

 , Neset Gumusburun 2,*
, Neset Gumusburun 2,* , Ozge Deniz Unyeli 1, Sebati Sinan Urkmez 3, Samettın Celik 1, Yesim Civil Urkmez 4
, Ozge Deniz Unyeli 1, Sebati Sinan Urkmez 3, Samettın Celik 1, Yesim Civil Urkmez 41 Department of Obstetrics and Gynecology, Samsun University Faculty of Medicine, 55080 Samsun, Turkiye
2 Department of Obstetrics and Gynecology, Istanbul Aydın University Faculty of Medicine, 34295 Istanbul, Turkiye
3 Department of Medical Biochemistry, Ondokuz Mayis University Faculty of Medicine, 55270 Samsun, Turkiye
4 Department of Medical Biochemistry, Samsun University Faculty of Medicine, 55090 Samsun, Turkiye
Abstract
Preeclampsia (PE) is a multisystem disease that can affect all pregnant women and lead to numerous feto-maternal complications. Currently, early prediction of this condition remains challenging. In this study, we aimed to evaluate the potential of maternal serum cadherin-6 (CDH-6) levels measured between 15 and 20 weeks of gestation, to predict the subsequent development of PE later in pregnancy.
In this prospective cohort study, 75 pregnant women, diagnosed with PE during the follow-up period, and 75 healthy pregnant women at matching gestational weeks were included. Blood samples from all 150 participants were first centrifuged and stored, and serum CDH-6 levels were analysed by enzyme-linked immunosorbent assay (ELISA).
Serum CDH-6 levels, measured in the second trimester, were significantly higher in pregnancies that later developed PE compared with controls (375.3 vs. 93.1 ng/mL, p < 0.001), with the highest levels observed in early-onset cases. CDH-6 showed an excellent diagnostic performance for PE (area under the curve [AUC] = 0.983) and a good accuracy in distinguishing early- from late-onset disease (AUC = 0.801).
High CDH-6 levels, detected in the second trimester, may serve as an early warning marker for the development of PE. This finding may contribute to clinical practice by enabling timely diagnosis of high-risk pregnancies.
The study is registered on the National Clinical Trial (NCT) at https://clinicaltrials.gov/study/NCT07467226?cond=NCT07467226&viewType=Card&rank=1 (registration number: NCT07467226).
Keywords
- cadherin-6
- preeclampsia
- pregnancy
- biomarker
- second trimester
Preeclampsia (PE) is a serious pregnancy-specific hypertensive disorder and remains one of the major causes of maternal and fetal morbidity and mortality worldwide [1]. The condition typically develops after 20 weeks of gestation and is characterised by hypertension accompanied by proteinuria or evidence of systemic organ dysfunction [2]. PE affects approximately 2–5% of all pregnancies and represents an important contributor to maternal mortality, particularly in low- and middle-income settings [3]. Although maternal deaths are rare in developed countries, recent reports indicate that the incidence of PE has increased and that it continues to contribute to maternal mortality [4, 5].
Although the pathogenesis of PE has not yet been fully elucidated, impaired placental invasion, inadequate remodelling of spiral arteries, placental hypoxia, and subsequent endothelial dysfunction are considered key contributing factors [6]. Failure of trophoblasts to reach adequate differentiation and invasion capacity, especially in early pregnancy, leads to decreased uteroplacental perfusion and underlies the development of PE [7].
In this context, adhesion molecules involved in placental development may play determinant roles in the pathogenesis of PE. Cadherins are calcium-dependent transmembrane glycoproteins that provide intercellular adhesion and play an important role in the regulation of the invasive capacity of trophoblasts [8]. Cadherin-6 (CDH-6), a type 2 cadherin, is prominently expressed in extravillous trophoblasts and plays an active role in the development of the kidney and central nervous system during embryogenesis. Controlled invasion of trophoblasts into the decidua during normal pregnancy is facilitated by the regulated expression of CDH-6 and related molecules [9].
A recent study has reported that serum CDH-6 levels may be associated with PE. In a pilot study conducted by Güvey et al. [10], CDH-6 and cadherin-11 (CDH-11) levels were significantly increased, especially in patients with early-onset and severe PE. These findings suggest that cadherin family molecules may have potential not only in placental development, but also in the diagnosis and prediction of pathological conditions.
On the other hand, the need for early biomarkers to predict PE is critical in clinical practice, as the development of PE can be prevented in high-risk pregnant women with the use of low-dose aspirin [11]. However, the methods currently used in clinical practice are often applied only after the onset of overt symptoms. However, several studies have reported that levels of circulating biomolecules may change weeks or even months before the onset of PE [12, 13]. In this context, early detection of CDH-6 may contribute to assessing the risk of PE.
The aim of this study is to investigate the potential of maternal serum CDH-6 levels measured in the early second trimester of pregnancy (15–20 weeks) to predict the subsequent development of PE. This approach may enable earlier intervention against PE and improve maternal and fetal outcomes.
This study was designed as a prospective observational cohort study and conducted in pregnant women followed at the Gynecology and Obstetrics Clinic of Samsun Training and Research Hospital between January 1, 2024, and December 1, 2024. Ethical approval was obtained prior to the analytical phase of the study (Ethics Committee Approval No. GOKAEK-2024/2/15). Blood samples were collected as part of routine antenatal care (triple screening tests) and stored under appropriate conditions. The study was observational in nature, and no additional procedures or interventions were performed prior to ethical approval. Following ethical approval, the stored samples were analyzed, and patients were followed prospectively until delivery. All participants provided written informed consent, and clinical data were obtained from prospectively recorded hospital records. This study was retrospectively registered at ClinicalTrials.gov (https://clinicaltrials.gov/) (Identifier: NCT07467226).
A total of 150 pregnant women were included in the study. Participants were selected from volunteers who presented for triple screening tests, had confirmed gestational age, and met the eligibility criteria. During the follow-up period, 75 pregnant women who met the diagnostic criteria for PE in the subsequent weeks were assigned to the study group. The control group consisted of 75 pregnant women who were followed during the same time period at the same center and who did not develop any pregnancy complications. No individual matching was performed between the groups; therefore, some demographic differences between groups were anticipated.
Pregnant women aged between 18 and 45 years with a singleton pregnancy and a gestational age of 15 to 20 weeks (confirmed by first-trimester ultrasound), whose serum samples obtained during screening tests were stored under appropriate conditions, and who either developed PE during the follow-up or had a healthy pregnancy were included in the study.
Pregnant women with a history of systemic diseases, such as chronic hypertension, pregestational diabetes, and renal disease; autoimmune diseases, such as systemic lupus erythematosus and antiphospholipid syndrome; multiple pregnancies; fetal structural or chromosomal abnormalities; active smoking or alcohol use; and those with a history of drug abuse or immunosuppressive therapy were excluded.
The 75 pregnant women included in the study group consisted of individuals
diagnosed with PE in accordance with international guidelines (blood pressure
Peripheral blood samples were collected from pregnant volunteers between the 16th and 18th weeks of gestation. Following collection, the samples were centrifuged at 3000 rpm for 5 minutes to separate the serum. The resulting serum was aliquoted into two portions. One portion was utilized for triple screening tests, including alpha-fetoprotein, unconjugated estriol, and human chorionic gonadotropin (hCG), as well as for routine biochemical and hematological analyses. The remaining serum was transferred into sterile 1.5 mL microcentrifuge tubes and stored at –80 °C until the day of analysis.
On the day of analysis, frozen serum aliquots were thawed at 4 °C, briefly vortexed, and centrifuged using a benchtop centrifuge to remove cellular debris. Serum concentrations of human CDH-6 were determined using a commercially available ELISA kit (BT Lab Company, Cat. No. E6937Hu; Shanghai, China), based on a double-antibody sandwich ELISA technique.
Prior to the assay, all reagents and serum samples were equilibrated to room temperature (25 °C). A five-point standard curve was generated using serial dilutions of CDH-6 standards (75.0, 150.0, 300.0, 600.0, and 1200.0 ng/mL; S1–S5). ELISA wells were assigned to standards, samples, and blanks. For blank wells, only Chromogen A, Chromogen B, and stop solution were added. For test wells, 50 µL of each standard or sample was added, followed by 40 µL of detection buffer and 10 µL of CDH-6 antibody solution. Subsequently, 50 µL of streptavidin–horseradish peroxidase (HRP) conjugate was added, and the plate was incubated at 37 °C for 60 minutes. After incubation, the plate was washed five times using 350 µL of wash buffer per well. Subsequently, 50 µL of Chromogen A and 50 µL of Chromogen B were added to each well, and the plate was incubated for an additional 10 minutes at 37 °C. The enzymatic reaction was terminated by adding 50 µL of stop solution. Absorbance was measured at 450 nm using a microplate reader (Synergy 4, Serial No. 233513; BioTek Instruments Inc., Winooski, VT, USA). CDH-6 concentrations were calculated based on the standard curve and expressed as ng/mL. According to the manufacturer’s instructions, the assay has a sensitivity of 4.93 ng/mL and a dynamic detection range of 10.0–2000.0 ng/mL. Samples exceeding the upper limit of detection were appropriately diluted and reanalyzed.
All statistical analyses were conducted using IBM SPSS Statistics version 21.0
(IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean
An a priori sample size calculation was not performed because of the observational and cohort design and the inclusion of all eligible participants during the study period. However, a post hoc power analysis was conducted. In addition, the narrow confidence intervals (CIs) and high sensitivity values suggest a low probability of false-negative results. Based on these findings, the statistical power of the study was considered to exceed 80%. Receiver operating characteristic (ROC) analyses were performed primarily to evaluate the discriminatory ability of serum CDH-6 levels for the presence of PE. Additional ROC analyses were conducted as secondary analyses to assess the ability of CDH-6 to differentiate early- and late-onset PE among affected cases. Continuous variables that were not normally distributed were summarized as median (minimum–maximum), and all between-group comparisons were performed using non-parametric tests based on median values. ROC curve analyses were performed to evaluate the diagnostic performance of serum CDH-6 levels for distinguishing PE from normotensive pregnancies. The area under the curve (AUC) was calculated to assess discriminatory ability. Optimal cutoff values were determined using the Youden index. Because the study groups were not matched for baseline characteristics, multivariable logistic regression analysis including maternal age, BMI, and parity was performed to reduce the potential confounding effect of these variables. ROC analyses were considered the primary approach for evaluating the biomarker performance of serum CDH-6 in predicting PE, whereas logistic regression analyses were performed as secondary analyses to explore associations within PE subgroups.
In this study, a total of 150 pregnant women who underwent serum sampling during the second trimester and whose birth outcomes were recorded afterwards were included. PE was developed in 75 participants during the subsequent weeks of pregnancy, whereas the remaining 75 completed pregnancy without complications and constituted the control group. Demographic and clinical data were fully recorded for both groups and were available for statistical analyses.
According to the data summarized in Table 1, pregnant women who developed PE
were significantly older than controls, with a higher median age (32 [20–43] vs.
26 [19–39] years; p
| Control group (n = 75) | PE group (n = 75) | p-value | |||
| Maternal characteristics | |||||
| Age (years) | 27.28 |
32.01 |
|||
| 26.0 (19.0–39.0) | 32.0 (20.0–43.0) | ||||
| BMI (kg/m2) | 25.48 |
26.84 |
0.249b | ||
| 25.0 (21.0–36.0) | 25.0 (21.0–39.0) | ||||
| Gravidity | 1.77 |
3.20 |
|||
| 1.0 (1.0–3.0) | 3.0 (1.0–8.0) | ||||
| Parity | 0.77 |
1.79 |
|||
| 0.0 (0.0–2.0) | 2.0 (0.0–6.0) | ||||
| Serum AST (U/L) | 16.76 |
34.70 |
|||
| 15.5 (9.7–38.8) | 22.7 (7.2–99.0) | ||||
| Serum ALT (U/L) | 12.30 |
42.38 |
|||
| 9.6 (3.6–51.5) | 13.8 (3.7–222.0) | ||||
| Plasma hemoglobin (g/dL) | 11.06 |
10.27 |
0.002b,* | ||
| 11.3 (7.6–14.4) | 10.2 (7.7–13.7) | ||||
| Plasma platelet (109/L) | 226.00 |
201.13 |
0.027b,* | ||
| 209.0 (101.0–497.0) | 190.0 (89.0–392.0) | ||||
| Systolic blood pressure (mmHg) | 111.40 |
173.44 |
|||
| 110.0 (85.0–130.0) | 170.0 (155.0–200.0) | ||||
| Diastolic blood pressure (mmHg) | 64.67 |
133.00 |
|||
| 65.0 (45.0–80.0) | 135.0 (110.0–160.0) | ||||
| Mode of delivery [n (%)] | Cesarean section | 42.0 (56.0%) | 35.0 (46.7%) | 0.253c | |
| Vaginal delivery | 33.0 (44.0%) | 40.0 (53.3%) | |||
| Serum CDH-6 (ng/mL) | 99.43 |
434.28 |
|||
| 93.1 (50.2–201.7) | 375.3 (189.8–776.0) | ||||
| Fetal characteristics | |||||
| Gestational age at birth (weeks) | 39.21 |
35.65 |
|||
| 39.0 (37.0–41.0) | 37.0 (29.0–41.0) | ||||
| Birth weight (g) | 3443.87 |
2692.27 |
|||
| 3500.0 (3000.0–3990.0) | 2700.0 (1310.0–5030.0) | ||||
| Apgar score (1 min) | 8.33 |
8.16 |
0.434b | ||
| 9.0 (4.0–9.0) | 9.0 (4.0–9.0) | ||||
| Apgar score (5 mins) | 8.79 |
8.64 |
0.717b | ||
| 9.0 (5.0–10.0) | 9.0 (4.0–10.0) | ||||
| MSAF [n (%)] | 11.0 (14.7%) | 16.0 (21.3%) | 0.288c | ||
| NICU [n (%)] | 13.0 (17.3%) | 17.0 (22.7%) | 0.414c | ||
Abbreviations: PE, preeclampsia; BMI, body mass index; AST, aspartate aminotransferase; ALT, alanine aminotransferase; CDH-6, cadherin-6; MSAF, meconium-stained amniotic fluid; NICU, neonatal intensive care unit.
aData are given as mean
bMann-Whitney U Test.
cPearson
*p
Table 2 summarizes maternal serum CDH-6 levels and neonatal outcomes. Median
CDH-6 levels were significantly higher in the PE group compared with controls
(375.3 [189.8–776.0] vs. 93.1 [50.2–201.7] ng/mL; p
| Control group (n = 75) | Late-onset PE group (n = 45) | Early-onset PE group (n = 30) | p-value | |||
| Maternal characteristics | ||||||
| Age (years) | 27.28 |
31.64 |
32.57 |
|||
| 26.0 (19.0–39.0)† | 31.0 (21.0–42.0)‡ | 33.5 (20.0–43.0)‡ | ||||
| BMI (kg/m2) | 25.48 |
27.13 |
26.40 |
0.385b | ||
| 25.0 (21.0–36.0)† | 26.0 (21.0–39.0)† | 25.0 (21.0–35.0)† | ||||
| Gravidity | 1.77 |
3.40 |
2.90 |
|||
| 1.0 (1.0–3.0) | 3.0 (1.0–8.0)‡ | 2.0 (1.0–7.0)‡ | ||||
| Parity | 0.77 |
1.89 |
1.63 |
|||
| 0.0 (0.0–2.0)† | 2.0 (0.0–6.0)‡ | 1.0 (0.0–5.0)‡ | ||||
| Serum AST (U/L) | 16.76 |
33.04 |
37.20 |
|||
| 15.5 (9.7–38.8)† | 21.5 (7.2–88.0)‡ | 23.7 (13.3–99.0)‡ | ||||
| Serum ALT (U/L) | 12.30 |
44.19 |
39.67 |
0.001b,* | ||
| 9.6 (3.6–51.5)† | 13.0 (3.7–222.0)‡ | 13.8 (4.6–199.0)‡ | ||||
| Plasma hemoglobin (g/dL) | 11.06 |
10.11 |
10.51 |
0.004b,* | ||
| 11.3 (7.6–14.4)† | 9.9 (7.7–13.1)‡ | 10.6 (7.9–13.7)† | ||||
| Plasma platelet (109/L) | 226.00 |
199.51 |
203.57 |
0.088b | ||
| 209.0 (101.0–497.0)† | 190.0 (89.0–377.0)† | 192.5 (91.0–392.0)† | ||||
| Systolic blood pressure (mmHg) | 111.40 |
171.98 |
175.63 |
|||
| 110.0 (85.0–130.0)† | 170.0 (155.0–195.0)‡ | 179.5 (155.0–200.0)‡ | ||||
| Diastolic blood pressure (mmHg) | 64.67 |
131.89 |
134.67 |
|||
| 65.0 (45.0–80.0)† | 130.0 (110.0–160.0)‡ | 135.0 (110.0–160.0)‡ | ||||
| Mode of delivery [n (%)] | Cesarean section | 40.0 (53.3%)† | 31.0 (68.9%)‡ | 9.0 (30.0%)† | 0.002c,* | |
| Vaginal delivery | 35.0 (46.7%)† | 14.0 (31.1%)‡ | 21.0 (70.0%)† | |||
| Serum CDH-6 (ng/mL) | 99.43 |
373.46 |
525.51 |
|||
| 93.1 (50.18–201.7)† | 359.69 (189.82–581.81)‡ | 523.86 (231.18–776.0)§ | ||||
| Fetal characteristics | ||||||
| Gestational age at birth (weeks) | 39.21 |
38.11 |
31.97 |
|||
| 39.0 (37.0–41.0)† | 38.0 (34.0–41.0)‡ | 32.0 (29.0–36.0)§ | ||||
| Birth weight (g) | 3443.87 |
3215.38 |
1907.60 |
|||
| 3500.0 (3000.0–3990.0)† | 3200.0 (1760.0–5030.0)‡ | 1717.5 (1310.0–3410.0)§ | ||||
| Apgar score (1 min) | 8.33 |
8.91 |
7.03 |
|||
| 9.0 (4.0–9.0)† | 9.0 (5.0–9.0)‡ | 7.0 (4.0–9.0)§ | ||||
| Apgar score (5 mins) | 8.79 |
9.33 |
7.60 |
0.001b,* | ||
| 9.0 (5.0–10.0)† | 9.0 (5.0–10.0)† | 7.0 (4.0–10.0)§ | ||||
| MSAF [n (%)] | 11.0 (14.7%)† | 1.0 (2.2%)† | 15.0 (50.0%)‡ | |||
| NICU [n (%)] | 13.0 (17.3%)† | 0.0 (0.0%)‡ | 17.0 (56.7%)§ | |||
aData are given as mean
bKruskal-Wallis Test.
cPearson
*p
†, Significant difference compared with the control group; ‡, Significant difference between late-onset and early-onset PE groups;
§, Significant difference compared with both control and late-onset PE groups; with p
As a secondary analysis, logistic regression was performed to evaluate the
association between serum CDH-6 levels and the timing of disease onset among PE
cases Table 3. The relationship between serum CDH-6 levels and early-onset (
| Variable | AOR (95% CI) | p-value |
| CDH-6 | 0.99 (0.98–0.99) | |
| Age | 0.95 (0.87–1.05) | 0.360 |
| BMI | 1.13 (0.99–1.28) | 0.054 |
| Parity | 0.56 (0.11–2.85) | 0.487 |
AOR, adjusted odds ratio; CI, confidence interval.
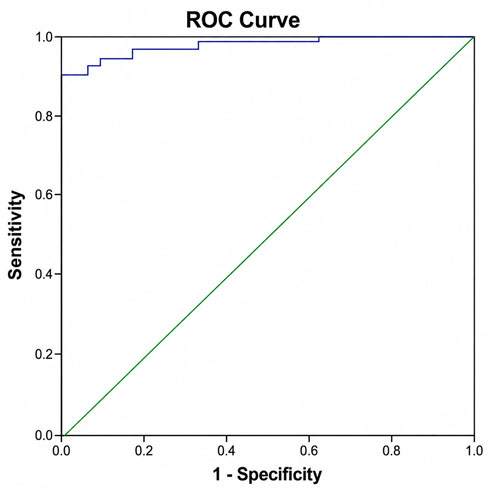
ROC analysis demonstrated that serum CDH-6 levels showed very high discriminatory performance in distinguishing PE from normotensive pregnant women (control group). The AUC was 0.983 (95% CI: 0.96–1.00). Using the Youden index, an optimal cutoff value of 103.5 was identified, yielding a sensitivity of 98.8% and a specificity of 69.1% (Table 4, Fig. 1).
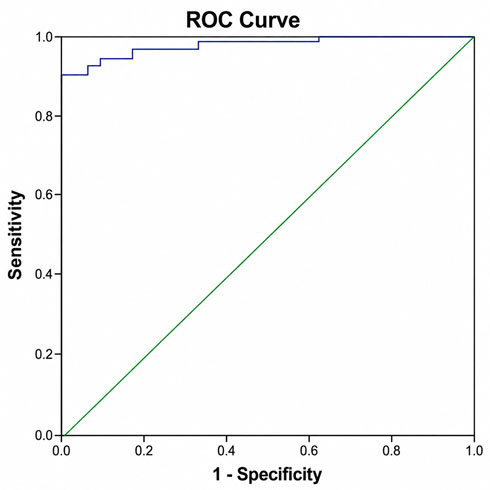 Fig. 1.
Fig. 1.
ROC curve for serum CDH-6 levels distinguishing PE from normotensive controls.
| Parameter | Value |
| AUC | 0.983 |
| 95% CI | 0.96–1.00 |
| Optimal cutoff (Youden index) | 103.5 |
| Sensitivity (%) | 98.8 |
| Specificity (%) | 69.1 |
ROC, receiver operating characteristic; AUC, area under the curve.
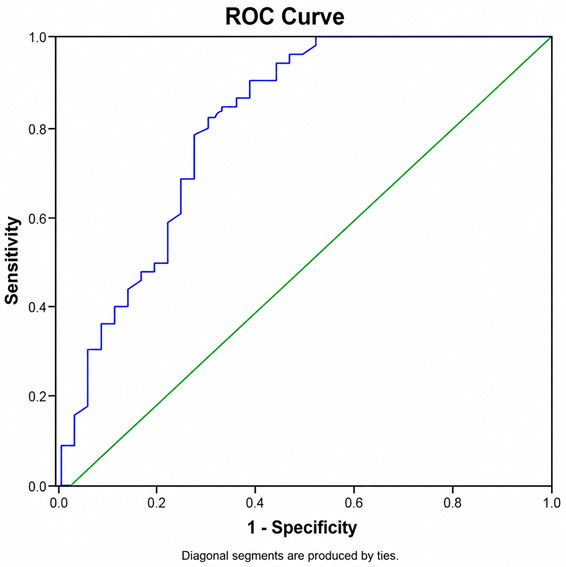
When PE cases were evaluated internally, ROC analysis revealed that serum CDH-6
levels had good discriminatory ability for distinguishing early-onset (
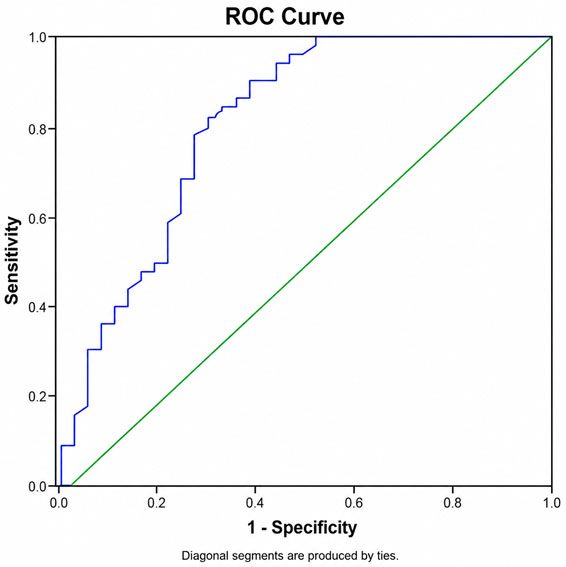 Fig. 2.
Fig. 2.
ROC curve for serum CDH-6 levels differentiating early-onset
(
| Parameter | Value |
| AUC | 0.801 |
| 95% CI | 0.70–0.90 |
| Optimal cutoff (Youden index) | 565.1 |
| Sensitivity (%) | 96.0 |
| Specificity (%) | 50.0 |
The present study demonstrated that maternal serum CDH-6 levels measured between 15–20 weeks of gestation were significantly higher in pregnancies that subsequently developed PE than in normotensive controls. Moreover, the more pronounced elevation observed in early-onset PE suggests that CDH-6 may be particularly useful for early risk stratification in high-risk pregnancies. In the present study, ROC analysis was used as the primary method to evaluate the predictive performance of CDH-6 for PE, whereas logistic regression analyses were performed as secondary analyses to examine the association of CDH-6 with disease subtypes.
PE is a complex pregnancy complication associated with substantial maternal and fetal morbidity, highlighting the importance of early identification of high-risk pregnancies. Despite extensive research on predictive biomarkers, reliable and widely applicable markers for early diagnosis remain lacking [15, 16, 17].
Recent studies have highlighted the roles of cadherins, a family of cell adhesion molecules, in pregnancy physiology and pathology [18, 19]. These molecules, which mediate intercellular adhesion, play a role in critical mechanisms such as trophoblast invasion and spiral artery remodelling during the placentation process [9]. In this context, members of the cadherin family are thought to contribute to the pathogenesis of PE.
A previous study has reported that CDH-11 levels were increased in preeclamptic placental tissues, which may limit trophoblast invasion by affecting cell-cell adhesion [10]. In the same study, CDH-6 levels were also shown to increase in association with PE, with this elevation becoming significant in the later weeks of pregnancy. Consistent with these findings, CDH-6 levels in our study exhibited a similar pattern of increase. In addition to the established roles of CDH-6 and CDH-11 in trophoblast invasion and placental development, recent evidence has highlighted the potential relevance of CDH-18 in PE. A recent study by Gumusburun et al. [20] demonstrated that maternal serum CDH-18 levels measured in the early second trimester were significantly higher in pregnancies that subsequently developed PE, particularly in early-onset cases. These findings strengthen the hypothesis that multiple members of the cadherin family may contribute to the pathophysiology of PE through mechanisms involving abnormal cellular adhesion, impaired trophoblast remodeling, and endothelial dysfunction.
Another notable finding of our study was that CDH-6 levels were higher in the early-onset PE group compared with late-onset cases. This may be explained by the fact that early-onset PE usually shows a more severe clinical course and is pathophysiologically associated with more pronounced endothelial dysfunction [21]. The literature also suggests a correlation between the levels of biomarkers used to predict PE and the severity of this pregnancy complication [10, 22, 23]. Accordingly, CDH-6 may be helpful in predicting not only the risk of PE, but also its severity and timing.
The literature has also reported that afamin, a glycoprotein associated with oxidative stress, exhibits increased serum levels in inflammatory conditions such as PE [12]. The association between oxidative stress markers such as afamine and PE suggests that CDH-6 may also be elevated in response to similar inflammatory processes. However, CDH-6 levels should be evaluated in correlation with other inflammatory and oxidative stress markers in order to establish this situation definitively.
Periostin is another matrix protein associated with PE. Increased periostin levels suggest a role in extracellular matrix remodelling and vascular permeability [24]. Sasaki et al. [25] reported that periostin levels were significantly higher in women with PE and that this increase may also be associated with fetal growth restriction. Similarly, the lower birth weights, lower Apgar scores, and increased NICU admission rates observed in the PE group in our study indicate a poor perinatal prognosis in these patients. In this context, our findings suggest that CDH-6 levels may be associated with perinatal outcomes beyond the diagnosis of PE. However, further studies with a longer follow-up period are needed to confirm this hypothesis and to determine whether CDH-6 is an independent prognostic biomarker.
The biomarker potential of the cadherin family has been demonstrated previously by Ahmed et al. [26], who reported high discriminatory performance based on ROC analysis. Consistent with these findings, we found that maternal serum CDH-6 levels exhibited strong diagnostic accuracy for predicting PE. CDH-6 distinguished preeclamptic pregnancies from normotensive controls with very high ROC performance, supporting its potential value as an early second-trimester screening biomarker. In addition, subgroup analyses showed that CDH-6 effectively differentiated early-onset from late-onset PE, indicating that higher CDH-6 levels may be associated with more severe disease phenotypes. Altogether, these results suggest that CDH-6 has clinically meaningful predictive value and may contribute to risk stratification during mid-pregnancy.
However, our study has several limitations. Firstly, its single-center design and relatively limited sample size may restrict the generalizability of the findings. Additionally, the sociodemographic homogeneity of the study population may have reduced the ability to account for potential environmental or genetic variability. Nevertheless, evaluating biomarker levels during the second trimester enabled assessment prior to the clinical onset of PE, which represents an important methodological strength. The prospective design, uniform follow-up protocol, and comprehensive analytical approach, including ROC analyses for diagnostic performance and subgroup evaluations, enhance the reliability of the results. Future multicenter studies with larger and more diverse populations, as well as complementary assessments such as placental or cord blood biomarker analyses, are needed to more definitively establish the clinical utility and broader applicability of CDH-6.
In this study, we reported that maternal serum CDH-6 levels measured in the early second trimester of pregnancy may serve as a significant biomarker for predicting PE that may develop in the subsequent weeks. In addition, higher CDH-6 levels were detected in early-onset cases, suggesting potential utility for early diagnosis of more severe cases of PE. When evaluated alongside perinatal outcomes, our findings suggest that CDH-6 may have not only predictive, but also prognostic value. Future studies with larger sample sizes and multicenter designs are needed to confirm these results and support clinical implementation.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
CSC and NG conceived and designed the study. SSU and YCU collected the data. ODU and SC performed data analysis and interpretation. NG drafted the manuscript. CSC, SC, SSU, ODU and YCU critically revised the manuscript for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was conducted in accordance with the Helsinki Declaration. The research protocol was approved by the Samsun University Non-Interventional Clinical Research Ethics Committee (Ethics Approval Number: GOKAEK-2024/2/15), and all participants provided signed informed consent forms.
Not applicable.
This research received no external funding.
The authors declare no conflicts of interest.
During the preparation of this work, the authors used ChatGPT (OpenAI) for assistance in improving the English language clarity and scientific expression of the manuscript. After using this tool, the authors carefully reviewed and edited the content and take full responsibility for the final version of the manuscript.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.