lung recruitment combined with prone positioning significantly improved oxygenation in post-operative ARDS patients with STAAD, as evidenced by increased PaO2 and PaO2/FiO2 ratios. These benefits were achieved without significant changes in PaCO2, heart rate, or lactate levels, suggesting that this strategy enhances gas exchange while maintaining hemodynamic stability.
Keywords
- aortic dissection
- acute respiratory distress syndrome
- prone position
- ventilation
Aortic dissection is a condition characterized by the tearing of the intima and media of the aorta due to various causes, leading to the separation of the intima from the media. Blood flows between these layers, resulting in the division of the aortic lumen into true and false lumens. This disease progresses rapidly and has a high mortality rate [1, 2, 3]. Due to differences in the extent of involvement, aortic dissection can be classified according to the Stanford classification into Type A and Type B. Stanford type A aortic dissection (STAAD) involves the ascending aorta, whereas Type B aortic dissection (TBAD) originates from the descending thoracic aorta but does not involve the ascending aorta [4, 5, 6]. Surgical treatment is currently the most effective method for treating patients with STAAD. Research has shown that hypoxemia, characterized by respiratory failure, is a common complication of STAAD surgery. Prolonged postoperative hypoxemia (Acute Respiratory Distress Syndrome, ARDS) can lead to damage in the lungs and other organs, thereby increasing perioperative mortality [7]. Therefore, it is crucial to actively prevent hypoxemia after surgery for aortic dissection. Ventilation in the prone position (PP) is one of the important methods for treating hypoxemia [8]. Lung recruitment (Recruitment manoeuvre, RM) refers to a treatment method where, during mechanical ventilation, a pressure higher than the average airway pressure is briefly applied to expand the lungs, promoting the opening of collapsed alveoli, thus improving the patient’s oxygenation and enhancing lung compliance [9]. However, there is currently controversy over whether lung recruitment can be used as a treatment method after cardiac surgery [10].
To study the clinical application effect of early lung recruitment combined with prone positioning ventilation in improving hypoxemia in patients after aortic dissection surgery, we conducted a retrospective analysis and summary of the efficacy of patients with ARDS following acute STAAD surgery who underwent early lung recruitment combined with prone positioning ventilation in our unit, in order to provide relevant experiential measures for clinical practice.
In this before-after/single-arm interventional study, changes in respiratory parameters and hemodynamics before and after early lung recruitment and prone position ventilation were investigated in patients with acute Stanford Type A aortic dissection who underwent surgical treatment at a Hospital in China from April 2017 to October 2023.
Patients were screened for eligibility according to the following inclusion and
exclusion criteria: Inclusion criteria: (1) Age
In this protocol, selected patients underwent lung recruitment combined with prone ventilation within 6 hours after surgery. All patients underwent early lung recruitment with the PEEP titration method under ventilator assistance, combined with patient blood gas analysis results, ensuring hemodynamic stability, with one RM performed at 1 hour and 4 hours, respectively.
Patient mechanical ventilation parameter settings: The synchronized intermittent mandatory ventilation (SIMV) mode was used, with a tidal volume (VT) of 6~8 mL/kg, PEEP of 5 cmH2O, and a respiratory rate of 12 breaths per minute.
Early Lung Recruitment Strategy: Before performing recruitment maneuvers (RM), patients should have a bedside chest X-ray or computed tomography (CT) to assess the potential for lung recruitment. Patients should be in a fully sedated state (with a richmond agitation-sedation scale (RASS) score of –3 to –5) and should not be breathing spontaneously. Set the peak pressure alarm limit to 40 cmH2O and the PEEP alarm limit to 20 cmH2O. In pressure-controlled ventilation (PCV), maintain the difference between inspiratory pressure and PEEP constant. Incrementally increase PEEP by 5 cmH2O every 30 seconds up to 20 cmH2O, maintaining ventilation for 2 minutes after each increase. Subsequently, employ a decremental method to titrate PEEP, maintaining tidal volume at 5 mL/kg. Decrease PEEP by 2 cmH2O every 2 to 3 minutes, selecting the optimal PEEP as determined for the patient.
Prone Position Ventilation Procedure: The classical method for prone positioning is adopted for prone position ventilation [11]. Based on the actual situation in our department, the following protocol has been formulated. Once the patient is transitioned to prone ventilation and hemodynamics are stable, lung recruitment maneuvers are performed at 1 hour and 4 hours, as detailed in Table 1.
| Standing position | Character | Division of labor and responsibilities |
| Position 1 | Physician or Respiratory Therapist | Stand at the head side of the patient, responsible for commanding the team and coordination, securing the tracheal intubation, and protecting the ventilator tubing. |
| Position 2 | Charge Nurse | Stand on the right side of the patient’s neck and shoulder, responsible for protecting the drainage tubing, such as central venous catheters, chest drainage tubes, and arterial catheters. Also, monitor the patient’s monitoring equipment and changes in the ventilator. |
| Position 3 | Nurse | Stand on the left side of the patient’s neck and shoulder, responsible for protecting the drainage tubing, such as central venous catheters, chest drainage tubes, arterial catheters, and urinary catheters. |
| Position 4 | Nurse | Stand on the right side of the patient’s hip and thigh root, assisting in the protection of catheters and drainage tubes such as urinary catheters, abdominal drainage tubes, and thoracic drainage tubes. |
| Position 5 | Nurse | Stand on the left side of the patient’s buttocks and thigh root to assist in protecting the urinary catheter, abdominal drainage tube, and thoracic drainage tube. |
Early Lung Recruitment Combined with Prone Position Termination Criteria:
(1) Oxygen saturation decreases by more than 5% from baseline or is less than 88%;
(2) Heart rate increases by more than 5% from baseline or 15 beats per minute;
(3) Mean arterial systolic pressure drops by more than 5% from baseline or is less than 60 mmHg;
(4) New occurrences of arrhythmias, accidental extubation, drain dislodgement, cardiac arrest, or other life-threatening situations;
(5) Other circumstances determined by the clinical physician to stop treatment.
This includes age, gender, body mass index, smoking history, drinking history, Acute Physiology and Chronic Health Evaluation II (APACHE-II), and surgical-related information, among others.
Dynamic monitoring of the patient’s heart rate (HR), oxygen saturation (SpO2), and central venous pressure (CVP). Records are kept for HR, SpO2, and CVP, as well as lactate levels at various time points: before and after early lung recruitment plus prone ventilation at 30 minutes, 1 hour, and post-ventilation at 2 hours and 4 hours.
Occurrences of respiratory or cardiac arrest, incidence of pressure ulcers, and accidental extubation rates are tracked.
Statistical analyses were performed using SPSS version 27.0 (IBM Corp., Armonk,
NY, USA). Categorical variables are presented as frequency and percentage [n
(%)], whereas continuous variables are expressed as mean
During the study period, researchers conducted a comprehensive analysis of acute aortic dissection surgeries, treating a total of 224 cases. The severity of this condition was evident from the outset, with 5 cases resulting in preoperative mortality due to the critical nature of the dissection itself. Postoperatively, an additional 14 patients succumbed to complications arising from multi-organ failure, highlighting the challenges and risks associated with this complex surgical intervention. In addressing the critical issue of ARDS complicating aortic dissection surgeries, researchers implemented a protocol involving early lung recruitment combined with prone ventilation. This intervention was applied to 41 patients, as detailed in Table 2 of the study. Fig. 1 shows the flowchart of patient selection.
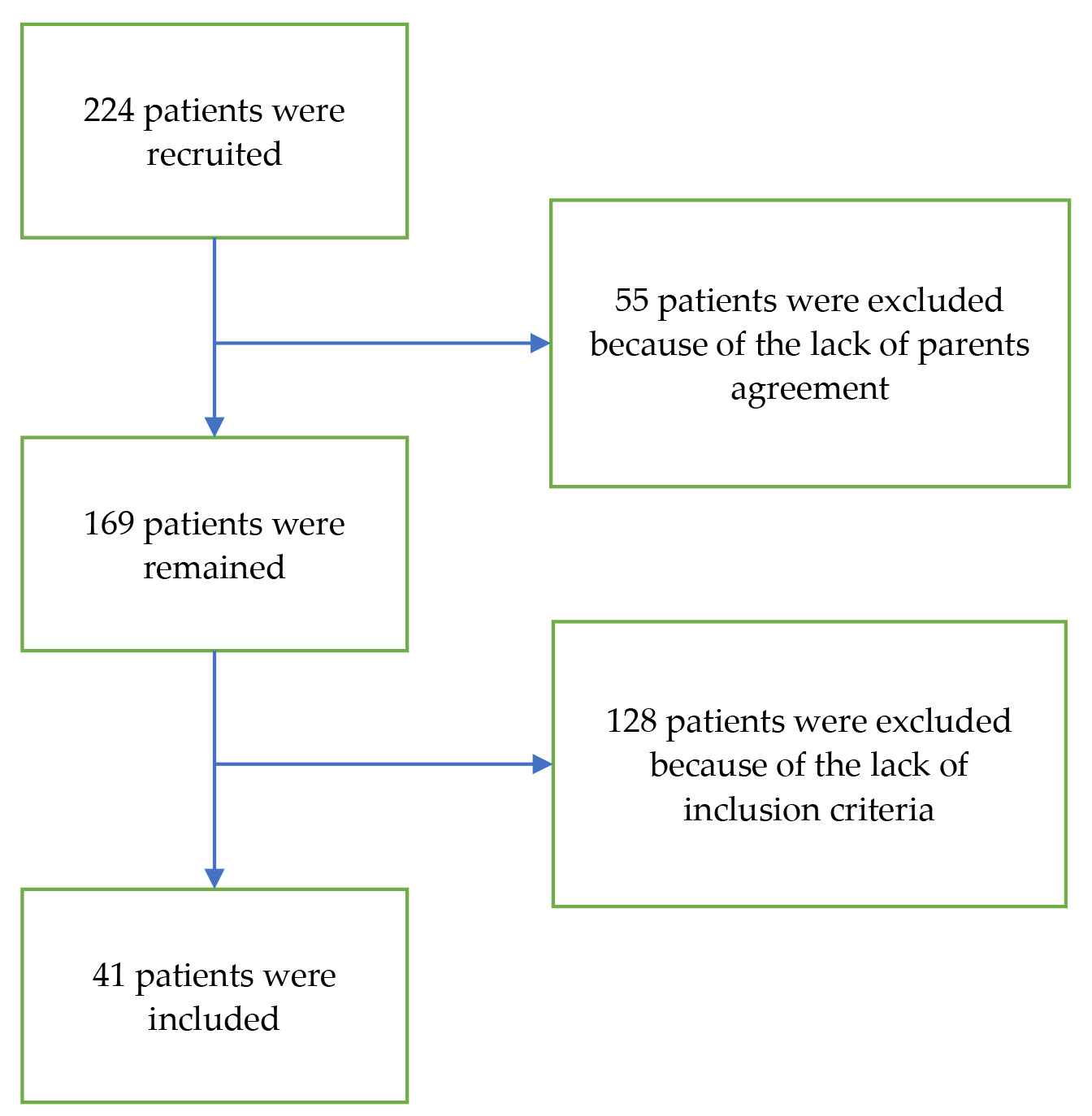 Fig. 1.
Fig. 1.
The flowchart of the participant recruitment.
| Characteristics | Data | |
| Age (years) | 49.05 | |
| Gender | ||
| Male | 33 (80.49%) | |
| Female | 8 (19.51%) | |
| Height (cm) | 172.66 | |
| Weight (kg) | 85.70 | |
| BMI (kg/m2) | 28.71 | |
| History of smoking | 22 (53.66%) | |
| History of drinking | 14 (34.15%) | |
| Basic lung disease | 2 (4.88%) | |
| Diabetes | 9 (21.95%) | |
| Mechanical ventilation time (h) | 58.89 | |
| Postoperative ICU hospitalization time (h) | 182.54 | |
| 24-hour drainage (mL) | 457.08 | |
| Total bleeding volume (mL) | 2225.11 | |
| Death rate | 2 (4.88%) | |
| Aortic cross clamping time (min) | 116 (85, 145) | |
| LVEF (%) | 60 (59, 61) | |
| Cycle stop time (min) | 13 (9.5, 23.5) | |
| Transfer time (min) | 201 (169.5, 236.5) | |
| APACHE II score (Score) | 18 (17, 20) | |
Values are expressed as mean
Table 2 summarizes the baseline characteristics and perioperative clinical data
of the study cohort (n = 41). The mean age of patients was 49.05
Regarding perioperative outcomes, the mean duration of mechanical ventilation
was 58.89
Table 3 presents the temporal changes in respiratory parameters measured at six time points before, during, and after early lung recruitment combined with prone positioning. All values are expressed as median with IQR. Since the majority of variables did not follow a normal distribution (Shapiro–Wilk test), the Friedman test was applied for repeated measures comparisons.
| Respiratory parameters | Time 0 | Time 1 | Time 2 | Time 3 | Time 4 | Time 5 | p-value |
| PaO2 (mmHg) | 66.29 |
84.31 |
102.34 |
94.83 |
94.54 |
90.83 |
|
| PaCO2 (mmHg) | 40.83 |
39.56 |
38.39 |
39.81 |
38.95 |
37.85 |
0.594 |
| PaO2/FiO2 (mmHg) | 98.51 |
125.95 |
153.98 |
156.34 |
158.24 |
158.47 |
|
| FiO2 (%) | 60 (60, 80) | 70 (60, 80) | 60 (60, 72.5) | 60 (60, 60) | 60 (55, 70) | 60 (50, 60) | |
| SPO2 (%) | 94 (92, 95) | 96 (94, 98) | 97 (96, 98.75) | 98 (95.5, 98) | 98 (96, 98) | 97 (96.5, 98) | |
| HR (minute) | 85.29 |
85.71 |
85.85 |
83.76 |
84.42 |
84.63 |
0.816 |
| CVP (cmH2O) | 12.88 |
12.81 |
12.15 |
12.46 |
12.07 |
11.63 |
|
| Lac (mmol/L) | 1.5 (1.0, 5.7) | 1.5 (1.0, 2.8) | 1.3 (0.9, 2.45) | 1.3 (1.0, 2.55) | 1.3 (1.0, 1.95) | 1.2 (1.0, 1.9) | 0.904 |
Time 0: before early lung recruitment, Time 1: 30 minutes After Initiation, Time
2: 1 Hour After Initiation, Time 3: 4 Hours After Initiation, Time 4: 2 Hours
After Completion, Time 5: 4 Hours After Completion. Values are expressed as mean
A significant overall effect of time was observed for PaO2,
PaO2/FiO2 ratio, FiO2 requirement, SpO2, and CVP (p
In contrast, PaCO2, HR, and lactate levels did not change significantly across time points (p = 0.594, p = 0.816, and p = 0.904, respectively), indicating stability of ventilation, hemodynamic status, and metabolic response during the study period.
The line graph depicts the changes in PaO2 (mmHg), PaCO2 (mmHg), and PaO2/FiO2 ratio (mmHg) across six time points before, during, and after early lung recruitment combined with prone positioning. PaO2 increased from 66 mmHg at baseline (Time 0) to 77 mmHg at Time 1 and peaked at 93 mmHg at Time 2, then remained elevated around 90–94 mmHg at subsequent time points. PaCO2 remained relatively stable throughout the observation period, ranging from 37 to 40 mmHg. The PaO2/FiO2 ratio showed a marked improvement from 95 mmHg at baseline to 118 mmHg at Time 1 and progressively increased to 154–157 mmHg by Time 5, reflecting enhanced oxygenation following the intervention (Fig. 2).
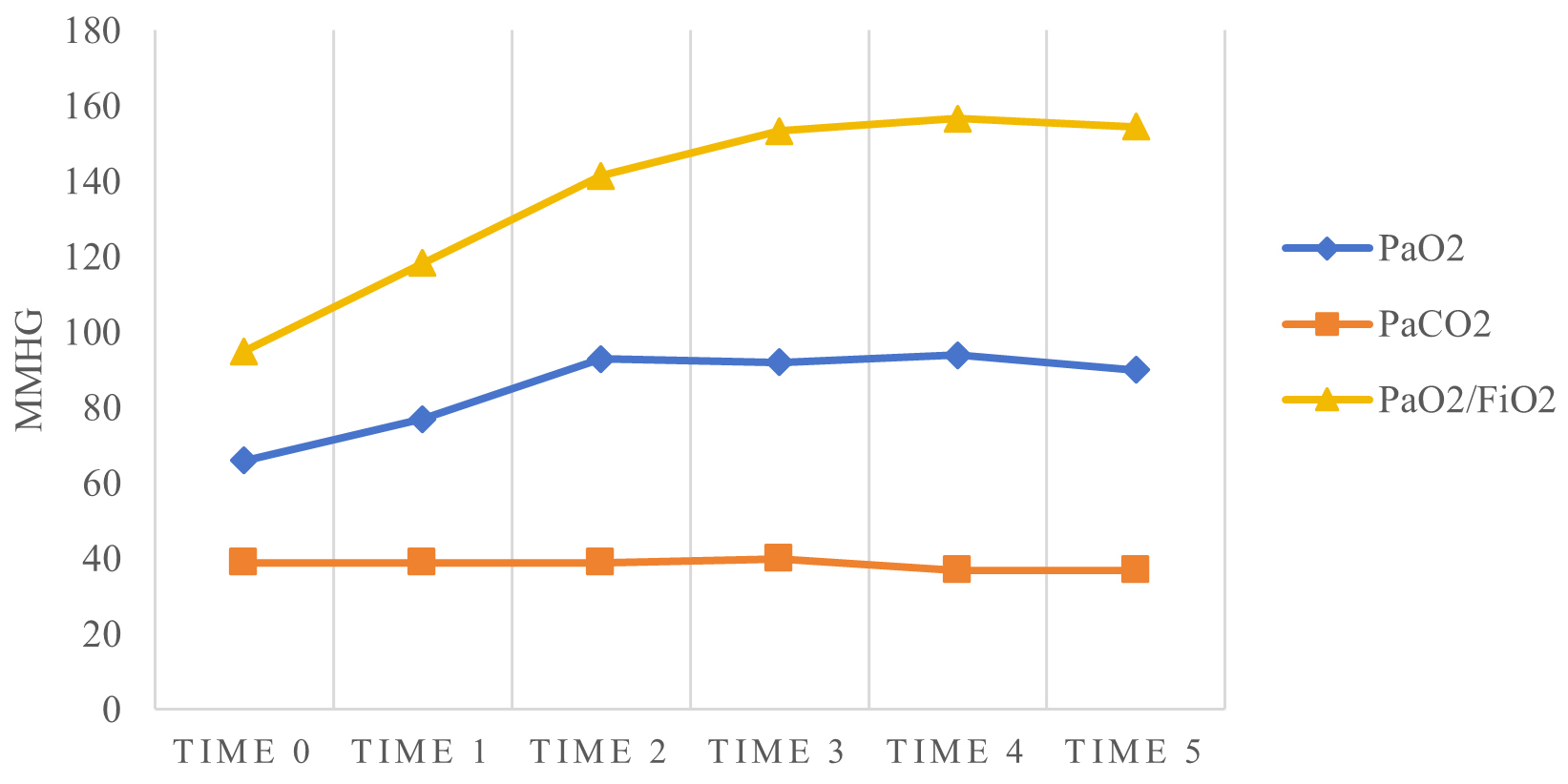 Fig. 2.
Fig. 2.
Temporal changes in PaO2, PaCO2, and PaO2/FiO2 ratio following early lung recruitment and prone positioning.
The line graph illustrates the changes in FiO2 (%) and SpO2 (%) at six consecutive time points during and after early lung recruitment combined with prone positioning. FiO2 initially increased from 60% at baseline (Time 0) to 70% at Time 1 and remained slightly elevated at 69% at Time 2, before returning to 60% from Time 3 onward. Correspondingly, SpO2 improved from 94.5% at baseline to 96% at Time 1 and 97% at Time 2, followed by minor fluctuations at later time points, reaching 97% at Time 5. These trends indicate an early improvement in oxygenation after the intervention, which was largely maintained throughout the subsequent time points (Fig. 3).
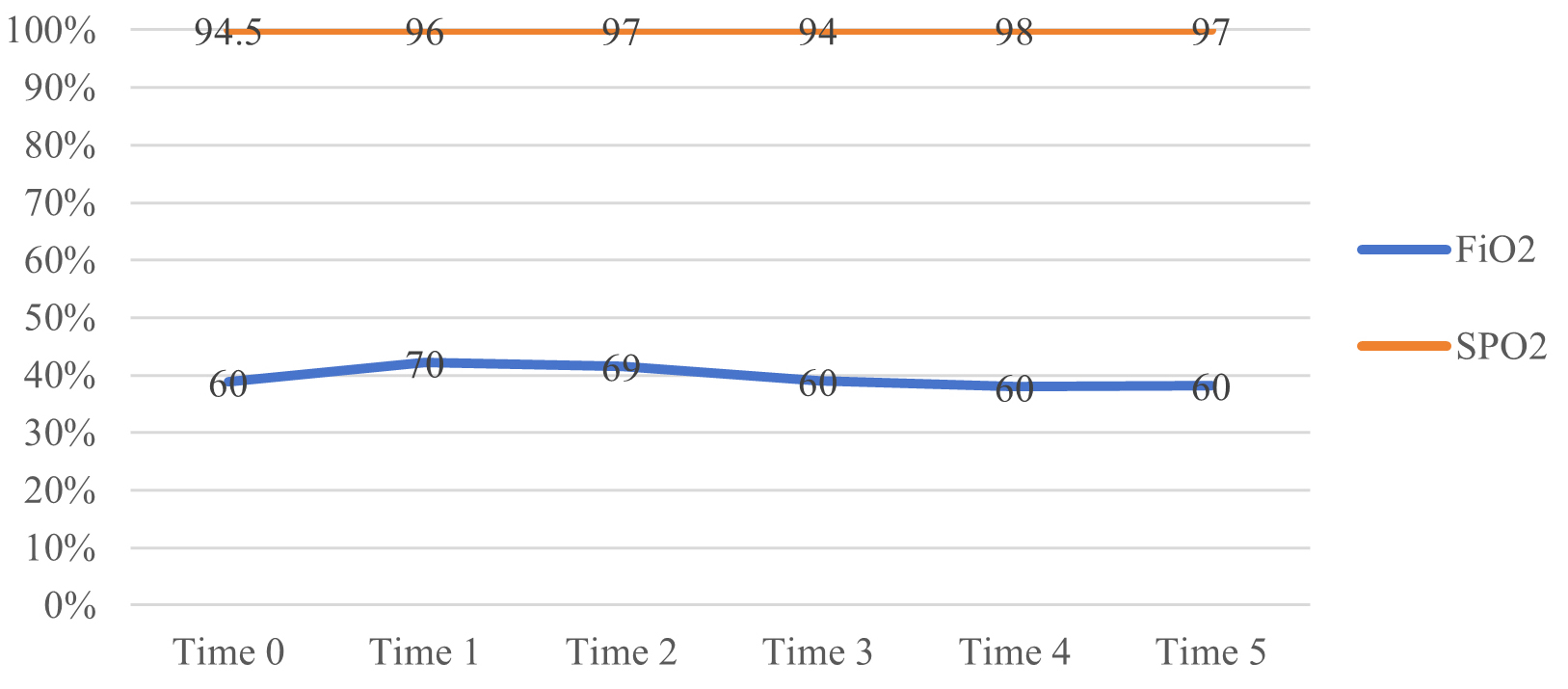 Fig. 3.
Fig. 3.
Temporal changes in FiO2 (%) and SpO2 (%) following early lung recruitment and prone positioning.
Postoperative complications from STAAD surgery have become a significant cause of patient mortality, with ARDS being one of the main complications. In this study, all included patients met the diagnostic criteria for moderate to severe ARDS [12]. The risk factors for ARDS after STAAD surgery are associated with interleukin-6 and systemic inflammatory response [13]. In addition, a risk factor analysis for STAAD identified obesity as a relevant factor [14, 15, 16]. It is related to young age, anemia, and the extensive transfusion of blood products [17].
Early lung recruitment combined with prone positioning can improve postoperative
hypoxemia in patients with aortic dissection. The results of this study show that
early lung recruitment combined with prone positioning can improve postoperative
hypoxemia in patients with aortic dissection. The main reason may be attributed
to extensive alveolar collapse in ARDS, which reduces the effective lung volume.
Early lung RM combined with prone positioning can more effectively reopen
collapsed alveoli while also increasing lung volume, thereby improving
oxygenation [18, 19, 20]. However, it is important to note that the persistent effect
of early RM on alveolar opening is limited, only improving oxygenation for a
period. This study only explored changes in respiratory parameters at 30 minutes,
1 hour, 4 hours after the maneuver, and 2 hours, 4 hours post-procedure; further
investigation into the duration of effects is warranted. Zhang et al.
[21] suggested lung recruitment if the patient’s lungs are recruitable. However,
Nielsen et al. [22] indicated that if ARDS patients have acute pulmonary
heart disease, especially involving right heart function, the implementation of
lung recruitment might affect the patient’s venous return and thereby right heart
function. Considering this, the recruitment pressures PEEP in this study were all
Early lung recruitment combined with prone positioning is relatively safe for
ARDS patients with aortic dissection. In this study, only one patient was allowed
to prematurely terminate prone ventilation due to arrhythmia as permitted by the
attending physician, indicating a certain level of safety with early lung
recruitment combined with prone positioning. However, some studies have reported
that the incidence of cardiac arrest during prone ventilation is 6.75% [12].
Additionally, Schmidt et al. [28] pointed out that lung recruitment
might cause barotrauma, exacerbating injury in non-collapsed alveolar regions,
and that not all alveoli in consolidated areas can be fully recruited. Therefore,
assessing the recruitable nature of the lungs in the early recruitment process is
particularly important. This study confirms that early lung recruitment combined
with prone positioning is relatively safe for ARDS patients with aortic
dissection. However, since this procedure requires significant manpower and has a
higher incidence of complications, it necessitates an assessment by the attending
physician regarding the necessity of a second operation. This study did not
evaluate the need for a second prone ventilation operation; future studies could
design strict randomized controlled trials to analyze the safety and
effectiveness of this approach in patients with moderate to severe ARDS after
STAAD surgery. Safety remains a critical concern in postoperative cardiac
patients. Although only one patient in our cohort experienced arrhythmia
requiring early termination, potential risks such as barotrauma and hemodynamic
instability must be considered. Our protocol employed conservative PEEP limits
(
The findings from this study underscore the critical role of early lung recruitment combined with prone ventilation in managing ARDS following acute aortic dissection surgeries. By systematically evaluating respiratory parameters at multiple time points, researchers elucidated the protocol’s effectiveness in enhancing oxygenation, optimizing respiratory mechanics, and mitigating postoperative complications. The observed improvements in oxygenation and respiratory metrics highlight the protocol’s potential to reduce the incidence and severity of ARDS, thereby improving patient outcomes and overall surgical success rates. These findings contribute valuable insights into evolving perioperative strategies aimed at enhancing respiratory support and minimizing the physiological burden associated with complex cardiovascular surgeries.
This study is limited by its single-center retrospective design and relatively small sample size. Furthermore, the absence of a control group (e.g., RM alone or PP alone) restricts the ability to attribute improvements solely to the combined intervention. Future prospective randomized controlled trials are warranted to confirm these findings and enhance their generalizability.
In summary, the use of early lung recruitment combined with prone positioning in postoperative STAAD patients with moderate to severe ARDS can improve oxygenation and is relatively safe, which can guide its application in clinical treatment. The documented improvements in respiratory parameters underscore the protocol’s efficacy in optimizing lung function and mitigating respiratory complications, thereby enhancing patient safety and recovery outcomes. Moving forward, continued research and clinical application of such protocols hold promise in advancing perioperative care practices and improving outcomes for patients facing the challenges of acute aortic dissection surgeries and associated respiratory complications. However, further research is still needed on the timing and duration of lung recruitment combined with prone positioning. Additionally, further investigation is required to determine whether this approach can be applied to other major cardiovascular diseases.
The data are available from the corresponding author on reasonable request.
XL: Conceptualization, methodology, investigation, writing—original draft preparation, writing—review and editing. SL: Conceptualization, methodology, investigation, writing—original draft preparation, writing—review and editing. GL: formal analysis, writing—review and editing. AM: formal analysis, writing—review and editing. XG: formal analysis, writing—review and editing. SJ: investigation, writing—review and editing. JZ: Conceptualization, methodology, writing—review and editing. All authors have read and agreed to the published version of the manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was carried out in accordance with the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of The Provincial Hospital affiliated with Shandong First Medical University (Protocol No. 2020-4007). All participants in the study provided their written informed consent.
Not applicable.
This study was funded by (1) Chinese medicine science and technology project in Shandong Province (Funding Number: M-20243601); (2) Chinese medicine science and technology project in Shandong Province (Funding Number: M-2022214).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.