

 , Cuiyun Liu 2,*
, Cuiyun Liu 2,* , Yuanyuan Zhu 2,*
, Yuanyuan Zhu 2,*1 Department of Obstetrics and Gynecology, The First Affiliated Hospital of Soochow University, 215006 Suzhou, Jiangsu, China
2 Department of Obstetrics and Gynecology, Women’s Hospital of Nanjing Medical University (Nanjing Women and Children’s Healthcare Hospital), 210004 Nanjing, Jiangsu, China
Abstract
Postmenopausal bleeding (PMB) is a potential indicator of endometrial malignancy. Blind dilation and curettage (D&C) may fail to detect focal lesions, whereas office hysteroscopy (OH) could improve diagnostic accuracy. However, direct comparative evidence between the two methods remains limited. This study aimed to compare the diagnostic outcomes of OH and D&C in women with PMB and to evaluate their diagnostic accuracy, lesion detection rate, and the clinical application.
A retrospective analysis was conducted on the clinical data of 108 patients with PMB who visited the gynecology outpatient clinic of our hospital from August 2023 to May 2025. Of these, 56 patients underwent D&C, and 52 patients underwent OH. Using postoperative pathological results as the diagnostic gold standard, the detection of various types of uterine cavity lesions by the two examination methods was documented. The diagnostic accuracy, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of each method were calculated and compared. Additionally, the incidence of adverse events, pain scores, patient satisfaction, and specimen quality were analyzed.
According to the gold standard, there was no significant difference in the distribution of pathological diagnoses between the D&C and the OH groups (p > 0.05). Regarding diagnostic efficacy, the OH group exhibited higher diagnostic accuracy (94.23%), sensitivity (94.00%), and NPV (40.00%) compared with the D&C group (46.43%, 43.40%, and 9.09%, respectively). The overall incidence of adverse events was lower in the OH group (3.85%) than in the D&C group (17.86%) (p = 0.030). Furthermore, the OH group experienced less pain, higher patient satisfaction, and superior specimen quality (p < 0.05), with no significant difference in examination duration compared to the D&C group (p = 0.256).
OH demonstrates higher diagnostic accuracy, sensitivity, and specificity than D&C, along with a lower incidence of adverse events in the evaluation of PMB. Although the direct visualization of hysteroscopy is key to improving sampling for pathological analysis, gross diagnostic impressions alone are unreliable. Clinicians should rely on definitive pathological results before establishing a final diagnosis.
Keywords
- postmenopausal bleeding
- office hysteroscopy
- dilation and curettage
- diagnostic accuracy
- pathological examination
Postmenopausal bleeding (PMB) refers to any form of vaginal bleeding occurring in women after natural menopause. Approximately 4% to 11% of postmenopausal patients experience PMB, accounting for 5% of the gynecological outpatient visits [1]. As a common symptom in middle-aged and elderly women, PMB mainly originates from the cervix, vagina, and endometrium. The bleeding can last for more than 7 days, and the symptoms often recur [2]. PMB is clinically significant because it may serve as the clinical manifestation of various underlying pathological conditions, including benign lesions and malignant tumors, especially endometrial cancer [3]. Therefore, the diagnosis and evaluation of PMB are crucial. From a clinical epidemiological perspective, although the incidence of endometrial cancer in PMB patients varies to some extent due to factors such as region, race, and lifestyle, it generally remains at a relatively high level [4]. A systematic review and meta-analysis involving 40,790 patients from 129 independent studies indicated that approximately 90% of women with endometrial cancer exhibit PMB; among women with PMB, 9% are diagnosed with endometrial cancer [5]. Moreover, the prognosis of endometrial cancer is closely related to its clinical stage at diagnosis. Early diagnosis and prompt, standardized treatment lead to a 5-year survival rate exceeding 80%, whereas the 5-year survival rate for advanced-stage disease is less than 30% [6]. Thus, for patients with PMB, whether an early and accurate diagnosis can be achieved directly determines the selection of subsequent treatment plans and the ultimate prognostic outcome.
Dilation and curettage (D&C) is an invasive diagnostic technique that involves dilating the cervical canal and then using a curette to “blindly” scrape endometrial tissue for pathological examination, primarily used for evaluating endometrial lesions [7]. Its core principle is to obtain endometrial tissue samples through scraping, followed by pathological analysis to establish a definitive diagnosis. For a considerable period in the past, D&C had been widely applied in the diagnosis of patients with PMB and became a routine clinical diagnostic method due to its relatively simple operation and low cost [8]. However, since D&C is a “blind scraping” procedure, during the operation, doctors cannot directly observe the actual conditions within the patient’s uterine cavity and can only rely on experience and tactile feedback for the procedure. This often leads to a higher likelihood of missed and misdiagnosed cases during the diagnostic process [9]. Particularly for some focal lesions, D&C often fails to accurately obtain diseased tissue, leading to diagnostic discrepancies.
In recent years, with advancements in minimally invasive medical technologies, office hysteroscopy (OH), as a novel uterine cavity examination technique, has gradually been widely applied in the field of gynecological clinical diagnosis [10]. Compared with traditional D&C, OH offers a unique advantage of “direct visualization”. Through the lens of the hysteroscope, doctors can directly observe the overall condition within the patient’s uterine cavity, including the morphology, color, and thickness of the endometrium, as well as the presence of lesions such as polyps, fibroids, and adhesions in the uterine cavity, along with detailed information about the location, size, shape, and boundaries of these lesions [11]. This method of examination under direct visualization enables doctors to more precisely locate the lesion sites and directly perform biopsy sampling of suspicious lesion tissues during the examination, thereby significantly enhancing the accuracy and reliability of lesion detection [12]. Additionally, OH typically does not require general anesthesia. Patients remain conscious during the procedure, experience a short postoperative recovery time, and have a low incidence of complications. Moreover, the examination can be completed in an outpatient setting, improving patients’ healthcare experience and treatment compliance [13].
Despite the advantages of OH in diagnosing PMB, there remains a lack of direct comparative studies on its diagnostic efficacy compared with traditional D&C. When faced with PMB patients, clinicians still encounter some confusion and controversy regarding whether to choose OH or traditional D&C as the preferred diagnostic method, making it difficult to establish a unified clinical diagnosis and treatment protocol. Based on the aforementioned clinical context and research needs, this study selected 108 PMB patients who visited the gynecological outpatient clinic of our hospital from August 2023 to May 2025 as the research subjects and retrospectively analyzed their clinical data. The patients were divided into the D&C group and the OH group according to the different examination methods they received. This study meticulously recorded the detection rates of different types of uterine cavity lesions by the two examination methods and the incidence rates of adverse reactions associated with the two examination procedures to comprehensively evaluate their clinical application value. The aim was to clarify the strengths and weaknesses of OH and D&C in diagnosing PMB, providing clinicians with a reliable basis for selecting the most appropriate diagnostic approach for individual patients. This will improve diagnostic accuracy, reduce missed diagnoses, and ultimately enhance patient outcomes and quality of life.
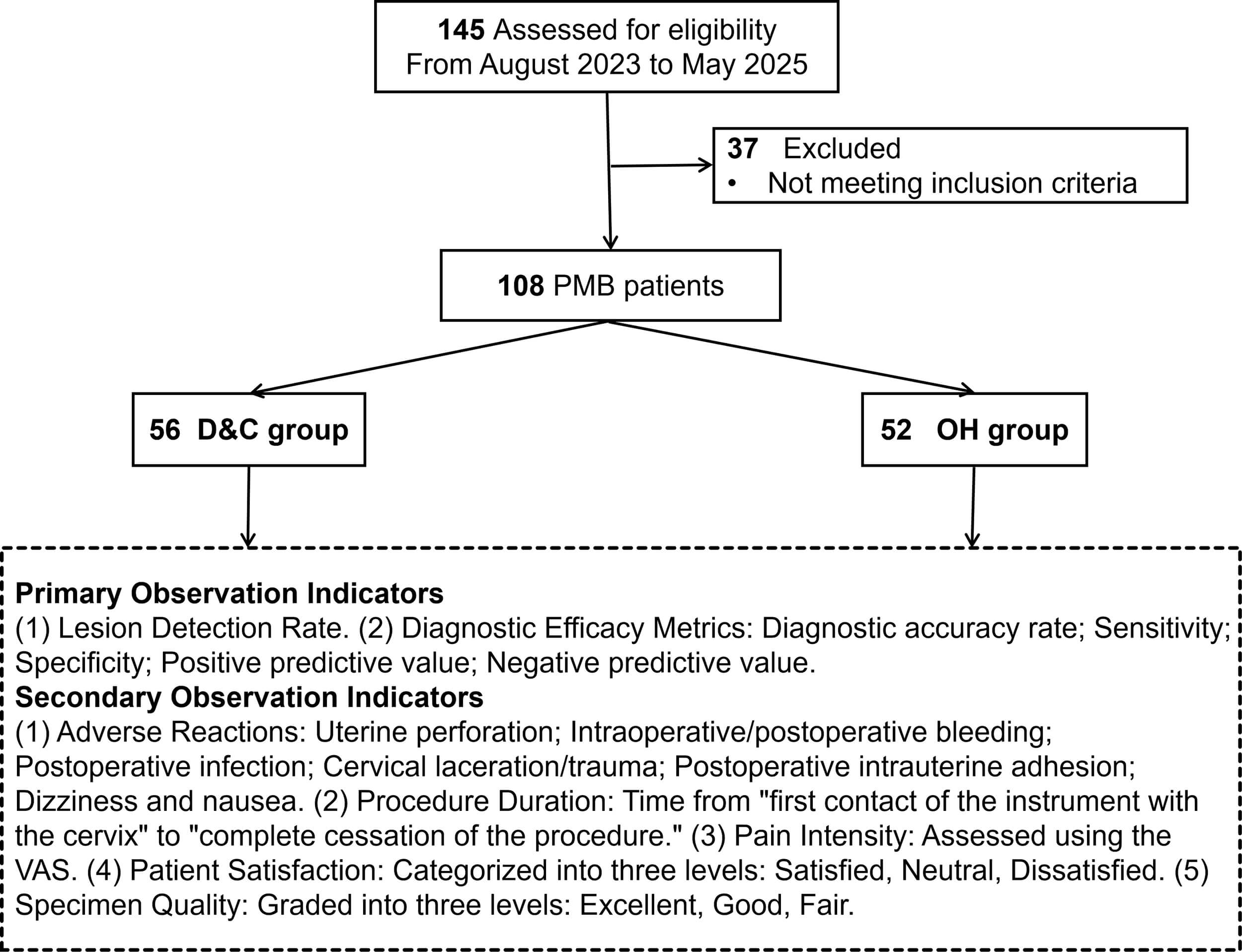
This study is a retrospective study. Data collection and analysis were conducted by researchers who were not involved in the treatment of the patients. Clinical data from 108 patients with PMB who visited the gynecological outpatient clinic of our hospital from August 2023 to May 2025 were selected. Among them, 56 patients underwent D&C, and 52 patients underwent OH. The choice of procedure (D&C vs. OH) was based on a combination of clinical assessment, patient preference, equipment availability, and the treating gynecologist’s judgment at the time of consultation. Postoperative histopathology served as the gold standard; detection rates for various uterine cavity lesions were compared between the two modalities. The study flowchart is presented in Fig. 1.
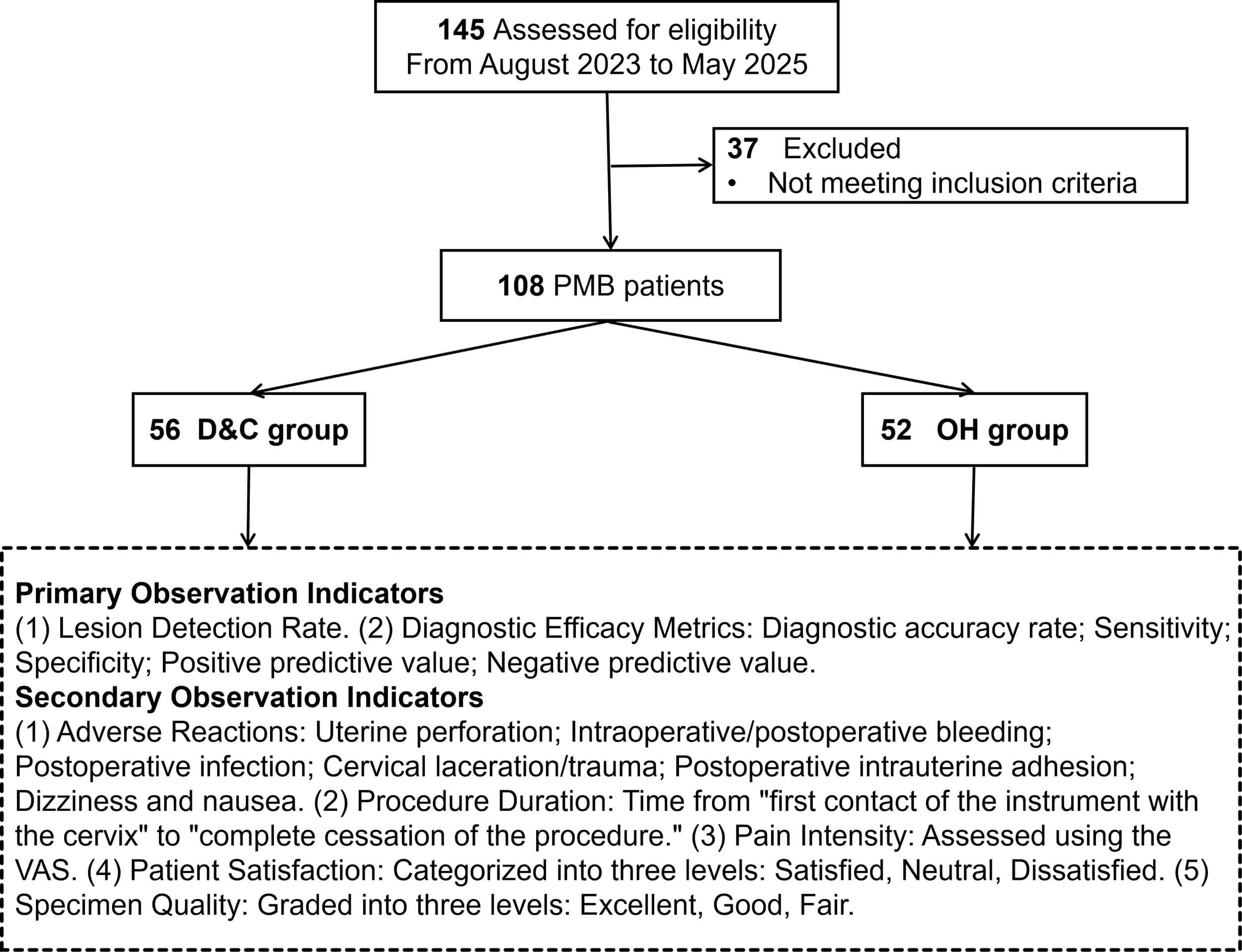 Fig. 1.
Fig. 1.
Research flowchart. PMB, postmenopausal bleeding; D&C, dilation and curettage; OH, office hysteroscopy.
(1) Recurrent vaginal bleeding occurring
(1) Previous diagnosis of endometrial cancer, endometrial atypical hyperplasia, or other gynecological malignancies; (2) Recent history of systemic or local vaginal use of estrogen, progestin, or other hormonal medications; (3) Severe mental disorders affecting the examination; (4) Abnormal coagulation function; (5) Dysfunction of vital organs; (6) Pregnancy-related bleeding.
This retrospective study included patients presenting to the gynecological
outpatient clinic of our hospital between August 2023 and May 2025. A search of
the electronic medical record system identified 108 eligible patients with PMB
who met the inclusion criteria. To assess the statistical power of the sample, we
conducted a post-hoc power analysis using G*Power software (version 3.1.9.7,
Heinrich-Heine-Universität Düsseldorf, Düsseldorf, North
Rhine-Westphalia, Germany). The parameters were set as follows: a two-sided
All examinations were performed by the same medical team. Prior to OH and D&C, patients were provided with detailed explanations of relevant precautions to alleviate their negative emotions and gain their trust and cooperation. Data extracted from the anesthesia and nursing records indicated that both the D&C and OH procedures were performed under local anesthesia. A paracervical block (using 1% lidocaine) was routinely administered to patients in both groups prior to the start of the procedure.
After voiding, patient was placed in the lithotomy position. The vulva and vagina were disinfected, and a sterile drape was placed. The examiner inserted one or two fingers of one hand into the vagina and used the other hand on the abdomen to palpate, thereby determining the size, position, and surrounding tissue conditions of the uterus. A disposable vaginal dilator provided by Anhui Huike Biological Engineering Technology Co., Ltd. (Hefei, Anhui, China) was used to expose the patient’s cervical os. The cervix and cervical canal were then disinfected again. The anterior or posterior lip of the cervix was grasped with forceps, and a uterine sound was used to determine the direction of the uterus and the depth of the uterine cavity. If the internal os of the cervix was too tight, a cervical dilator was used to dilate it until a small curette could be inserted. A piece of saline-soaked gauze was placed in the posterior vaginal fornix. A specially designed diagnostic curette was used to collect endometrial tissue from the inner wall of the uterine cavity, the fundus, and both lateral angles in an outside-to-inside manner. During the procedure, relevant hemostatic interventions were performed as necessary. For patients with significant uterine bleeding, scraping the endometrium clean was sufficient to achieve hemostasis. Specimens were fixed in 95% ethanol for pathological analysis. After the etiology was determined, targeted treatment was administered. Postoperatively, patients were advised to abstain from sexual activity for 30 days.
The patient was instructed to assume the lithotomy position. After routine vulvar and surrounding area disinfection, leg covers were placed, and sterile drapes were positioned over the abdomen and perineum. The vagina was dilated with a speculum to expose the cervix to the examiner’s view. The vagina and cervix were disinfected again, and then a probe was used to determine the depth of the uterine cavity. The cervix was further dilated until the internal diameter of the cervical os exceeded the outer sheath of the hysteroscope. Normal saline was infused to distend the uterine cavity. Under a Karl Storz hysteroscope (3.7 mm outer sheath, Karl Storz SE & Co. KG, Tuttlingen, Germany), a comprehensive examination of the uterine cavity endometrium, fundus, anterior and posterior walls of the uterine cavity, bilateral fallopian tube ostia, and cervical os was conducted. During the procedure, if focal lesions were identified, targeted biopsies were obtained using hysteroscopic biopsy forceps under direct visual guidance. In cases where no focal abnormality was seen, multiple systematic endometrial biopsies were taken from the anterior, posterior, and lateral uterine walls. All biopsy specimens were collected and sent for histopathological analysis. After the etiology was determined, targeted treatment was administered.
This examination relies on the gross morphological features of the scraped tissue and subsequent histopathological diagnosis for assessment [15, 16]. Endometrial hyperplasia: A large volume of scraped material is obtained, often in the form of diffuse, unevenly thickened endometrial fragments. Endometrial polyp: Pink, soft, cord-like tissue with a polypoid morphology is scraped out. Endometrial cancer: The scraped material appears grayish-white, crumbly like bean curd residue, or as fragile, necrotic tissue resembling rotten flesh, often accompanied by necrosis. Endometritis: During curettage, purulent discharge may flow from the uterine cavity, and the scraped material may have a foul odor or purulent exudate. Endometrial atrophy: A small amount of tissue is scraped, with the endometrium appearing extremely thin, pale, and fragmented into delicate pieces; or only a small amount of mucus is seen with almost no endometrial tissue.
This diagnosis was based on visual observation of the uterine cavity morphology, endometrial color, vascular patterns, and space-occupying lesions, as well as histopathological diagnosis [17]. Endometrial hyperplasia: The endometrium exhibits diffuse or focal thickening with an uneven surface, which may exhibit villous, polypoid, or finger-like projections. The number and distribution of glandular openings are increased and may be irregular. Endometrial polyp: Pedunculated or sessile neoplastic growths of various shapes are visible within the uterine cavity. The surface appears smooth, with a color similar to or more vividly red than the surrounding endometrium. The tissue is soft and may sway with the movement of the hysteroscope or irrigation fluid. Endometrial cancer: The affected area often presents as grayish-white, friable, irregular nodules or polypoid protrusions. The surface vessels are abnormally dilated, tortuous, and disorganized, with a tendency for contact bleeding. Endometritis: The endometrium is hyperemic and edematous, appearing scarlet red, with punctate or diffuse hemorrhagic spots. In severe cases, purulent discharge may accumulate within the uterine cavity. Endometrial atrophy: The endometrium is thin, pale, and smooth, with clear vascular patterns. The uterine cavity is easily distended, and punctate or patchy hemorrhagic spots may be visible.
For all patients, the “pathological report obtained from the first D&C or OH” was used as the preliminary gold standard [18]. All pathological diagnoses were based on the World Health Organization (WHO) 2020 classification system [19]. For hyperplasia, distinction was made between hyperplasia without atypia and atypical hyperplasia/Endometrial Intraepithelial Neoplasia (EIN). If the pathology indicates “benign endometrium”, “endometrial atrophy”, or “a small amount of fragmented endometrium”, and the patient undergoes a second OH or hysterectomy due to reasons such as persistent/recurrent bleeding or abnormal ultrasound findings, the gross pathology of the “second surgery/total resection specimen” is considered the final gold standard. The accuracy of the initial diagnosis was then retrospectively determined based on this final result. If the patient did not undergo further surgery after the initial diagnostic procedure, the initial pathological diagnosis was accepted as the definitive gold standard by default. This approach, while practical in a retrospective setting, may not capture instances where the initial D&C or OH biopsy missed a focal lesion, potentially leading to an overestimation of the diagnostic performance for both methods. However, this potential bias applies equally to both groups being compared.
(1) Detection of Lesions: The number of cases and detection rates of common uterine cavity lesions associated with PMB in the two groups were statistically analyzed. The types of lesions included the following five categories, covering common benign and malignant clinical conditions: endometrial atrophy, endometrial polyps, endometritis, endometrial hyperplasia, endometrial cancer, and absence of abnormalities.
(2) Diagnostic Efficacy Indicators: Based on the determination results of the
“gold standard”, true positives (TP), true negatives (TN), false positives (FP),
and false negatives (FN) were calculated. In this study, given the multiple
pathological categories (e.g., endometrial polyp, hyperplasia, cancer, etc.), we
adopted a per-lesion classification approach for calculating diagnostic metrics.
TP was defined as a case where the diagnostic method correctly identified both
the presence and the exact type of pathological lesion. FP was defined as a case
where a lesion was reported but not confirmed by the gold standard. FN was
defined as either a missed lesion (no lesion reported when one was present) or a
misclassified lesion (incorrect type identified). TN was defined as a correct
“no abnormality” diagnosis in patients with no pathological findings. The core
diagnostic efficacy indicators of the two groups were then compared: ①
Diagnostic Accuracy: This reflects the overall correctness of the diagnostic
method in distinguishing between “diseased” and “non-diseased” states. The
calculation formula is: (TP + TN) / Total number of cases
(1) Procedure-Related Adverse Reactions: All adverse reactions directly
associated with the procedure occurring intraoperatively or within 30 days
postoperatively were recorded. The classification and criteria for determination
are as follows: ① Uterine Perforation: Intraoperative exacerbation of
abdominal pain, unexpected increase in uterine cavity depth, or postoperative
imaging indicating disruption of the continuity of the uterine myometrium.
② Cervical Laceration/Trauma: Intraoperative visualization of cervical
mucosal tears and bleeding, or postoperative gynecological examination revealing
structural abnormalities. ③ Intraoperative/Postoperative Bleeding:
Intraoperative blood loss
(2) Procedure Duration: Defined as the time from “initial contact of the instrument with the cervix” to “complete conclusion of the procedure (including specimen collection)”, measured in minutes to compare the efficiency differences between the two procedures.
(3) Pain Score: The Visual Analog Scale (VAS) was used to assess the patient’s pain level, with a scoring range of 0–10: 0 indicates no pain, and 10 indicates the most severe pain. Patients marked their pain level 30 minutes post-procedure; lower scores indicated milder pain.
(4) Patient Satisfaction: Thirty minutes after the procedure, patients were interviewed to evaluate their overall healthcare experience using a 3-point Likert-type scale with the following categories: Satisfied (coded as 3), Neutral (coded as 2), and Unsatisfied (coded as 1) for the purpose of non-parametric statistical comparison. Satisfied: Perceived the procedure as smooth, with tolerable pain, and were satisfied with the examination process and result communication. Average: Perceived minor discomfort during the procedure but found it acceptable, with basic approval of the examination process. Unsatisfied: Perceived severe pain or significant adverse reactions during the procedure, and was dissatisfied with the examination process or communication services.
(5) Specimen Quality: Two experienced pathologists evaluated the quality of the submitted tissue specimens, categorized into three levels: Excellent (coded as 3), Good (coded as 2), and Fair (coded as 1) for the purpose of non-parametric statistical comparison. Excellent: Sufficient tissue volume obtained, with intact tissue structure allowing clear observation of endometrial glands, stroma, and lesion characteristics, meeting the requirements for pathological diagnosis. Good: Sufficient tissue volume obtained, with relatively intact tissue structure allowing identification of major lesion characteristics, without affecting pathological diagnosis. Fair: Insufficient tissue volume obtained or severe tissue fragmentation, with unclear key lesion characteristics, potentially compromising diagnostic accuracy.
All statistical analyses were performed using IBM SPSS Statistics v26.0 software
(IBM Corp., Armonk, NY, USA). Continuous variables were first assessed for
normality using the Shapiro-Wilk test. Normally distributed continuous variables
(e.g., age, body mass index [BMI]) were presented as “Mean
Table 1 compares the baseline data of PMB patients in the D&C group and the OH
group, including indicators such as age, BMI, marital status, family type,
underlying diseases, duration of menopause, number of pregnancies, number of
deliveries, and endometrial thickness before treatment. No statistically
significant differences were observed in any baseline indicators between the two
group (p
| Variables | Total (n = 108) | D&C Group (n = 56) | OH Group (n = 52) | Statistic | p | |
| Age (years), Mean |
56.24 |
55.45 |
57.10 |
t = 1.231 | 0.221 | |
| BMI (kg/m2), Mean |
23.99 |
23.66 |
24.35 |
t = 1.350 | 0.180 | |
| Marriage, n (%) | Married | 75 (69.44) | 37 (66.07) | 38 (73.08) | - | 0.904 |
| Unmarried | 9 (8.33) | 5 (8.93) | 4 (7.69) | |||
| Divorced | 14 (12.96) | 8 (14.29) | 6 (11.54) | |||
| Widowed | 10 (9.26) | 6 (10.71) | 4 (7.69) | |||
| Household type, n (%) | City | 40 (37.04) | 21 (37.50) | 19 (36.54) | 0.918 | |
| Rural | 68 (62.96) | 35 (62.50) | 33 (63.46) | |||
| Underlying diseases, n (%) | Hypertension | 13 (12.04) | 6 (10.71) | 7 (13.46) | 0.661 | |
| Hyperlipidemia | 14 (12.96) | 8 (14.29) | 6 (11.54) | 0.671 | ||
| Type 2 diabetes mellitus | 10 (9.26) | 4 (7.14) | 6 (11.54) | 0.649 | ||
| Osteoporosis | 8 (7.41) | 3 (5.36) | 5 (9.62) | 0.634 | ||
| Coronary heart disease | 9 (8.33) | 5 (8.93) | 4 (7.69) | 1.000 | ||
| Duration since menopause (years), Median (Q1, Q3) | 3.00 (2.75, 4.00) | 3.00 (3.00, 4.00) | 3.50 (2.00, 5.00) | Z = –0.674 | 0.500 | |
| Number of deliveries, Median (Q1, Q3) | 2.00 (1.00, 2.00) | 2.00 (1.00, 2.00) | 2.00 (1.00, 3.00) | Z = –0.297 | 0.766 | |
| Endometrial thickness (mm), Median (Q1, Q3) | 7.00 (6.00, 9.00) | 7.00 (6.00, 9.00) | 7.00 (6.00, 8.25) | Z = –0.380 | 0.704 | |
| Number of pregnancies, Median (Q1, Q3) | 2.00 (1.00, 3.00) | 2.00 (1.00, 3.00) | 2.00 (1.00, 3.00) | Z = –0.301 | 0.763 | |
Note: SD, standard deviation; BMI, body mass index; t, t-test;
Z, Mann-Whitney test;
Table 2 presents the distribution of final pathological diagnoses confirmed by
the gold standard among 108 PMB patients. The specific diagnoses included
endometrial atrophy (27 cases, 25.00%), endometrial polyps (22 cases, 20.37%),
endometrial hyperplasia (17 cases, 15.74%), endometritis (19 cases, 17.59%),
endometrial cancer (18 cases, 16.67%), and no abnormalities (5 cases, 4.63%).
Among the 56 patients in the D&C group, the above-mentioned lesions were
identified in 15, 11, 8, 9, 10, and 3 cases, respectively. In the OH group, which
comprised 52 patients, the corresponding numbers were 12, 11, 9, 10, 8, and 2
cases, respectively. No statistically significant difference was observed in the
distribution of pathological diagnosis types between the two groups
(
| Pathological diagnosis type | Total (n = 108) | D&C Group (n = 56) | OH Group (n = 52) | p | |
| Endometrial atrophy | 27 (25.00) | 15 (26.79) | 12 (23.08) | 0.720 | 0.982 |
| Endometrial polyp | 22 (20.37) | 11 (19.64) | 11 (21.15) | ||
| Endometrial hyperplasia | 17 (15.74) | 8 (14.29) | 9 (17.31) | ||
| Endometritis | 19 (17.59) | 9 (16.07) | 10 (19.23) | ||
| Endometrial cancer | 18 (16.67) | 10 (17.86) | 8 (15.38) | ||
| No abnormality | 5 (4.63) | 3 (5.36) | 2 (3.85) |
Note:
Table 3 presents the diagnostic results corresponding to different types of uterine cavity lesions confirmed by the gold standard among 56 patients in the D&C group. Among the 15 patients with endometrial atrophy in the D&C group, 9 were correctly diagnosed, 0 were misdiagnosed, and 6 were missed. Of the 11 patients with endometrial polyps, 5 were correctly diagnosed, 3 were misdiagnosed as endometrial hyperplasia, and 3 were missed. Among the 8 patients with endometrial hyperplasia, 3 were correctly diagnosed, 2 were misdiagnosed as endometrial polyps, and 3 were missed. Of the 9 patients with endometritis, 3 were correctly diagnosed, 0 were misdiagnosed, and 6 were missed. Among the 10 patients with endometrial cancer, 3 were correctly diagnosed, 4 were misdiagnosed as endometrial hyperplasia, and 3 were missed. For the 3 patients with no abnormalities, all were correctly diagnosed. Table 3 presents the diagnostic results for different types of uterine cavity lesions confirmed by the gold standard among 52 patients in the OH group. Among the 12 patients with endometrial atrophy in the OH group, all 12 were correctly diagnosed, with 0 misdiagnoses and 0 missed cases. Of the 11 patients with endometrial polyps, 10 were correctly diagnosed, 0 were misdiagnosed, and 1 was missed. Among the 9 patients with endometrial hyperplasia, all 9 were correctly diagnosed, with 0 misdiagnoses and 0 missed cases. Of the 10 patients with endometritis, 9 were correctly diagnosed, 0 were misdiagnosed, and 1 was missed. Among the 8 patients with endometrial cancer, 7 were correctly diagnosed, 1 was misdiagnosed as endometrial hyperplasia, and 0 were missed. For the 2 patients with no abnormalities, both 2 were correctly diagnosed.
| Pathological diagnosis type | Gold standard | D&C | ||
| Number of confirmed cases | Number of misdiagnosed cases | Number of missed diagnosis cases | ||
| Endometrial atrophy | 15 | 9 (60.00) | 0 (0.00) | 6 (40.00) |
| Endometrial polyp | 11 | 5 (45.45) | 3 (27.27) | 3 (27.27) |
| Endometrial hyperplasia | 8 | 3 (37.50) | 2 (25.00) | 3 (37.50) |
| Endometritis | 9 | 3 (33.33) | 0 (0.00) | 6 (66.67) |
| Endometrial cancer | 10 | 3 (30.00) | 4 (40.00) | 3 (30.00) |
| No abnormality | 3 | 3 (100.00) | 0 (0.00) | 0 (0.00) |
| Pathological diagnosis type | Gold standard | OH | ||
| Number of confirmed cases | Number of misdiagnosed cases | Number of missed diagnosis cases | ||
| Endometrial atrophy | 12 | 12 (100.00) | 0 (0.00) | 0 (0.00) |
| Endometrial polyp | 11 | 10 (90.91) | 0 (0.00) | 1 (9.09) |
| Endometrial hyperplasia | 9 | 9 (100.00) | 0 (0.00) | 0 (0.00) |
| Endometritis | 10 | 9 (90.00) | 0 (0.00) | 1 (10.00) |
| Endometrial cancer | 8 | 7 (87.50) | 1 (12.50) | 0 (0.00) |
| No abnormality | 2 | 2 (100.00) | 0 (0.00) | 0 (0.00) |
Table 4 presents the basic statistical data for diagnosis in the D&C group and the OH group. Among the 56 patients in the D&C group, 53 were confirmed to have the disease and 3 were disease-free according to the gold standard, corresponding to 23 TP, 3 TN, 0 FP, and 30 FN. In the OH group of 52 patients, 50 patients had the disease and 2 were disease-free by the gold standard, corresponding to 47 TP, 2 TN, 0 FP, and 3 FN.
| Group | Diseased | Disease-free | TP | TN | FP | FN |
| D&C Group (n = 56) | 53 (94.64) | 3 (5.36) | 23 (41.07) | 3 (5.36) | 0 (0.00) | 30 (53.57) |
| OH Group (n = 52) | 50 (96.15) | 2 (3.85) | 47 (90.38) | 2 (3.85) | 0 (0.00) | 3 (5.77) |
Note: TP, true positive; TN, true negative; FP, false positive; FN, false negative.
Table 5 compares the diagnostic efficacy indicators between the two groups based on the data in Table 4. The results show that the diagnostic accuracy, sensitivity, specificity, PPV, and NPV in the D&C group were 46.43%, 43.40%, 100.00%, 100.00%, and 9.09%, respectively. In the OH group, these indicators were 94.23%, 94.00%, 100.00%, 100.00%, and 40.00%, respectively.
| Diagnostic efficacy indicators | D&C Group (n = 56) | OH Group (n = 52) |
| Diagnostic accuracy rate | 46.43% (95% CI: 32.99%–60.26%) | 94.23% (95% CI: 84.05%–98.79%) |
| Sensitivity | 43.40% (95% CI: 29.84%–57.72%) | 94.00% (95% CI: 83.45%–98.75%) |
| Specificity | 100.00% (95% CI: 29.24%–100.00%) | 100.00% (95% CI: 15.81%–100.00%) |
| PPV | 100.00% (95% CI: 85.18%–100.00%) | 100.00% (95% CI: 92.45%–100.00%) |
| NPV | 9.09% (95% CI: 1.92%–24.33%) | 40.00% (95% CI: 5.27%–85.34%) |
Note, PPV, positive predictive value; NPV, negative predictive value.
Table 6 compares the occurrence of procedure-related adverse reactions between patients in the D&C group and the OH group. In the D&C group, there was 1 case of uterine perforation, 4 cases of intraoperative/postoperative bleeding, 3 cases of infection, 1 case of cervical laceration/trauma, and 1 case of post-procedure intrauterine adhesion. There were no cases of dizziness or nausea, resulting in a total adverse reaction rate of 17.86%. In the OH group, there was only 1 case of infection and 1 case of dizziness/nausea. No cases of uterine perforation, bleeding, cervical laceration/trauma, or post-procedure intrauterine adhesion were observed, leading to a total adverse reaction rate of 3.85%. The difference in adverse reaction rates was statistically significant (p = 0.030), indicating a significantly lower rate in the OH group compared to the D&C group.
| Types of adverse events | D&C Group (n = 56) | OH Group (n = 52) | p |
| Uterine perforation | 1 (1.79) | 0 (0.00) | |
| Intraoperative/postoperative bleeding | 4 (7.14) | 0 (0.00) | |
| Postoperative infection | 3 (5.36) | 1 (1.92) | |
| Cervical laceration/trauma | 1 (1.79) | 0 (0.00) | |
| Postoperative intrauterine adhesion | 1 (1.79) | 0 (0.00) | |
| Dizziness and nausea | 0 (0.00) | 1 (1.92) | |
| Overall adverse reactions | 10 (17.86) | 2 (3.85) | 0.030 |
Note: -, Fisher exact.
Table 7 compares the examination operation times among 108 PMB patients. The overall operation time for the entire cohort was 13.50 (11.00, 18.00) minutes. In the D&C group, the operation time was 13.00 (10.75, 16.00) minutes, while in the OH group, it was 15.00 (11.00, 18.00) minutes. No statistically significant difference was observed between the two groups (Z = –1.135; p = 0.256).
| Variables | Check the operation time |
| Total (n = 108) | 13.50 (11.00, 18.00) |
| D&C Group (n = 56) | 13.00 (10.75, 16.00) |
| OH Group (n = 52) | 15.00 (11.00, 18.00) |
| Z | –1.135 |
| p | 0.256 |
Note: Z, Mann-Whitney test.
Table 8 compares the pain VAS scores among 108 PMB patients. The overall VAS
score for the entire cohort was 5.00 (3.75, 7.00) points. In the D&C group, the
VAS score was 6.50 (5.00, 7.00) points, while in the OH group, it was 4.00 (2.00,
5.00) points. A statistically significant difference in pain VAS scores was
observed between the two groups (Z = –5.922; p
| Variables | VAS |
| Total (n = 108) | 5.00 (3.75, 7.00) |
| D&C Group (n = 56) | 6.50 (5.00, 7.00) |
| OH Group (n = 52) | 4.00 (2.00, 5.00) |
| Z | –5.922 |
| p |
Note: Z, Mann-Whitney test. VAS, Visual Analog Scale.
Table 9 compares post-operative satisfaction levels between the D&C group and the OH group. The median satisfaction score in the D&C group was 3.00 (2.00, 3.00), while in the OH group it was 3.00 (3.00, 3.00). A statistically significant difference was observed in the distribution of satisfaction (p = 0.002), with patients in the OH group demonstrating significantly higher satisfaction compared to those in the D&C group.
| Variables | Satisfaction |
| Total (n = 108) | 3.00 (3.00, 3.00) |
| D&C Group (n = 56) | 3.00 (2.00, 3.00) |
| OH Group (n = 52) | 3.00 (3.00, 3.00) |
| Z | –3.154 |
| p | 0.002 |
Note: Z, Mann-Whitney test.
Table 10 compares the quality of specimens submitted for pathological
examination between the D&C group and the OH group. The median specimen quality
score in the D&C group was 3.00 (2.00, 3.00), while in the OH group it was 3.00
(3.00, 3.00). A statistically significant difference was observed in the
distribution of specimen quality between groups (p
| Variables | Specimen quality |
| Total (n = 108) | 3.00 (3.00, 3.00) |
| D&C Group (n = 56) | 3.00 (2.00, 3.00) |
| OH Group (n = 52) | 3.00 (3.00, 3.00) |
| Z | –4.094 |
| p |
Note: Z, Mann-Whitney test.
PMB serves as a crucial warning signal for malignant endometrial lesions, and its accurate diagnosis directly influences treatment plans and the long-term prognosis of patients. In clinical practice, although traditional D&C has long been a routine method for diagnosing PMB, the issue of missed diagnosis of focal lesions due to its “blind scraping” nature has not been effectively resolved. OH, with its technical advantages of direct visualization and targeted biopsy, offers a new approach to overcoming this diagnostic bottleneck [20]. This study retrospectively analyzed clinical data of 108 PMB patients, using postoperative pathological examination as the “gold standard” to systematically compare the diagnostic efficacy, safety, and patient experience-related indicators between OH and D&C. The results demonstrated that OH significantly outperformed D&C in core efficacy indicators such as diagnostic accuracy, sensitivity, and specificity. It is critical to emphasize that this superior performance stems from OH’s ability to provide direct visualization, which enables precise lesion localization and targeted biopsy, thereby yielding specimens of higher diagnostic quality for pathological examination. The final diagnosis in all cases relied on histopathological confirmation, not on visual inspection alone. Moreover, OH was associated with a lower incidence of adverse reactions, higher patient satisfaction, and superior quality of specimens submitted for examination.
The most notable technical advantage of OH lies in its “direct visualization” characteristic, which fundamentally addresses the inherent flaw of the “blind scraping” procedure in D&C [21]. In this study, the diagnostic accuracy rates of OH for endometrial atrophy, hyperplasia, polyps, and other lesions all exceeded 90%, with the diagnostic accuracy rate for endometrial cancer reaching 87.5% and the missed diagnosis rate being less than 10%. In contrast, the diagnostic accuracy rates of D&C for most lesions were less than 60%, with the diagnostic accuracy rate for endometritis being only 33.33% and the highest missed diagnosis rate reaching 66.67% (for endometritis). The core reason for these discrepancies is that OH, through a 2.9 mm 0° hysteroscope lens, enables comprehensive observation of the morphological features, color, vascular patterns, and details of space-occupying lesions in the endometrial cavity under a clear visualization provided by distension with 5% glucose solution [22]. For example, endometrial hyperplasia manifests as diffuse or focal thickening, with an uneven surface, an increased number of glandular openings, and abnormal distribution. Endometrial cancer, on the other hand, presents as grayish-white, friable, irregular nodules or polypoid protrusions, with abnormally dilated and tortuous surface vessels [23]. These visual features allow physicians to directly identify the location, size, boundaries, and nature of the lesions, avoiding the “blind operation” in D&C that relies on “tactile sensation and experience”.
Furthermore, this study acknowledges the role of pre-operative transvaginal ultrasound in evaluating endometrial pathologies. Although all patients underwent ultrasound examination with measurement of endometrial thickness, retrospective analysis suggests that for patients whose pre-operative ultrasound indicated possible focal lesions, traditional D&C is more prone to missed diagnosis due to its “blind curettage” nature. In contrast, the direct visualization advantage of OH enables precise localization and targeted biopsy of such focal lesions, which may be a key factor contributing to the significantly higher diagnostic accuracy of the OH group compared to the D&C group in this study. Future research could be designed prospectively to systematically compare the diagnostic performance of OH and D&C in patients pre-classified by ultrasound into focal versus diffuse endometrial pathologies.
From an anatomical perspective, the uterine cavity is shaped like an inverted triangle. Endometrial tissues in areas such as the uterine horns and fundus are prone to being missed by the curette during D&C procedures. In contrast, OH can flexibly adjust the viewing angle through its lens, providing clear visualization of all regions within the uterine cavity. It can even detect tiny polyps or focal hyperplasia with diameters smaller than 5 mm [24]. Kaveh et al. [25] also demonstrated that OH combined with biopsy is the gold standard for identifying malignant changes in endometrial polyps, offering advantages in identifying minute polyps and focal hyperplasia. In this study, the diagnostic accuracy rate for “no abnormality” cases in the OH group reached 100%, with a false-positive rate of only 1.92% (1/52). This supports that direct visualization imaging technology can effectively distinguish between “physiological atrophy” and “pathological lesions”, reducing misjudgments of normal endometrial tissues. Among the eight patients with endometrial cancer in the OH group, seven were correctly diagnosed, while one was misdiagnosed as having endometrial hyperplasia. This misdiagnosis may have been due to atypical lesion morphology, such as ambiguous glandular atypia and inconspicuous stromal infiltration. Nappi et al. [26] found that some patients may have coexisting atypical endometrial hyperplasia and endometrial cancer. In their study, 37.5% of patients with atypical endometrial hyperplasia were postoperatively diagnosed with cancer. Such lesions may exhibit similar morphological features under OH, such as dense glandular structures and disorganized architecture, making it difficult to distinguish them solely through biopsy. A definitive diagnosis often requires postoperative total uterine pathology. Additionally, OH allows for targeted biopsy of suspicious lesions during the examination, as opposed to the extensive scraping in D&C. This not only improves the efficiency of obtaining diseased tissue but also avoids interference from normal tissue in pathological diagnosis [27]. In this study, the “excellent specimen rate” in the OH group reached 92.31% (48/52), significantly higher than the 58.93% (33/56) in the D&C group, directly reflecting the advantage of targeted sampling. The study by Di Spiezio Sardo et al. [28] confirmed that endometrial biopsy under direct OH visualization significantly improves sample adequacy (RR 1.13, 95% CI 1.10–1.17) compared to blind sampling and reduces the risk of missing endometrial cancer or hyperplasia (RR 0.16, 95% CI 0.03–0.92).
Diagnostic efficacy is a core indicator for evaluating the clinical value of examination techniques. The OH group exhibited significantly higher diagnostic accuracy (94.23%), sensitivity (94.00%), and NPV (40.00%) compared to the D&C group (46.43%, 43.40%, and 9.09%, respectively). It should be noted that in this study, both missed diagnoses and misclassifications of lesion type were grouped as FN for the purpose of calculating diagnostic accuracy metrics. This stringent classification was chosen to reflect a clinically conservative approach, as misclassifying a malignant lesion carries significant clinical consequences similar to a missed diagnosis. While this approach may lead to a more pronounced underestimation of sensitivity and NPV for D&C, particularly given its tendency for misclassification, it underscores the clinical superiority of OH in providing accurate lesion-specific diagnoses. Future studies may consider separate analyses for missed vs. misclassified lesions to further delineate diagnostic performance.
From a clinical perspective, high sensitivity indicates that OH can more effectively identify patients who are “truly diseased”, thereby reducing the rate of missed diagnoses. In this study, the OH group had only 3 FN cases (5.77%), whereas the D&C group had 30 FN cases (53.57%). Among the 30 FN cases in the D&C group, subsequent investigation revealed that the initial ‘blind’ procedure had completely missed 3 cases of endometrial cancer and 3 cases of endometrial hyperplasia. Furthermore, D&C misclassified an additional 4 cases of cancer as hyperplasia. These findings highlight a significant limitation of D&C, as its failure to detect or correctly classify these premalignant and malignant lesions can lead to critical delays in diagnosis and treatment. The prognosis of endometrial cancer is closely related to its diagnostic stage, and the high sensitivity of OH can assist clinicians in promptly capturing signals of malignant lesions, thus avoiding delays in treatment due to missed diagnoses. Meanwhile, the high specificity and high PPV of OH can reduce the risk of overdiagnosis and overtreatment. It is noteworthy that although the NPV in the OH group (40.00%) was higher than that in the D&C group (9.09%), there is still room for improvement. This relatively low NPV is primarily attributable to the high prevalence of endometrial pathology in the studied PMB population. According to the Bayesian principles of diagnostic testing, NPV is inversely influenced by disease prevalence; when prevalence is very high, the number of true negative cases is inherently small, which mathematically limits the NPV value. In clinical terms, this means that in a high-risk population such as symptomatic PMB patients, a negative test result should still be interpreted with caution and may warrant further investigation if clinical suspicion persists. This may be related to the extremely low proportion of “no abnormality” cases among patients with PMB. When disease prevalence is excessively high, the NPV is susceptible to influence. In clinical practice, it is necessary to combine OH with other diagnostic modalities, such as ultrasonography, to make comprehensive judgments and further optimize the diagnostic process.
In addition to diagnostic accuracy, safety and patient tolerability are also key for clinical acceptance [29, 30]. This study revealed a significantly lower overall adverse reaction rate in the OH group (3.85%) compared to the D&C group (17.86%). Moreover, no severe complications, such as uterine perforation, cervical laceration, or post-operative intrauterine adhesions, occurred in the OH group. From an operational perspective, D&C requires dilation of the cervical os using a cervical dilator to a size that allows the curette to enter, a process that is prone to causing cervical mucosal tears. Additionally, its blind scraping may lead to uterine perforation due to improper force application or abnormal uterine positioning. In contrast, OH only necessitates cervical dilation slightly larger than the outer sheath of the hysteroscope, which is significantly less extensive than that required for D&C. Furthermore, the direct visualization during OH enables real-time observation of the anatomical relationships between the cervical canal and uterine cavity, avoiding blind force application and fundamentally reducing the risk of mechanical injury [31]. OH also demonstrates significant advantages in hemorrhage and infection control. The incidence of intraoperative/postoperative bleeding in the D&C group reached 7.14% (4/56), primarily due to excessive endometrial trauma or vascular injury caused by blind scraping [32]. In contrast, targeted biopsy in OH results in only minimal localized trauma, and the continuous irrigation of the uterine cavity with distension fluid during the procedure reduces both bleeding and infection risks [33]. In this study, no intraoperative/postoperative bleeding occurred in the OH group, and the infection rate was only 1.92% (1/52), lower than the 5.36% (3/56) in the D&C group. Additionally, patients in the OH group reported a median pain VAS score of 4.00 (interquartile range: 2.00, 5.00), significantly lower than the 6.50 (5.00, 7.00) in the D&C group. Patient satisfaction reached 94.23% (49/52) in the OH group, far exceeding the 71.43% (40/56) in the D&C group. The minimally invasive, low-pain, and convenient nature of OH significantly enhances patient compliance with diagnosis and treatment, particularly among elderly patients with PMB, reducing their fear of invasive procedures and facilitating the clinical goal of “early diagnosis and early treatment” [34, 35, 36]. Furthermore, D&C lacks real-time assessment of intrauterine conditions. If suspected malignant lesions are identified during the procedure, the operation must be terminated, and further examinations scheduled, prolonging the diagnostic and therapeutic process. In contrast, OH allows for “diagnostic treatment” during the examination, such as the removal of small polyps or the separation of mild adhesions, enabling one-stop diagnosis and treatment and shortening patients’ healthcare journeys [37, 38].
Although OH demonstrates significant advantages in the diagnosis of PMB, its clinical application still faces the following limitations that require continuous improvement in practice. First, the equipment and technical thresholds are relatively high. OH requires specialized OH equipment and well-trained operators. The cost of equipment acquisition is substantial, and physicians require systematic training to independently perform the procedure, which may hinder its widespread adoption in primary healthcare institutions. In the future, a “tiered diagnosis and treatment” model could be implemented, wherein basic OH equipment is deployed in county-level hospitals, accompanied by enhanced technical training for primary care physicians to gradually expand the application of OH. Second, there are risks associated with distension media. OH relies on distension media to expand the uterine cavity. Excessive distension pressure or prolonged procedural duration may lead to excessive absorption of distension fluid, potentially causing water intoxication, particularly in elderly PMB patients with concurrent cardiac or renal dysfunction, where the risk is heightened [39]. In clinical practice, it is essential to strictly control distension pressure and procedural duration while closely monitoring patients’ vital signs to promptly identify and manage complications related to distension media [40]. Third, the diagnosis of certain special cases still requires adjunctive modalities. Although OH provides clear visualization of intrauterine lesions, its diagnostic value for cervical canal or myometrial pathologies is limited. A comprehensive assessment incorporating cervical cytology, human papillomavirus (HPV) testing, or ultrasonography is necessary for accurate diagnosis [41].
This study is a retrospective analysis, with data obtained from previous medical records, which may introduce selection bias. For instance, patients with more complex conditions might have been more inclined to opt for OH examination, while those with simpler conditions might have opted for D&C. Although no statistically significant differences in baseline characteristics were observed between the two groups in this study, a hidden bias cannot be entirely ruled out. Furthermore, this study has a retrospective, non-paired design. All patients underwent only one of the two examinations (OH or D&C), rather than a direct, within-patient comparison. This design may introduce residual confounding, as factors such as the complexity of the patient’s condition, physician preference, or the clinical decision-making process may have influenced the choice of diagnostic method, potentially affecting the accuracy of the performance comparison between OH and D&C. Future prospective studies, particularly those employing a randomized controlled trial design or a paired comparison where both methods are used in the same patient, would provide a more rigorous evaluation of their diagnostic efficacy. Third, regarding the gold standard, for patients without subsequent surgical confirmation, the initial pathological diagnosis was used as the definitive endpoint. This methodological constraint, common in diagnostic studies where invasive follow-up is not universally justified, carries the risk of verification bias. If the initial procedure (either D&C or OH) missed a significant lesion that remained undetected because no further surgery was performed, the diagnostic accuracy for that case would be incorrectly counted as correct. This could lead to an overestimation of the performance for both techniques. Nevertheless, this potential bias is non-differential, as it affected both study groups similarly, and the primary comparative analysis between OH and D&C within this framework remains valid. Future prospective studies with planned, uniform confirmatory surgery (e.g., hysterectomy) for all enrolled PMB patients would provide a more robust gold standard.
Moreover, retrospective studies lack standardized control over the details of examination procedures, which may affect the comparability of results. Additionally, this study included only 108 patients from a single hospital, resulting in a relatively small sample size that may limit the generalizability of the findings. Furthermore, multiple secondary endpoints were analyzed without statistical adjustment for multiplicity. Therefore, the reported p-values for these secondary outcomes should be interpreted cautiously. Variations in OH equipment and operator expertise across different regions and hospitals may influence the diagnostic performance of OH, necessitating further validation through multicenter, large-sample studies. Furthermore, subgroup analyses could be conducted for different populations, such as elderly patients, those with underlying medical conditions, or patients with a longer duration of menopause, to clarify the advantages and applicability of OH in specific subgroups and develop individualized diagnostic protocols.
Through a systematic comparison of the diagnostic performance OH and D&C in the diagnosis of PMB patients, this study confirms that OH, with its technical advantages of direct visualization, targeted sampling, and a minimally invasive profile, significantly outperforms D&C in terms of diagnostic efficacy, safety, and patient experience. The high accuracy and sensitivity of OH effectively reduce the rates of missed and misdiagnosed cases, providing a reliable basis for the early diagnosis and precise treatment of PMB patients. However, it is essential to underline that the final diagnosis must be based on histopathological examination. Gross diagnostic impressions obtained through direct visualization alone are insufficient and potentially misleading. All clinicians should await pathology results before making definitive clinical decisions. Its low incidence of adverse reactions and high patient satisfaction enhance treatment adherence, thereby facilitating the optimization of PMB diagnostic and therapeutic strategies.
The data that support the findings of this study are available from the corresponding authors, upon reasonable request.
XZ: Developed and planned the study, performed experiments, and interpreted results; Edited and refined the manuscript with a focus on critical intellectual contributions. YZ, CL: Participated in collecting, assessing, and interpreting the date; Made significant contributions to date interpretation and manuscript preparation. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study was approved by the Ethics Committee of The First Affiliated Hospital of Soochow University (Approval No.: 2025-1052). The study was carried out in accordance with the guidelines of the Declaration of Helsinki. We secured a signed informed consent form from every participant.
Not applicable.
This research received no external funding.
The authors declare no conflicts of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.