

 , Lijuan Ding 1, Na Xu 1, Ni Wang 1, Chen Chen 1,*
, Lijuan Ding 1, Na Xu 1, Ni Wang 1, Chen Chen 1,*
1 Department of Obstetrical, The Affiliated Wuxi People’s Hospital of Nanjing Medical University, (Wuxi People’s Hospital), (Wuxi Medical Center Nanjing Medical University), 214000 Wuxi, Jiangsu, China
Abstract
Labor induction in full-term pregnancies with unfavorable cervical conditions requires safe and effective methods. Oral misoprostol solution and cervical balloon placement are commonly used, but comparative evidence remains limited. The aim of this study was to compare the efficacy and safety of oral misoprostol solution and cervical balloon placement in pregnant women with unfavorable cervical conditions.
This retrospective clinical study included 610 full-term pregnant women who underwent labor induction between January 2023 and January 2025. Participants were divided into two groups: an oral misoprostol group (n = 310) and a cervical balloon group (n = 300). Primary outcome measures included mode of delivery, specifically the vaginal delivery rate, cesarean section rate, 12-hour vaginal delivery rate, and 24-hour vaginal delivery rate. Secondary outcome measures included indications for cesarean section, oxytocin usage, delivery conditions, delivery complications, patient satisfaction, and neonatal outcomes.
The misoprostol group had a significantly higher vaginal delivery rate (57.42% vs. 47.67%; p = 0.016). Labor duration was shorter (781.55 ± 267.30 min vs. 972.09 ± 360.24 min; p < 0.001), and oxytocin use rates (52.26% vs. 78.67%; p < 0.001) and artificial rupture of membranes rate (59.68% vs. 77.33%; p < 0.001) were lower. The misoprostol group also had a lower neonatal infection rate (0.65% vs. 3.00%; p = 0.029) and higher patient satisfaction (95.81% vs. 89.33%; p = 0.002). In contrast, the cervical balloon group had higher incidences of poor progress during the first stage of labor (49.68% vs. 37.12%; p = 0.032) and chorioamnionitis (6.37% vs. 1.52%; p = 0.039).
Oral misoprostol solution was more effective for labor induction in full-term pregnant women with unfavorable cervical conditions, and was associated with lower cesarean section rates, reduced oxytocin use, and higher patient satisfaction. It also demonstrates favorable safety outcomes across key indicators. Thus, these findings support its use as a preferred option in clinical practice.
Keywords
- misoprostol
- cervical balloon
- pregnancy
- full-term pregnancy
- cervical ripening
- labor
- induced
- pregnant women
In clinical medicine, term pregnancy delivery is defined as delivery occurring from 37 completed weeks (259 days) to less than 42 weeks (294 days) of gestation [1]. The initiation mechanism of this physiological process involves a complex multifactorial regulatory system, encompassing the activation of the fetal hypothalamic-pituitary-adrenal (HPA) axis, dynamic changes in placental hormones, alterations in uterine myometrial sensitivity, and a cascade of inflammatory factor reactions, among others [2, 3]. Any abnormality in any of these links may prevent the normal initiation of the delivery mechanism. However, in clinical practice, many terms pregnant women are unable to naturally progress into the labor stage due to various physiological, psychological, or pathological factors and must rely on artificial intervention methods to induce labor [4]. Otherwise, a series of severe problems, such as placental aging or dysfunction, fetal distress, and neonatal asphyxia, may arise, thereby posing a threat to the life safety of both the mother and the infant [5]. Labor induction at term refers to the process of accelerating uterine contractions and initiating the delivery process through various methods, such as pharmacological or mechanical means, after 37 completed weeks of gestation and before the onset of spontaneous uterine contractions, aiming to achieve an effect similar to that of natural childbirth [6]. The primary objective of labor induction is to facilitate timely delivery from an unfavorable intrauterine environment and to alleviate or resolve maternal comorbidities or pregnancy-related complications [7]. The success of labor induction is closely associated with cervical maturity. The more mature the cervix is, the higher the success rate of labor induction [8].
Cervical ripening is an important physiological change that occurs in women during the late stages of pregnancy. Essentially, it involves a series of biochemical and morphological alterations in cervical tissue under the regulation of endogenous hormones. These changes include the degradation of collagen fibers, a significant increase in the content of glycosaminoglycans such as hyaluronic acid in the extracellular matrix, and an increase in water retention. Ultimately, these processes lead to cervical softening, shortening, and enhanced dilatation capacity, thereby creating the necessary conditions for normal childbirth [9]. This process is not only crucial for spontaneous labor but also as a prerequisite for successful induction [10]. Clinical interventions aimed at promoting cervical ripening attempt to replicate this physiological process through pharmacological or mechanical methods. Their mechanisms including promoting the synthesis of endogenous prostaglandins, enhancing collagenase activity, and altering the physicochemical properties of the extracellular matrix [11]. Ideally, interventions to promote cervical ripening should achieve biological effects similar to those of natural ripening, effectively improving cervical compliance while maintaining normal uterine contraction rhythms and avoiding complications such as tetanic contractions, birth canal injuries, or inadequate placental perfusion [12]. It is noteworthy that insufficient cervical ripening significantly affects the outcome of labor induction, not only prolonging labor and increasing maternal physical exertion but also potentially leading to failed induction and subsequent emergency cesarean section, thereby increasing risks for both mother and neonate [13]. Consequently, the selection of safe, effective, and highly predictable methods for promoting cervical ripening has become a critical issue in optimizing delivery management and improving pregnancy outcomes.
Misoprostol, a synthetic analog of prostaglandin E1, is a widely used drug in
the fields of pregnancy termination and labor induction due to its significant
pharmacological effects [14]. By activating prostaglandin receptor–mediated
signaling pathways, misoprostol promotes cervical connective tissue remodeling,
enhances collagen degradation, and increases cervical compliance. Additionally,
it sensitizes uterine smooth muscle to oxytocin, facilitating the initiation of
effective uterine contractions [15]. Misoprostol acts rapidly and offers
remarkable cost-effectiveness, making it well-suited for use in healthcare
institutions at all levels [16]. Cervical balloon placement is a commonly used
mechanical method for labor induction [17]. The balloon is a double-lumen
catheter made of silicone. It is inserted into the cervical canal, and
physiological saline is injected into the balloon. The mechanical expansion of
the balloon stimulates the cervix, promoting cervical ripening and dilation [18].
This method does not directly stimulate uterine smooth muscle contraction but
instead applies mechanical pressure to the cervix, mimicking the pressure exerted
by the fetal head on the cervix during natural childbirth, thereby achieving the
effect of labor induction [19]. In clinical obstetric practice, oral misoprostol
solution administration and cervical balloon placement, as two commonly used
methods for promoting cervical ripening, have been widely applied in the labor
induction process for pregnant women with unfavorable cervical conditions. Common
indications for induction in such cases include, but are not limited to,
hypertensive disorders of pregnancy (e.g., preeclampsia), gestational diabetes
mellitus requiring delivery, oligohydramnios, post-term gestation (
Against this background, there remains a lack of consensus and limited robust comparative evidence regarding the efficacy and safety of oral misoprostol solution versus cervical balloon placement for labor induction in this specific population. Therefore, this study aimed to compare the labor induction effects and safety of oral misoprostol solution and cervical balloon placement in full-term pregnant women with unfavorable cervical conditions.
This study is a retrospective observational study, with data collection and analysis conducted by researchers not involved in the patients’ treatment. A total of 610 cases of term pregnancy induction among parturients admitted to The Affiliated Wuxi People’s Hospital of Nanjing Medical University from January 2023 to January 2025 were selected. Group allocation (oral misoprostol vs. cervical balloon) was determined by physician preference and clinical judgment, taking into account factors such as cervical Bishop score, patient tolerance, and institutional protocols at the time of induction. The cases were divided into an oral misoprostol group (310 cases) and a cervical balloon group (300 cases) based on different induction methods. The study compared the effectiveness and safety of oral misoprostol solution versus cervical balloon placement in pregnant women with unfavorable cervical conditions. The detailed study protocol is illustrated in Fig. 1.
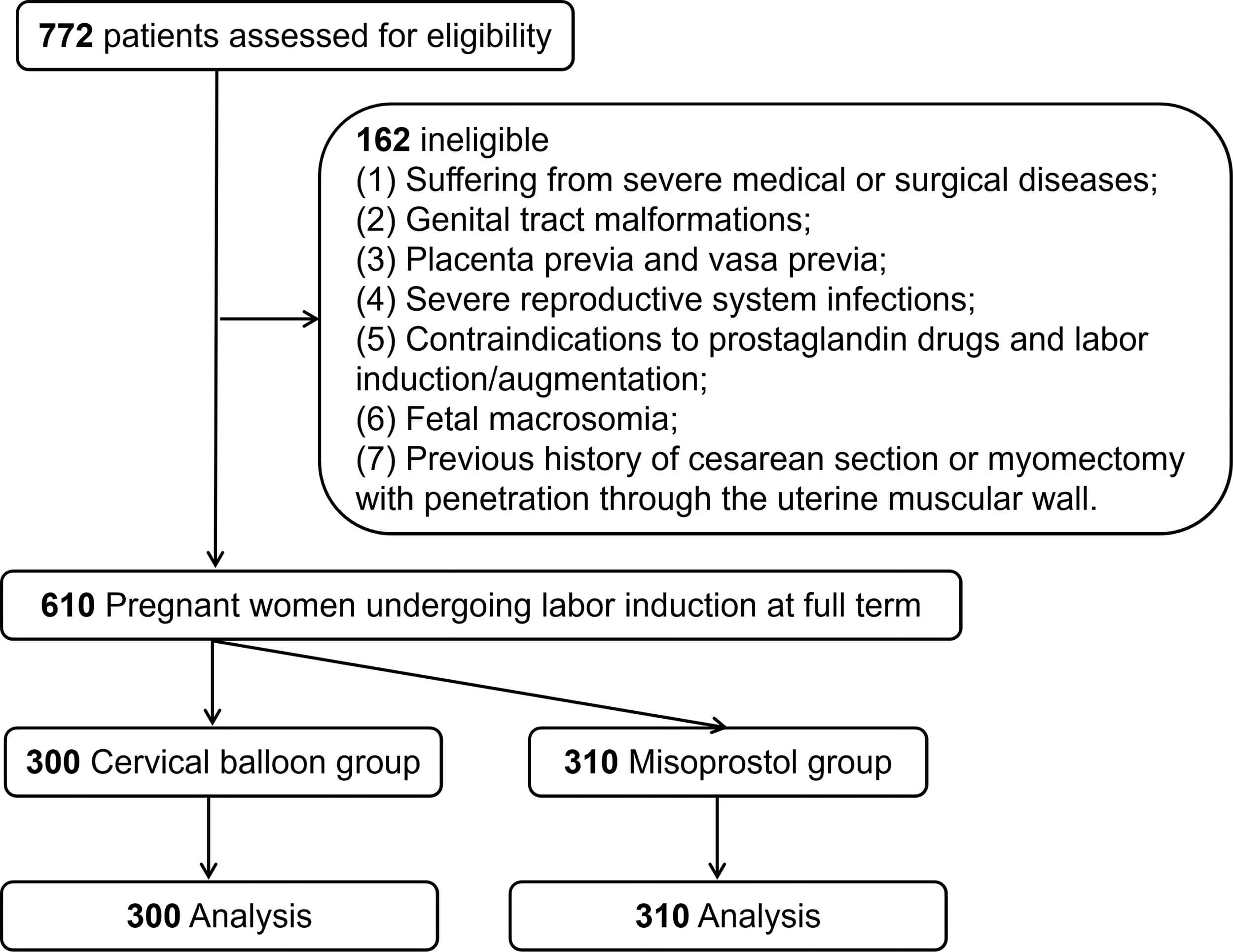 Fig. 1.
Fig. 1.
Research flowchart.
Participants were eligible for inclusion if they met all of the following
criteria: (1) Primiparous women with a gestational age between 37 and 42 weeks;
(2) Singleton pregnancy in cephalic presentation; (3) Written informed consent
provided by the parturient and her family; (4) Intact fetal membranes; (5)
Cervical Bishop score
Participants were excluded if any of the following conditions were present: (1) Pregnant women with severe medical or surgical conditions that render them unable to tolerate the induction process or increase the risk associated with induction; (2) Reproductive tract malformations, such as vaginal septum or uterine septum, which are expected to make vaginal delivery difficult; (3) Placenta previa and vasa previa; (4) Severe reproductive system infections; (5) Contraindications to prostaglandin drugs and labor induction/augmentation; (6) Macrosomia; (7) A history of previous cesarean section or a history of myomectomy that penetrated the uterine myometrium.
Sample size estimation was performed using G-Power software [22]. Assuming an
effect size of 0.3, a two-tailed significance level (
A total of 610 parturients undergoing term pregnancy induction were finally collected in this study and were divided into an oral misoprostol group (n = 310) and a cervical balloon group (n = 300) based on different induction methods.
All parturients underwent an oxytocin challenge test (OCT) before oral
administration of misoprostol solution. After confirmation of a negative OCT
result, contraindications were excluded, and informed consent was obtained. Half
an hour after discontinuing the OCT, the relevant contraindications were
reconfirmed. Specific drug preparation [23]: Dissolve one misoprostol tablet (0.2
mg, Misoprostol Tablets, China Resources Zizhu Pharmaceutical Co., Ltd. (Beijing, China), National
Medical Products Administration Approval No. H20000668) in 200 mL of warm water.
After thorough stirring, a 1 µg/mL misoprostol aqueous solution is
prepared. Initially, 25 mL of the solution was administered orally, followed by
50 mL after 2 hours, and subsequently 50 mL every 4 hours. Continuous monitoring
of uterine contractions and fetal heart rate was conducted throughout
administration. If uterine hyperstimulation occurred before the next scheduled
dose, drug administration should be temporarily suspended (for those with
premature rupture of membranes, drug administration should be stopped). The maximum
daily dose did not exceed 200 µg. The cervical condition was evaluated daily.
If the cervical Bishop score is
A disposable double-balloon cervical dilator (18F; length 40 cm; maximum balloon capacity 80 mL; Yangzhou Qiangjian Medical Equipment Co., Ltd. (Yangzhou, Jiangsu, China)) was used. All parturients underwent an OCT before balloon placement, and informed consent was obtained following confirmation of a negative result. The fetal heart rate was auscultated before insertion, and closer monitoring of uterine contractions and the fetal heart rate was conducted after placement. All pregnant women underwent cervical balloon placement at 21:00 on the day of cervical ripening promotion. The placement method was as follows: After bladder emptying, the parturient was positioned in the dorsal lithotomy position. Following routine perineal disinfection and sterile draping, a vaginal speculum was used to expose the cervix, and the vagina and cervix were disinfected. The anterior and posterior lips of the cervix were grasped with cervical forceps. The distal end of the cervical dilating balloon catheter was grasped with an oval forceps and inserted through the cervix so that both balloons entered the internal cervical os. The uterine balloon was inflated with 40 mL of sterile saline. After inflation, the balloon was pulled outward until the uterine balloon was snug against the internal cervical os. Then, the vaginal balloon was inflated with 20 mL of sterile saline. Subsequently, the fluid volume in the intrauterine and vaginal balloons was increased sequentially (by 20 mL each time) until each balloon reached 60 mL [24].
If spontaneous labor did not occur, the balloon was removed at 07:00 the following morning. After performing a cervical Bishop score, artificial rupture of membranes (ARM) was carried out (except in cases of spontaneous rupture of membranes). After ARM, the patient was observed for two hours. If no effective uterine contractions occurred, 2.5 U of oxytocin combined with 500 mL of 0.9% sodium chloride injection was administered intravenously for planned delivery (the initial drip rate was 5 drops/minute and was adjusted according to the uterine contractions). Typically, the drip rate was increased by 5 drops every 15–30 minutes until effective uterine contractions were achieved. The maximum drip rate usually did not exceed 40 drops/minute; however, in non-responsive cases, the oxytocin concentration could be changed to 5 U and readjusted. If delivery had not occurred 12 hours after ARM, cefuroxime 1.5 g was administered intravenously as prophylactic anti-infective treatment.
Detailed baseline data of patients were collected, including patient age, educational level, occupation, height, pre-pregnancy body mass index (BMI), gestational age at induction, and Bishop score.
The mode of delivery was evaluated, with specific focus on the rates of vaginal delivery, cesarean section, delivery within 24 hours, vaginal delivery within 12 hours, and vaginal delivery within 24 hours.
① Indications for Cesarean Section: Specific reasons for cesarean section were recorded, including slow progress in the first stage of labor, difficult progress during the second stage of labor, abnormal fetal heart rate, meconium-stained amniotic fluid, deterioration in the parturient’s condition, chorioamnionitis, massive hemorrhage during delivery, and umbilical cord prolapse.
② Oxytocin Usage: The use of oxytocin was observed, including whether oxytocin was administered, the time interval from induction to oxytocin infusion, and the duration of oxytocin infusion.
③ Patient’s Delivery Status: The time from patient enrollment to induction, the time from induction to delivery, and cervical changes within 12 hours and 24 hours were recorded. Additionally, intraoperative artificial rupture of membranes and potential side effects during induction were observed.
④ Delivery Complications: Complications occurring during delivery were recorded, such as uterine hyperstimulation, postpartum hemorrhage, postpartum infection, urinary retention, and nausea and vomiting.
⑤ Patient Satisfaction: Patient satisfaction with the induction process was assessed based on their willingness to choose the same method for future inductions.
⑥ Neonatal Outcomes: Neonatal birth outcomes were recorded, including birth weight, Apgar score, neonatal mortality, and neonatal morbidity.
Data analysis was conducted using SPSS 25.0 statistical software (IBM Corp.,
Armonk, NY, USA). For variables such as age, height, and BMI, if they followed a
normal distribution, they were expressed as mean
Table 1 compares the baseline characteristics between the cervical balloon group
and the misoprostol group. There were no significant differences between the two
groups in terms of age, educational level, occupation, height, pre-pregnancy BMI,
underlying diseases, weight gain during pregnancy, gestational age at induction,
and Bishop score (p
| Variables | Cervical balloon group (n = 300) | Misoprostol group (n = 310) | Test | 95% CI | t/ |
p-value | |
| Age (years) | 27.12 |
26.95 |
Independent sample t-test | –0.553 to 0.890 | 0.458 | 0.647 | |
| Education | |||||||
| Primary | 46 (15.33) | 59 (19.03) | - | 1.886 | 0.389 | ||
| Secondary | 189 (63.00) | 193 (62.26) | |||||
| University | 65 (21.67) | 58 (18.71) | |||||
| Occupation | |||||||
| Manual labor | 63 (21.00) | 55 (17.74) | - | 1.944 | 0.378 | ||
| Mental labor | 154 (51.33) | 176 (56.77) | |||||
| Housewife | 83 (27.67) | 79 (25.48) | |||||
| Underlying diseases | |||||||
| Hypertension | 35 (11.67) | 32 (10.32) | - | 0.282 | 0.596 | ||
| Diabetes | 32 (10.67) | 35 (11.29) | - | 0.061 | 0.806 | ||
| Hyperlipemia | 38 (12.67) | 41 (13.23) | - | 0.042 | 0.837 | ||
| Height (cm) | 162.45 |
162.78 |
Independent sample t-test | –1.226 to 0.565 | –0.725 | 0.469 | |
| Prepregnancy BMI (kg/m2) | 22.83 |
22.92 |
Independent sample t-test | –0.650 to 0.450 | –0.357 | 0.721 | |
| Weight gain during pregnancy (kg) | 17.33 |
17.14 |
Independent sample t-test | –0.051 to 0.861 | 0.519 | 0.604 | |
| Induced labor gestational age (weeks) | 39.46 |
39.55 |
Independent sample t-test | –0.278 to 0.114 | –0.820 | 0.413 | |
| Bishop score | |||||||
| 0 |
119 (39.67) | 132 (42.58) | - | 0.535 | 0.465 | ||
| 4 |
181 (60.33) | 178 (57.42) | |||||
Note: BMI, body mass index; CI, confidence interval. The same below.
Table 2 compares the delivery outcomes between the cervical balloon group and the misoprostol group. The results show that the misoprostol group significantly outperformed the cervical balloon group in terms of the vaginal delivery rate (57.42% vs. 47.67%) (p = 0.016). These data indicate that oral misoprostol is more effective in improving the success rate of vaginal delivery and shortening the labor process.
| Variables | Cervical balloon group (n = 300) | Misoprostol group (n = 310) | Test | p-value | |
| Vaginal delivery rate | 143 (47.67) | 178 (57.42) | 5.817 | 0.016 | |
| Cesarean section rate | 157 (52.33) | 132 (42.58) | |||
| Delivery rate within 24 hours | 255 (85.00) | 290 (93.55) | 11.702 | 0.001 | |
| Vaginal delivery rate within 12 hours | 88/143 (61.54) | 115/178 (64.61) | 0.321 | 0.571 | |
| Vaginal delivery rate within 24 hours | 141/143 (98.60) | 176/178 (98.88) | Fisher’s exact | - | 1.000 |
Table 3 compares the distribution of indications for cesarean section between
the two groups. The cervical balloon group had significantly higher incidences of
poor progress during the first stage of labor (49.68% vs. 37.12%) and
chorioamnionitis (6.37% vs. 1.52%) compared to the misoprostol group (p
| Variables | Cervical balloon group (n = 157) | Misoprostol group (n = 132) | p-value | |
| Poor progress in the first stage of labor | 78 (49.68) | 49 (37.12) | 4.593 | 0.032 |
| Difficulty in the progression of the second stage of labor | 1 (0.64) | 2 (1.52) | 0.023 | 0.880 |
| Fetal heart rate abnormalities | 42 (26.75) | 41 (31.06) | 0.650 | 0.420 |
| Meconium-stained amniotic fluid | 21 (13.38) | 27 (20.45) | 2.594 | 0.107 |
| Maternal deterioration | 2 (1.27) | 4 (3.03) | 0.396 | 0.529 |
| Chorioamnionitis | 10 (6.37) | 2 (1.52) | 4.246 | 0.039 |
| Massive hemorrhage during childbirth | 2 (1.27) | 7 (5.30) | 2.638 | 0.104 |
| Umbilical cord prolapses or presentation | 1 (0.64) | 0 (0.00) | Fisher’s exact - | 1.000 |
Table 4 compares oxytocin use between the two groups of parturients. The results
show that the oxytocin usage rate in the cervical balloon group was significantly
higher than that in the misoprostol group (78.67% vs. 52.26%, p
| Variables | Cervical balloon group (n = 300) | Misoprostol group (n = 310) | Test | 95% CI | t/ |
p-value |
| Using oxytocin | 236 (78.67) | 162 (52.26) | - | 46.891 | ||
| Time from induction of labor to oxytocin infusion (min) | 368.46 |
548.99 |
Independent sample t-test | –190.127 to –170.947 | –36.971 | |
| Duration of oxytocin infusion (min) | 375.23 |
247.78 |
Independent sample t-test | 117.210 to 137.701 | 24.431 |
Table 5 presents a comparison of labor and delivery characteristics between the
two groups of parturients. The results show that the misoprostol group had
significantly shorter total labor duration (781.55
| Variables | Cervical balloon group (n = 300) | Misoprostol group (n = 310) | Test | 95% CI | t/ |
p-value | |
| Time from induction of labor to delivery (min) | |||||||
| All women (min) | 972.09 |
781.55 |
Independent sample t-test | 140.209 to 240.868 | 7.435 | ||
| Vaginal delivery only (min) | 695.11 |
651.65 |
Independent sample t-test | 12.476 to 74.445 | 2.760 | 0.006 | |
| Cesarean section only (min) | 1224.37 |
956.72 |
Independent sample t-test | 196.903 to 338.397 | 7.446 | ||
| No cervical change | |||||||
| Within 12 h | 1 (0.33) | 1 (0.32) | Fisher’s exact | - | - | 1.000 | |
| Within 24 h | 0 (0.00) | 0 (0.00) | - | - | - | ||
| Intraoperative artificial rupture of membranes | 232 (77.33) | 185 (59.68) | - | 21.947 | |||
| Side effects during the induction of labor | |||||||
| Diarrhea | 2 (0.67) | 4 (1.29) | - | 0.137 | 0.711 | ||
| Vomiting | 11 (3.67) | 14 (4.52) | - | 0.280 | 0.597 | ||
Table 6 compares the incidence of delivery complications between the two groups
of parturients. No statistically significant differences were observed in the
incidence of complications such as uterine hyperstimulation (0.65% vs. 0.33%),
postpartum hemorrhage (0.65% vs. 0.67%), puerperal infection (0.32% vs.
1.00%), urinary retention (5.81% vs. 5.00%), and nausea and vomiting (4.84%
vs. 4.67%) between the misoprostol group and the cervical balloon group
(p
| Variables | Cervical balloon group (n = 300) | Misoprostol group (n = 310) | p-value | |
| Uterine hyperstimulation | 1 (0.33) | 2 (0.65) | 0.001 | 0.977 |
| Postpartum hemorrhage | 2 (0.67) | 2 (0.65) | 0.220 | 0.639 |
| Postpartum infection | 3 (1.00) | 1 (0.32) | 0.286 | 0.593 |
| Urinary retention | 15 (5.00) | 18 (5.81) | 0.194 | 0.660 |
| Nausea and vomiting | 14 (4.67) | 15 (4.84) | 0.010 | 0.920 |
Table 7 compares maternal satisfaction levels of parturients between the two groups. When women were allowed to choose their preferred cervical ripening method, 89.33% of patients in the cervical balloon group expressed satisfaction, compared with 95.81% in the oral misoprostol group. The difference in satisfaction between the two groups was statistically significant (p = 0.002).
| Variables | Cervical balloon group (n = 300) | Misoprostol group (n = 310) | RD (95% CI) | p-value | |
| Dissatisfied | 32 (10.67) | 13 (4.19) | 6.48% (2.33% to 10.62%) | 9.349 | 0.002 |
| Satisfied | 268 (89.33) | 297 (95.81) |
RD, risk difference.
Table 8 compares the neonatal outcomes between the two groups. No significant
differences between the misoprostol group and the cervical balloon group in terms
of live birth rate (both 100%), birth weight (2651.33
| Variables | Cervical balloon group (n = 300) | Misoprostol group (n = 310) | Test | 95% CI | Effect size | p-value | ||
| Birth outcome | ||||||||
| Live birth | 300 (100.00) | 310 (100.00) | - | - | - | - | ||
| Stillbirth | 0 (0.00) | 0 (0.00) | ||||||
| Birth weight (g) | 2620.48 |
2651.33 |
Independent sample t-test | –73.938 to 12.240 | –1.406 | 0.160 | ||
| Apgar score | ||||||||
| at 1 min | ||||||||
| 12 (4.00) | 11 (3.55) | - | 0.086 | 0.770 | ||||
| 288 (96.00) | 299 (96.45) | |||||||
| at 5 min | ||||||||
| 1 (0.33) | 2 (0.65) | - | 0.001 | 0.977 | ||||
| 299 (99.67) | 308 (99.35) | |||||||
| at 10 min | ||||||||
| 0 (0.00) | 0 (0.00) | - | - | - | - | |||
| 300 (100.00) | 310 (100.00) | |||||||
| Neonatal death | 0 (0.00) | 0 (0.00) | - | - | - | |||
| Incidence of neonatal diseases | ||||||||
| No incidence | 286 (95.33) | 303 (97.74) | - | 2.661 | 0.103 | |||
| Neonatal jaundice | 4 (1.33) | 3 (0.97) | - | 0.002 | 0.965 | |||
| Neonatal hypoglycemia | 0 (0.00) | 1 (0.32) | Fisher’s exact | - | - | 1.000 | ||
| Neonatal hypoxic-ischemic encephalopathy | 1 (0.33) | 0 (0.00) | Fisher’s exact | - | - | 1.000 | ||
| Septicemia | 0 (0.00) | 1 (0.32) | Fisher’s exact | - | - | 1.000 | ||
| Neonatal infection | 9 (3.00) | 2 (0.65) | - | 4.774 | 0.029 | |||
Induction of labor is an important intervention for terminating pregnancy, especially in full-term pregnancies with unfavorable cervical conditions. The selection of an appropriate induction method is therefore crucial for ensuring maternal and neonatal safety and improving the quality of childbirth [25]. In recent years, with the continuous advances in medical technology, multiple induction methods have been widely applied in clinical practice. Among these, oral misoprostol solution and cervical balloon placement are two commonly used induction techniques. However, controversy remains regarding the comparative effectiveness and safety in the induction of full-term pregnancies, and robust evidence-based data are still limited. This study conducted a retrospective analysis of the clinical data from 610 parturients who underwent full-term pregnancy induction at our hospital between January 2023 and January 2025. The aim was to comprehensively evaluate the clinical value of oral misoprostol solution and cervical balloon placement for inducing labor in women with unfavorable cervical conditions and to provide a scientific basis for clinical practice.
For pregnant women with unfavorable cervical conditions, successful vaginal delivery during the induction process is an important indicator for evaluating the effectiveness of induction. Misoprostol, through its prostaglandin E1 activity, can soften the cervix and increase its dilatability, thereby creating more favorable conditions for natural childbirth [26]. In contrast, although cervical balloons can facilitate cervical ripening to some extent, their effect is less pronounced than that of misoprostol. The results of this study demonstrated that the vaginal delivery rate in the misoprostol group (57.42%) was significantly higher than that in the cervical balloon group (47.67%), while the cesarean section rate was lower (42.58% vs. 52.33%). These findings indicate that misoprostol has a clear advantage in promoting natural childbirth. Consistent with our results, Kemper et al. [27] conducted a systematic search of randomized controlled trials (RCTs) comparing catheters with oral misoprostol for the induction of labor in full-term singleton pregnancies from inception to April 2019, including four trials providing individual participant data with a total of 2815 subjects. The results showed that for women undergoing induction, the effectiveness of catheters was lower than that of oral misoprostol, with a slightly reduced likelihood of vaginal delivery among subjects using catheters (Risk Ratio = 0.95, 95% CI = 0.91–0.99), supporting the conclusions of this study. This difference may be attributable to the distinct pharmacological mechanism of misoprostol. Misoprostol directly acts on uterine smooth muscle and cervical tissue, increasing the frequency and intensity of uterine contractions while softening and dilating the cervix [28]. In contrast, cervical balloon primarily functions through physical compression and dilation of the cervical canal, with a relatively weaker regulatory effect on uterine contractions [29]. Additionally, the delivery rate within 24 hours was significantly higher in the misoprostol group than in the cervical balloon group, and the labor duration was shorter. This suggests that misoprostol can more effectively shorten the time interval from induction to delivery. From a clinical perspective, reducing labor duration not only alleviates the suffering of parturients but also reduce the risk of maternal and neonatal complications associated with prolonged labor. By enhancing the coordination and intensity of uterine contractions, misoprostol promotes more rapid cervical dilation and accelerates the labor process. In contrast, the physical mechanism of cervical balloon dilation is relatively slow in achieving effective cervical ripening, often necessitating artificial rupture of membranes to strengthen contractions and expedite labor. Notably, this study showed that the incidence of poor progress during the first stage of labor reached 49.68% in the cervical balloon group, suggesting that mechanical dilation may lack coordination between cervical ripening and the onset of contractions, increasing the risk of labor stagnation. Misoprostol, by directly stimulating uterine smooth muscle to produce regular contractions while simultaneously promoting cervical softening, enabling contractile forces to be more effectively translated into the power for cervical dilation. In contrast, reliance on mechanical dilation with cervical balloons may lead to cervical tissue edema, increasing uterine contraction resistance, which is also an important reason for its high incidence of poor progress in the first stage of labor [30].
The present study also demonstrated that the oxytocin usage rate and the duration of oxytocin infusion were significantly lower in the misoprostol group than in the balloon group. It is important to note that the induction of the labor process carries significant clinical risks, which are particularly prominent in medical settings that lack electronic oxytocin infusion pumps and fetal electronic monitoring equipment. A major challenge in such settings is the difficulty in precisely regulating uterine contraction intensity. Insufficient stimulation may prolong labor and increase the failure rate of induction, whereas excessive stimulation can markedly elevate the risk of fetal distress [31]. From a mechanistic perspective, cervical balloons have a pharmacological advantage of not directly inducing uterine contractions during the cervical ripening phase. By physically stimulating the cervix, cervical balloons promote the synthesis and secretion of endogenous prostaglandins, leading to cervical softening and dilation, ultimately facilitating natural childbirth. This mechanism avoids direct stimulation of the uterus and fetus by drugs, reducing the risks of overly strong or uncoordinated contractions, as well as adverse reactions caused by improper drug use [32]. However, clinical observations from this study revealed that approximately 80% of parturients still required intravenous oxytocin infusion during subsequent labor stages. This indicates that while cervical balloons are effective for cervical ripening, they still rely on oxytocin to maintain and enhance uterine contractions to ensure successful delivery. This reliance poses significant fetal safety risks in medical settings lacking precise infusion equipment. For example, improper dosage control of oxytocin can lead to overly strong or irregular contractions, increasing the risks of fetal distress in utero and even uterine rupture [33]. Therefore, the safety advantages of cervical balloons during the cervical ripening phase may be offset by the risks associated with subsequent oxytocin infusion. In contrast, misoprostol exhibits dual pharmacological effects by both inducing uterine contractions and promoting cervical ripening. This dual action allows a greater proportion of parturients to achieve vaginal delivery without reliance on oxytocin infusion, thereby suggesting potential safety advantages. Notably, the incidence of meconium-stained amniotic fluid was higher in the misoprostol group, which may be attributable to pharmacological stimulation of fetal intestinal smooth muscle [34]. In the absence of continuous electronic fetal heart rate monitoring, meconium-stained amniotic fluid, as an important clinical indicator of fetal distress, may itself constitute an indication for cesarean section. Although meconium staining is not directly causally associated with fetal hypoxia, considering the potential risk of meconium aspiration syndrome, this phenomenon remains clinically significant. It is worth noting that the introduction of electronic fetal heart rate monitoring in cases with meconium staining may further reduce the cesarean section rate in the misoprostol group, thereby potentially amplifying the observed differences in clinical efficacy between the two induction methods.
There were no significant differences between the two groups in most complications (such as postpartum hemorrhage and amniotic fluid embolism). However, a higher incidence of chorioamnionitis was observed in the cervical balloon group (6.37% vs. 1.52%; p = 0.039). While this difference reached statistical significance, the overall number of events was small (10 vs. 2 cases). This observation warrants attention and suggests a potential association between mechanical manipulation and infection risk that should be considered in clinical practice, though it requires confirmation in larger studies. In clinical practice, it is therefore essential to strictly control the timing of balloon placement, minimize the duration of catheter retention, and strengthen post-procedural monitoring of body temperature and blood parameters. Regarding neonatal infections, the misoprostol group demonstrated significant advantages, which may be attributable to the shorter duration of labor and the inherent anti-inflammatory properties of the drug. A study by Kruit and Rahkonen [35] also confirmed that, compared with oral misoprostol, the use of cervical balloons was associated with nearly a threefold increase in the incidence of chorioamnionitis and a twofold increase in neonatal infections. Nevertheless, it should be noted that excessive doses of misoprostol may lead to overly strong uterine contractions, increasing the risk of fetal distress. Accordingly, strict control of the clinical dosage is essential, with a single dose not exceeding 50 µg. The safety controversy surrounding misoprostol primarily relates to its dose-effect relationship. Early studies suggested that oral misoprostol might increase the risk of uterine rupture. Misoprostol is rapidly absorbed, with serum concentrations peaking within 30 minutes after administration and a primary metabolic half-life of approximately 120 minutes. These pharmacokinetic characteristics necessitate repeated dosing every 1–2 hours in clinical practice to ensure effective induction of uterine contractions [36]. Although frequent dosing may increase the clinical management burden, it allows for more precise dose regulation, thereby reducing the risk of uterine hyperstimulation. In contrast, a single large dose followed by prolonged observation may fail to promptly address sudden episodes of frequent contractions, increasing the risk of adverse pregnancy outcomes. In the present study, a low-dose regimen was employed, and no related adverse events were observed, indicating that the safety of misoprostol is manageable when administered at appropriate doses.
The results of this study indicate that among women in the oral misoprostol group who may require labor induction in the future, the proportion wiling to choose this method again was significantly higher than that in the cervical balloon group. Flament et al. [37] evaluated women’s satisfaction with cervical ripening methods during labor induction. The results showed that women were generally satisfied when given the autonomy to choose a method, with 95.3% of patients in the oral misoprostol group expressing satisfaction, a figure higher than the 90.5% in the cervical balloon group, which is largely consistent with the findings of our study. This may be attributed to the fact that oral misoprostol, during the initial labor induction process, avoids the discomfort vaginal examinations required for cervical balloon insertion, thereby reducing physical trauma and psychological burden [38]. Additionally, some participants were spared from oxytocin infusion, while others avoided cesarean sections. These factors may positively influence women’s preferences regarding future labor induction methods.
This study aimed to optimize labor induction strategies for pregnant women with unfavorable cervical conditions. By systematically comparing oral misoprostol solution and cervical balloon placement in terms of labor induction success rate, labor duration, cesarean section rate, and maternal-fetal complications, it confirms that misoprostol offers advantages in improving the 24-hour vaginal delivery rate, reducing the cesarean section rate and oxytocin usage, and achieving higher maternal satisfaction. These findings provide crucial evidence-based support for optimizing labor induction protocols in clinical practice, streamlining the induction process, enhancing delivery safety, and potentially reducing unnecessary cesarean sections, thereby improving maternal and neonatal outcomes. Additionally, the study results may inform the formulation and updating of clinical guidelines and contribute to the promotion of standardized obstetric care.
This study has certain limitations. Firstly, as a retrospective study, it is inherently susceptible to selection bias. For example, doctors may have been more inclined to select cervical balloon induction for high-risk parturients, which could affect the comparability of outcomes between groups. Second, all participants were recruited from a single hospital, and the findings may be influenced by the medical standards of the region and the baseline characteristics of the patients, thus limiting their generalizability. Additionally, this study did not explore the differences in effects between various doses of misoprostol or different amounts of water used to inflate the balloon. Furthermore, investigations incorporating assessments of cervical collagenase activity and uterine myometrial electrophysiological signals may help elucidate the molecular mechanisms underlying the observed differences between induction methods, thereby providing a stronger scientific foundation for clinical decision-making.
In conclusion, for term pregnant women with unfavorable cervical conditions, oral misoprostol solution significantly outperforms cervical balloons in terms of induction effectiveness, safety, and patient acceptability. Its primary advantages include a substantial increase in vaginal delivery rates, significant shortening of labor duration, and lower cesarean section rates and oxytocin use. When used at a reasonable dose, the risks of neonatal infection and maternal-fetal complications remain low. Moreover, this medication is cost-effective and easy to administer, which may reduce healthcare resource utilization and underscores its high clinical value.
The data supporting the findings of this study can be obtained from the corresponding author, upon request.
SL: Developed and planned the study, performed experiments, and interpreted results. Edited and refined the manuscript with a focus on critical intellectual contributions. LD, NX: Participated in collecting, assessing, and interpreting the data. Made significant contributions to data interpretation and manuscript preparation. NW, CC: Provided substantial intellectual input during the drafting and revision of the manuscript. Made substantial contributions to the design of the work; interpreted data for the work. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was carried out in accordance with the guidelines of the Declaration of Helsinki, and the protocol was approved by the Affiliated Wuxi People’s Hospital of Nanjing Medical University Ethics Committee (approval number: KY23123). All patients or their families/legal guardians gave their informed consent for inclusion before they participated in the study.
Not applicable.
This research was funded by Wuxi Municipal Health Commission Maternal and Child Health Research Project (No. FYKY202202).
The authors declare no conflicts of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.