



1 Maternal-Infantile Department, Gubbio and Gualdo Tadino Hospital, ASL 1 Umbria, 06127 Perugia, Italy
According to the US Food and Drug Administration (2014), the rates of unsuspected sarcomas found during or after gynecological surgeries intended to treat presumed benign fibroids are 1/352 for uterine sarcoma and 1/498 for leiomyosarcoma [1, 2]. This disclosure highlights the need to avoid uterus and leiomyoma morcellation and has provoked a careful review of clinical records at many centers to determine the prevalence of the unintended morcellation of uterine malignancies and establish its impact on malignancy outcomes. A meta-analysis of the risk of unintended malignancy in surgeries for benign gynecological conditions was first reported in 2015 [1], revealing malignancy rates of ~1/8300 (only prospective studies assessed) and 1/2000 (both prospective and retrospective studies assessed). This result contradicts the previously reported risk of malignancy (1/352) and supports uterus and leiomyoma morcellation performed in many gynecological surgeries, especially laparoscopic ones. Similar results have been reported in other systematic reviews [3, 4]; however, the need for morcellation remains debatable. On the one hand, the morcellation of a benign tumor is not advisable because of the risk of disseminating an occult malignancy with unclear outcomes [4, 5]. Adverse outcomes appear to be particularly higher for the morcellation of leiomyosarcomas [6], which are one of the several types of occult uterine malignancies. On the other hand, minimally invasive surgery has many advantages, and patients may accept the very low risk of the unintended morcellation of an occult uterine disease during the presurgical counseling phase. However, this is not the case in Italy, where any presurgical agreement can be questioned in the case of a complication [7] to justify legal claims. Therefore, for legal purposes, a presurgical diagnosis of the benign or malignant nature of any fibroid-resembling uterine mass is required in Italy.
The presurgical assessment of uterine fibroids is commonly performed through sonography. Evidence-based guidelines encourage diagnostic process deepening through the combined consideration of lactate dehydrogenase (LDH) levels (and LDH isoenzyme levels wherever possible) and sonographic scores [8, 9, 10, 11]. Several methods for improving the performance of ultrasonographic techniques are currently under assessment [12, 13]. However, Huang et al. [14] demonstrated that the sonographic diagnosis of uterine sarcomas can be made more accurate by considering clinical and laboratory findings, an approach easily implementable in real-world settings.
According to a recent meta-analysis [11], sonographic sarcoma detection is only
moderately accurate, as follows from its positive likelihood ratio of 6.65 and
sensitivity of 0.76. These estimates originate from experimental studies, and
real-world performance is therefore expected to be lower. The actual ability of
diagnostic tools—ultrasonography [8, 9, 10, 11, 12, 13], magnetic resonance imaging (MRI) [15],
clinical and laboratory tests [14], endometrial sampling [16, 17], and positron
emission tomography (PET) [18, 19]—to detect leiomyosarcomas can be determined
only if the prevalence of undiagnosed leiomyosarcomas is known in a real-world
context. This prevalence can be obtained from the rate of occult leiomyosarcomas
reported in clinical series of hysterectomies. To the older relevant studies
listed in the Cui and Wright review [2] were added more old and recent clinical
series [20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55] found during the literature research drawn for writing this paper.
All these series were pooled for being able to estimate the rate of undiagnosed
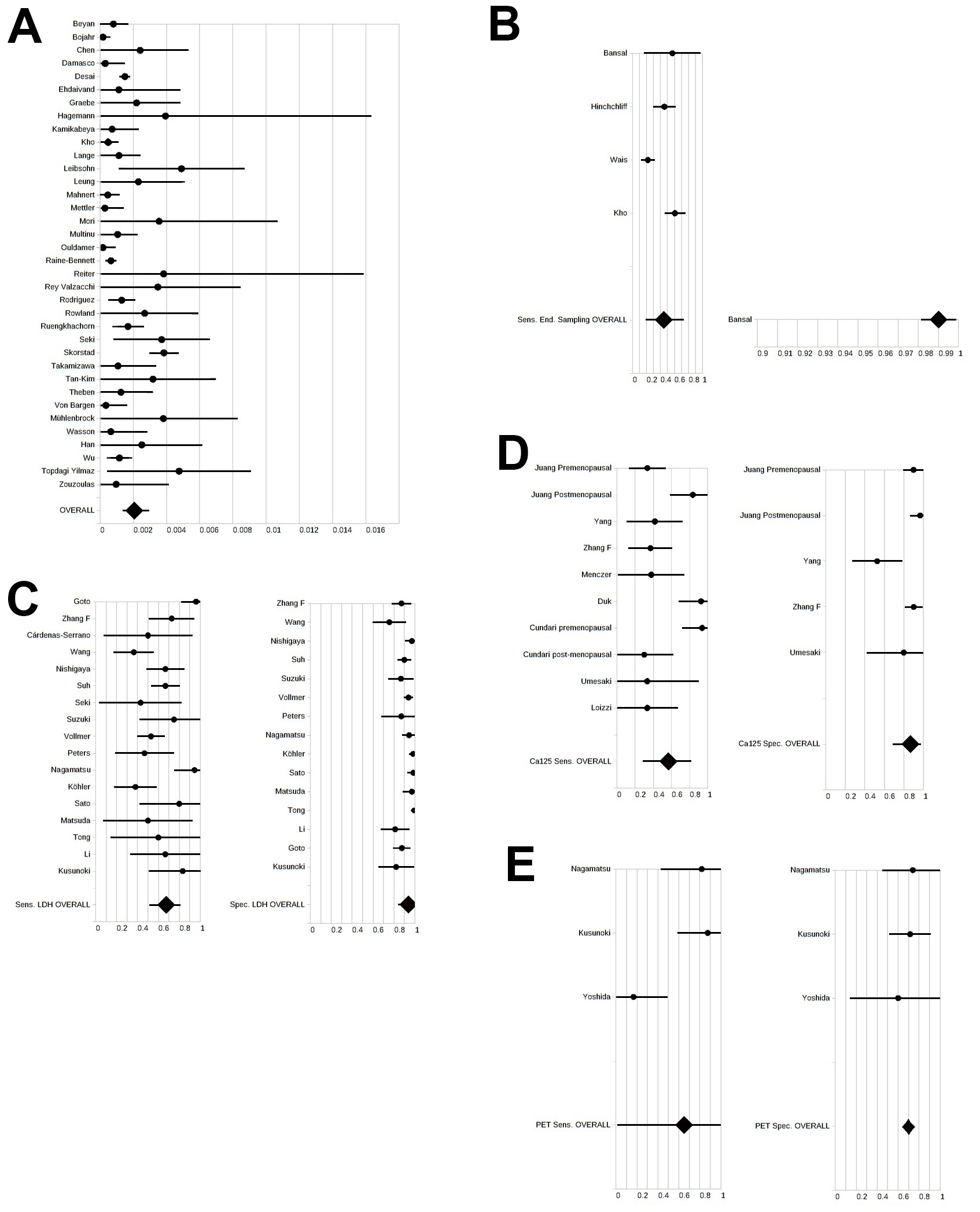
leiomyosarcomas in hysterectomized patients (0.00206344, Fig. 1A). For instance, based on the rates of
hysterectomy (reported as 1.6/1000 (0.0016) in 2024 [56]) and leiomyosarcoma
(0.0000064 [57]) in Italy, the rate of undiagnosed leiomyosarcomas can be
estimated using Bayes’ theorem as 0.00206344
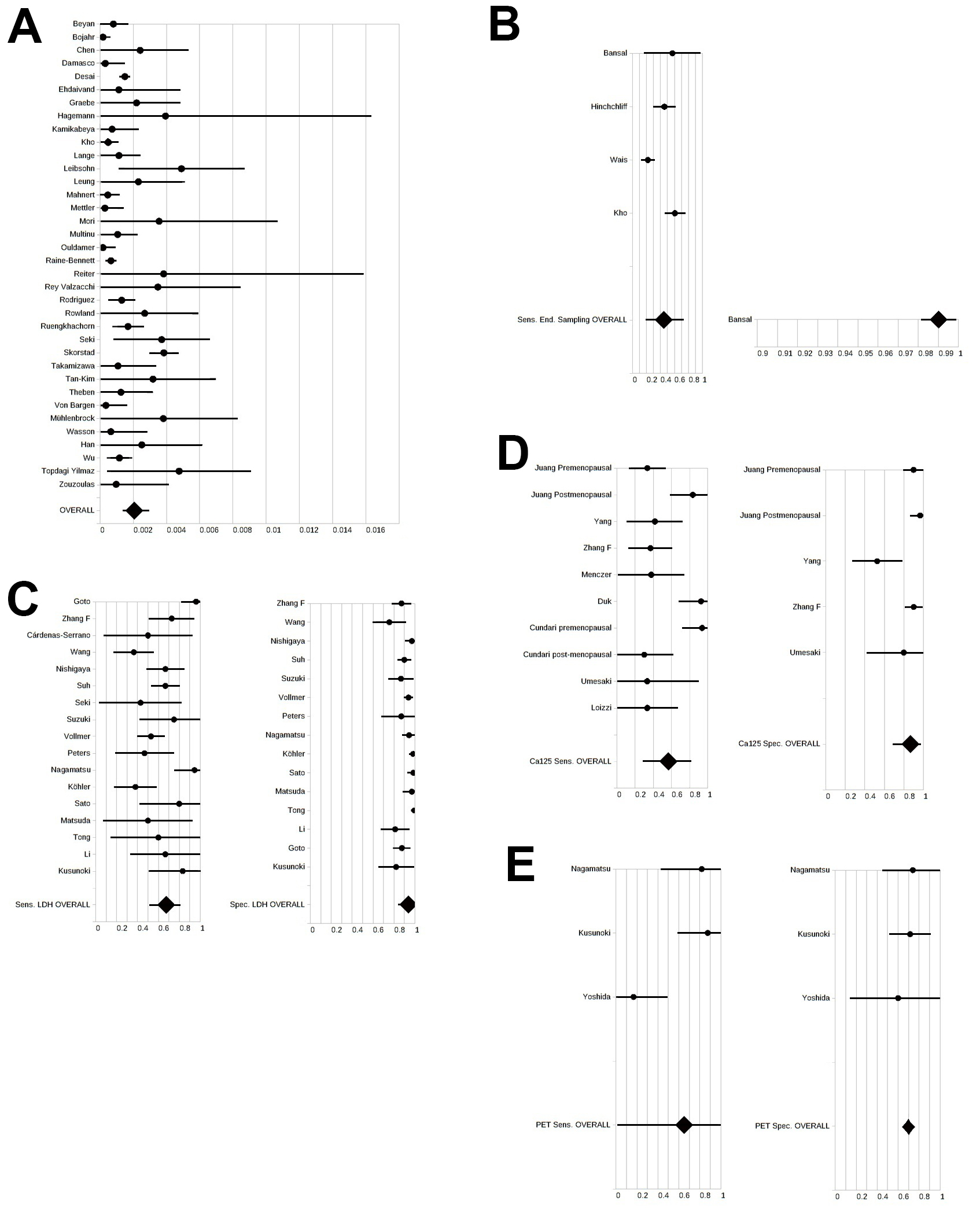 Fig. 1.
Fig. 1.
Forest plots. In all cases, the series search was not systematic, and no quality assessment was performed. (A) Forest plot for the overall rate of occult leiomyosarcoma in reported hysterectomy series. Random-effects model, I2 = 99.9%. (B) Forest plot for the overall endometrial sampling sensitivity. Random-effects model, I2 = 93.0%, forest plot on the left. The endometrial sampling specificity (forest plot on the right) is only available from Bansal et al. [16]. (C) Forest plot for the overall LDH sensitivity (random-effects model, I2 = 92.9%, forest plot on the left) and specificity (random-effects model, I2 = 99.5%, forest plot on the right). (D) Forest plot for the overall Ca125 sensitivity (random-effects model, I2 = 94.5%, forest plot on the left) and specificity (random-effects model, I2 = 95.0%, forest plot on the right). (E) Forest plot for the overall PET sensitivity (random-effects model, I2 = 96.0%, forest plot on the left) and specificity (fixed model, I2 = 0.0%, forest plot on the right). Ca125, cancer antigen 125; End. Sampling, endometrial sampling; LDH, lactate dehydrogenase; PET, positron emission tomography; Sens., sensitivity; Spec., specificity.
Most of these diagnoses would be made using a first-line sonographic check. In fact, it is unreliable to assume that all supposed leiomyomas detected by a simple sonographic check (without following the recently established scoring-point guidelines for detecting the rarest uterine sarcomas [8]) underwent MRI before surgery, with presurgery PET being even less likely. Based on the key concept of Huang et al. [14], however, additional clinical and laboratory tests, along with endometrial sampling [58], might be performed more commonly for presumed leiomyomas and might be included in decision-making algorithms to optimize surgery type and morcellation choice.
Table 1 (Ref. [11, 15, 16, 17, 19, 44, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77]) (box 1) reports the probabilities of positive uterine leiomyosarcoma detection for different diagnostic tools (Italy, 2024). These probabilities were calculated from positive likelihood ratios as reported elsewhere [11, 15]. Otherwise, sensitivity and specificity data extracted from the literature were pooled to obtain overall sensitivities and specificities, which were standardized and used to calculate the overall likelihood ratio for each positive finding.
| Box 1 | ||||
| Diagnostic test | Probability of positive test | Probability of single positive test | Probability of the positive test being associated with other positive tests | |
| Ultrasonography* | Diagnosed | 0.517140 | 0.001522 | 0.516353 |
| Undiagnosed | 0.525795 | 0.001387 | 0.525066 | |
| MRI** | Diagnosed | 0.556258 | 0.002565 | 0.554831 |
| Undiagnosed | 0.561134 | 0.002213 | 0.559892 | |
| LDH*** | Diagnosed | 0.484070 | 0.000958 | 0.483607 |
| Undiagnosed | 0.515790 | 0.001210 | 0.515166 | |
| End. Sampling**** | Diagnosed | 0.319401 | 0.000137 | 0.319357 |
| Undiagnosed | 0.347600 | 0.000175 | 0.347540 | |
| Ca125***** | Diagnosed | 0.298886 | 0.000039 | 0.298874 |
| Undiagnosed | 0.326142 | 0.000056 | 0.326124 | |
| PET****** | Diagnosed | 0.271750 | 0.000021 | 0.271744 |
| Undiagnosed | 0.297582 | 0.000031 | 0.297572 | |
| Box 2 | ||||
| Diagnostic test | Probability of negative test | Probability of single negative test | Probability of the negative test being associated with other negative tests | |
| Ultrasonography* | Diagnosed | 0.288192 | 0.000030 | 0.288183 |
| Undiagnosed | 0.307074 | 0.000033 | 0.307064 | |
| MRI** | Diagnosed | 0.283165 | 0.000027 | 0.283156 |
| Undiagnosed | 0.301718 | 0.000030 | 0.301709 | |
| LDH*** | Diagnosed | 0.469881 | 0.000760 | 0.469524 |
| Undiagnosed | 0.500667 | 0.000873 | 0.500229 | |
| End. Sampling**** | Diagnosed | 0.482775 | 0.000398 | 0.482583 |
| Undiagnosed | 0.514405 | 0.001056 | 0.513862 | |
| Ca125***** | Diagnosed | 0.482722 | 0.000916 | 0.482279 |
| Undiagnosed | 0.514349 | 0.001055 | 0.513806 | |
| PET****** | Diagnosed | 0.482594 | 0.000914 | 0.482153 |
| Undiagnosed | 0.514213 | 0.001053 | 0.513671 | |
| Box 3 | ||||
| Diagnostic test | Odds ratio for positive test | Odds ratio for single positive test | Odds ratio for the positive test being associated with other positive tests | |
| Ultrasonography | 1.630 | 4.255 | 1.616 | |
| MRI | 2.048 | 4.373 | 2.040 | |
| LDH | 2.719 | 1.715 | 1.000 | |
| End. Sampling | 3.793 | 1.644 | 0.995 | |
| Ca125 | 3.956 | 1.649 | 0.995 | |
| PET | 4.182 | 1.649 | 0.996 | |
Probabilities in boxes 1 and 2 were obtained by converting the likelihood ratios reported at aggregate levels or recalculated from the sensitivities and specificities pooled from nonsystematically collected articles. When possible, references from reviews were preferentially assessed. These probabilities were used to calculate odds ratios for detecting leiomyosarcoma in box 3. MRI, magnetic resonance imaging; LDH, lactate dehydrogenase; PET, positron emission tomography; End, endometrial.
*Calculated from the data of Raffone et al. [11] assuming that leiomyosarcomas account for 60% of all uterine sarcomas (according to Associazione Italiana Oncologia Medica [AIOM] guidelines [57]).
**Calculated from the data of Raffone et al. [15] assuming that leiomyosarcomas account for 60% of all uterine sarcomas (according to according to AIOM guidelines[57]).
***Pooled sensitivity and specificity: Data were extrapolated from [44, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73]. The cut-off for a normal LDH level is slightly different among studies.
****Recalculated by pooling the sensitivities and specificities from [16] and [17] and [58] and [59].
*****Studies pooled from Cundari et al. [74], Umesaki et al. [19], Zhang et al. [73], and Loizzi et al. [75].
******From the pooled data of Nagamatsu et al. [65], Kusunoki et al. [76], and Yoshida et al. [77].
The likelihood ratios for positive uterine sarcoma detection by ultrasonography and MRI were reported in the meta-analyses of Raffone et al [11, 15]. The likelihood ratios for endometrial sampling revealing positive or suspected leiomyosarcoma were obtained by pooling the sensitivities and specificities reported in previous studies[16, 17]. These studies included those reviewed by Ricci et al. [18] and those [58, 59] incidentally found during the full-text search performed for writing the present draft (Fig. 1B) [16]. The likelihood ratios for the positive detection of leiomyosarcoma at elevated LDH levels (various cut-offs) were calculated by pooling the sensitivities and specificities reported in different studies or recalculated from the data presented therein (Fig. 1C) [19, 44, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73]. The likelihood ratios for the positive detection of leiomyosarcoma at elevated cancer antigen 125 (Ca125) levels were calculated in the same way based on the works of Umesaki et al. [19], Zhang et al. [73], Cundari et al. (own work [74] and referenced studies [74, 78, 79, 80, 81]), and Loizzi et al. [75] (Fig. 1D). The likelihood ratios for the positive detection of leiomyosarcoma given a positive PET outcome (obtained using [18F]fluorodeoxyglucose and the cut-off reported by Umesaki et al. [19]) were recalculated by pooling sensitivities and specificities from the work of Nagamatsu et al. [65] (which incorporates the data of Umesaki et al. [19]), Kusunoki et al. [76], and Yoshida et al. [77]) (Fig. 1E).
The probabilities computed from the likelihood ratios for positive tests (Table 1, box 1, second column) were combined to estimate the probabilities of a single and multiple positive diagnostic findings for leiomyosarcoma in diagnosed cases of uterine leiomyosarcomas in Italy in 2024 (Table 1, box 1, third and fourth columns). As highlighted in Table 1 (box 1, third column), unique positive findings obtained using ultrasonography, MRI, PET, LDH, endometrial sampling, or Ca125 are very uncommon, unlike multiple positive findings.
Analogously, Table 1 (box 2) reports the estimated probabilities extracted from the likelihood ratios for a negative test in undiagnosed cases of leiomyosarcomas in Italy in 2024. As highlighted in box 2 (third column), an undiagnosed Italian patient with leiomyosarcoma is unlikely to have had a single negative test and minimally more likely to have had more than one negative test (fourth column). Thus, at least one positive finding is usually present. From the positive and negative values in diagnosed and undiagnosed cases of leiomyosarcomas (previously estimated as 0.48414 and 0.51586, respectively), we recalculated how much each diagnostic test can increase the odds of detecting leiomyosarcoma in affected Italian patients in 2024. The estimated odds ratios are reported in Table 1 (box 3).
The above results suggest that gynecologists should look for more than a single positive finding among diagnostic tests for leiomyosarcoma. A single positive finding increases the probability of detecting leiomyosarcoma, especially if ultrasonography and MRI are not informative (Table 1, box 3). Thus, the decision to perform morcellation during surgery can be better advised in all suspected cases.
In conclusion, especially in Italy, where leiomyosarcoma detection is a legally sensitive matter, the practice guideline–suggested algorithm [8] of requesting MRI only in the case of suspicious sonography or high LDH levels might be insufficient to drive secure morcellation. In many hospital settings worldwide, an expert assessment of MRI data, ultrasonographic patterns, and the ability to identify LDH isoenzymes (as suggested by Di Cello et al. [82] and reported in practice guidelines [8]) is not possible. Therefore, gynecologists might collect additional information to exclude leiomyosarcoma, with endometrial sampling and PET being methods of particular interest.
All work was conceived and completed by UI.
Not applicable.
Not applicable.
This research received no external funding.
The author declares no conflicts of interest. Ugo Indraccolo is serving as one of the Editorial Board members of this journal. We declare that Ugo Indraccolo had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Michael Friedrich and Michael H. Dahan.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.