

 , Fang Wang 1, Shanshan Zhu 1, BenZhi Dou 1,*
, Fang Wang 1, Shanshan Zhu 1, BenZhi Dou 1,*
1 Department of Obstetrics and Gynecology, Anhui No.2 Provincial People’s Hospital, 230012 Hefei, Anhui, China
Abstract
Neonatal hypoglycemia (NH) is a common metabolic complication among infants born to mothers with gestational diabetes mellitus (GDM) and may adversely affect neurodevelopment. Delivery mode, particularly cesarean section (CS), has been proposed as a potential risk factor for NH; however, existing evidence remains inconsistent. This study aimed to evaluate the association between delivery mode and the risk of NH in pregnancies complicated by GDM.
This retrospective study included women with GDM who delivered at ≥35 weeks of gestation at Anhui No.2 Provincial People’s Hospital between January 2024 and December 2024. NH was defined as any blood glucose measurement <2.6 mmol/L within the first 24 hours of life, consistent with American Academy of Pediatrics guidelines. Maternal and neonatal characteristics were compared between the NH and non-NH groups. Independent risk factors for NH were identified using multivariable logistic regression. The predictive performance of CS for NH was evaluated by calculating sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV).
Among 201 women with GDM who met the inclusion criteria, 44 neonates (21.89%) developed NH. The rate of CS was significantly higher in the NH group compared with the non-NH group (81.82% vs. 39.49%, p < 0.001). After adjustment for potential confounders, CS remained an independent risk factor for NH (adjusted odds ratio [OR] = 4.48, 95% confidence interval [CI]: 1.56–12.87; p = 0.005). CS was associated with a sensitivity of 81.8%, a specificity of 60.5%, a PPV of 36.7%, and an NPV of 92.2% for NH.
CS independently increases the risk of NH in infants born to mothers with GDM. Delivery mode should be considered in perinatal management strategies to improve early identification and prevention of NH.
Keywords
- gestational diabetes mellitus
- neonatal hypoglycemia
- cesarean section
- delivery mode
- risk factor
Gestational diabetes mellitus (GDM) is the most prevalent metabolic disorder during pregnancy, affecting approximately 7%–14% of pregnancies worldwide [1, 2]. In mainland China, a systematic review and meta-analysis of studies that used the IADPSG criteria reported a pooled GDM prevalence of 14.8%. This rate exceeds that reported in many Western populations and may reflect genetic susceptibility, dietary patterns, and increasing maternal age [3]. GDM not only increases the risk for pregnant women, such as gestational hypertension and elevated cesarean section (CS) rates, but also contributes to adverse neonatal outcomes, including unstable blood glucose, macrosomia, and respiratory distress syndrome [4, 5]. Neonatal hypoglycemia (NH) is one of the most common metabolic disturbances in the early neonatal period, and its incidence is markedly higher among infants with established risk factors such as maternal diabetes, growth restriction, or prematurity [6]. In this study, NH was defined as any blood glucose concentration below 2.6 mmol/L within the first 24 hours of life, consistent with widely used operational thresholds for at-risk late preterm and term infants [7]. If not promptly identified and managed, neonatal hypoglycemia can result in acute brain injury that predominantly affects the posterior cerebral regions, as demonstrated by magnetic resonance imaging studies [8, 9]. Long-term follow-up neuroimaging study has revealed that NH is associated with smaller volumes of deep gray matter structures, including the caudate nucleus and thalamus, which persist into mid-childhood [8]. Consequently, timely identification of risk factors is crucial for prevention and early intervention.
Beyond its occurrence, NH exhibits a dose-dependent relationship with subsequent
neurodevelopmental outcomes. Data from the Children with Hypoglycemia and Their
Later Development (CHYLD) prospective cohort demonstrated that more severe NH
(blood glucose
Delivery mode represents an important perinatal factor that may influence neonatal metabolic adaptation, particularly in pregnancies complicated by GDM. CS can mitigate certain obstetric risks, such as dystocia and severe perineal trauma in cases of suspected macrosomia; however, it may also delay the onset of breastfeeding, alter early neonatal stress responses, and increase the likelihood of maternal postoperative complications and impaired early mother–infant contact [13]. In contrast, vaginal delivery (VD) is accompanied by labor-associated hormonal surges and catecholamine release, which may facilitate neonatal glucose homeostasis. These physiological differences have led to ongoing debate regarding whether delivery mode independently contributes to NH risk in infants born to mothers with GDM.
The approach to GDM management may also modify the relationship between maternal diabetes and neonatal outcomes. A recent systematic review and meta-analysis of 18 randomized controlled trials demonstrated that lifestyle intervention, including diet and physical activity, reduced the risk of NH by 27% (relative risk [RR] = 0.73, 95% confidence interval [CI]: 0.54–0.98), with the greatest effect when intervention was initiated before the third-trimester [14]. Furthermore, pharmacologic management with metformin, compared with insulin, has been associated with a 35% lower rate of NH (RR = 0.65, 95% CI: 0.52–0.81), although the underlying mechanisms remain under investigation [15]. These findings suggest that both lifestyle and pharmacologic interventions may attenuate neonatal metabolic risk in pregnancies complicated by GDM.
Several observational studies have examined factors associated with NH in pregnancies complicated by GDM, suggesting that maternal glycemic control, a history of uterine scarring, and delivery mode may influence neonatal glucose instability [16, 17]. In particular, more stringent management of maternal blood glucose has been associated with a lower incidence of NH in some cohorts, implying a potential protective effect of optimized glycemic control [18]. However, these findings are often limited by heterogeneous study populations, variable definitions and timing of hypoglycemia assessment, and incomplete adjustment for key confounders, including maternal body mass index (BMI), diabetes treatment modality (dietary management versus insulin or oral hypoglycemic agents), and the timing of glucose measurements. Previous observational study has suggested that CS may be associated with NH and related early clinical consequences, particularly in the context of adverse maternal or perinatal metabolic conditions [19]. Moreover, the distinction between diet-controlled and pharmacologically treated GDM, both of which may independently influence neonatal glucose homeostasis, has often been overlooked. These limitations underscore the need for more rigorous evaluation of delivery mode as a potential determinant of NH in well-characterized GDM cohorts.
Recent systematic reviews and meta-analyses have further elucidated risk factors for NH in pregnancies complicated by GDM. A 2024 meta-analysis by Wang et al. [20], synthesizing 12 case-control studies encompassing 991 neonates with NH and 4388 controls, found that CS was associated with nearly twofold higher odds of NH (odds ratio [OR] = 1.90, 95% CI: 1.23–2.92). Other identified risk factors included gestational diabetes itself (OR = 1.65), gestational hypertension (OR = 2.79), and small-for-gestational-age status (OR = 2.88). These findings indicate that both maternal characteristics and perinatal factors contribute to neonatal glucose instability.
Despite these robust meta-analytic findings, several knowledge gaps remain. Most previous studies included mixed populations (GDM and non-GDM) or did not comprehensively adjust for key confounders such as uterine scarring, maternal age, gestational age, maternal BMI, and gravidity, factors that are particularly relevant in Asian cohorts with high CS rates. In China, the CS rate remains notably elevated. A recent national analysis of more than 7.6 million births reported an overall rate of 44.5% in 2020, with rates of about 40% even among low-risk term singleton vertex deliveries [21]. Furthermore, few studies have quantified the predictive performance of delivery mode as a standalone risk factor in well-characterized GDM populations. Therefore, in a retrospective study of 201 women with GDM from a tertiary center in China, the present study aimed to: (1) determine whether CS remains independently associated with NH after adjustment for key confounders, and (2) assess its clinical predictive value using sensitivity, specificity, PPV, and NPV.
This retrospective study included clinical records of all singleton pregnancies complicate by GDM that met the inclusion criteria and delivered in the Department of Obstetrics of Anhui No.2 Provincial People’s Hospital from January 2024 to December 2024. The study was approved by the Ethics Committee of Anhui No.2 Provincial People’s Hospital (Approval No: (R) 2025-107) and was conducted in accordance with the Declaration of Helsinki. The ethics committee waived the requirement for informed consent due to the retrospective design and use of anonymize data.
Inclusion criteria were as follows: (1) diagnosis of GDM based on the criteria
recommended by the International Federation of Gynecology and Obstetrics (FIGO),
confirmed by a 75 g oral glucose tolerance test (OGTT) [22]; (2) singleton
pregnancy; and (3) gestational age
Exclusion criteria were as follows: (1) pre-existing diagnosis of type 1 or type 2 diabetes before pregnancy; (2) multiple pregnancy; (3) severe comorbid conditions, such as cardiac, hepatic, or renal disorders; (4) known severe structural or genetic abnormalities in the fetus; and (5) severely incomplete clinical data.
The following maternal and infant data were obtained from the hospital electronic medical record system:
(1) Maternal general characteristics: age, pre-pregnancy height, weight, and BMI (BMI = weight (kg) / height (m)2).
(2) Obstetric-related information: gravidity, parity, gestational age (days), delivery mode (vaginal or cesarean), presence of uterine scar, and other pregnancy complications. Results of the 75 g OGTT. including fasting, 1-hour, and 2-hour plasma glucose levels, were extracted directly from the electronic medical record system.
(3) Laboratory tests: fasting blood glucose levels at GDM diagnosis.
(4) Neonatal information: gender, birth weight (grams), presence of macrosomia
(birth weight
All patients with GDM were managed according to FIGO and American Diabetes
Association (ADA) guidelines. Initial treatment consisted of medical nutrition
therapy and physical activity. Pharmacologic therapy (metformin or insulin) was
initiated if glycemic targets were not achieved within 1–2 weeks [23, 24].
Glycemic targets were defined as follows: fasting plasma glucose
NH was defined based on widely applied operational thresholds in previous
neonatal studies. Any blood glucose value
Delivery mode: categorized as VD, including spontaneous VD and forceps or vacuum-assisted VD, or CS, including elective and emergency procedures.
Scarred uterus: defined as a history of uterine surgery, such as myomectomy, uterine rupture repair, or previous CS [25].
Statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk,
NY, USA) and R software (R Foundation for Statistical Computing, Vienna, Austria;
version 4.3.0). Quantitative variables were first assessed for normality.
Normally distributed data are presented as mean
Variables with a p-value
The predictive performance of delivery mode for NH was evaluated using
sensitivity, specificity, positive predictive value (PPV), and negative
predictive value (NPV). All statistical tests were two-sided, and a
p-value
A total of 201 pregnant women with GDM met the inclusion criteria. Among them,
44 (21.89%) neonates developed NH, whereas 157 (78.11%) did not. Table 1
summarizes the maternal and neonatal characteristics of the hypoglycemia and
non-hypoglycemia groups. Maternal age and gestational age differed significantly
between the two groups. The mean maternal age was higher in the hypoglycemia
group than the non-hypoglycemia group (32.50 vs. 30.57 years, p =
0.004), whereas the gestational period was slightly shorter (270.61 vs. 273.20
days, p = 0.028). When expressed in weeks, the mean gestational age was
38.9
| Variables | Total (n = 201) | Non-NH (n = 157) | NH (n = 44) | Statistic | p-value | |
| Age (mean |
31.00 |
30.57 |
32.50 |
t = –2.90 | 0.004 | |
| Gestational age (mean |
272.64 |
273.20 |
270.61 |
t = 2.21 | 0.028 | |
| Gestational age (mean |
38.95 |
39.03 |
38.66 |
t = 2.21 | 0.028 | |
| Height (mean |
161.75 |
161.94 |
161.05 |
t = 1.18 | 0.238 | |
| Weight (mean |
74.98 |
74.82 |
75.55 |
t = –0.41 | 0.679 | |
| BMI (mean |
28.84 |
28.75 |
29.16 |
t = –0.56 | 0.574 | |
| Fasting blood glucose (mean |
5.08 |
5.07 |
5.14 |
t = –0.73 | 0.465 | |
| Primipara, n (%) | 0.149 | |||||
| No | 118 (58.71) | 88 (56.05) | 30 (68.18) | |||
| Yes | 83 (41.29) | 69 (43.95) | 14 (31.82) | |||
| Gravidity, n (%) | 0.071 | |||||
| 124 (61.69) | 102 (64.97) | 22 (50.00) | ||||
| 77 (38.31) | 55 (35.03) | 22 (50.00) | ||||
| Delivery mode, n (%) | ||||||
| VD | 103 (51.24) | 95 (60.51) | 8 (18.18) | |||
| CS | 98 (48.76) | 62 (39.49) | 36 (81.82) | |||
| Scarred uterus, n (%) | ||||||
| No | 137 (68.16) | 119 (75.80) | 18 (40.91) | |||
| Yes | 64 (31.84) | 38 (24.20) | 26 (59.09) | |||
| Comorbidities, n (%) | 0.896 | |||||
| No | 61 (30.35) | 48 (30.57) | 13 (29.55) | |||
| Yes | 140 (69.65) | 109 (69.43) | 31 (70.45) | |||
| Hypothyroidism, n (%) | 0.894 | |||||
| No | 177 (88.06) | 138 (87.90) | 39 (88.64) | |||
| Yes | 24 (11.94) | 19 (12.10) | 5 (11.36) | |||
| Neonatal gender, n (%) | 0.112 | |||||
| Male | 108 (53.73) | 89 (56.69) | 19 (43.18) | |||
| Female | 93 (46.27) | 68 (43.31) | 25 (56.82) | |||
| Birth weight, g, M (Q1, Q3) | 3450.00 (3200.00, 3780.00) | 3460.00 (3150.00, 3800.00) | 3400.00 (3327.50, 3772.50) | Z = –0.17 | 0.865 | |
| Initial neonatal blood glucose (mean |
3.72 |
4.13 |
2.24 |
t = 14.57 | ||
| Macrosomia, n (%) | 0.219 | |||||
| No | 171 (85.07) | 131 (83.44) | 40 (90.91) | |||
| Yes | 30 (14.93) | 26 (16.56) | 4 (9.09) | |||
| NICU admission, n (%) | 0.233 | |||||
| No | 179 (89.05) | 142 (90.45) | 37 (84.09) | |||
| Yes | 22 (10.95) | 15 (9.55) | 7 (15.91) | |||
t: t-test, Z: Mann-Whitney test,
Variables with p
As shown in Table 2, multivariate analysis demonstrated that only delivery mode
remained an independent predictor of NH. Compared with VD, CS significantly
increased the risk of NH, with an adjusted OR of 4.48 (95% CI: 1.56–12.87,
p = 0.005). Maternal age, gestational age, gravidity, and uterine
scarring were not significantly associated with NH in the multivariate model (all
p
| Variables | Univariate | Multivariate | |||||||||
| β | S.E | Wald | p-value | OR (95% CI) | β | S.E | Wald | p-value | OR (95% CI) | ||
| Scarred uterus | |||||||||||
| No | 1.00 (Reference) | 1.00 (Reference) | |||||||||
| Yes | 1.51 | 0.36 | 17.72 | 4.52 (2.24–9.14) | 0.39 | 0.55 | 0.52 | 0.472 | 1.48 (0.51–4.32) | ||
| Delivery mode | |||||||||||
| VD | 1.00 (Reference) | 1.00 (Reference) | |||||||||
| CS | 1.93 | 0.42 | 20.79 | 6.90 (3.01–15.82) | 1.50 | 0.54 | 7.73 | 0.005 | 4.48 (1.56–12.87) | ||
| Age | 0.12 | 0.04 | 7.78 | 0.005 | 1.13 (1.04–1.23) | 0.05 | 0.05 | 1.00 | 0.318 | 1.05 (0.95–1.16) | |
| Gestational age | –0.05 | 0.02 | 4.58 | 0.033 | 0.95 (0.91–0.99) | –0.02 | 0.03 | 0.46 | 0.497 | 0.98 (0.93–1.04) | |
| Gravidity | |||||||||||
| 1.00 (Reference) | 1.00 (Reference) | ||||||||||
| 0.62 | 0.34 | 3.20 | 0.073 | 1.85 (0.94–3.65) | –0.13 | 0.46 | 0.07 | 0.783 | 0.88 (0.36–2.16) | ||
OR, odds ratio; CI, confidence interval.
CS showed a sensitivity of 81.8%, specificity of 60.5%, PPV of 36.7%, and NPV of 92.2% for NH (Table 3). These results indicate that although CS is characterized by a relatively low PPV, VD is associated with a high NPV (92.2%) for the occurrence of NH in pregnancies complicated by GDM. Fig. 1A illustrates the distribution of NH according to delivery mode, and Fig. 1B shows that initial neonatal blood glucose levels were significantly lower in the CS group than in the VD group.
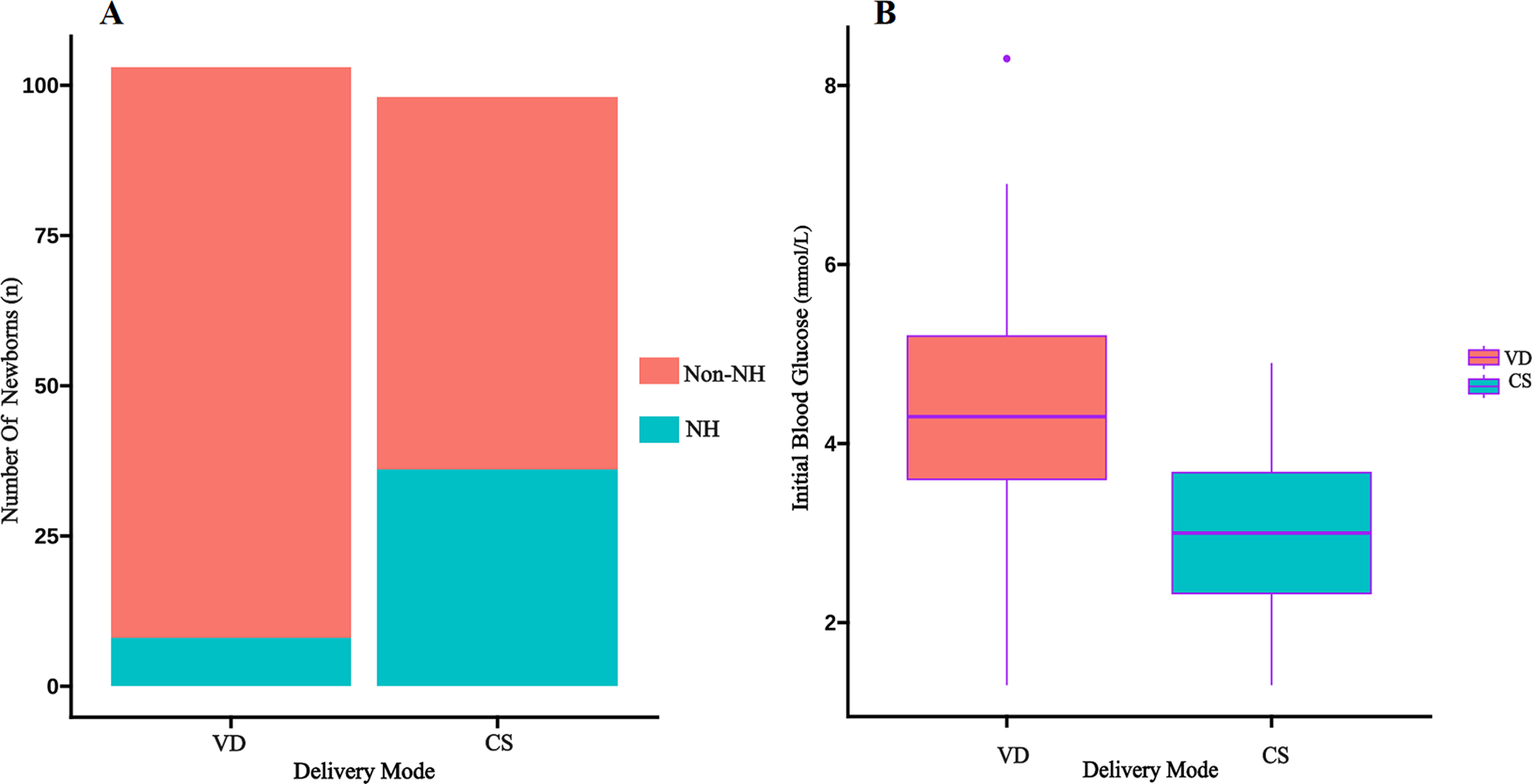 Fig. 1.
Fig. 1.
Association between delivery mode and neonatal hypoglycemia. (A) Stacked bar chart of NH event counts by delivery mode. (B) Box plot of initial neonatal blood glucose by delivery mode, this point represents an outlier in the box plot (beyond 1.5×IQR) and reflects an actual observation.
| AUC (95% CI) | Specificity (95% CI) | Sensitivity (95% CI) | NPV (95% CI) | PPV (95% CI) |
| 0.712 (0.642–0.781) | 0.605 (0.529–0.682) | 0.818 (0.704–0.932) | 0.922 (0.871–0.974) | 0.367 (0.272–0.463) |
AUC, area under the curve; NPV, negative predictive value; PPV, positive predictive value.
This retrospective study evaluated the association between delivery mode and NH among 201 pregnancies complicated by GDM. After adjustment for maternal age, gestational age, gravidity, and a history of uterine scarring, CS remained independently associated with an increased risk of NH, with an adjusted OR of 4.48 compared with VD. In addition, analysis of predictive metrics showed that VD was associated with a high NPV (92.2%), which indicates that neonates delivered vaginally were unlikely to develop hypoglycemia, whereas the PPV of CS was relatively modest. These findings suggest that delivery mode may contribute to early neonatal metabolic risk stratification and should be considered in perinatal monitoring strategies for pregnancies complicated by GDM.
Our findings are consistent with previous studies reporting an association between CS and NH. A 2024 meta-analysis by Wang et al. [20] showed that the odds of hypoglycemia were nearly twice as high in infants delivered by CS compared with those delivered vaginally (OR = 1.90, 95% CI: 1.23–2.92). Similarly, a cohort study by Ogunyemi et al. [19] reported that NH in term infants was associated with several obstetric and perinatal factors, including mode of delivery, highlighting the potential role of CS in neonatal glucose instability. Another study of 4602 infants reported that CS was associated with an increased likelihood of requiring glucose infusion (OR = 1.4, 95% CI: 1.1–1.9), with earlier onset of hypoglycemia particularly evident among infants of obese mothers [16]. Our study extends these observations by focusing specifically on pregnancies complicated by GDM, in which we observed a higher OR associated with CS. This stronger association may reflect the unique metabolic environment of GDM: chronic in utero hyperglycemia, persistent neonatal hyperinsulinemia, absence of labor-induced counterregulatory hormonal surges, and delayed initiation of feeding may collectively heighten the risk of hypoglycemia in this subgroup [27, 28, 29]. Previous studies have reported that cesarean delivery is more frequent among neonates with hypoglycemia; however, it may not remain an independent predictor after adjustment for confounding factors, with maternal obesity and glycemic control playing more prominent roles in neonatal glucose regulation [16, 18]. The larger effect size observed in our study population may be attributable to differences in the definition of hypoglycemia, the higher incidence of NH in our population, or variations in confounder adjustment and population characteristics.
The high CS rate observed in our study (48.76% overall) reflects broader trends in China. A 2023 analysis of 7.6 million deliveries across 4359 hospitals reported an overall CS rate of 44.5%, approximately three times the World Health Organization recommended maximum of 15% [21]. Multiple factors have been proposed to contribute to the elevated CS rate in China, including maternal preference, often related to fear of labor pain, provider- and system-level drivers, a high prevalence of repeat CSs, and variation in obstetric practice and capacity across hospitals [30]. In pregnancies complicated by GDM, CS may be indicated more frequently due to concerns about macrosomia, shoulder dystocia, and labor dystocia. Given the association between CS and NH observed in our study, these high CS rates may amplify the population-level burden of neonatal metabolic complications in China.
The increased susceptibility to NH after CS in GDM pregnancies may be explained
by several disruptions in perinatal glucose regulation. In GDM, chronic maternal
hyperglycemia enhances placental glucose transfer and induces fetal
Our study has several strengths. It incorporated a comprehensive set of maternal and neonatal characteristics, which enabled a more thorough assessment of risk factors and reduced the likelihood of residual confounding. By adjusting for key variables, including uterine scarring, gestational age, gravidity, and maternal age, the multivariate model provided a more accurate estimate of the independent association between CS and NH. Clinically, these findings have important implications for perinatal care. First, delivery mode should be incorporated into risk stratification algorithms for identification of neonates at elevated risk of hypoglycemia. Second, when CS is indicated in GDM pregnancies, enhanced monitoring protocols should be implemented, including earlier and more frequent glucose measurements. Third, interventions known to reduce NH risk, such as maintaining maternal glucose stability preoperatively, ensuring early skin-to-skin contact, and promoting early breastfeeding, should be prioritized. Individualized delivery decisions should be made through multidisciplinary collaboration, with assessment of maternal glycemic control, estimated fetal weight, and available delivery resources.
This study has several limitations that warrant acknowledgment. First, as a single-center retrospective study, residual selection bias cannot be fully excluded, and the observational design does not allow causal inference regarding the relationship between delivery mode and NH. Second, because infants delivered before 35 weeks were excluded to limit confounding from prematurity, our findings may not generalize to moderately or late preterm GDM pregnancies, which constitute an important high-risk subgroup. Third, several potentially relevant maternal variables, including the distinction between elective and emergency CS, diabetes treatment modality (dietary management vs. insulin or oral hypoglycemic agents), and physical activity or dietary patterns, were not consistently documented in the medical record system and therefore could not be incorporated into the multivariate model. Fourth, mechanistic indicators such as continuous maternal glucose profiles, neonatal cord blood insulin or counterregulatory hormones (e.g., cortisol, catecholamines), and markers of metabolic adaptation were unavailable, which limited our ability to explore physiological pathways linking delivery mode to neonatal glucose instability. Fifth, this study focused only on early NH and did not include longitudinal assessment of neurodevelopment, cognitive function, or behavioral outcomes, which limits evaluation of the long-term consequences of hypoglycemia. Finally, as the study was conducted in a single maternity center in China, the applicability of these findings to other healthcare systems, including international or resource-limited settings, warrants further validation through multicenter prospective studies.
CS is an independent risk factor for NH in infants born to mothers with GDM. In clinical practice, clinicians should ensure maternal and fetal safety, consider glycemic control and labor-related risks, select the delivery mode accordingly, and strengthen postpartum neonatal blood glucose monitoring to reduce adverse outcomes associated with hypoglycemia.
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
QL contributed to study conception, data collection, and initial drafting of the manuscript. FW contributed to data analysis, interpretation, and critical revision. SZ contributed to methodology design, statistical analysis, and data curation. BD contributed to overall supervision, final approval of the version to be published, and accountability for all aspects of the work. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Anhui No.2 Provincial People’s Hospital (Approval No. (R) 2025-107). Because the study used de-identified retrospective data, the requirement for informed consent was waived by the ethics committee.
Not applicable.
This research received no external funding.
The authors declare no conflicts of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/CEOG47854.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.