



 , Petra Bukovec 1,2, Vladka Salapura 2,3, Gregor Norčič 2,4, Dominik Habes 5,6, David Lukanović 1,2, Marina Jakimovska 1,2
, Petra Bukovec 1,2, Vladka Salapura 2,3, Gregor Norčič 2,4, Dominik Habes 5,6, David Lukanović 1,2, Marina Jakimovska 1,21 Department of Gynaecology, Division of Gynaecology and Obstetrics, University Medical Centre Ljubljana, 1000 Ljubljana, Slovenia
2 Medical Faculty, University of Ljubljana, 1000 Ljubljana, Slovenia
3 Clinical Radiology Institute, University Medical Centre Ljubljana, 1000 Ljubljana, Slovenia
4 Department of Abdominal Surgery, University Medical Centre Ljubljana, 1000 Ljubljana, Slovenia
5 Department of Obstetrics and Gynecology, University Hospital Hradec Kralove, 500 05 Hradec Kralove, Czech Republic
6 Department of Obstetrics and Gynecology, Faculty of Medicine in Hradec Kralove, Charles University, 500 05 Hradec Kralove, Czech Republic
Abstract
Obstetric anal sphincter injuries (OASIS) represent a serious complication of vaginal delivery that can result in chronic anal incontinence and reduced quality of life. Accurate diagnosis is essential for optimal repair and prevention of long-term morbidity. This review summarizes current evidence on the advantages of elastography as a diagnostic adjunct for the detection of OASIS.
Elastography is an advanced ultrasound (US)-based imaging technique that quantifies tissue stiffness, enabling functional assessment of the anal sphincter complex beyond anatomical visualization. By distinguishing the mechanical properties of healthy muscle, acute tears, and fibrotic tissue, elastography may improve the detection of subtle or occult sphincter defects that conventional endoanal US may miss.
Shear-wave elastography (SWE) has demonstrated moderate to good intraobserver and interobserver reliability, with reported intraclass correlation coefficients (ICC) that vary by measurement conditions. Preliminary studies indicate that greater sphincter stiffness may be protective against perineal tears, suggesting potential for risk stratification. Elastography is non-invasive, free of ionizing radiation, and suitable for repeated evaluation during recovery. However, its diagnostic superiority over standard US for high-grade OASIS remains unconfirmed, and correlations with functional outcomes, such as incontinence severity, are inconsistent. Key limitations include operator dependency, a steep learning curve, and a lack of standardized acquisition protocols. Integration with artificial intelligence (AI) could improve consistency and diagnostic accuracy.
Elastography represents a promising adjunct to traditional imaging for the evaluation and management of OASIS. By providing quantitative, biomechanical insights into sphincter integrity, it holds potential to improve early diagnosis, guide rehabilitation, and support recovery monitoring. However, robust evidence demonstrating superiority over established imaging modalities for the diagnosis of OASIS remains limited. Larger, longitudinal studies are needed to validate the clinical utility of elastography and to standardize the use of this technique in obstetric practice.
Keywords
- obstetric anal sphincter injury
- elastography
- ultrasound imaging
- perineal trauma
- pelvic floor
Obstetric anal sphincter injuries (OASIS) are a significant and often debilitating complication of vaginal delivery that impacts a woman’s short- and long-term health and well-being [1]. These injuries encompass a spectrum of damage that ranges from partial tears to complete disruption of the external anal sphincter (EAS) and internal anal sphincter (IAS) anal sphincters, often leading to anal incontinence, perineal pain, sexual dysfunction, and reduced quality of life [2]. Standard imaging techniques for detecting these injuries, assessing repairs, and monitoring occult tears remain a clinical challenge and contribute to underdiagnosis and subsequent chronic morbidity [3]. Assessment of OASIS includes patient history, clinical examination (digital rectal examination and examination of the levator), and, when indicated, imaging to define structural defects and functional tests to evaluate sphincter performance. Endoanal ultrasound (US), including three-dimensional (3D) techniques, is widely used as the reference imaging modality for detecting sphincter defects, whereas magnetic resonance imaging (MRI) may be used in selected cases. Anal manometry provides a functional assessment and may complement imaging but is not an imaging reference standard [4]. These limitations have prompted interest in complementary imaging approaches that can provide a more comprehensive and accurate assessment of the anal sphincter complex. Elastography, a novel US-based imaging technique that includes shear-wave elastography (SWE) and strain elastography (real-time tissue elastography), has emerged as a promising tool to evaluate tissue stiffness and structural integrity. It offers enhanced capabilities for detailed characterization of the anal sphincter musculature [5]. This method uses the mechanical properties of tissue to assess its condition. The premise is that injured or fibrotic sphincter muscles may exhibit stiffness characteristics that differ from those of healthy tissue. The use of elastography in this area is relatively recent.
This manuscript was conducted as a structured narrative review. Relevant literature was identified through searches of PubMed/MEDLINE and Embase up to November 2025. The search strategy combined keywords and MeSH terms including “elastography”, “shear-wave elastography”, “strain elastography”, “OASIS”, “anal sphincter injury”, “perineal body”, “perineal trauma”, and “anal sphincter stiffness”. Reference lists of selected articles were also screened to identify additional relevant studies. Studies reporting negative or null findings were included to ensure balanced representation of the current evidence.
Recent systematic reviews and meta-analyses [6, 7, 8] have evaluated US-based modalities for the diagnosis of OASIS, including endoanal, transperineal, and endovaginal US. However, elastography has not been incorporated as a primary diagnostic modality in these analyses, and its performance has not been directly compared with that of established imaging techniques. The existing elastography literature consists primarily of prospective reliability studies and small cohort investigations, which demonstrate promising feasibility and potential value for risk stratification but have not been synthesized in an OASIS-focused review or assessed alongside current reference imaging techniques. As summarized in Table 1 (Ref. [6, 7, 8]), prior systematic reviews have focused on conventional US modalities and clinical risk factors, without including elastography as a diagnostic tool or evaluating its comparative performance.
| Author (Year) | Study type | Focus | Imaging modalities included | Elastography presence | OASIS-specific analysis | Diagnostic accuracy metrics reported |
| Packet et al., 2023 [6] | Systematic review and meta-analysis | Predictive factors for OASIS | Clinical and obstetric variables | No | Yes | No imaging comparison |
| Sideris et al., 2020 [7] | Meta-analysis | Risk of OASIS and anal incontinence | Clinical risk factors | No | Yes | No imaging comparison |
| Pang et al., 2025 [8] | Meta-analysis | Diagnostic performance for OASIS | Endoanal, transperineal, endovaginal US | No | Yes | Yes (US modalities only) |
| Present Review | Narrative critical synthesis | Elastography in OASIS | Elastography (strain and SWE) | Yes (primary focus) | Yes (exclusive focus) | Explicit identification of absence of high-grade diagnostic accuracy trials |
OASIS, obstetric anal sphincter injuries; US, ultrasound; SWE, shear-wave elastography.
This narrative review provides a focused and critical evaluation of elastography in the diagnosis of OASIS. It examines the potential contribution of biomechanical tissue assessment alongside conventional imaging and clearly distinguishes technical feasibility from validated diagnostic and prognostic applications. The review highlights the absence of prospective diagnostic accuracy studies in confirmed high-grade OASIS and outlines specific research priorities that must be addressed before elastography can be integrated into routine clinical practice. To our knowledge, this is the first review dedicated exclusively to the assessment of the role of elastography in OASIS diagnosis. The central thesis of this review is that elastography may provide clinically relevant biomechanical information by quantifying tissue stiffness, which reflects structural composition and remodeling of the anal sphincter complex. However, its diagnostic and prognostic value depends on the establishment of reproducible associations among stiffness patterns, confirmed structural injury, and functional outcomes.
OASIS is recognized as a major cause of maternal morbidity and often results in symptoms such as fecal and flatus incontinence, as well as persistent perineal pain [9]. Vaginal birth is a significant contributing factor to pelvic floor dysfunction, affecting approximately 10% of women who give birth every year. Most women undergoing surgery for related conditions, such as genital organ prolapse and urinary or fecal incontinence, are also affected by this issue [10]. The findings highlight a strong correlation between perineal trauma and adverse postpartum outcomes, including an increased risk of postpartum depression and anxiety, as well as a diminished quality of life due to chronic pain [11]. It is crucial to understand the anatomical and physiological changes in the anal sphincter complex that occur with age, particularly in the context of childbirth, to ensure accurate diagnosis and management of these disorders [12]. The integrity of the anal sphincter is fundamental to continence, and damage incurred during childbirth can compromise its muscular and neurological components, leading to long-term functional impairment [13]. Physiological changes that affect sphincter muscle and sensory functions, as well as potential damage to the endopelvic fascia, contribute significantly to fecal incontinence after delivery [12]. Furthermore, the complex relationship among anatomical damage, neurological disruption, and altered biomechanics necessitates the use of highly sensitive diagnostic tools to accurately characterize the extent and nature of these injuries.
Accurate diagnosis of OASIS remains clinically challenging despite the availability of established imaging modalities. Digital rectal examination, although routinely performed in the immediate postpartum period, is operator-dependent and may fail to detect occult or partial sphincter defects. Endoanal US, 3D US, and MRI are effective in identifying structural discontinuity in the sphincter complex; however, these techniques are primarily anatomical and provide limited information on tissue composition and mechanical integrity. They do not quantify biomechanical properties such as tissue stiffness, which may reflect edema, muscle disruption, fibrosis, or altered functional resilience. Furthermore, conventional imaging does not assess biomechanical susceptibility to injury during pregnancy or quantify changes in tissue properties during healing and rehabilitation. As a result, important aspects of sphincter integrity, including subtle remodeling, early fibrotic changes, or altered elastic behavior under stress, may not be fully characterized by morphology alone. These limitations highlight the need for complementary imaging approaches that provide quantitative biomechanical information alongside structural assessment.
Elastography provides quantitative and qualitative information on tissue elasticity, which changes in injured or fibrotic tissue. This technique measures the mechanical properties of tissue by assessing its response to applied force, thereby distinguishing between healthy and pathological tissue based on their relative stiffness [14]. Compared with conventional US, this noninvasive imaging modality offers a significant advantage by providing insight into the microstructural integrity of tissues, which is crucial for identifying subtle changes indicative of OASIS. Precise evaluation of the pelvic floor muscles is essential for tailoring appropriate treatment. Consequently, integration of elastography into the diagnostic protocol for OASIS could significantly improve the detection of subtle tissue alterations and provide objective, quantitative data to inform clinical decision-making. This methodology is particularly promising for distinguishing among muscle tears, scarring, and edema, as these conditions often appear similar on conventional imaging but have distinct elastic properties [14]. This capability is particularly beneficial for identifying occult injuries, in which subtle architectural distortion or fibrotic changes may contribute to symptoms such as fecal incontinence or pelvic pain. Elastography can map tissue stiffness in real time, which allows dynamic assessment of sphincter function and reveals areas of reduced contractility or increased rigidity that are not apparent on static images.
Elastography is based on the principle that changes in tissue composition and structure may be reflected by alterations in mechanical stiffness [14]. This approach enables the quantitative assessment of tissue elasticity and provides more detailed characterization of the anal sphincter musculature than conventional imaging techniques. The fundamental premise is that diseased or injured tissues often exhibit altered mechanical properties compared with healthy tissue. For example, fibrosis can lead to increased stiffness, whereas edema can lead to decreased stiffness [15]. Application of elastography in this context represents a significant advance, as it moves beyond anatomical visualization to functional tissue characterization [14]. Furthermore, both US elastography and magnetic resonance elastography (MRE) have been widely used to characterize tissue elasticity in various medical contexts, which supports their value as an adjunct to conventional imaging techniques [16].
The central thesis of this review is that tissue stiffness represents a measurable biomechanical dimension of sphincter integrity that may influence susceptibility to perineal injury, reflect structural disruption, and evolve during post-repair remodeling. However, its clinical utility depends on demonstrating reproducible associations with confirmed structural injury and functional outcomes.
An emerging model suggests that stiffness of the perineal body and EAS, as measured by SWE, may be associated with mechanical resilience during vaginal delivery. This model integrates biomechanical measurement, computational modeling, and clinical observations, while recognizing that the current evidence remains preliminary.
Pregnancy induces adaptive remodeling of pelvic floor tissues. Animal studies show increases in pelvic floor muscle stiffness and sarcomere number, which may enhance resistance to mechanical strain during delivery. In human studies, women with higher EAS stiffness during Valsalva in late pregnancy (27.0 kPa vs. 18.2 kPa) had a lower incidence of perineal tears, which suggests that greater stiffness may confer mechanical resilience under intrapartum stress [5, 17].
These findings support the hypothesis that antenatal stiffness assessment could contribute to risk stratification, although prospective validation in larger cohorts is required.
Computational modeling identifies the superior perineal body and its junction with the urogenital hiatus and anal sphincter complex as regions of maximal mechanical stress during childbirth, with reported stretch ratios that approach 1.95 and stress concentration near the EAS.
Elastographic data further indicate that a larger perineal body area at rest
during labor is associated with increased tear risk (1.0 vs. 0.3 cm2,
p
After delivery and surgical repair, healing involves collagen deposition and scar formation, which may increase tissue stiffness without restoring normal contractility. Postnatal studies show that increased pelvic floor muscle stiffness is associated with forceps delivery and pelvic floor symptoms, suggesting that excessive stiffness may reflect trauma or maladaptive remodeling rather than functional recovery [20, 21].
Residual sphincter defects, reduced manometric pressures, IAS defects, and levator avulsion remain independent predictors of anal incontinence [22, 23]. Importantly, increased stiffness should not be interpreted as synonymous with restored functional competence.
Ex vivo studies demonstrate distinct stiffness profiles across perineal tissues, including skin, vaginal wall, EAS, IAS, and anal mucosa. These differences likely reflect specialized mechanical roles during childbirth and variable susceptibility to injury [24, 25].
The aforementioned techniques, which include strain elastography, SWE, and MRE, each leverage distinct principles to quantify tissue stiffness, and offer varying degrees of penetration depth, spatial resolution, and applicability to different anatomical regions.
Strain elastography measures tissue deformation in response to an applied force, typically manual compression or physiological motion. The technology provides qualitative or semiquantitative maps of relative tissue stiffness and is widely utilized for the characterization of breast, thyroid, and prostate lesions. Its advantages include simplicity and broad availability; however, it is operator-dependent and less reproducible than SWE, with limited quantitative capability [1, 2, 3, 4]. Strain elastography assesses tissue deformation in response to external compression and provides a qualitative or semiquantitative measure of stiffness based on visual color mapping or strain ratios [14].
SWE generates and tracks the propagation speed of shear waves induced by acoustic radiation force. The measured shear wave velocity is directly related to tissue stiffness, allowing quantitative assessment. It is used for liver fibrosis staging, musculoskeletal evaluation, and tumor characterization. SWE provides quantitative stiffness measurements with reported moderate-to-good reproducibility, although reliability varies by anatomical site, acquisition protocol, and operator experience [14, 26, 27, 28, 29]. This noninvasive approach enables quantitative assessment of tissue stiffness and may detect biomechanical alterations that are not apparent on conventional imaging (Fig. 1). On the other hand, 3D endoanal US enables detailed visualization of the anal sphincter complex and accurate identification of OASIS (Fig. 2).
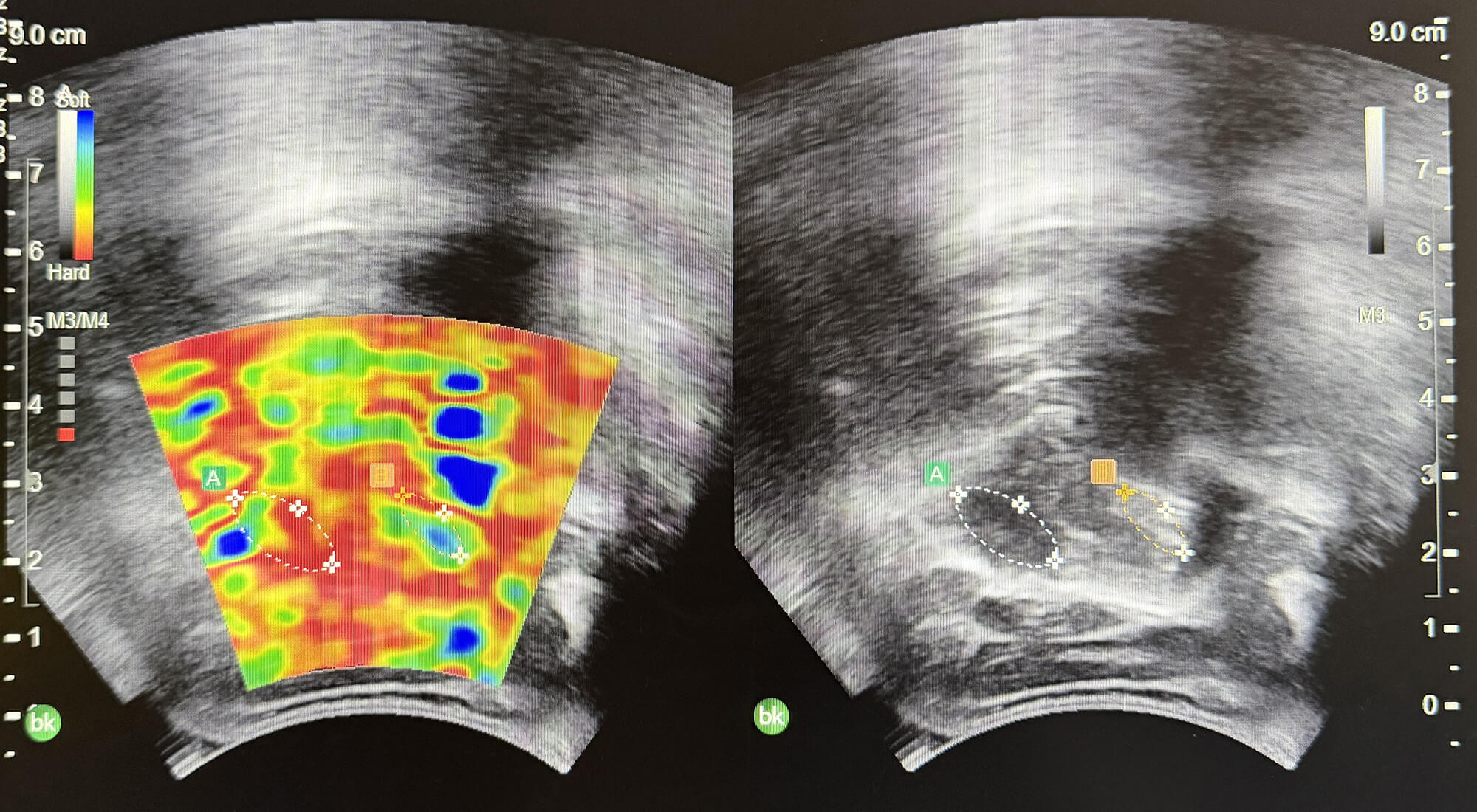 Fig. 1.
Fig. 1.
Elastographic comparison between two regions of interest (ROIs), labeled A and B, demonstrating different stiffness characteristics. Color mapping illustrates relative differences in tissue elasticity/density, highlighting the ability of elastography to distinguish tissues with varying biomechanical properties (photo by KDS).
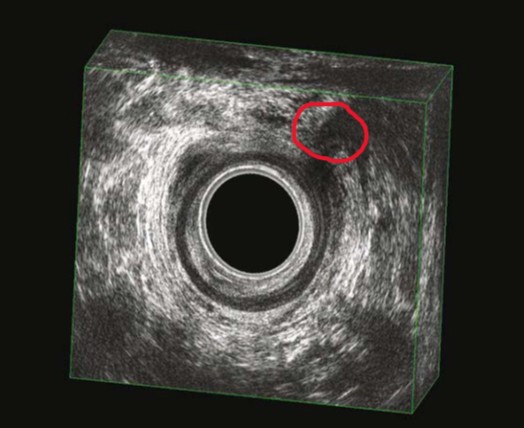 Fig. 2.
Fig. 2.
3D endoanal US image of the anal sphincter complex. The circled hypoechoic region indicates a disruption involving more than 50% of the thickness of the EAS, consistent with a Grade 3B OASIS. The IAS appears preserved. This noninvasive approach offers superior sensitivity for the detection of subtle tissue abnormalities, such as fibrosis, hematoma, and edema. The area of interest is encircled (photo by KDS). 3D, three-dimensional; EAS, external anal sphincter; IAS, internal anal sphincter.
MRE uses low-frequency mechanical vibrations in conjunction with MRI to visualize shear wave propagation, thereby facilitating whole-organ stiffness mapping. MRE is regarded as the most precise noninvasive technique for liver fibrosis staging and is used with increasing frequency for other organs. It interrogates large tissue volumes and is less affected by obesity, but it is limited by cost, availability, and susceptibility to iron overload or ascites [9, 10, 11, 12, 13, 14].
While MRE methods such as atomic force microscopy may provide insight into tissue biomechanics at the cellular level, they are currently research tools and not clinically applicable for OASIS diagnosis. Therefore, this review focuses on US-based elastography techniques [14].
Each method contributes uniquely to the diagnostic landscape, with atomic force microscopy-based elastography also emerging as a high-resolution technique for assessing biomechanical properties at the cellular level. This approach is particularly useful for understanding the microstructural changes associated with disease progression [30], although it currently faces technical and practical challenges that limit its clinical applicability [31].
The utilization of elastography in the diagnosis of OASIS is a relatively recent
development. Numerous qualitative studies have examined this field. In a study by
Allgayer et al. [15], visual elastogram color (i.e., qualitative
assessment) was compared with area-based quantification of elastic properties of
IAS vs. EAS in patients with fecal incontinence from various causes (e.g.,
surgery, Crohn’s disease), not limited to obstetric cases. The authors reported
differences in elastogram color distribution between IAS and EAS. However, no
significant correlation was observed between elastography findings and clinical
or functional parameters, including incontinence severity. Elastography reveals
various stiffness patterns; however, its clinical diagnostic value in these cases
remains uncertain [15]. The study by Gachon et al. [17] on pelvic floor
muscles and EAS stiffness during pregnancy is among the more recent research in
this field and suggests a potential predictive value, with greater EAS stiffness
associated with fewer tears. In this study, nulliparous pregnant women were
analyzed according to the following schedule: three checkup visits during
pregnancy at 14 to 18 weeks, 24 to 28 weeks, and 34 to 38 weeks. The objective of
the study was to measure the elastic properties (i.e., shear modulus, via SWE) of
the levator ani muscle and the EAS, both at rest and during the Valsalva
maneuver. The findings of the present study indicate no significant changes in
the elastic properties of the skin across pregnancy. However, in the latter
group, women with an intact perineum at the time of delivery exhibited higher EAS
stiffness (shear modulus) during the Valsalva maneuver in late pregnancy, in
comparison to those who sustained perineal tears. This suggests that greater EAS
stiffness under stress may be protective, whereas lower stiffness may predispose
to tearing [5]. In a subsequent study conducted in 2023, an in vivo
evaluation of the elastic properties of the EAS was performed in nulliparous
pregnant women (aged
The study used elastography in a small sample of women who delivered vaginally in order to analyze the size (e.g., area, length) of the perineal body, the EAS, the IAS, the anal mucosa, as well as the stiffness via SWE at rest and during the Valsalva maneuver in labor. The results revealed that the perineal body area at rest before expulsive efforts was larger in women who sustained perineal tears. Furthermore, changes in perineal body dimensions were observed between the onset of labor and the expulsive phase. However, all tears in this cohort were first-degree. This finding suggests a potential correlation between stiffness and the risk of tearing [19].
The usefulness of elastography was also assessed in patients with rectal cancer receiving chemoradiotherapy. Real-time strain elastography (RTE) was performed via endoanal US, with the objective of evaluating the stiffness (“elasticity”) of the IAS and relating it to the resting pressure measured by manometry. The findings revealed a trend of inverse correlation, albeit not statistically significant, whereby a stiffer sphincter (i.e., lower strain) was associated with lower resting pressure. The application of RTE to endoanal ultrasonography enabled the establishment of a method to evaluate IAS elasticity [8].
Based on the current literature, SWE of the EAS appears feasible in terms of pregnant women, with reported intraobserver ICC values approaching 0.90 under resting conditions and moderate-to-good interobserver agreement, depending on the measurement settings [5]. Preliminary evidence suggests that women who exhibit a higher degree of EAS stiffness under specific conditions (e.g., Valsalva) during pregnancy may demonstrate a reduced risk of perineal tears. This finding suggests the potential for its use in predicting future outcomes [5]. There is limited definitive evidence linking elastography measurements to higher-degree OASIS (i.e., third- and fourth-degree tears), or to the diagnosis of existing sphincter defects. Most studies are small in scale, and the tears assessed are either first-degree or defined as general perineal tear rather than confirmed OASIS. Comparison with US imaging (e.g., 2D/3D transperineal US [TPUS], endovaginal US [EVUS]) and endoanal US remains the standard for the detection of anatomical defects. Numerous studies have compared the sensitivity, specificity, and other performance metrics of diverse US modalities. However, recent reviews have not demonstrated compelling evidence that elastography significantly improves or contributes meaningfully to the OASIS diagnosis. It may serve as a complementary tool [32]. In cases where anatomical defects are detected by US, correlations with anal incontinence symptoms and manometry findings, including lower resting and squeeze pressures, are frequently observed.
Elastography quantifies tissue stiffness, which may reflect underlying tissue composition and structural changes (e.g., edema, tearing, fibrosis). However, current evidence that links stiffness measurements to injury severity categories and long-term functional outcomes remains limited and inconsistent. Therefore, elastography findings should be interpreted as complementary biomechanical information rather than a validated surrogate for clinical severity or prognosis. For example, the study by Allgayer et al. [15] on fecal incontinence showed differences in stiffness patterns but no strong correlation with incontinence severity. Future studies should distinguish feasibility and reproducibility outcomes from diagnostic accuracy and from prognostic or functional correlations, as these represent distinct levels of evidence.
While elastography offers significant advantages in the assessment of OASIS, there are limitations to its use. These relate primarily to operator dependency, technical constraints, and the need for standardized protocols. In addition to the favorable findings reported in existing studies, it is imperative to emphasize the key caveats and gaps in the current evidence. Many elastography studies are pilot in nature, with limited sample sizes and few higher-degree OASIS cases. A significant proportion of studies that examine the perineal body using elastography often report a predominance of first-degree tears. Data on third- and fourth-degree tears, and on the performance of elastography in these cases, remain limited. Longitudinal data remains scarce, with limited information regarding alterations in stiffness after repair and whether early postpartum elastography can predict long-term outcomes, including continence and quality of life.
To date, a variety of methods have been employed. Several factors must be considered, including the type of device, the probe, the measurement conditions (rest, Valsalva, or contraction), operator dependency, definitions of “stiff” vs. “soft”, and the region-of-interest (ROI). The correlation between function and symptoms remains unclear. Although identification of anatomical or stiffness differences is important, the key clinical value lies in the capacity to detect injury or altered elasticity for diagnostic and management purposes. Indeed, this ability to identify such changes may enable interventions that improve outcomes. However, it remains unclear whether elastography provides sufficient diagnostic value compared with established imaging techniques (i.e., endoanal ultrasound [EAUS], 3D TPUS, MRI) to justify its incorporation into routine postpartum screening for OASIS [5, 19, 33].
Based on the current evidence, it is imperative to emphasize the potential roles for elastography in this field. The utilization of this technique during pregnancy or labor may be a viable option for the purpose of risk stratification. If larger-scale studies demonstrate that specific stiffness metrics (e.g., EAS stiffness, perineal body dimensions and stiffness) can reliably predict the risk of perineal tears or sphincter injury, elastography could assist in the identification of women at higher risk who may benefit from preventive strategies such as perineal support, episiotomy, or modified pushing techniques. Elastography has the potential to complement US imaging, particularly in centers where EAUS or high-quality US is available, by incorporating a functional component (stiffness) into anatomical assessment. Following OASIS repair, elastography may facilitate monitoring of the healing process and may correlate with functional outcomes, such as reduced elasticity associated with fibrosis or scar formation. Finally, this method may support research and improve understanding of pathophysiology by clarifying the alterations that occur in the sphincter and pelvic floor muscles during pregnancy, labor, and the postpartum period, as well as the progression of stiffness, its correlation with tearing, and the processes involved in recovery.
Notwithstanding the aforementioned limitations, ongoing advances in elastography technology, including improved transducer designs and sophisticated image processing algorithms, continue to expand its diagnostic capabilities and reduce technical artefacts.
The application of elastography for diagnosing OASIS presents several significant advantages over traditional imaging modalities, primarily by providing quantitative measures of tissue mechanical properties that may reflect injury severity and healing-related tissue changes.
Specifically, elastography has the capacity to differentiate between muscle tears and fibrotic scar tissue, a distinction that is critical for prognosis and for guiding subsequent therapeutic interventions (Fig. 1). Furthermore, the quantitative nature of elastographic measurements allows for precise monitoring of healing progression and the assessment of the effectiveness of rehabilitation strategies, which offers a stronger basis for clinical decision-making [14]. This technological advancement enables clinicians to move beyond subjective assessments and provides objective data that can inform personalized treatment plans and improve long-term outcomes for patients with OASIS. Beyond diagnosis, the potential of elastography to provide real-time feedback during pelvic floor muscle training is significant, which could optimize rehabilitation protocols by enabling targeted exercises that address specific areas of sphincter weakness or fibrosis. This approach may enhance functional recovery.
Elastography is a promising adjunct technique in the assessment of OASIS, as it provides quantitative measures of tissue stiffness that may reflect underlying muscle damage and fibrotic changes. However, current evidence does not yet demonstrate clear superiority over established imaging modalities. Evidence from other clinical fields (e.g., breast imaging) demonstrates that elastography can improve tissue characterization when combined with conventional US. However, these findings cannot be directly extrapolated to OASIS, where the diagnostic task focuses on the identification of sphincter discontinuity and structural defects. Therefore, cross-domain evidence is presented herein only to illustrate the general capabilities of elastography rather than to support diagnostic performance in OASIS [34, 35].
It is important to acknowledge that prospective diagnostic accuracy studies evaluating elastography in confirmed high-grade (third- or fourth-degree) OASIS are notably absent from the current literature. No published study has systematically reported sensitivity, specificity, or predictive values for elastography in detecting anal sphincter injuries using established reference standards such as endoanal US or MRI. The available evidence is limited to feasibility and reliability data from small cohort studies, which demonstrate technical feasibility but do not allow conclusions regarding true diagnostic performance. Notably, recent meta-analyses that evaluate the diagnostic performance of US modalities for OASIS have not included elastography as a diagnostic modality [8]. The lack of diagnostic accuracy studies in high-grade OASIS represents a critical evidence gap and is identified as a key research priority.
Elastography may facilitate the detection of subtle or occult sphincter abnormalities that are difficult to identify with conventional imaging, potentially enabling earlier intervention and preventing the risk of long-term complications such as fecal incontinence [36, 37]. However, this potential remains unvalidated in prospective studies, and the clinical significance of elastography-detected abnormalities has yet to be established.
As a non-ionizing imaging modality, elastography avoids the risks associated with radiation exposure and is a safe option for repeated assessments, particularly important in patient populations that require frequent monitoring. Furthermore, the relatively short acquisition time and real-time imaging capabilities of US-based elastography enhance patient comfort, facilitating broader acceptance and applicability in clinical settings [38].
The ability to quantify tissue stiffness numerically offers the potential for an objective and reproducible metric for assessing the structural integrity and functional status of the anal sphincter complex, potentially distinguishing among healthy tissue, acute tears, and chronic fibrotic changes. In principle, these objective data may allow for a more precise classification of injury severity and assist in the development of tailored treatment strategies. However, validated stiffness thresholds that distinguish injury grades have not been established, and studies with adequate power have not demonstrated correlations between elastographic parameters and clinical outcomes. This quantitative assessment may also enable longitudinal monitoring of healing post-repair and may provide insight into the efficacy of surgical interventions and guide rehabilitation protocols, yet this application remains investigational [38, 39].
Various elastography techniques, including transperineal and endoanal approaches, have been adapted to the specific anatomical characteristics of the anal sphincter. Each approach offers distinct theoretical advantages in accessibility, resolution, and ability to characterize the complex multilayered structure of the sphincter [8, 37].
Transperineal elastography, performed via an external approach, offers a noninvasive and comprehensive overview of the entire anal sphincter complex and may be useful for initial screening and follow-up examinations in a less intrusive manner [40, 41].
Endoanal elastography has the potential to provide higher-resolution images and more localized strain measurements by placing the transducer directly within the anal canal. Theoretically, this approach allows detailed assessment of individual sphincter layers and more precise identification of specific defects or areas of fibrosis. This direct contact may also minimize artefacts and signal attenuation, potentially providing clearer elastographic maps for detailed diagnostic analysis. This technique is proposed as being particularly advantageous for the evaluation of complex or recurrent injuries, with the potential to offer a refined understanding of the sphincter’s biomechanical state and to aid in the precise surgical planning. However, comparative diagnostic accuracy data are lacking [8].
The accuracy and reliability of elastographic measurements are contingent on the skill and experience of the sonographer. Sonographers should recognize that consistent probe application and image acquisition are crucial to obtaining valid data. This inherent subjectivity necessitates extensive training and adherence to standardized protocols to mitigate interoperator variability and ensure reproducibility of results, particularly in complex cases such as OASIS assessment. Furthermore, the learning curve associated with mastering advanced elastography techniques may impede its widespread adoption in general clinical practice. The standardization of imaging protocols, coupled with the emergence of artificial intelligence (AI)-driven analysis tools, has the potential to mitigate this dependency, thereby enhancing the reliability and accessibility of the technique [42]. The diagnostic efficacy of elastography can also be hampered by technical constraints, such as the inherent limitations of US signal penetration in obese patients or the presence of gas within the bowel, which can obscure the anal sphincter and compromise image quality. Furthermore, anatomical variations or prior surgical interventions may alter normal tissue architecture, thus challenging the accurate interpretation of stiffness measurements and potentially leading to misdiagnosis [43]. These challenges underscore the ongoing need for advanced technological solutions and rigorous training methodologies to fully harness the potential of elastography in clinical settings. Ongoing research aims to overcome these technical hurdles through innovations in transducer design, software algorithms, and the integration of machine learning (ML) for automated image analysis. These advances will improve the robustness and applicability of elastography across diverse patient populations.
The complexity of elastography requires a substantial learning curve for operators to achieve proficiency, which impacts widespread clinical adoption of this advanced diagnostic modality. This includes not only the acquisition of high-quality elastograms but also their accurate interpretation, often requiring specialized training beyond conventional US education.
The initial investment in elastography equipment and the ongoing costs associated with specialized training for personnel can present a significant barrier to implementation, particularly in healthcare settings with limited resources. Furthermore, maintenance and upgrading of these sophisticated systems add to the long-term financial burden, making careful cost-benefit analyses essential before widespread integration.
These innovations include the development of higher-frequency probes that offer improved spatial resolution, as well as novel elastography techniques such as SWE and strain elastography, which provide quantitative measurements of tissue stiffness [44]. The further integration of AI and ML algorithms may automate image analysis and enhance diagnostic accuracy, thereby reducing operator dependency and improving the efficiency of elastography in clinical practice [45]. The application of AI/ML models has the potential to facilitate a more nuanced understanding of tissue characteristics by identifying subtle patterns not discernible to the human eye. This, in turn, may improve diagnostic precision and potentially reduce the necessity for invasive procedures [45].
The integration of AI and ML algorithms is poised to revolutionize the interpretation of elastographic data by enabling automated segmentation, classification, and quantification of tissue stiffness, thereby enhancing diagnostic accuracy and reproducibility. This integration is pivotal in addressing current limitations, including operator dependency and the demanding learning curve, by offering objective and consistent analyses of elastography images.
These advanced computational methods are capable of analyzing large elastography datasets, identifying subtle patterns indicative of injury and disease progression that may be overlooked by human interpretation, thereby enhancing diagnostic precision. Specifically, image-based deep learning algorithms have demonstrated considerable potential in medical imaging, offering automated interpretation and improved diagnostic accuracy across a range of modalities, including echocardiography and general wound assessment. These AI-driven approaches can recognize complex patterns and features within medical images that are not readily discernible to the human eye. This provides a new perspective on which image features are most valuable for decision support [46]. The application of deep learning in elastography has the potential to significantly alleviate the workload on healthcare providers while simultaneously improving the sensitivity of early detection for anal sphincter injuries.
Although elastography shows investigational potential in the assessment of OASIS, the available evidence derives predominantly from small pilot studies with limited sample sizes, and there is a notable scarcity of investigations that specifically evaluate higher-grade (third- and fourth-degree) OASIS. Several studies have reported neutral or negative findings that warrant cautious interpretation of novel imaging approaches. Huber et al. [4] reported that 3D-EAUS performed in a maternity ward setting did not provide additional diagnostic value beyond clinical examination, with a sensitivity of 30.4% and a positive predictive value of 9.9%. Similarly, Taithongchai et al. (2019) [33] reported low positive predictive values (0.37–0.63) for introital and transperineal US in identifying sphincter defects, concluding that these modalities may have limited reliability for definitive defect identification. The American College of Obstetricians and Gynecologists (ACOG, 2018) [47] reported a false-positive rate of approximately 24% for endoanal ultrasonography and does not recommend routine postpartum EAUS for occult OASIS screening. In the context of perineal body assessment, Zhou et al. [48] found no statistically significant association between perineal body measurements and levator hiatal area, suggesting that isolated morphometric parameters may not adequately reflect pelvic floor support. Taken together, these findings suggest that both conventional US modalities and emerging elastography techniques face important diagnostic limitations. At present, no imaging modality has demonstrated sufficiently robust and reproducible diagnostic accuracy to independently redefine OASIS classification or replace established multimodal clinical assessment.
Additional limitations specific to elastography include substantial heterogeneity across studies in equipment, probes, acquisition protocols, measurement conditions (rest, Valsalva maneuver, contraction), and stiffness quantification methods. This variability limits the comparability and generalizability of the findings. Vukasović et al. [49] further highlighted significant heterogeneity in perineal body imaging methodologies across published studies, emphasizing the urgent need for consensus acquisition protocols and standardized reporting frameworks before elastography can be integrated into routine clinical practice. Elastographic assessment also remains operator-dependent and involves a learning curve, which may influence reproducibility in routine clinical settings.
Furthermore, longitudinal data that evaluate whether elastographic parameters correlate with clinically meaningful long-term outcomes, such as anal continence, quality of life, or response to surgical repair and rehabilitation, remain lacking.
Importantly, these methodological and evidentiary limitations directly impair routine clinical implementation. In the absence of validated normative reference ranges, clinicians cannot reliably determine whether a measured stiffness value reflects physiologic variation or pathologic change. Heterogeneity in acquisition protocols and equipment prevents reproducible application across centers, limiting external validity and widespread adoption. Without robust prospective diagnostic accuracy data relative to established reference standards, elastography cannot be integrated into diagnostic algorithms or justify modification of existing OASIS classification systems. Moreover, the lack of demonstrated correlation with long-term functional outcomes prevents stiffness measurements from informing prognosis, surgical planning, or rehabilitation strategies. As a result, elastography currently remains an investigational or adjunctive modality rather than a validated component of standard OASIS assessment.
To translate elastography from an investigational modality into a clinically integrated diagnostic adjunct, several structured research objectives must be addressed. Normative reference values for EAS and perineal body stiffness should be established through adequately powered, multicenter studies, stratified by parity, gestational stage, and measurement conditions. Prospective diagnostic accuracy trials that directly compare elastography with established reference standards, such as endoanal US and/or MRI, in women with clinically confirmed high-grade OASIS are required, with systematic reporting of sensitivity, specificity, predictive values, and likelihood ratios. Longitudinal outcome studies are necessary to determine whether elastographic parameters correlate with clinically meaningful endpoints, including anal continence, symptom severity, quality of life, and response to surgical repair or rehabilitation. Finally, methodological standardization through consensus guidelines that address probe selection, ROI placement, acquisition protocols, measurement conditions, and stiffness reporting units is essential to ensure reproducibility and cross-study comparability. Addressing these defined research priorities will determine whether elastography remains a research tool or evolves into a validated adjunct in OASIS diagnostics.
While elastography presents a promising noninvasive diagnostic tool for OASIS, its widespread adoption hinges on overcoming current technical challenges and improving accessibility. Continued research and technological advancements, particularly integration of AI for automated analysis, are critical to realize its full potential in clinical practice. Elastography is an emerging tool in obstetric and pelvic floor imaging, particularly SWE and strain elastography. Current evidence supports its feasibility and reliability in measuring EAS stiffness during pregnancy, with early data suggesting a potential role in risk stratification, postpartum monitoring, and possibly early detection of occult sphincter injury. However, for established OASIS, endoanal US, 3D US (translabial or transperineal), and MRI remain the reference standards. On the contrary, manometry serves as a complementary functional assessment tool. Further multicenter studies with standardized protocols, validated reference ranges, and integration of AI are required to define the diagnostic and prognostic value of elastography in this field.
KDS conceived the idea for the article, performed the literature review, and drafted the manuscript. PB, VS, GN, DH, DL, and MJ reviewed the literature, supervised the work, and contributed to manuscript editing and final approval. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflicts of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.