








 , Jiexiong Huang 1, Xiaowei Luo 2, Liangli Hong 1, Qiancheng Qiu 1, Shuiqin Lin 1, Bin Wang 3
, Jiexiong Huang 1, Xiaowei Luo 2, Liangli Hong 1, Qiancheng Qiu 1, Shuiqin Lin 1, Bin Wang 31 Department of Pathology, The First Affiliated Hospital of Shantou University Medical College, 515041 Shantou, Guangdong, China
2 Department of Pathology, Hunan Provincial People’s Hospital, 410005 Changsha, Hunan, China
3 Department of Reproductive Medicine, The First Affiliated Hospital of Shantou University Medical College, 515041 Shantou, Guangdong, China
Abstract
Chronic endometritis (CE) is a prevalent gynecological disorder and a major cause of female infertility. However, clearly defined clinical or histopathological diagnostic criteria for CE are still lacking. Immunohistochemical (IHC) staining targeting plasma cell markers CD38 and CD138 has shown potential for diagnosing CE, but quantitative standards for these markers have not been established. This study aimed to determine quantitative thresholds of CD38- and CD138-positive plasma cells for the pathological diagnosis of CE, using hysteroscopic diagnosis as a reference, and to validate these thresholds by analyzing marker expression changes before and after anti-inflammatory therapy.
A total of 165 endometrial biopsy samples were collected from infertile women and subjected to IHC staining for CD38 and CD138. The number of CD38- and CD138-positive cells was counted in hotspot areas under a high-power field (HPF, 40 × 10 magnification). To determine optimal diagnostic criteria, we tested a series of quantitative thresholds [ranging from ≥1 to ≥10 positive cells/HPF] and analyzed the consistency between pathological diagnoses based on each threshold and hysteroscopic diagnoses. Additionally, 90 patients with CE who received anti-inflammatory therapy were included to compare CD38 and CD138 expression levels before and after treatment, and the negative conversion rate was calculated to verify the superiority of the identified thresholds.
(1) CD38 and CD138 showed no significant difference in plasma cell detection in endometrial tissue (p = 0.630), but their combined use improved clinical diagnostic concordance compared with single-marker staining. (2) When the diagnostic criterion was defined as an average of ≥5 CD38- and CD138-positive cells/HPF in hotspot areas, no significant difference was observed between pathological and hysteroscopic diagnoses (McNemar test, p = 0.233), with moderate consistency (Kappa = 0.422, p < 0.05). This threshold was optimal among all criteria tested. (3) The number of CD38- and CD138-positive cells decreased significantly after anti-inflammatory therapy in 90 patients (p < 0.001). Using an average of ≥4 CD38- and CD138-positive cells/HPF as the diagnostic criterion yielded the highest CE negative conversion rate after treatment, with a statistically higher rate than criteria 1–3 (p < 0.05), while no significant difference was observed among criteria 4–7.
We recommend combined hysteroscopic and pathological diagnosis for CE in infertile women. IHC staining for CD38 and CD138 provides reliable plasma cell identification and serves as an adjunctive tool for CE diagnosis. This study identifies an average of ≥5 CD38- and CD138-positive cells/HPF in hotspot areas as the primary reference cutoff for CE histopathologic evaluation, with moderate consistency with hysteroscopy (Kappa = 0.422), and ≥4 positive cells/HPF as the secondary cutoff for monitoring treatment response, which showed the highest negative-conversion rate (78.9%). Tailored to the diagnostic and treatment needs of infertile women, these clinically validated hierarchical thresholds, when integrated with hysteroscopy and histopathology, enhance the accuracy of adjunctive CE auxiliary diagnosis, and provide a targeted reference for clinical decision-making in infertility management and treatment response evaluation.
Keywords
- chronic endometritis
- plasma cells
- clinicopathology
- immunohistochemistry
- CD38
- CD138
Chronic endometritis (CE) presents as a type of persistent and chronic endometrial inflammation, and investigations have shown that the clinical symptoms of patients with CE are typically not obvious or mild. In clinical practice, it is usually considered that CE and recurrent abortion, infertility, and repeated embryo implantation failure are due to persistent and chronic inflammation of the endometrium that may affect endometrial receptivity [1]. The prevalence of CE in infertile women presently varies greatly in different studies, and one of the important reasons for this is the lack of a diagnostic standard and specific quantitative index for the diagnosis of CE.
Unlike acute endometritis, which is typically caused by direct intrauterine pathogen infection, CE is more closely linked to microbiome dysbiosis in the uterine cavity [2,3]. The uterine cavity is not absolutely sterile, and the imbalance of resident microbial communities—rather than single pathogenic organisms—may drive the persistent low-grade inflammation characteristic of CE [3,4]. However, the exact composition of dysbiotic microbiomes and their pathogenic mechanisms in CE remain incompletely elucidated [2]. The confounding effect of microbiome dysbiosis combined with acute pathogenic organisms has stunted progress in CE research to date, which is also reflected in our observation that microbial culture is not recommended for routine CE diagnosis [3].
CE can lead to infertility, as bacterial endotoxins derived from dysbiotic microbiota and subsequent endometrial microenvironment alterations may constitute one of the causes of implantation failure of healthy embryos [5]. In addition, various types of cytokines in the endometrium of CE patients participate in the pathologic process that subserves the promotion of B-cell differentiation and plasma cell functioning in endometrial homeostasis [6]. A majority of clinical investigators agree that the most effective treatment for restoring fertility in CE patients is the application of antibiotics. Studies have shown that curettage and antibiotic therapy reduce the degree of inflammation in CE patients [7], and it has been reported that patients with successfully treated CE demonstrate higher ongoing pregnancy, clinical pregnancy, and implantation rates than patients with persistent CE [8,9].
Histopathologic diagnosis is the gold standard for many diseases. The most specific and key histopathologic feature of CE is endometrial stromal plasma cell (ESPC) infiltration, which is widely recognized as a diagnostic indicator in clinical and research settings. However, the diagnostic criteria for accurately identifying ESPCs and the minimum number of ESPCs required for diagnosis remain ununified. Microscopic identification of plasma cells, monocytes, and plasmacytoid stromal cells is challenging. Late endometrial secretory phase changes, menstrual cycle characteristics, or secondary alterations induced by exogenous progesterone therapy before biopsy may mask plasma cell presence [10]. Moreover, normal endometrial stroma may contain individual plasma cells, while other pathological changes such as stromal spindle cell transformation, superficial mucosal interstitial edema, interstitial disruption, and focal lymphocyte aggregation lack specificity and clear clinical correlation [11,12,13].
Other common diagnostic methods for CE include hysteroscopy and microbial culture. Hysteroscopy is an important reference for CE diagnosis [14,15,16], with key manifestations including: ① diffuse endometrial congestion (the “strawberry sign”); ② endometrial thickening, edema, and focal congestion; and ③ scattered micropolyps on the endometrial surface [17,18]. Its advantage lies in intuitive visualization and overall assessment of endometrial conditions, but it has inherent subjectivity—different observers may interpret features like endometrial edema differently [19]. Although CE onset and progression are closely linked to microorganisms [3], microbial culture is not recommended for routine CE diagnosis. CE can be caused by various microorganisms (not just bacteria), and many bacteria are non-culturable, leading to technical limitations.
While ESPC infiltration is the consensus histopathologic diagnostic basis for CE, the minimum number of ESPCs required for diagnosis remains debated. Some studies propose diagnosing CE with ≥1 plasma cell per tissue section [20], while others require ≥4–6 plasma cells per high-power field (HPF) [18,21]. A nationwide survey in Japan [22] reported varied diagnostic cutoffs ranging from 3–5 cells/20 high-power fields for chronic endometritis. A systematic review and meta-analysis by Riemma et al. [23] further highlighted the variability in hysteroscopic diagnostic criteria across studies, emphasizing methodological inconsistencies in published reports. This discrepancy highlights the lack of standardized quantification criteria.
The use of immunohistochemical (IHC) staining for CD38 and CD138—classic plasma cell markers—has gained attention for CE diagnosis, but their application remains controversial. First, the specificity of these markers is not absolute. CD38 is not exclusive to plasma cells; it is also expressed on pre-B cells, immature B cells, and normal epithelial cells [24]. CD138 shows non-specific expression in secretory endometrial glands, metaplastic squamous epithelium, and trophoblast cells [25], which may lead to misidentification of non-plasma cell populations as ESPCs. Second, technical factors contribute to diagnostic variability. Non-specific cross-reactivity of CD138 IHC frequently occurs in endometrial epithelial cells, which may be misidentified as stromal plasma cells and lead to overdiagnosis of chronic endometritis [26]. Factors such as antigen retrieval time, primary antibody incubation duration, and antibody concentration can exacerbate this problem [27]. For example, prolonged antigen retrieval may increase non-specific binding, while inappropriate antibody dilution can enhance background staining. Third, clinical and histological confounders further complicate interpretation. The menstrual cycle phase affects endometrial morphology—secretory phase changes may mimic inflammatory infiltrates, and exogenous hormone therapy can alter marker expression [10]. Additionally, individual differences in immune status may lead to variable CD38/CD138 expression levels in plasma cells, affecting quantitative accuracy.
These controversies and potential false-positive sources have hindered the widespread acceptance of CD38/CD138 IHC as a standardized CE diagnostic tool. There is an urgent need to clarify the optimal application of these markers, including standardized staining protocols, quantitative thresholds, and combined interpretation strategies, to improve diagnostic reliability.
In this study, we aimed to address these gaps by: (1) optimizing CD38/CD138 IHC protocols to reduce non-specific staining; (2) comparing the diagnostic consistency of single vs. combined marker use; (3) determining optimal quantitative thresholds for CE diagnosis using hysteroscopy as a reference; and (4) validating these thresholds by analyzing marker expression changes before and after anti-inflammatory therapy. This research seeks to establish a hierarchical reference system for CD38/CD138-based CE diagnosis, providing a reliable basis for clinical decision-making.
This was a retrospective, single-center, observational study with a diagnostic test and therapeutic validation design. The study was conducted at the Reproductive Medicine Center of the First Affiliated Hospital of Shantou University Medical College between June 2020 and December 2021.
The research was divided into two core phases: ① Diagnostic threshold exploration phase: A total of 165 infertile women who underwent both hysteroscopy and endometrial biopsy were enrolled. Using hysteroscopic diagnosis as the clinical reference standard, we evaluated the diagnostic performance of different quantitative thresholds of CD38- and CD138-positive cells (≥1 to ≥10 cells/HPF) via IHC staining, aiming to identify the optimal threshold for pathological diagnosis of CE. ② Therapeutic validation phase: Among the 165 enrolled patients, 90 cases diagnosed with CE (based on preliminary pathological criteria) who received standardized anti-inflammatory therapy and underwent post-treatment endometrial biopsy were included. We compared the changes in CD38- and CD138-positive cell counts before and after treatment, and calculated the negative-conversion rate to validate the clinical utility of the identified thresholds.
All study procedures, including patient enrollment, sample collection, IHC staining, result interpretation, and data analysis, were performed in accordance with standardized operating protocols. Two independent pathologists blinded to the hysteroscopic results conducted the IHC staining interpretation and cell counting to minimize observer bias. The statistical analysis plan was pre-specified to assess diagnostic consistency (Kappa test, McNemar test) and therapeutic response (Wilcoxon rank-sum test), ensuring the rigor and objectivity of the study.
We collected pathological paraffin blocks, hysteroscopic findings, and relevant clinical data from 165 infertile patients who visited the Reproductive Medicine Center of the First Affiliated Hospital of Shantou University Medical College from June 2020 to December 2021. Hematoxylin and eosin staining staining and immunohistochemical staining were performed on the paraffin blocks for subsequent analysis.
Our enrollment criteria were as follows:
(1) infertile women aged 20–45 years;
(2) patients who were not previously diagnosed with CE and never received systemic treatment;
(3) patients who were informed as to our study and agreed to undergo hysteroscopy and endometrial tissue pathological biopsy; and
(4) clinical and pathologic case data that were relatively complete.
Exclusion criteria were as follows:
(1) a previous diagnosis of CE;
(2) a history of endometrial malignant tumors;
(3) recent acute reproductive tract or uterine infection;
(4) recent receipt of a large number of antibiotics; and
(5) women who had ever received CE or infertility-related treatment.
In addition, to minimize biological variability caused by menstrual cycle phases, only endometrial tissues sampled during the proliferative phase were included. The proliferative phase was confirmed based on the patient’s last menstrual period and histomorphological features of the endometrium (e.g., glandular structure, stromal cell density, and absence of secretory changes), ensuring uniform hormonal background across all specimens.
Clinical data included the patient’s age, pregnancy history, and the gross appearance of the endometrium during hysteroscopy. All data were collected from clinical medical records and pathology application forms.
Hysteroscopic CE criteria were meeting any or several of the following: ① endometrial mucosa showing diffuse congestion, and a congested endometrial middle with a white center point, such as “strawberry sign”; ② endometrial thickening, edema, and focal congestion; and ③ coverage of the endometrial surface by scattered micropolyps (referred to as multiple polyps <1 mm in diameter).
The chief instruments, antibodies, reagents, and other consumables required for the study are shown in Tables 1,2,3.
| Antibody type | Clone number | Reagent concentration | Company |
|---|---|---|---|
| CD38 | MX044 | 1:100 | China Fuzhou Maixin Biotechnology Development Co., Ltd., Fuzhou, Fujian, China |
| CD138 | Ml15 | 1:100 | China Fuzhou Maixin Biotechnology Development Co., Ltd., Fuzhou, Fujian, China |
| Instrument name | Model | Company |
|---|---|---|
| Paraffin-based tissue embedding machine | Leica EG1160 | LEICA, Wetzlar, Hesse, Germany |
| A paraffin-based tissue microtome | Leica RM2235 | LEICA, Wetzlar, Hesse, Germany |
| Fully automated IHC staining apparatus | AS300 | Shenzhen Daan Material Technology Co., Ltd., Shenzhen, Guangdong, China |
| Slide flotation machine | YABO 200 | Changzhou Yabo Electronic Equipment Co., Ltd., Changzhou, Jiangsu, China |
| Electric heating constant temperature blast-drying box | DHG-9070A | Shanghai Yiheng Technology Co., Ltd., Shanghai, China |
| Water-insulated electric heating incubator | The PYX-DHS-40X50 model | Shanghai Yuejin Medical Device, Shanghai, China |
| Electromagnetic oven | / | Midea Electric Appliance Company, Foshan, Guangdong, China |
| Side-by-side refrigerator | / | Midea Electric Appliance Company, Foshan, Guangdong, China |
| Forward placement microscope and imaging system | OLYMPUS BX51 | OLYMPUS Corporation, Tokyo, Japan |
| Liquid transfer gun | / | Eppendorf SE, Hamburg, Germany |
| Autoclave | GB13623-2003 | Supor Electric Appliance Company, Hangzhou, Zhejiang, China |
IHC, immunohistochemical.
| Material type | Catalog Number | Company |
|---|---|---|
| Diaminobenzidine (DAB) Chromogen Kit | (240)06396500188 | Roche Diagnostics GmbH, Mannheim, Germany |
| Ethyl alcohol | 1280340101601 | Xilong Science Co., Ltd., Shantou, Guangdong, China |
| Dimethylbenzene | 1210000101601 | Xilong Science Co., Ltd., Shantou, Guangdong, China |
| Formaldehyde | 1340040101601 | Xilong Science Co., Ltd., Shantou, Guangdong, China |
| Hematoxylin dye, liquid | (240)05277965001 | Roche Diagnostics GmbH, Mannheim, Germany |
| Eosin stain | BA4022 | Zhuhai Besso Biotechnology Co., Ltd., Zhuhai, Guangdong, China |
| Reaction Buffer Concentrate 10X | (240)05353955188 | Roche Diagnostics GmbH, Mannheim, Germany |
| Ethylenediaminetetraacetic acid (EDTA) | (240)05424569188 | Roche Diagnostics GmbH, Mannheim, Germany |
| Concentrated hydrochloric acid | 3203111 | Guangzhou Wexis Biotechnology Co., Ltd., Guangzhou, Guangdong, China |
| Microtome knife | PP3053835BR02 | KAI INDUSTRIES CO., LTD., Tokyo, Japan |
| Cationic anti-stripping slides | PRO-04 | Matsunami Glass Ind., Ltd., Izumi, Osaka, Japan |
| Neutral gum | 00210277 | Shanghai Specimen Model Factory, Shanghai, China |
| 3% Hydrogen peroxide solution | 0644070159 | Roche Diagnostics GmbH, Mannheim, Germany |
All endometrial specimens were exposed to 10% neutral formalin solution within 30 minutes after removal, and all specimens were collected by a pathologist according to the pathologic material specifications. After extraction, the tissue was further fixed, dehydrated, rendered transparent, and then embedded in paraffin. We subsequently again determined the basic information, such as wax block number, hospitalization number, name, sex, and age. The wax blocks were contiguously sliced at a 3-μm thickness. Anti-stripping slides were used for section adherence, and the slides were heated at a constant temperature for 1 hour.
The H&E staining method, which is one of the most widely used paraffin section staining methods in scientific research and clinical work, was adopted herein. Under the action of alkaline hematoxylin and acidic eosin, the basophilic nuclear chromatin and eosinophilic cytoplasm and extracellular matrix will appear blue–purple and red, respectively. The specific steps used for H&E staining were as follows:
(1) A glass slide was placed on a glass slide frame, and the glass slide frame was soaked in three cylinders of xylene solution for 10 minutes each, followed by soaking in absolute ethanol, 95% ethanol, 90% ethanol, and 80% ethanol solutions for 2 minutes each.
(2) The frame was washed with running water for 2 minutes, soaked in hematoxylin dye solution for 10 minutes, then flushed with running water for several seconds.
(3) The frame was immersed in 0.5% hydrochloric acid alcohol for 5 seconds, soaked in saturated lithium carbonate solution for several seconds, and then flushed with flowing water for several seconds.
(4) The frame was then soaked in water-soluble eosin staining solution for 1 minute, after which it was rinsed with running water for several seconds.
(5) The frame was then soaked in 80% ethanol, 90% ethanol solution, and absolute ethanol for 2 minutes each, after which it was placed in three cylinders of xylene for 2 minutes each and sealed with neutral gum.
The film was then observed under a microscope.
The specific steps for IHC staining were as follows:
(1) We placed the glass slide on the glass slide frame and soaked the glass slide frame in three cylinders of xylene solution for 10 minutes each.
(2) We then serially dipped the slides in absolute ethanol, 95% ethanol, 90% ethanol, and 80% ethanol solution for 2 min each.
(3) We rinsed the slides with running water for 2 min and thrice soaked them in phosphate-buffered saline (PBS) solution for 3 min each time.
(4) The slides were placed in a peroxidase blocking agent of 3% hydrogen peroxide solution for 10 min, then soaked in the configured ethylenediaminetetraacetic acid (EDTA) repair solution for antigen repair, and washed in PBS solution thrice for 3 min each.
(5) We added primary antibody and incubated the complex for 2 h at room temperature and washed the slides in PBS solution thrice for 3 min each time.
(6) The secondary antibodies were added and incubated for 20 min at room temperature, and slides were washed thrice in PBS solution for 3 min.
(7) Color development of the diaminobenzidine (DAB) mixture was as follows. We left the slides at room temperature for 6 min, then rinsed them in water to stop color development, held slides in hematoxylin for 8 min at room temperature, washed with running water and dipped in 0.5% hydrochloric acid alcohol for 5 s for differentiation.
(8) We flushed the slides with water, dipped them in saturated lithium carbonate solution for several seconds, and then again flushed them with flow-through water.
(9) Subsequently, we soaked the slides in 75% ethanol, 95% ethanol solution, and absolute ethanol consecutively for 2 min each.
(10) Then, we held slides in three-cylinder xylene for 2 min each, sealed them with neutral tree gum sealant, and finally analyzed them microscopically.
All stained sections were evaluated and counted by two experienced pathologists. CD138 exhibited membranous and cytoplasmic positivity, while CD38 showed exclusive membranous positivity. We observed constitutive stromal CD138 expression in proliferative-phase endometria—characterized by diffuse weak staining with indistinct cell boundaries, which is considered physiological background expression rather than pathological plasma cell infiltration. To avoid potential misclassification of stromal background staining as specific plasma cell positivity, our senior pathological technicians optimized the CD138 protocol via long-term validation:
Antigen retrieval: Reduced from 24 to 16 min (Cell Conditioner #1, 100 ℃) to minimize non-specific antibody binding [27] while preserving epitope exposure;
Primary antibody incubation: Shortened from 28 to 20 min (anti-CD138, PREP KIT 34) to attenuate background adsorption without compromising specific plasma cell staining [27].
This optimized protocol (Laboratory Protocol #534: CD138, 16-20) enhanced specificity by retaining distinct target signals and weakening diffuse stromal non-specific staining, alongside stringent morphological interpretation criteria for distinguishing specific plasma cell staining from physiological background expression.
Specific CD138 positivity: Defined as membranous/cytoplasmic brownish-yellow staining with clear cell boundaries (plasma cell phenotype); We observed constitutive stromal CD138 expression in proliferative-phase endometria—characterized by diffuse weak staining with indistinct cell boundaries, which is considered physiological background expression rather than pathological plasma cell infiltration (confirmed non-specific by protocol optimization).
Dual-marker verification: Only CD138+/CD38+ cells were counted. Combined markers improve plasma cell identification specificity and effectively exclude single-marker background staining (e.g., CD138 physiological stromal expression) [25].
To further validate that our approach excluded physiological CD138 expression, we compared CD138+/CD38+ cell counts between hysteroscopically confirmed CE-negative (n = 67) and CE-positive (n = 98) groups. In CE-negative cases, the median number of CD138+/CD38+ cells/HPF was 1 [interquartile range(IQR): 0–2], which was significantly lower than the median of 6 (IQR: 4–8) in CE-positive cases (p < 0.001). This finding confirms that physiological background expression was negligible under our optimized protocol and interpretation criteria, and did not interfere with pathological plasma cell quantification.
After a complete analysis of the entire section, positive cell hotspots were localized. For the definition of hotspots, we identified the single most concentrated area of CD38+/CD138+ positive cells (dense aggregation). Cell counting was performed exclusively in this single hotspot under one high-power field (40 × 10 magnification), rather than averaging counts across multiple HPFs. This approach ensures consistency with the clinical practice of prioritizing the most prominent pathological lesion for diagnostic reference. We acknowledge that a whole section counting approach has been validated in the literature as the method with the lowest intra- and inter-observer variability for plasma cell quantification in endometrial tissues [28]. This approach involves systematic counting of positive cells across the entire endometrial section, minimizing sampling bias by capturing the spatial distribution of plasma cells. However, to maintain consistency with the majority of existing CE diagnostic studies [21,22], which predominantly adopt hotspot-based counting (focusing on the most concentrated area of positive cells), we selected the single hotspot counting method for our analysis. Notably, our optimized staining protocol (reduced antigen retrieval time and primary antibody incubation duration) and strict dual-marker verification (only CD38+/CD138+ cells with clear morphological features were counted) were implemented to mitigate potential variability associated with hotspot selection. While the whole section approach offers superior reproducibility, our method aligns with clinical practice and literature conventions, facilitating direct comparison of our proposed thresholds with previous findings. We recognize the trade-off between reproducibility and consistency with existing data, and this consideration is highlighted to allow readers to make an informed appraisal of our results. The number of CD138- and CD38-positive cells in the hotspot was recorded as shown in Fig. 1 (400×).
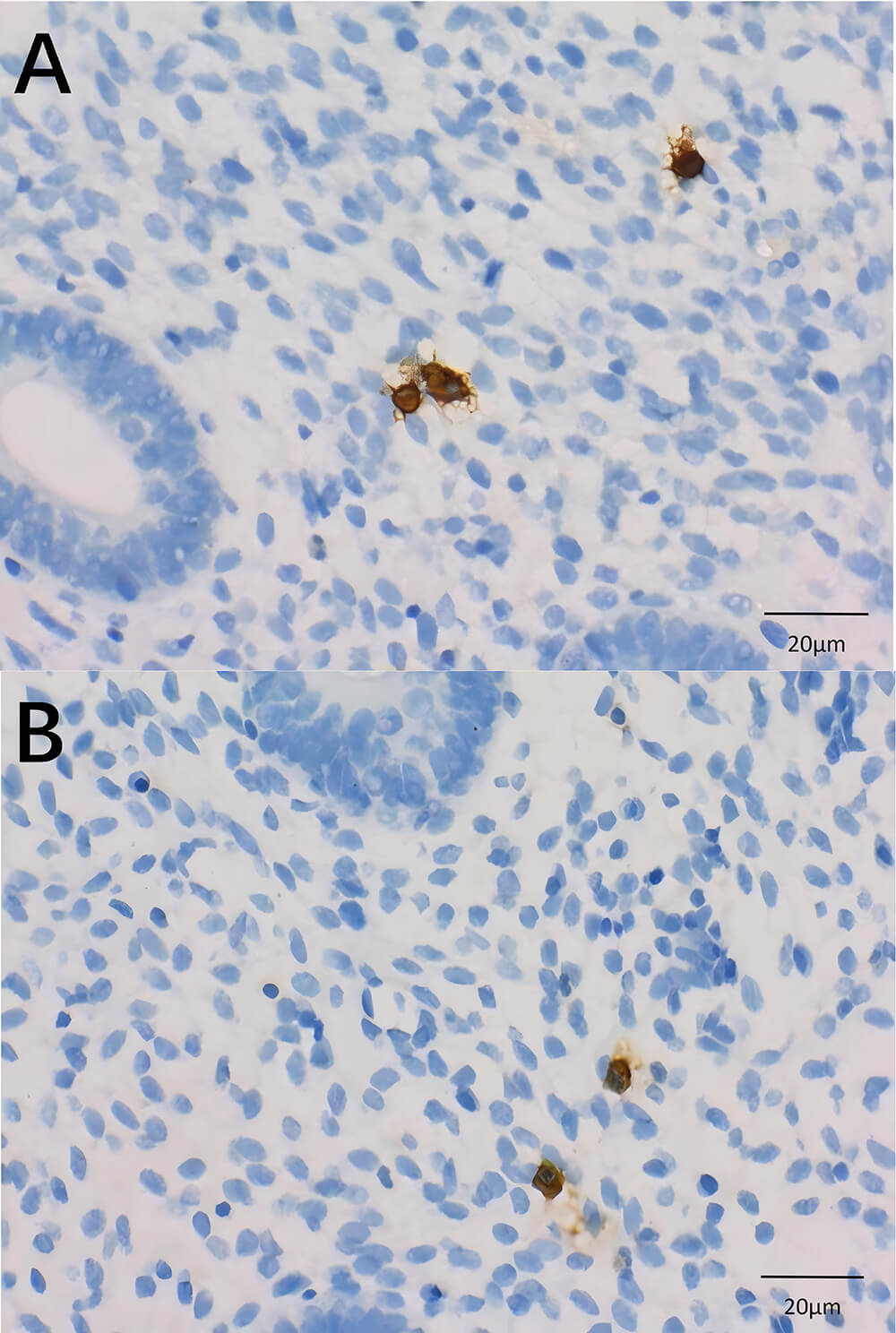 Fig. 1.
Fig. 1.Interpretative criteria using IHC. (A) CD138-positive cells, with the membrane and cytoplasm stained brownish yellow. (B) CD38-positive cells, with membranes stained brownish yellow (magnification, 400×). Scale bar: 20 μm.
2.4.5.1 CE Diagnostic Criteria were Preset
With reference to the relevant literature [28,29], we preset 10 CD138- and CD38-positive cells as quantification criteria for the gradient as CE pathologic diagnostic criteria:
preset standard 1: ≥1 hotspot-positive cells/HPF to diagnose CE;
preset standard 2: ≥2 hotspot-positive cells/HPF to diagnose CE;
preset standard 3: ≥3 hotspot-positive cells/HPF to diagnose CE;
preset standard 4: ≥4 hotspot-positive cells/HPF to diagnose CE;
preset standard 5: ≥5 hotspot-positive cells/HPF to diagnose CE;
preset standard 6: ≥6 hotspot- positive cells/HPF to diagnose CE;
preset standard 7: ≥7 hotspot-positive cells/HPF to diagnose CE;
preset standard 8: ≥8 hotspot-positive cells/HPF to diagnose CE;
preset standard 9: ≥9 hotspot-positive cells/HPF to diagnose CE;
preset standard 10: ≥10 hotspot-positive cells/HPF to diagnose CE.
2.4.5.2 Grouping of CD138 and CD38 Staining Results
To further explore how to combine CD38 and CD138 to improve the consistency between pathologic diagnosis and clinical hysteroscopic diagnosis, the experimental data after IHC staining were subdivided into five groups under the proposed quantitative index as follows:
A CD38-positive group: that is, the number of CD38-staining positive cells was taken as the standard, regardless of the number of CD138-positive cells.
A CD138-positive group: that is, the number of positive cells stained with CD138 was taken as the standard, regardless of the number of CD38-positive cells.
Both CD38- and CD138-positive groups: that is, the number of positive cells stained for both CD38 and CD138 met the criteria.
CD38- or CD138-positive group: that is, the number of positive cells stained for CD38 or CD138 met one of the criteria.
CD38 and CD138 mean positive group: the number of positive cells stained for CD38 or CD138 was counted, and the average that met the criteria was interpreted as positive.
The anti-inflammatory treatment administered to the 90 CE patients was standardized empirical antibiotic therapy, consistent with the core recommendations of the Expert Consensus on the Diagnosis and Treatment of Fertility-Related Chronic Endometritis (2025 Edition) [18]. The specific protocol and implementation details were unified to ensure the reliability of therapeutic validation:
Treatment agent and dosage: All patients received the same combined antibiotic regimen: oral doxycycline 100 mg twice daily + oral metronidazole 500 mg three times daily. This regimen was selected based on the consensus that CE is predominantly caused by bacterial infections (e.g., Escherichia coli, Enterococcus faecalis) and mycoplasma [18], and the combination covers both aerobic and anaerobic pathogens with proven efficacy in CE treatment [9,18].
Treatment timing: Therapy was initiated within 1 week after the initial endometrial biopsy and pathological confirmation of CE. To avoid hormonal interference, the 14-day full course was completed within a single menstrual cycle (proliferative phase to early secretory phase), as recommended by the consensus [18].
Treatment standardization and monitoring: All patients were instructed to complete the full course without interruption. Clinical follow-up was conducted at 2 weeks post-treatment to assess adherence and adverse reactions (e.g., gastrointestinal discomfort), with no serious side effects reported.
Post-treatment biopsy timing: Endometrial re-biopsy was performed in the proliferative phase of the next menstrual cycle (7–14 days after the last menstrual period), ensuring a consistent hormonal background with the initial biopsy to minimize variability in CD38/CD138 expression due to cycle phase [18].
The above data were collected and collated, and statistical analysis was performed using SPSS 25.0 (IBM Corporation, Armonk, NY, USA). All statistical tests were two-sided to comprehensively assess potential differences or correlations in both directions, ensuring the objectivity and rigor of the analysis.
Measurement data were analyzed using the Mann-Whitney U test (for comparing CD38 and CD138 positive cell counts), and the Wilcoxon signed-rank test (for analyzing pre- and post-treatment differences), with statistical significance indicated at p < 0.05. Counting data were analyzed using the χ2 test, including the paired χ2 test (McNemar test) for evaluating consistency between pathological and hysteroscopic diagnoses, and the Kappa consistency test for assessing agreement between the two methods. For the McNemar test, p < 0.05 indicated a significant difference between the two diagnostic methods, while p > 0.05 indicated no statistically significant difference. For the Kappa consistency test: a Kappa value <0.40 indicated poor agreement, 0.40≤ Kappa value <0.75 indicated moderate agreement, and a Kappa value ≥0.75 indicated good agreement.
For the CD138 threshold variability across studies, the 95% CI was calculated using a random-effects model to account for inter-study heterogeneity.
For the negative-conversion rate of the ≥4 CD38/CD138 positive cells/HPF threshold in the therapeutic validation phase, the 95% CI was computed using the Wilson score method, which is robust for binomial proportion data and provides reliable estimates even for small sample sizes.
For the Kappa consistency coefficient (κ = 0.422) between the pathological diagnosis (≥5 CD38/CD138 positive cells/HPF) and hysteroscopic diagnosis, the 95% CI was calculated using the standard error method for Kappa coefficients, further supporting the reliability of the moderate consistency between the two diagnostic methods.
Post-hoc power analysis was performed using G*Power 3.1 software (Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany) to verify the adequacy of the sample size:
Based on the Kappa consistency coefficient (κ = 0.422) between the pathological diagnosis (≥5 CD38/CD138 positive cells/HPF) and hysteroscopic diagnosis, parameters were set as follows: α = 0.05 (two-sided), sample size n = 165, Kappa effect size f = 0.25 (defined as a moderate effect size for Kappa consistency analysis). The post-hoc power was calculated to confirm sufficient power to detect the moderate consistency between the two diagnostic methods with a low probability of type II error.
For the McNemar paired difference analysis (p = 0.233) between the two diagnostic methods, the post-hoc power was calculated based on the discordant rate (27.3%, 45/165). With α = 0.05 (two-sided) and sample size n = 165, the post-hoc power was computed to confirm that the study had adequate power to detect potential differences in diagnostic results between hysteroscopy and histopathology.
To further validate the optimal diagnostic thresholds of CD38- and CD138-positive cell counts, sensitivity, specificity, and receiver operating characteristic (ROC) curve analysis were performed. Hysteroscopic diagnosis was used as the gold standard for defining true positive (TP), true negative (TN), false positive (FP), and false negative (FN) cases.
Sensitivity: The proportion of truly CE-positive patients (hysteroscopy-positive) correctly identified by the CD38/CD138 threshold, calculated as TP/(TP + FN).
Specificity: The proportion of truly CE-negative patients (hysteroscopy-negative) correctly identified by the threshold, calculated as TN/(TN + FP).
Area under the ROC curve (AUC): A summary metric reflecting the overall diagnostic performance of the threshold, with values ranging from 0.5 (no diagnostic value) to 1.0 (perfect diagnostic value).
ROC curves were plotted for each of the four marker combinations (CD38-positive, CD138-positive, CD38- and CD138-positive, CD38- or CD138-positive) across the 10 preset quantitative thresholds (≥1 to ≥10 cells/HPF). The AUC was calculated for each curve to compare diagnostic efficacy between marker combinations.
The optimal threshold for each marker combination was determined by the Youden index (Youden index = sensitivity + specificity – 1), which maximizes the balance between sensitivity and specificity.
Statistical comparisons of AUC values between different marker combinations were conducted using the DeLong test to assess significant differences in diagnostic performance. AUC values threshold were reported with 95% confidence intervals (CIs) calculated using the Wilson score method. All analyses were performed using SPSS 25.0, with p < 0.05 considered statistically significant.
We enrolled a total of 165 female patients with a median age of 32 (23–43 in December 2021), with 42 at or over 35 years of age (25.5%) and 123 under 35. Of these, 50 (30.3%) were clinically diagnosed with primary infertility and 115 (69.7%) with secondary infertility, and 98 (59.4%) patients showed positive hysteroscopic results. Among them, some showed diffuse endometrium with scattered white dots. There were six cases (3.6%) with “strawberry sign” and 65 with endometrial thickening and edema, with/without focal congestion (39.4%). The remaining 27 cases (16.4%) in the CE-positive group presented with multiple small polyps. A total of 67 cases (40.6%) had normal hysteroscopic morphology without any characteristic CE manifestations and were classified as CE negative (see Table 4).
| Clinicopathologic features | N (%) (n = 165) | |
|---|---|---|
| Age | ||
| Median (M) | 32 (29–35) | |
| <35 Years old | 123 (74.5%) | |
| ≥35 years old | 42 (25.5%) | |
| Clinical diagnosis | ||
| Primary infertility | 50 (30.3%) | |
| Secondary infertility | 115 (69.7%) | |
| Hysteroscopic diagnostic results | ||
| CE positive | 98 (59.4%) | |
| “Strawberry sign” | 6 (3.6%) | |
| Neointimal thickening, edema, and/or congestion | 65 (39.4%) | |
| Multiple small polyps | 27 (16.4%) | |
| CE negative | 67 (40.6%) | |
Note: Data are presented as percentages or medians (M). n, number of samples.
Infiltration of ESPCs is currently accepted as the histologic manifestation of classical CE. However, upon removal of the characteristic ESPC infiltration, nonspecific changes in endometrial stroma exert an effect on CE, and these manifestations may be secondary changes caused by persistent and chronic inflammation [11]. As observed in this study, the changes in endometrial stroma were diverse, including stromal spindle cell changes, interstitial edema, mesenchymal rupture, and focal lymphocyte aggregation (Fig. 2); these changes were masked in the stroma, and ESPCs proved hard to find. Therefore, it was difficult to accurately identify and count ESPCs in H&E-stained sections.
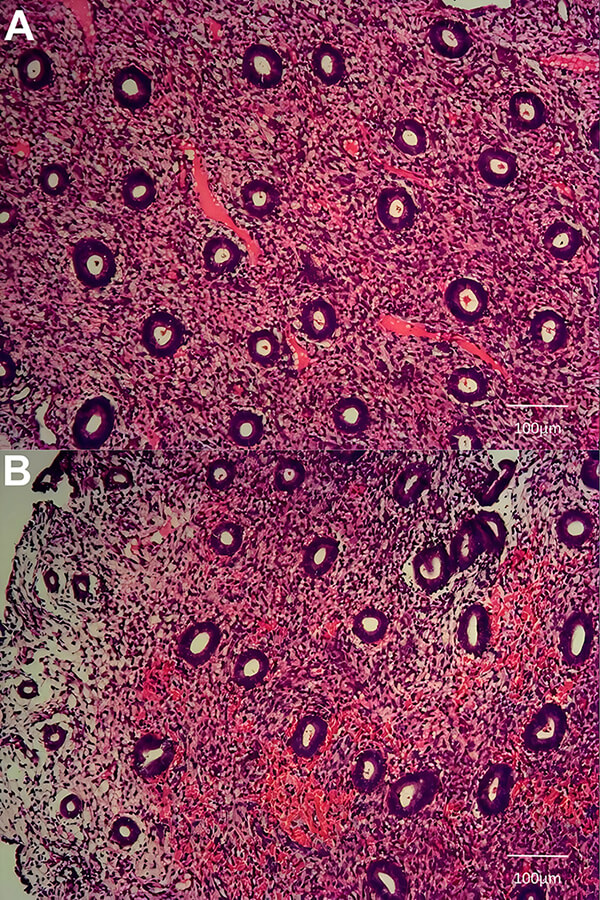 Fig. 2.
Fig. 2.Histopathological changes of endometrial stroma in chronic endometritis. (A) Endometrial stroma with extensive congestion. (B) Endometrial stroma with edema and spindle cell-like changes (magnification, 100×). Scale bar: 100 μm.
Two plasma cell-specific immunophenotype antibodies to CD38 and CD138 were used herein to jointly assist in the recognition of ESPCs, and the staining results are shown in Fig. 3. After IHC staining, we counted positive cells in the hotspot of each section at high magnification and then further evaluated the results. The results showed that the median for CD38-positive cell number was 5 (M: 2–7), while the median for CD138-positive cells was 5 (M: 2–6.5) (the specific results are shown in Fig. 4).
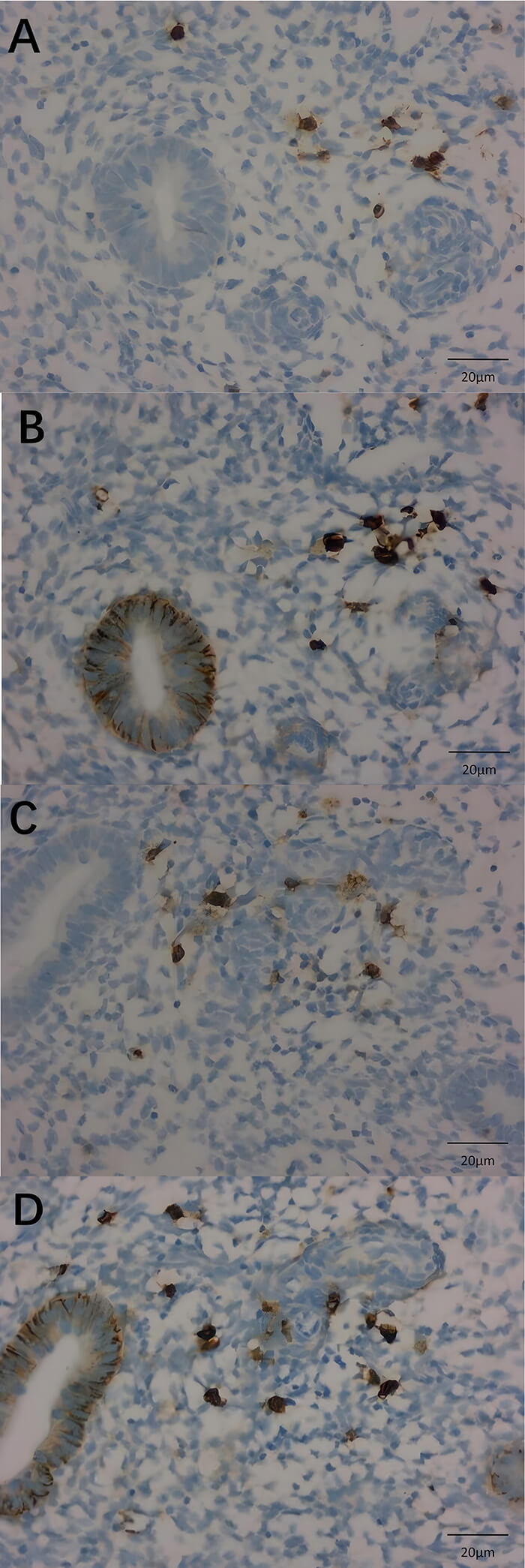 Fig. 3.
Fig. 3.CD38- and CD138-staining results. (A) and (C) denote CD38 staining, and (B) and (D) denote CD138 staining. (A–D) are magnified in the same field (400×). Scale bar: 20 μm.
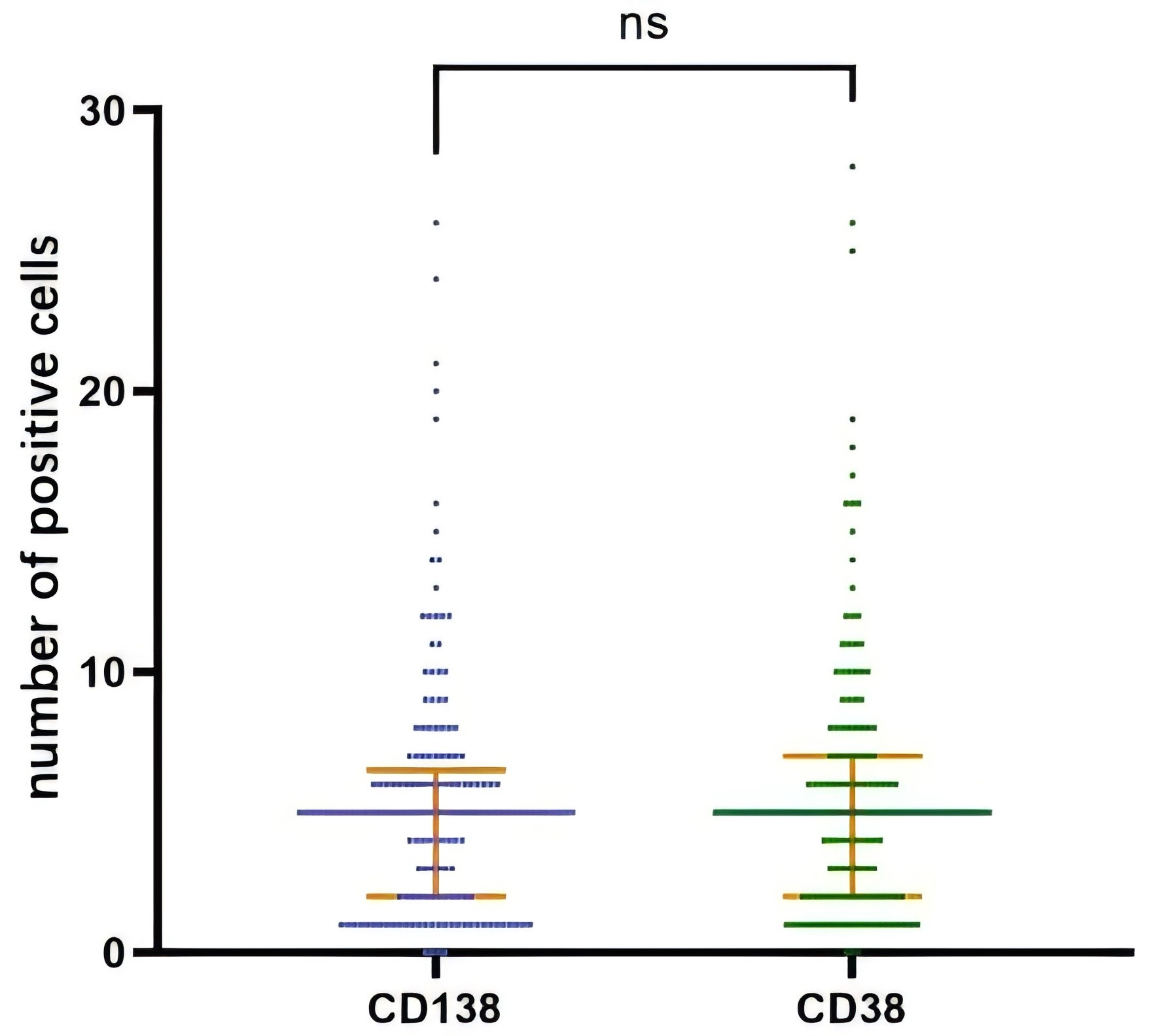 Fig. 4.
Fig. 4.Results of IHC staining for CD138 and CD38. Note: ns, not significant; orange lines indicate the median and interquartile range.
We subsequently compared results using the Mann-Whitney U test and found no difference in the number of CD38 and CD138 cells in a high-magnification microscopic field in the hotspot (p = 0.630 > 0.050). This indicated that although there were some differences in the cellular profiles regarding the positive expression of the respective cells, the results for CD38 and CD138 positivity in endometrial tissue with respect to ESPC recognition were relatively consistent.
ROC curve analysis was performed with hysteroscopic diagnosis as the reference standard to evaluate the diagnostic performance of the CD38/CD138 mean value (Fig. 5).
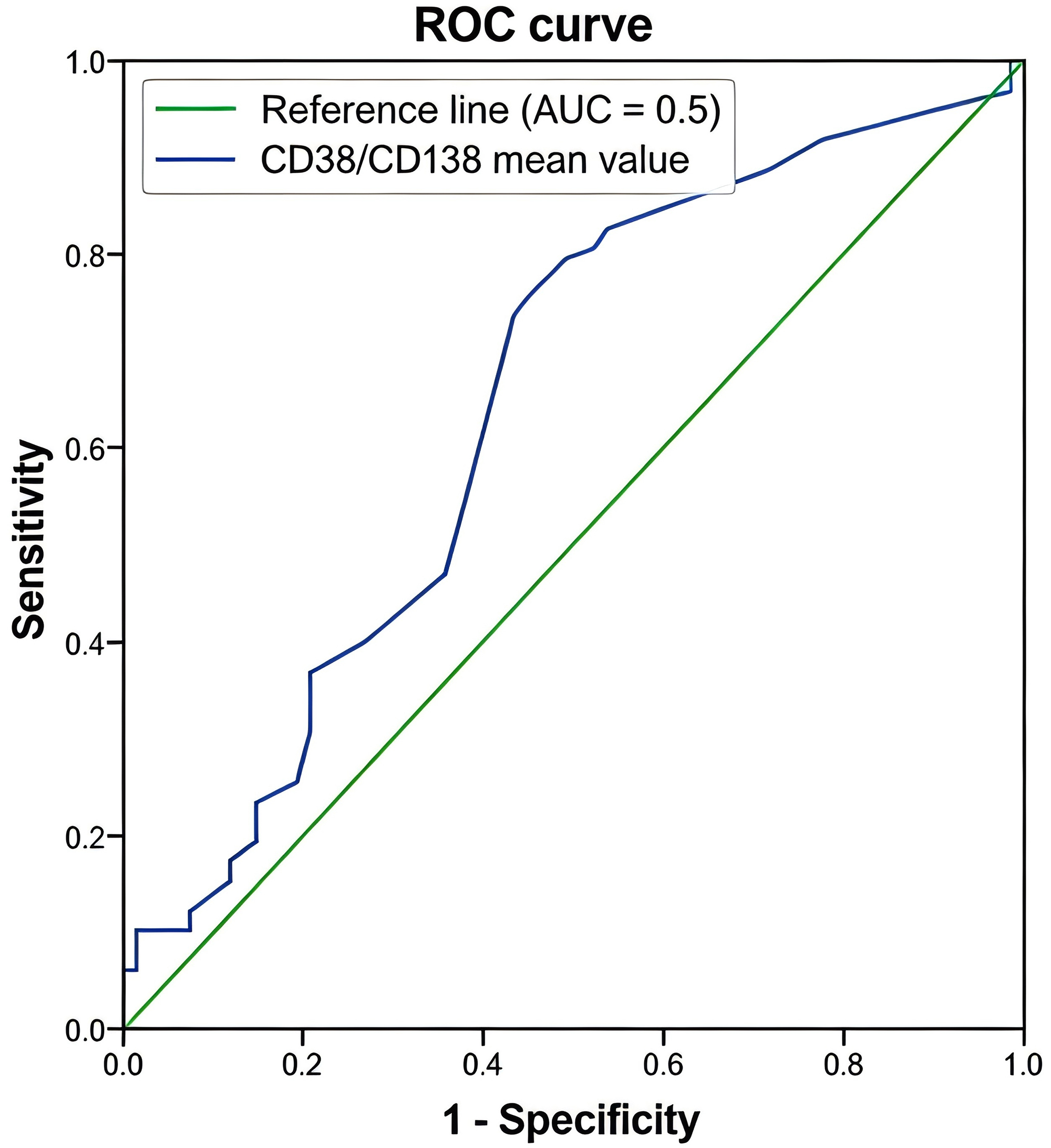 Fig. 5.
Fig. 5.ROC curve for the diagnostic performance of CD38/CD138 mean value in chronic endometritis. The blue curve represents the ROC curve of the CD38/CD138 mean value (AUC = 0.642, 95% CI: 0.554–0.730). The green solid line indicates the reference line (AUC = 0.5), corresponding to no diagnostic value. The Y-axis denotes Sensitivity (true positive rate), and the X-axis denotes 1 - Specificity (false positive rate). ROC,receiver operating characteristic; AUC, area under the ROC curve.
AUC: The AUC for the CD38/CD138 mean value was 0.642 (95% CI: 0.554–0.730, asymptotic p = 0.002), indicating moderate diagnostic efficacy.
Optimal threshold by Youden index: The Youden index (sensitivity + specificity – 1) was maximized at a mean value of 4.25 cells/HPF (Youden index = 0.307), with corresponding sensitivity of 0.755, 1-specificity of 0.448, and specificity of 0.552 (Table 5).
| Threshold (Mean Cells/HPF) | Sensitivity | 1-Specificity | Specificity | Youden index |
|---|---|---|---|---|
| 4.00 | 0.796 | 0.493 | 0.507 | 0.303 |
| 4.25 (ROC-derived optimal) | 0.755 | 0.448 | 0.552 | 0.307 |
| 5.00 | 0.735 | 0.433 | 0.567 | 0.302 |
Note: 1-Specificity corresponds to the false positive rate. Youden Index = Sensitivity + Specificity – 1, representing the balance of diagnostic efficiency.
ROC curve characteristics: The curve exhibited a gradual rise in sensitivity with decreasing specificity across the tested thresholds (ranging from –1 to 26.5 cells/HPF). Key threshold points aligned with the pre-specified diagnostic and treatment monitoring thresholds:
At 4.0 cells/HPF: Sensitivity = 0.796, Specificity = 0.507, Youden index = 0.303.
At 5.0 cells/HPF: Sensitivity = 0.735, Specificity = 0.567, Youden index = 0.302.
The pre-specified primary diagnostic threshold (5.0 cells/HPF) maintained a Youden index close to the ROC-derived optimal value (0.302 vs. 0.307), confirming its balanced sensitivity and specificity for clinical diagnosis.
Based on the optimal diagnostic threshold identified in this study (average of ≥5 CD38- and CD138-positive cells/HPF in the hotspot area), the histopathological prevalence of CE among the 165 enrolled infertile women was 64.8% (107/165).
This prevalence was calculated as follows: Using the hierarchical cutoff system proposed in the study, the primary diagnostic threshold (≥5 positive cells/HPF) was adopted to define histopathologically confirmed CE. Among the 165 patients, 107 cases met this criterion, accounting for 64.8% of the total study population.
The hysteroscopic prevalence of CE in this study was 59.4% (98/165), as previously reported in Table 4. The histopathological prevalence (64.8%) is slightly higher than the hysteroscopic prevalence, which is consistent with the clinical reality that IHC can detect subtle plasma cell infiltration that is not always visible under hysteroscopy [18]. This prevalence is also in line with the range of CE prevalence (26.38%–36.32%) reported in the Expert Consensus on the Diagnosis and Treatment of Fertility-Related Chronic Endometritis (2025 Edition) [18] for infertile and recurrent implantation failure (RIF) populations, confirming the reliability of our data.
The histopathological prevalence of 64.8% further supports the clinical relevance of our proposed threshold: it reflects the actual burden of CE in infertile women based on objective plasma cell quantification, avoiding overdiagnosis from overly loose thresholds or underdiagnosis from overly strict ones. This prevalence is comparable to the 32%–45% histopathological prevalence reported in similar studies [29], indicating consistency with current research findings in the field.
In this study component, we attempted to alter the minimal number of the quantification standard of plasma cells, so as to further interpret the number of CE-positive and -negative patients under different criteria, and also to introduce the hysteroscopic diagnostic results of patients. A paired χ² test (McNemar test) and the Kappa consistency test were employed for the above data.
(1) The specific statistical results of the CD38-positive group are shown in Table 6. We ascertained that when the quantification standard was set at ≥5 hotspot-positive cells/HPF, p > 0.050 indicates no statistically significant difference was detected. from the hysteroscopic results (McNemar test, p = 0.401 > 0.050), with weak consistency (Kappa value = 0.348 < 0.400). Under the remaining criteria, we noted significant differences between the pathologic diagnosis and the hysteroscopic diagnostic results (McNemar test, p-value < 0.05).
| Preset quantification standard | N (%) (n = 165) | McNemar test | Kappa consistency test | |||
|---|---|---|---|---|---|---|
| Both positive | Both negative | Discordant | p-value | Kappa value | p-value | |
| Standard 1 | 96 (58.2%) | 1 (0.6%) | 68 (41.2%) | 0.001 | 0.006 | 0.796 |
| Standard 2 | 88 (53.3%) | 15 (9.1%) | 62 (37.6%) | 0.001 | 0.135 | 0.032 |
| Standard 3 | 82 (49.7%) | 26 (15.8%) | 57 (34.5%) | 0.001 | 0.239 | 0.001 |
| Standard 4 | 80 (48.5%) | 32 (19.4%) | 53 (32.1%) | 0.007 | 0.334 | 0.001 |
| Standard 5 | 76 (46.1%) | 38 (23.0%) | 51 (30.9%) | 0.401 | 0.348 | 0.001 |
| Standard 6 | 42 (25.5%) | 49 (29.7%) | 74 (44.8%) | 0.001 | 0.147 | 0.036 |
| Standard 7 | 30 (18.2%) | 52 (31.5%) | 83 (50.3%) | 0.001 | 0.073 | 0.244 |
| Standard 8 | 25 (15.2%) | 55 (33.3%) | 85 (51.5%) | 0.001 | 0.066 | 0.250 |
| Standard 9 | 20 (12.1%) | 58 (35.2%) | 87 (52.7%) | 0.001 | 0.060 | 0.248 |
| Standard 10 | 18 (10.9%) | 60 (36.4%) | 87 (52.7%) | 0.001 | 0.068 | 0.164 |
Note: Both positive = Concurrent positive results of CD38 staining and hysteroscopy; Both negative = Concurrent negative results of CD38 staining and hysteroscopy; Discordant = Inconsistent results between the two methods. HPF = high-power field (40 × 10 magnification). All data were analyzed using the paired chi-square test (McNemar test) and Kappa consistency test. Data are presented as n (%).
(2) The specific statistical results of the CD138-positive group are shown in Table 7. When the quantification standard was set as ≥5 hotspot-positive cells/HPF, p > 0.050 indicates no statistically significant difference was detected between the hysteroscopic results and the pathologic diagnostic results (McNemar test, p-value = 0.480 > 0.050), with weak consistency (Kappa value = 0.363). Similarly, under the remaining plasma cell quantification criteria, we discerned a significant difference between the pathologic diagnosis results and the hysteroscopic diagnosis (McNemar test, p-value < 0.05), with no consistency between the two.
| Preset quantification standard | N (%) (n = 165) | McNemar test | Kappa consistency test | |||
|---|---|---|---|---|---|---|
| Both positive | Both negative | Discordant | p-value | Kappa value | p-value | |
| Standard 1 | 96 (58.2%) | 2 (1.2%) | 67 (40.6%) | 0.001 | 0.011 | 0.699 |
| Standard 2 | 87 (52.7%) | 25 (15.2%) | 53 (32.1%) | 0.001 | 0.281 | 0.001 |
| Standard 3 | 83 (50.3%) | 31 (18.8%) | 51 (30.9%) | 0.005 | 0.326 | 0.001 |
| Standard 4 | 81 (49.1%) | 35 (21.2%) | 49 (29.7%) | 0.044 | 0.362 | 0.001 |
| Standard 5 | 76 (46.1%) | 39 (23.6%) | 50 (30.3%) | 0.480 | 0.363 | 0.001 |
| Standard 6 | 42 (25.5%) | 48 (29.1%) | 75 (45.4%) | 0.001 | 0.133 | 0.058 |
| Standard 7 | 30 (18.2%) | 56 (33.9%) | 79 (47.9%) | 0.001 | 0.125 | 0.038 |
| Standard 8 | 24 (14.5%) | 59 (35.8%) | 82 (49.7%) | 0.001 | 0.130 | 0.014 |
| Standard 9 | 14 (8.5%) | 59 (35.8%) | 92 (55.7%) | 0.001 | 0.035 | 0.444 |
| Standard 10 | 11 (6.7%) | 60 (36.4%) | 94 (57.0%) | 0.001 | 0.044 | 0.260 |
Note: Both positive = Concurrent positive results of CD138 staining and hysteroscopy; Both negative = Concurrent negative results of CD138 staining and hysteroscopy; Discordant = Inconsistent results between the two methods. HPF = 40 × 10 magnification. All data were analyzed using the paired chi-square test (McNemar test) and Kappa consistency test. Data are presented as n (%).
(3) The statistical results of the CD38- and CD138-positive groups are shown in Table 8. When the quantification criteria were set to find ≥3, ≥4, or ≥5 positive cells in 1 HPF in hotspots, the hysteroscopic results and pathologic diagnosis results did not differ (McNemar test; p-values were equal to 0.704, 0.689, and 0.229, respectively), and there was weak consistency (Kappa values were 0.147, 0.256, and 0.292, respectively) relative to the ≥5 positive cells in 1 HPF. However, the pathologic diagnostic results under the other quantification criteria were significantly different from the hysteroscopic diagnosis (McNemar test, p < 0.05), with no consistency between the two.
| Preset quantification standard | N (%) (n = 165) | McNemar test | Kappa consistency test | |||
|---|---|---|---|---|---|---|
| Both positive | Both negative | Discordant | p-value | Kappa value | p-value | |
| Standard 1 | 86 (52.1%) | 1 (0.6%) | 78 (47.3%) | 0.000 | 0.144 | 0.007 |
| Standard 2 | 85 (51.5%) | 14 (8.5%) | 66 (40.0%) | 0.019 | 0.036 | 0.633 |
| Standard 3 | 80 (48.5%) | 23 (13.9%) | 62 (37.6%) | 0.704 | 0.147 | 0.058 |
| Standard 4 | 79 (47.9%) | 30 (18.2%) | 56 (33.9%) | 0.689 | 0.256 | 0.001 |
| Standard 5 | 72 (43.6%) | 37 (22.4%) | 56 (33.9%) | 0.229 | 0.292 | 0.001 |
| Standard 6 | 34 (20.6%) | 43 (26.1%) | 88 (53.3%) | 0.001 | 0.094 | 0.082 |
| Standard 7 | 22 (13.3%) | 50 (30.3%) | 93 (56.4%) | 0.001 | 0.079 | 0.074 |
| Standard 8 | 19 (11.5%) | 53 (32.1%) | 93 (56.4%) | 0.001 | 0.095 | 0.039 |
| Standard 9 | 14 (8.5%) | 55 (33.3%) | 96 (58.2%) | 0.001 | 0.081 | 0.035 |
| Standard 10 | 11 (6.7%) | 56 (33.9%) | 98 (59.4%) | 0.001 | 0.083 | 0.010 |
Note: Both positive = Concurrent positive results of combined CD38/CD138 staining and hysteroscopy; Both negative = Concurrent negative results of combined CD38/CD138 staining and hysteroscopy; Discordant = Inconsistent results between the two methods. HPF = 40 × 10 magnification. All data were analyzed using the paired chi-square test (McNemar test) and Kappa consistency test. Data are presented as n (%).
(4) The analysis results of the CD38- or CD138-positive group are shown in Table 9. Only when the quantification standard was set at ≥5 hotspot-positive cells/HP, p > 0.050 indicates no statistically significant difference was detected between hysteroscopic and pathologic diagnostic results (McNemar test, p-value = 0.085; Kappa value = 0.365). However, the pathologic diagnostic results under the remaining quantification criteria were not consistent with the hysteroscopic diagnosis.
| Preset quantification standard | N (%) (n = 165) | McNemar test | Kappa consistency test | |||
|---|---|---|---|---|---|---|
| Both positive | Both negative | Discordant | p-value | Kappa value | p-value | |
| Standard 1 | 98 (59.4%) | 1 (0.6%) | 66 (40.0%) | 0.001 | 0.018 | 0.225 |
| Standard 2 | 90 (54.5%) | 14 (8.5%) | 61 (37.0%) | 0.001 | 0.142 | 0.018 |
| Standard 3 | 85 (51.5%) | 23 (13.9%) | 57 (34.5%) | 0.001 | 0.227 | 0.001 |
| Standard 4 | 82 (49.7%) | 30 (18.2%) | 53 (32.1%) | 0.005 | 0.299 | 0.001 |
| Standard 5 | 80 (48.5%) | 36 (21.8%) | 49 (29.7%) | 0.085 | 0.365 | 0.001 |
| Standard 6 | 46 (27.9%) | 44 (26.7%) | 75 (45.4%) | 0.001 | 0.118 | 0.107 |
| Standard 7 | 38 (23.0%) | 50 (30.3%) | 77 (46.7%) | 0.001 | 0.122 | 0.073 |
| Standard 8 | 30 (18.2%) | 53 (32.1%) | 82 (49.7%) | 0.001 | 0.080 | 0.208 |
| Standard 9 | 24 (14.5%) | 55 (33.3%) | 86 (52.1%) | 0.001 | 0.050 | 0.394 |
| Standard 10 | 21 (12.7%) | 56 (33.9%) | 88 (53.3%) | 0.001 | 0.035 | 0.527 |
Note: Both positive = Concurrent positive results of CD38/CD138 “or” staining and hysteroscopy; Both negative = Concurrent negative results of CD38/CD138 “or” staining and hysteroscopy; Discordant = Inconsistent results between the two methods. HPF = 40 × 10 magnification. All data were analyzed using the paired chi-square test (McNemar test) and Kappa consistency test. Data are presented as n (%).
(5) When the number of CD38- and CD138-positive cells was averaged, the results were consistent with the hysteroscopic results (the specific results are shown in Table 10). When the quantification criterion was set at ≥5 HPF/positive cells in the hotspot area, p > 0.050 indicates no statistically significant difference was detected between hysteroscopic results and pathologic diagnostic results (McNemar test, p-values of 0.233, 95% CI for discordant rate: 20.1%–34.5%). When the quantification standard was set at 5 hotspot-positive cells/HPF, the consistency increased to moderate agreement (Kappa value of 0.422 > 0.400, 95% confidence interval [95% CI]: 0.298–0.546), which was still superior to the standard of 4 hotspot-positive cells/HPF (Kappa = 0.299 < 0.400, 95% CI: 0.176–0.422, p < 0.001).
| Preset quantification standard | N (%) (n = 165) | McNemar test | Kappa consistency test | |||
|---|---|---|---|---|---|---|
| Both positive | Both negative | Discordant | p-value | Kappa value | p-value | |
| Standard 1 | 98 (59.4%) | 1 (0.6%) | 66 (40.0%) | 0.000 | 0.018 | 0.225 |
| Standard 2 | 90 (54.5%) | 15 (9.1%) | 60 (36.4%) | 0.000 | 0.159 | 0.010 |
| Standard 3 | 83 (50.3%) | 27 (16.4%) | 55 (33.3%) | 0.001 | 0.266 | 0.001 |
| Standard 4 | 81 (49.1%) | 31 (18.8%) | 53 (32.1%) | 0.053 | 0.299 | 0.001 |
| Standard 5 | 80 (48.5%) | 40 (24.2%) | 45 (27.3%) | 0.233 | 0.422 | 0.001 |
| Standard 6 | 49 (29.7%) | 44 (26.7%) | 72 (43.6%) | 0.030 | 0.148 | 0.046 |
| Standard 7 | 36 (21.8%) | 53 (32.1%) | 76 (46.1%) | 0.001 | 0.142 | 0.030 |
| Standard 8 | 25 (15.2%) | 54 (32.7%) | 86 (52.1%) | 0.001 | 0.053 | 0.360 |
| Standard 9 | 19 (11.5%) | 57 (34.5%) | 89 (53.9%) | 0.001 | 0.038 | 0.460 |
| Standard 10 | 15 (9.1%) | 59 (35.8%) | 91 (55.2%) | 0.001 | 0.029 | 0.540 |
Note: Both positive = Concurrent positive results of CD38/CD138 mean staining and hysteroscopy; Both negative = Concurrent negative results of CD38/CD138 mean staining and hysteroscopy; Discordant = Inconsistent results between the two methods. HPF = 40 × 10 magnification. All data were analyzed using the paired chi-square test (McNemar test) and Kappa consistency test. Data are presented as n (%).
We analyzed the results of 90 patients who possessed CD38- and CD138-positive cells in 1 HPF in the hotspot area, and we counted them again, averaged them, compared them with the initial diagnostic data, and assessed the number of positive cells before and after treatment (the specific results are shown in Fig. 6). A total of 77 patients showed a diminution in the number of positive cells after the corresponding treatment, with a median difference before vs. after treatment of 5 (M: 1–7). We additionally demonstrated that the number of CD38- and CD138-positive cells before vs. after treatment was statistically significant (p < 0.001) and that the number of CD38- and CD138-positive cells decreased significantly after anti-inflammatory treatment.
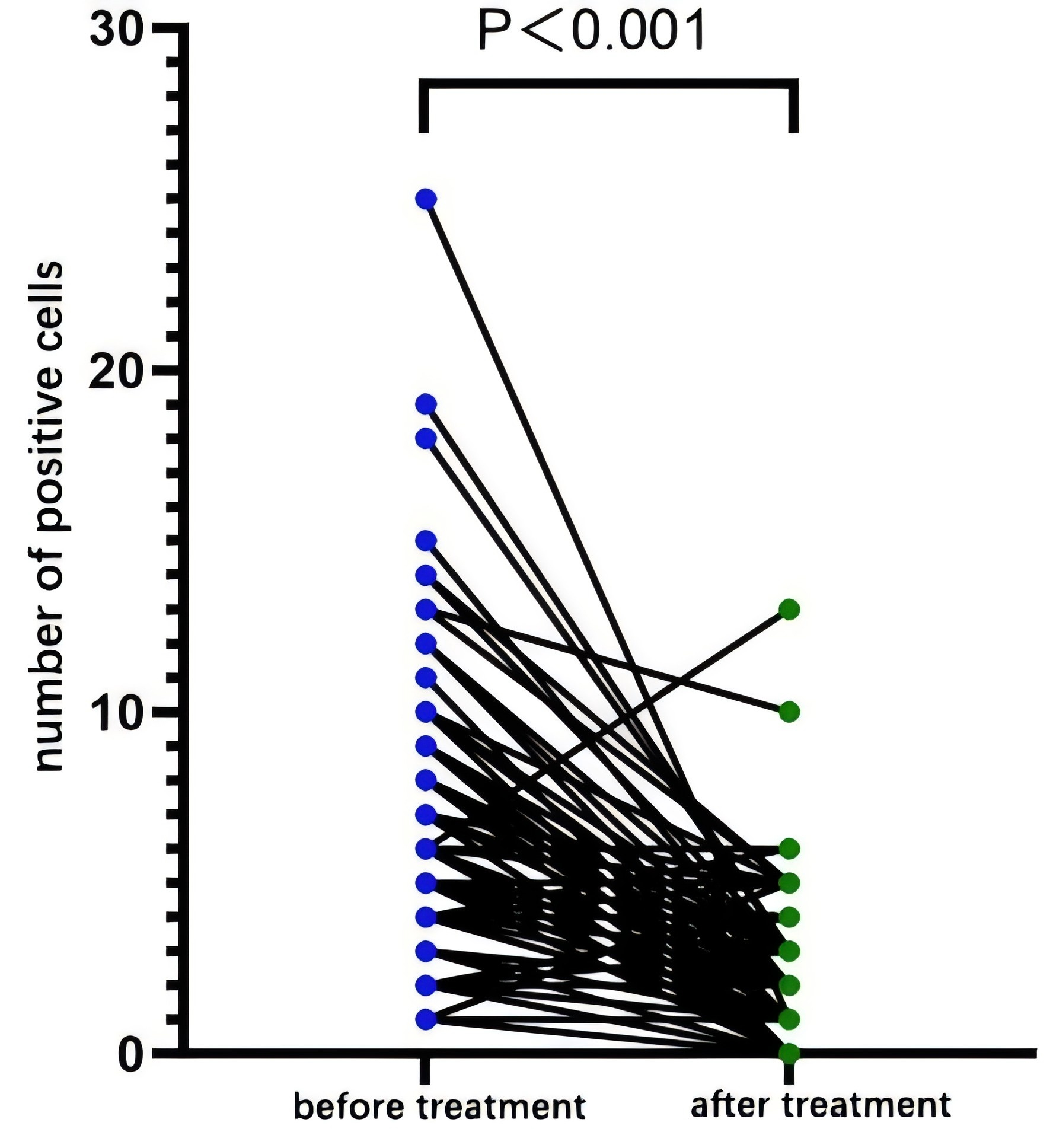 Fig. 6.
Fig. 6.Comparison of endometrial stromal plasma cells before and after treatment. Note: Data were analyzed using the Wilcoxon signed-rank test..
Entering the above 10 preset quantitative criteria into the data of 90 cases for review, we found that when the quantitative criteria were ≥4 as an average for CD38- and CD138-positive cells/HPF, 60 (78.9%) patients changed from positive before treatment to negative after treatment, and the negative rate was significantly higher than that for the other quantitative criteria (Table 11).
| Preset quantification criteria | Number of positive cases before treatment | Number of positive cases after treatment | Number of cases turning to negative after treatment |
|---|---|---|---|
| Standard 1 | 90 | 65 | 25 (27.8%) |
| Standard 2 | 86 | 48 | 38 (44.2%) |
| Standard 3 | 80 | 30 | 50 (62.5%) |
| Standard 4 | 76 | 16 | 60 (78.9%) |
| Standard 5 | 69 | 19 | 50 (72.5%) |
| Standard 6 | 53 | 14 | 39 (73.6%) |
| Standard 7 | 40 | 11 | 29 (72.5%) |
| Standard 8 | 30 | 9 | 21 (70.0%) |
| Standard 9 | 22 | 7 | 15 (68.2%) |
| Standard 10 | 16 | 5 | 11 (68.8%) |
Note: Negative cases are presented as percentages; n = number of positive cases before treatment.
To compare the diagnostic efficiency of ten quantified criteria for the negative conversion rate after standard treatment, a comparison test among groups was conducted. We found no significant differences in criteria 4 through 7 (p > 0.05), but we did in criteria 1 through 3 (p < 0.05). This suggests that when the average value for CD38- and CD138-positive cells ≥4/HPF was used as the diagnostic criterion for CE, the anti-inflammatory treatment rate in terms of the pathologic diagnosis turning negative was the highest. When CE patients were reviewed with this quantitative standard, the maximal number of patients responded to anti-inflammatory treatment, which indirectly suggests that CE may exist when there are ≥4 ESPCs/HPF in hotspots.
The infiltration of ESPCs is the basic consensus diagnostic standard for CE pathology, and the IHC staining can assist in improving the sensitivity in identifying plasma cells and augmenting the efficiency and accuracy of diagnosis. In addition to marking plasma cells, CD38 shows positive expression on pre-B cells, immature B cells, and normal epithelial cells; as does CD138, in addition to marking plasma cells, secretory endometrial glands, metaplastic squamous epithelium, and trophoblast cells. Furthermore, the combination of CD38 and CD138 can be used to better judge the infiltration of ESPCs. Our experimental results also revealed that when the combined adoption of CD38/CD138 and the mean value of positivity for both cell types were employed to interpret results, the concordance between pathologic diagnosis and hysteroscopic diagnosis was at its highest (Kappa = 0.422, p < 0.05). We thus hypothesize that using CD38 and CD138 markers and applying the average value of the two cell types for CE diagnosis produces results superior to the other four scenarios [18].
We acknowledge that most existing studies supporting the diagnostic value of CD38/CD138 or the efficacy of anti-inflammatory therapy for CE are uncontrolled, non-randomized, and underpowered, which may lead to inconsistent conclusions and limit the generalizability of their findings. This is indeed a critical limitation in the current literature that needs to be emphasized. Notably, high-quality randomized controlled trials (RCTs) remain limited, with only clinical trial protocols published to date [30]. Such trials may enroll mixed populations, and inclusion of both fertile and infertile women without stratification may mask the specific impact of CE on infertile populations, which is the focus of our study. Unlike the present study, which exclusively enrolled infertile women (excluding those with non-infertility-related CE), such mixed cohorts may have diluted the therapeutic effect of anti-inflammatory therapy in the subgroup of infertile patients with CE-related implantation failure. Given that CE-related endometrial dysfunction has distinct clinical consequences in infertile patients (e.g., implantation failure) compared to fertile populations, this inherent population heterogeneity highlights the need for population-specific diagnostic criteria tailored to infertility management. Our study addresses critical gaps in existing CE diagnostic criteria by standardizing key methodological variables that have confounded prior threshold studies. Unlike single-marker staining approaches [21], our optimized dual-marker (CD38/CD138) protocol reduces non-specific background staining, improving the accuracy of plasma cell identification. By restricting specimens to the proliferative phase, we eliminate hormonal variability [10]—a factor that has contributed to threshold discrepancies in previous studies. Our focus on infertile women ensures that our thresholds are tailored to the population most likely to benefit from CE diagnosis and treatment, avoiding the dilution of effects that may occur in mixed fertile/infertile cohorts.
Notably, the constitutional stromal CD138 expression in the proliferative phase—highlighted by the reviewer as a “dirty secret” in the field—was systematically evaluated and excluded in our study. This physiological expression, characterized by diffuse weak staining without clear plasma cell morphology, could lead to false-positive diagnoses if not properly distinguished. Our optimized IHC protocol (shortened antigen retrieval and primary antibody incubation) and dual-marker (CD138+/CD38+) verification effectively minimized this interference, as evidenced by the low median count of 1 CD138+/CD38+ cell/HPF in hysteroscopically CE-negative cases. Regarding the potential pathological significance of persistent constitutional CD138 expression proposed by the reviewer, our data showed no correlation between this background staining and clinical outcomes (e.g., infertility type or hysteroscopic findings). However, we acknowledge this as a valuable direction for future research—particularly exploring whether enhanced or persistent physiological CD138 expression predisposes individuals to CE development or impaired endometrial receptivity.
The hierarchical threshold system proposed in our study (≥5 cells/HPF for diagnosis, ≥4 cells/HPF for treatment monitoring) fills a practical gap in clinical practice. Clinicians require distinct criteria for initial diagnosis (prioritizing specificity to avoid unnecessary antibiotic use) and treatment monitoring (prioritizing sensitivity to ensure response assessment). Our findings address this need by demonstrating that the ≥5 cells/HPF threshold maximizes consistency with hysteroscopy (a reliable clinical reference), while the ≥4 cells/HPF threshold maximizes treatment response detection—providing an actionable framework for routine clinical use. These methodological standardizations and targeted designs enable our findings to complement existing literature, which has reported inconsistent thresholds due to unstandardized variables. A large number of studies have recently focused on the quantification of the minimal number of ESPCs needed as the diagnostic standard of CE pathology, and these have generated numerous new advances. In a prospective study, Hirata et al. [20] posited that CE should be diagnosed with the criterion of ≥1 plasma cells/10 HPF in the endometrial stroma. In another prospective cohort study, Rimmer et al. [21] ascertained a quantitative value of 4–6 CD138-positive cells/HPF in women with a history of recurrent abortion or repeated implantation failure for more than 12 months. Notably, a nationwide survey in Japan [22] highlighted inconsistent diagnostic criteria, including cutoffs of 3–5 cells/20 high-power fields for chronic endometritis. This threshold is lower than our primary cutoff (≥5 cells/HPF), which may be due to their inclusion of both primary and secondary infertility patients without strict restriction on menstrual cycle phase—whereas we only included proliferative phase specimens to reduce hormonal variability. A meta-analysis by Riemma et al. [23] further synthesized evidence from multiple studies, supporting the diagnostic value of hysteroscopy for chronic endometritis, with high pooled sensitivity and specificity demonstrated across eligible studies, confirming hysteroscopy as a reliable primary diagnostic tool. Additionally, Riemma et al. [23] noted that diagnostic performance can be optimized when hysteroscopic findings are combined with histopathological and immunohistochemical evaluation, which is consistent with our finding that dual-marker averaging yields the highest consistency with hysteroscopy (Kappa = 0.422). In a large-scale retrospective study in China, Li et al. [29] reported that the β-hCG-positivity rate, clinical pregnancy rate, and live-birth rate were significantly reduced in subjects with ≥5 CD138-positive cells/HPF (p = 0.04, p = 0.01, and p = 0.04, respectively), thus establishing a standard of ≥5 plasma cells in at least one HPF among 30 HPFs. Furthermore, some scholars have adopted plasma cell counts per unit area, a method with the lowest observer variability [28], providing an alternative quantification strategy for CE diagnosis.
The conclusions of the above studies varied greatly, and this may have been related to the differences in multiple factors such as race, age, and pregnancy history among the study subjects. Researchers also directly related the establishment of CE histopathologic diagnostic criteria with pregnancy outcomes of the subjects, and this index was used to determine the suitability of the diagnostic criteria. However, adverse pregnancy outcomes in CE patients are affected by multiple factors beyond the condition itself, including maternal age and genetic factors .
We now wish to clarify the utilization of the pathologic method for CE diagnosis from other perspectives. We first investigated the difference and consistency between pathologic diagnosis and hysteroscopic diagnosis by quantifying the number of CD38- and CD138-positive cells. Additionally, we ascertained that when the pathologic diagnostic criteria were set to ≥5 average positive cells for CD38 and CD138/HPF, the difference was small but acceptable, and the consistency was relatively high (Kappa = 0.422 < 0.75, p = 0.00). This may have been due to sensitivity and specificity bias, as hysteroscopy focuses on the overall apparent appearance of the endometrium, while histopathologic examination focuses on the microscopic changes in the endometrial tissue. In the early stages of CE, it may be difficult to detect an obvious and typical false-negative diagnosis, and histopathology alone is inadequate for diagnosing CE; thus, clinicians may rely on hysteroscopy for CE diagnosis. Second, when we compared the number of CD38- and CD138-positive cells before and after anti-inflammatory treatment, we found that the average number of positive cells was ≥4/HPF and that the difference in the number of positive cells before and after treatment was statistically significant. The evaluation of the endometrial microenvironment in CE patients previously depended upon hysteroscopic observation by clinicians and the assessment of endometrial tissue sections by pathologists. The establishment of negative criteria is now of great significance for physicians in determining the endometrial microenvironment of CE patients and thereby further allows the judgment of therapeutic efficacy in patients. We have not uncovered any reports in the literature and do not know of any extant investigations that involve the establishment of CE in patients using positive vs. negative criteria. Our proposed CD38/CD138 quantitative thresholds provide a reliable pathological reference for CE diagnosis, and clinical evidence has confirmed that hysteroscopy combined with CE screening significantly improves pregnancy outcomes in patients with previous failed embryo transfer [31], underscoring the clinical rationality of their combination and the practical value of standardized diagnostic criteria.
Considering the aforementioned two aspects, the dual cutoffs of average CD38- and CD138-positive cells (≥4/HPF or ≥5/HPF) both showed favorable performance in clinical practice: the ≥5/HPF cutoff optimized the consistency with clinical hysteroscopy (Kappa = 0.422), while the ≥4/HPF cutoff maximized the negative conversion rate after treatment (78.9%). Additionally, a consistent reduction in the number of positive cells was observed before and after treatment in both cutoff groups. Although both cutoffs exhibited clinical relevance, simply suggesting the two without prioritization may lead to ambiguity and confusion for readers. Notably, the 78.9% negative-conversion rate under the ≥4/HPF threshold is unlikely to be attributed to spontaneous resolution of CE, Yasuo and Kitaya [32] demonstrated that natural remission of chronic endometritis rarely occurs without targeted antibiotic therapy, and the spontaneous resolution rate was reported to be as low as 12.7% in untreated patients—far lower than the treatment-induced negative-conversion rate in our study. This comparison confirms that the significant reduction in CD38- and CD138-positive cells observed post-treatment is a specific effect of anti-inflammatory therapy rather than the natural outcome of uterine microbiota self-regulation or immune clearance of mild infections. Thus, the ≥4/HPF cutoff not only demonstrates superior sensitivity for monitoring treatment response but also reflects the clinical benefit of targeted therapy, further validating its utility as a secondary reference threshold.
Given that diagnostic accuracy and consistency with the clinically recognized reference method of hysteroscopy (a valuable adjunct to histopathology) are core requirements for pathologic reference criteria, we propose ≥5/HPF as the primary cutoff value for the pathologic diagnosis of CE for conservative and reliable diagnosis. This primary cutoff is supported by its superior agreement with hysteroscopy (Kappa = 0.422), which serves as a well-recognized clinical diagnostic reference. Meanwhile, the ≥4/HPF cutoff can be used as a secondary indicator for clinical scenarios emphasizing treatment response monitoring, considering its advantage in predicting negative conversion (78.9%).
The prioritization of ≥5/HPF aligns with its proven clinical relevance in guiding fertility management. Bulut et al. [33] demonstrated that a cutoff of ≥5 CD138+ plasma cells significantly impacts the reproductive outcomes of frozen embryo transfer, confirming that this stricter threshold can effectively identify clinically meaningful CE cases. Santoro et al. [34] further emphasized plasma cells as core markers for CE diagnosis and highlighted that standardized cutoff selection improves diagnostic consistency, which our primary cutoff of ≥5/HPF facilitates.
For the supplementary use of ≥4/HPF, it remains valuable in specific high-risk scenarios. Hue et al. [35] reported a substantial CE prevalence among infertile patients (including those with recurrent implantation failure, RIF) and emphasized the need to consider confounders in CD138-based diagnosis, supporting the need for cautious diagnostic interpretation in this vulnerable group. Similarly, Guo et al. [4] linked CE to metabolic abnormalities in infertile women with non-uniform endometrial echogenicity, supporting that early CE diagnosis and intervention could help optimize reproductive prognosis.
Hysteroscopy serves as a key reference for CE diagnosis, but its standalone utility has been debated. Gkrozou et al. [14] concluded in a systematic review that hysteroscopy alone is insufficient for definitive CE diagnosis, supporting our approach of integrating CD38/CD138 cutoffs with hysteroscopic findings. Dang et al. [36] further demonstrated a weak but significant correlation only between endometrial micropolyps and CD138 positivity, while overall hysteroscopic findings showed poor agreement with histology, which justifies our use of hysteroscopy agreement (Kappa = 0.422) as a validation metric for the ≥5/HPF cutoff. This combined diagnostic paradigm aligns with contemporary clinical practices and strengthens the robustness of our cutoff recommendations.
Our study has several limitations that should be acknowledged. First, as a single-center retrospective cohort study, potential selection bias exists, and our findings may not be generalizable to diverse populations (e.g., different ethnicities, healthcare settings beyond reproductive medicine centers, or patients with comorbidities like polycystic ovary syndrome). Second, the lack of a placebo control group prevents us from fully excluding the impact of spontaneous fluctuations in endometrial plasma cell counts (low spontaneous resolution) [32] on post-treatment changes, though the high negative-conversion rate (78.9%) far exceeds the reported spontaneous resolution rate (12.7%) [32], supporting that the reduction in plasma cells is primarily treatment-induced. Third, our sample size (n = 165 for diagnostic exploration, n = 90 for therapeutic validation) is relatively modest, which may limit the precision of threshold estimates, especially for subgroup analyses (e.g., primary vs. secondary infertility). Fourth, we did not collect prospective reproductive outcome data for all patients, and the clinical relevance of our thresholds is supported by alignment with outcome-validated criteria from independent studies [22,23,29] rather than direct in-study outcomes. Fifth, the tissue volumes of endometrial specimens varied, which may have introduced bias into cell counting results.
Future multicenter prospective studies are warranted to validate our hierarchical threshold system in more diverse populations and directly link it to reproductive outcomes. Additionally, research incorporating a placebo control group or serial biopsies across multiple cycles (without treatment) would help clarify the independent effects of cycle-to-cycle variability and anti-inflammatory therapy, further enhancing the robustness of conclusions regarding treatment efficacy in CE management. Standardization of IHC staining protocols (e.g., antigen retrieval time, antibody concentration) across institutions is also needed to reduce inter-laboratory variability and promote the widespread adoption of CD38/CD138-based CE diagnosis.
This study indicates that using ≥5/HPF as the primary reference cutoff for average CD38- and CD138-positive cells can assist in histopathologic evaluation of CE with minimal bias and favorable accuracy (McNemar test, p = 0.233; Kappa = 0.422, p < 0.05), which may partially mitigate CE overdiagnosis in clinical practice. Meanwhile, an average of ≥4 CD38- and CD138-positive cells/HPF shows superior performance in monitoring treatment response, as it yielded the highest negative-conversion rate (78.9%) among all tested thresholds after anti-inflammatory therapy (p < 0.05), making it a suitable secondary reference cutoff.
Despite the lack of unified CE diagnostic criteria, integrating this hierarchical reference system (≥5 cells/HPF for diagnosis, ≥4 cells/HPF for treatment monitoring) with hysteroscopy and histopathology enhances the accuracy of CE auxiliary diagnosis in infertile women, providing a targeted reference basis for clinical decision-making in infertility management and treatment response evaluation.
The datasets generated and analyzed during the current study are not publicly available due to the need to protect the privacy and confidentiality of study participants, in compliance with ethical standards and relevant data protection regulations. However, de-identified data can be made available from the corresponding author upon reasonable request, subject to approval from the local institutional ethics committee to ensure no breach of participant confidentiality. Authors confirm that all relevant raw data and metadata are retained in accordance with scientific record-keeping standards and are accessible for verification by the journal editors or peer reviewers if required. For guidance on data deposition, authors have referred to the FAIRsharing and re3data.org platforms.
XC and JH designed the research. XC, XL, and SL conducted the research. QQ contributed to technical guidance, protocol optimization and result interpretation of immunohistochemical experiments. BW provided assistance and advice regarding the hysteroscopy results. XC, JH, XL, and LH carried out pathological review and the result interpretation of H&E staining and immunohistochemical staining results. XL analyzed the data. All authors contributed to the editorial revisions of the manuscript. All authors have read and approved the final version of the manuscript. All authors have actively participated in the work and agreed to be accountable for all aspects of the work, ensuring the accuracy and integrity of every part.
This study was conducted in strict accordance with the ethical principles outlined in the Declaration of Helsinki and relevant national regulations on medical research involving human subjects. The clinical procedures (including hysteroscopy, endometrial biopsy, and preservation of pathological paraffin blocks) for the enrolled patients were approved by the Ethics Committee of the First Affiliated Hospital of Shantou University Medical College in 2019 (approval number: SUMCFAH-EC-Research-2019), which explicitly authorized the use of residual clinical specimens and de-identified diagnostic data for subsequent retrospective medical research. Given that this study is a retrospective analysis of existing clinical data and pathological specimens collected between June 2020 and December 2021 (no additional interventions, no direct risks to participants, and complete anonymization of all data/specimens), the specific research protocol was reviewed by the same Ethics Committee in 2025 and granted a Statement on Exemption from Ethical Review. This exemption is supplementary to the 2019 initial approval, confirming that no additional ethical review is required for the retrospective analysis of pre-authorized materials. All patients provided written informed consent for clinical examinations and specimen collection during their initial medical visits (as approved by the 2019 ethical review), and the consent form explicitly covered the use of residual specimens and data for research purposes. No additional consent was needed for this retrospective study, in line with the terms of the 2025 ethical exemption. Data management and specimen storage strictly adhered to medical confidentiality regulations and institutional policies. The Ethics Committee conducted regular oversight, and no ethical violations or privacy breaches were reported throughout the study period.
We thank LetPub for its linguistic assistance during the preparation of this manuscript. We also appreciate the technical support from the Pathology Department of the First Affiliated Hospital of Shantou University Medical College.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.