

 , Danting Zhong 1, Weikang Chen 1, Fang Zhang 1, Lanfeng Xing 1,*
, Danting Zhong 1, Weikang Chen 1, Fang Zhang 1, Lanfeng Xing 1,*
1 Department of Reproductive Endocrinology, School of Medicine, Women’s Hospital, Zhejiang University, 310006 Hangzhou, Zhejiang, China
Abstract
Infertility has become a global public health and psychosocial challenge, bringing substantial psychological pressure to affected individuals and couples. To investigate the effects of fertility stress and social support in infertile patients and their spouses, and to examine the mediating role of irrational parenthood cognition.
Using convenience sampling, 425 infertile couples were recruited from a reproductive center in Zhejiang Province from January 2023 to June 2024. Participants completed questionnaires including general demographic information, the Irrational Parenthood Cognition Scale, and the Fertility Problem Inventory (FPI) and the Social Support Rating Scale (SSRS). Data were analyzed using descriptive statistics, paired-samples t-tests, Harman’s single-factor test, Pearson correlation analysis, and the Actor-Partner Interdependence Mediation Model (APIMeM).
In infertile couples, social support was negatively correlated with both irrational parenthood cognition and fertility stress (p < 0.01), whereas irrational parenthood cognition was positively correlated with fertility stress (p < 0.01). For actor effects, wives’ social support influenced their own fertility stress through their own, but not their husbands’, irrational parenthood cognition, whereas husbands’ social support influenced their own fertility stress through both their own and their wives’ irrational parenthood cognition. For partner effects, husbands’ social support influenced wives’ fertility stress through the wives, but not their own, irrational parenthood cognition, whereas wives’ social support influenced husbands’ fertility stress through both their own and their husbands’ irrational parenthood cognition.
Clinical interventions should address infertile patients and their spouses as an integrated unit, targeting both fertility cognition and social support to alleviate fertility stress.
Keywords
- infertility
- fertility stress
- social support
- irrational parenthood cognitions
- Actor-Partner Interdependence Mediation Model (APIMeM)
Infertility refers to the failure to conceive after one year of regular sexual intercourse without contraception [1]. Data from the World Health Organization shows [2] that the incidence of infertility has been increasing annually, reaching 10% to 20%, with one in every six couples experiencing fertility issues, making it the third major health concern after cancer and cardiovascular diseases [3]. Irrational fertility cognition refers to a cognitive bias in people’s perception of reproduction, believing that one must have a child to achieve a happy life [4]. Influenced by traditional Chinese fertility concepts, many couples view having a child as the bond that sustains family and marital happiness, and parenting is considered one of life’s important goals. As a special reproductive health defect, infertility affects over 80% of patients, who bear significant reproductive burdens and psychological stress [5]. A study has demonstrated [6] that support from a spouse is directly or indirectly related to stress experienced by oneself or the spouse. In family relationships, when women are more likely to feel support from their partners, they are more prone to conceive and engage in reproductive behavior [7], and family support plays a significant role in reproductive decision-making [8]. Research indicates that social support influences women’s fertility values, and there is a significant positive correlation between fertility cognition and social support among women [9]. Previous studies focusing solely on infertile women or men failed to fully understand the crucial role played by their spouses. For infertile couples, childbearing is a shared challenge, necessitating a comprehensive analysis of the couple as a whole. This study employs Kenny’s Actor-Partner Interdependence Model Extended to Mediation (APIMeM) [10, 11] to examine the relationship between social support, irrational fertility cognition, and fertility stress in infertile couples. In this model, an individual’s dependent variable is influenced not only by their own independent variables (subject effect) but also by specific object variables within a defined scope (object effect). Independent variables affect outcome variables through both direct effects (direct effect) and mediated effects via intermediate variables (indirect effect). The study investigated whether fertility stress in infertile couples is simultaneously influenced by their own and their spouse’s social support, and analyzed whether irrational fertility cognition serves as a mediating factor in this relationship. This study aimed to clarify the underlying mechanisms and provide theoretical foundations for clinical personalized interventions.
A convenience sampling method was employed to recruit 425 infertile couples from a reproductive medical center in Zhejiang Province between January 2023 and June 2024. Inclusion criteria: (i) meeting the diagnostic criteria for infertility as described by the World Health Organization [1]; (ii) infertility caused by female factors; (iii) all participants voluntarily participated and signed the informed consent form. Exclusion criteria: individuals with a history of mental illness or use of antipsychotic medications within the past three months; those unable to communicate effectively or comprehend written content; participants who declined cooperation after the researcher’s explanation or withdrew during the study. The sample size was calculated based on the principle of 5–10 times the number of questionnaire items for analysis, yielding a required range of 415–830 participants. Accounting for a 20% potential attrition rate, the final target sample size was determined to be 498–996 participants. The study adhered to the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Women’s Hospital, School of Medicine, Zhejiang University (IRB-20220124-R). All participants provided informed consent prior to enrollment.
The general information questionnaire was designed by the researcher according to the purpose of the survey, including age, residence, education level, occupation, annual family income, length of marriage, and marital history.
The Irrational Parenthood Cognition Questionnaire (IPCQ) was developed in the Netherlands and translated into Chinese [12]. It was created to test fertility awareness in women of reproductive age. The questionnaire contains 14 items, scored using a 5-point scale (1–5 points, from strongly disagree to strongly agree). The total score ranges from 14 to 70 points, with 42 points serving as the cutoff for irrational parenthood cognition. Higher scores indicate the belief that having a child would contribute to happiness. The Cronbach’s alpha for the scale was 0.87.
Fertility stress was measured using the Fertility Problem Inventory (FPI) [13, 14]. The inventory consists of 46 items categorized into subscales: social, sexual, and relationship concerns, rejection of child-free living, and the need for parenthood. The comprehensive FPI is frequently applied to assess infertility stress worldwide, and its total and subscale scores are reliable and valid. The total fertility pressure score and its sub-scales demonstrate high levels of reliability and validity, with Cronbach’s alpha coefficients ranging from 0.77 to 0.93, making them widely used in international infertility research. Due to their strong specificity and comprehensiveness, they have been validated for clinical evaluation of infertility patients in China [15].
We used the Social Support Rating Scale (SSRS) [16] to assess the social support status of patients with infertility. It consists of 10 items that span objective and subjective assistance and social support utilization. The overall score comprises the sum of scores (64) from the 10 items, with higher scores indicating better social support. The Cronbach’s alpha coefficients for all dimensions of social support ranged from 0.89 to 0.94, with an overall test-retest reliability of 0.92, and have been widely used in clinical practice [17].
Trained investigators explained the purpose and significance of the study to eligible infertile couples and obtained their informed consent. Participants then completed an electronic questionnaire via Questionnaire Star APP (Wenjuanxing, Changsha, Hunan, China), with on-site submission. Investigators provided standardized instructions for any queries during the process and verified submissions immediately. A total of 900 questionnaires were distributed, with 850 valid responses collected, yielding an effective response rate of 94.5%.
Data analysis was performed using SPSS 26.0 statistical software (IBM Corp.,
Armonk, NY, USA). The data were analyzed using descriptive statistics, paired
samples t-tests, Harman’s single factor test, Pearson’s correlation
analysis, and the APIMeM model was employed using structural equation modeling to
account for the non-independence of data from couples. The APIMeM model was
constructed using Mplus 8.3 software (Los Angeles, CA, USA), with fertility
pressure as the dependent variable, social support as the independent variable,
and irrational parenthood cognition as the mediating variable. The APIMeM model
was built using maximum likelihood estimation [18, 19], with bootstrap mediation
effect testing (repeated sampling 2000 times) at a significance level of
General demographic data of 425 infertile couples: male age 22–50 years, female age 20–46 years. The demographic profiles of the 425 infertile couples, including age, residential area, ethnicity, marital history, duration of marriage, educational level, occupation, and annual household income, are presented in Table 1.
| Variable | Groups | Wives | Husbands |
| Age (years) | 145 (34.1) | 88 (20.7) | |
| 31–35 | 186 (43.8) | 164 (38.6) | |
| 36–40 | 82 (19.3) | 103 (24.2) | |
| 12 (2.8) | 70 (16.5) | ||
| Residence | Countryside | 123 (28.9) | 123 (28.9) |
| City | 270 (63.5) | 270 (63.5) | |
| Urban and rural areas | 32 (7.5) | 32 (7.5) | |
| Nationality | Han Chinese | 414 (97.4) | 411 (96.7) |
| Minority | 11 (2.6) | 14 (3.3) | |
| Marital Status | First Marriage | 363 (85.4) | 363 (85.4) |
| Remarriage | 62 (14.6) | 62 (14.6) | |
| Marriage duration (years) | 1–2 | 100 (23.5) | 100 (23.5) |
| 3–5 | 201 (47.3) | 201 (47.3) | |
| 6–10 | 90 (21.2) | 90 (21.2) | |
| 34 (8.0) | 34 (8.0) | ||
| Level of Education | Primary and less | 65 (15.3) | 57 (13.4) |
| Junior | 68 (16.0) | 68 (16.0) | |
| Senior | 110 (25.9) | 87 (20.5) | |
| Tertiary | 154 (36.2) | 159 (37.4) | |
| College/university degree | 28 (6.6) | 54 (12.7) | |
| Occupation | Worker | 38 (8.9) | 71 (16.7) |
| Farmer | 7 (1.6) | 11 (2.6) | |
| Civil Servant | 10 (2.4) | 14 (3.3) | |
| Self-employed | 39 (9.2) | 57 (13.4) | |
| Teacher | 37 (8.7) | 15 (3.5) | |
| Professional/technical | 52 (12.2) | 118 (27.8) | |
| Freelance | 84 (19.8) | 56 (13.2) | |
| Others | 158 (37.2) | 83 (19.5) | |
| Annual household income (RMB) | 56 (13.2) | 56 (13.2) | |
| 50,000–100,000 | 122 (28.7) | 122 (28.7) | |
| 100,001–300,000 | 149 (35.1) | 149 (35.1) | |
| 98 (23.1) | 98 (23.1) |
Abbreviations: N, number of couples. 1 USD
To assess potential common method bias, Harman’s single-factor test was
utilized. The results revealed 18 factors with eigenvalues
The total social support scores for 425 wives were (41.192
| Variable | Wives | Husbands | t | p |
| SSRS | 41.192 |
43.795 |
–7.537 | |
| IPC | 41.907 |
38.586 |
8.786 | |
| FPI | 146.414 |
142.162 |
3.306 | 0.001 |
Abbreviations: SSRS, Social Support Rating Scale; IPC, Irrational Parenthood Cognition; FPI, Fertility Problem Inventory.
The results demonstrated significant negative correlations between social support and both irrational parenthood cognitions and fertility stress among infertile couples. Conversely, irrational parenthood cognitions showed significant positive correlations with fertility stress. Detailed correlation coefficients are presented in Table 3.
| Variable | 1 | 2 | 3 | 4 | 5 | 6 |
| SSRS of wife | 1 | |||||
| SSRS of husband | 0.572** | 1 | ||||
| IPC of wife | –0.509** | –0.413** | 1 | |||
| IPC of husband | –0.387** | –0.541** | 0.651** | 1 | ||
| FPI of wife | –0.565** | –0.459** | 0.685** | 0.520** | 1 | |
| FPI of husband | –0.484** | –0.516** | 0.593** | 0.651** | 0.690** | 1 |
** indicates p
An initial Actor-Partner Interdependence Mediation Model (APIMeM) was
constructed with irrational parenthood cognitions as the mediating variable
between social support and fertility stress. The model was tested using bootstrap
resampling with 2000 iterations, with the final solution converging on a
saturated model (Fig. 1). The results demonstrated that the model fit well with
the binary data, with
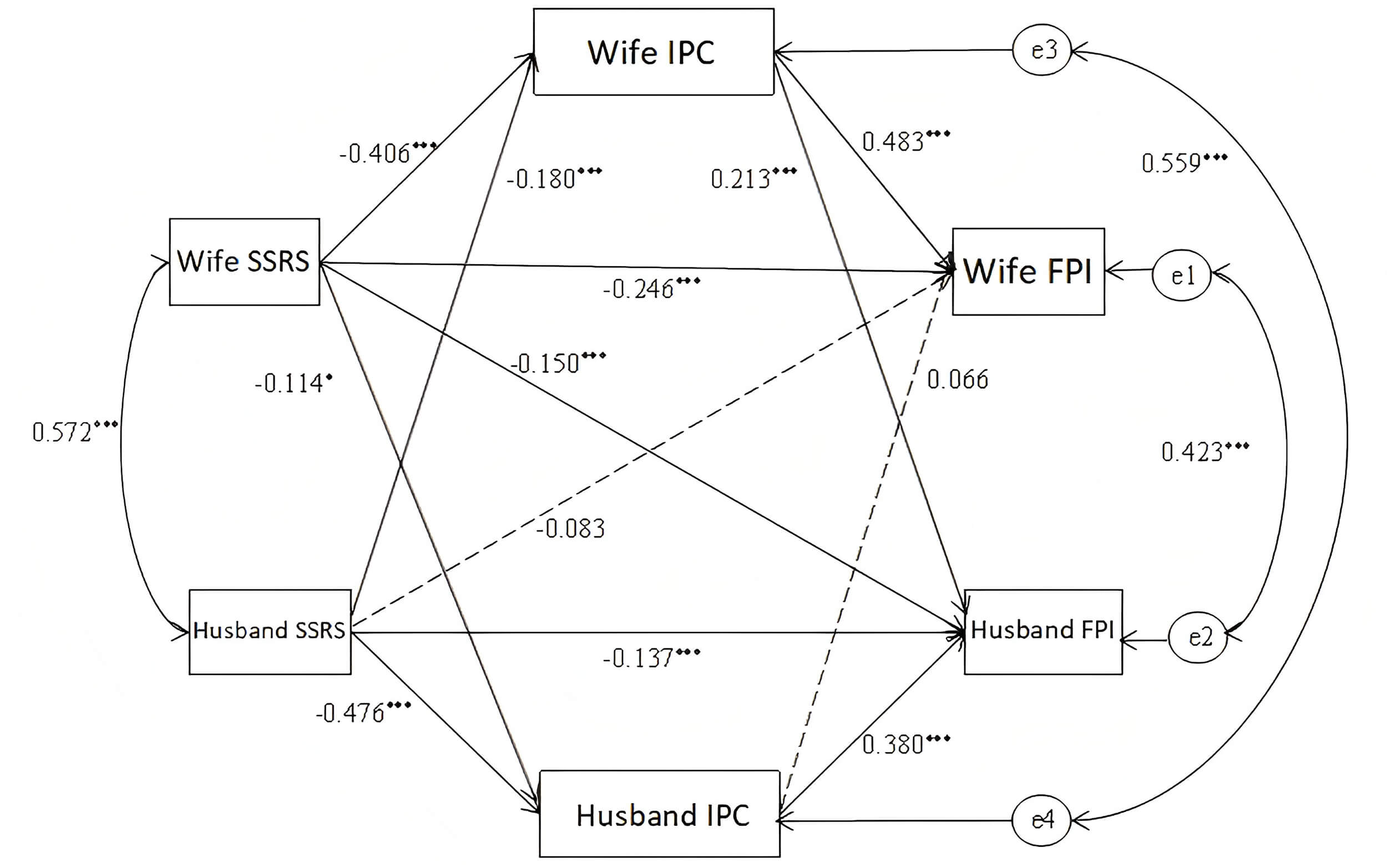 Fig. 1.
Fig. 1.
Path analysis model in infertile couples. (e1–e4 are
error terms, * indicates p
The effect size of the constrained simplified model is shown in Table 4. The
social support of the individual significantly predicts the fertility pressure of
the individual and the spouse (both the subject effect and the object effect are
significant). Specifically, the wife’s social support had a direct effect on her
own fertility pressure (
| Effect | SE | 95% CI | Effect proportion (%) | p | ||
| Subject effect of wife | Total effect | –0.450 | 0.046 | (–0.536, –0.363) | 0.000 | |
| Direct effect | –0.246 | 0.042 | (–0.329, –0.164) | 54.67% | 0.000 | |
| Total indirect effect | –0.204 | 0.030 | (–0.264, –0.147) | 45.33% | 0.000 | |
| Wife SSRS→Wife IPC→Wife FPI | –0.196 | 0.030 | (–0.26, –0.140) | 43.56% | 0.000 | |
| Wife SSRS→Husband IPC→Wife FPI | –0.008 | 0.007 | (–0.023, 0.005) | 1.78% | 0.289 | |
| Object effect of wife | Total effect | –0.201 | 0.051 | (–0.296, –0.102) | 0.000 | |
| Direct effect | –0.083 | 0.050 | (–0.182, 0.012) | 41.29% | 0.097 | |
| Total indirect effect | –0.118 | 0.033 | (–0.185, –0.051) | 58.71% | 0.000 | |
| Husband SSRS→Wife IPC→Wife FPI | –0.087 | 0.025 | (–0.137, –0.042) | 43.28% | 0.001 | |
| Husband SSRS→Husband IPC→Wife FPI | –0.031 | 0.026 | (–0.082, 0.019) | 15.42% | 0.227 | |
| Subject effect of Husband | Total effect | –0.356 | 0.043 | (–0.439, –0.267) | 0.000 | |
| Direct effect | –0.137 | 0.046 | (–0.224, –0.042) | 38.48% | 0.003 | |
| Total indirect effect | –0.219 | 0.029 | (–0.278, –0.166) | 61.52% | 0.000 | |
| Husband SSRS→Wife IPC→Husband FPI | –0.038 | 0.014 | (–0.072, –0.015) | 10.67% | 0.007 | |
| Husband SSRS→Husband IPC→Husband FPI | –0.181 | 0.026 | (–0.234, –0.128) | 50.84% | 0.000 | |
| Object effect of Husband | Total effect | –0.280 | 0.049 | (–0.379, –0.181) | 0.000 | |
| Direct effect | –0.150 | 0.046 | (–0.242, –0.060) | 53.57% | 0.001 | |
| Total indirect effect | –0.130 | 0.029 | (–0.190, –0.073) | 46.43% | 0.000 | |
| Wife SSRS→Wife IPC→Husband FPI | –0.087 | 0.020 | (–0.131, –0.05) | 31.07% | 0.000 | |
| Wife SSRS→Husband IPC→Husband FPI | –0.043 | 0.021 | (–0.088, –0.005) | 15.36% | 0.041 | |
As shown in Table 4, the indirect effect of social support on fertility pressure
through irrational fertility cognition is significant for both husband and wife.
The wife’s subjective indirect effect (
This study employed the subject-object interdependence mediation model to investigate the underlying mechanisms linking social support, irrational fertility beliefs, and reproductive stress in infertile couples. The findings demonstrated significant subject and object effects across these psychological variables, highlighting the importance of considering the bidirectional interaction between partners in psychological interventions for infertile couples.
The results revealed that the husband’s social support level was significantly
higher than that of the wife (p
The correlation analysis demonstrated that social support was significantly negatively correlated with irrational fertility cognition and fertility pressure, while irrational fertility cognition was significantly positively correlated with fertility pressure. This study demonstrated that higher scores in irrational fertility cognition correlate with greater fertility pressure and lower utilization of social support, consistent with findings by Li et al. [26] and Li et al. [27]. It also validated the cognitive behavioral theory’s perspective that irrational beliefs exacerbate psychological stress [28, 29]. Fertility pressure refers to the various limiting factors faced by individuals or families when deciding to have children, which include physiological, psychological, material, and environmental factors. In addition to obvious pressure, such as economic pressure, there is an important hidden factor: the traditional fertility concept. The traditional conception of fertility, shaped by centuries of socio-psychological and cultural sedimentation, has profoundly influenced reproductive behaviors. This cultural phenomenon is manifested in the pursuit of a large family size with the belief that more children mean greater blessings, the emphasis on male heirs for old-age support, the gender bias favoring sons over daughters, the value placed on continuing the family line, and the ideal of a large extended family where generations live under one roof. In the traditional cultural context of China, childbirth is considered necessary, so this invisible social pressure may increase the psychological burden of patients and may also damage the relationship between infertile patients and their family and friends [30]. For infertile couples, excessive reproductive pressure may lead to negative emotions such as inferiority, resulting in active or passive separation from family and social relationships, thereby damaging the quality of life. Therefore, we also need to pay attention to the number, size, and mutual relationships among family members.
Studies have shown that high levels of social support are crucial in preventing anxiety and depression, particularly after failed fertility treatments [31]. The rationality of these infertile patients’ cognition of fertility is related to the degree of social support they get from family, friends, or society. The higher the degree of social support they get and the more effectively they can use the social support, the more rational their cognition of fertility. This suggests that social support, as an important psychological resource, may alleviate fertility pressure by reducing irrational fertility cognition. Strengthening the social support system may be an effective way to intervene in fertility pressure.
The APIMeM analysis further revealed the mediating role of irrational fertility cognition in the “social support-fertility pressure” pathway. Regarding the principal effect, the wife’s social support primarily alleviates her reproductive stress by reducing her irrational beliefs about childbirth. This demonstrates that her cognitive regulation plays a central role in stress management. The social support received by individuals effectively modulates their irrational beliefs about reproduction, thereby mitigating reproductive stress. This finding aligns with the cognitive behavioral theory’s assertion that “cognitive regulation is pivotal in stress formation” [28, 29]. The husband’s subjective effect also indirectly influences his fertility pressure through his own and his wife’s irrational fertility cognition, which indicates that the husband’s pressure experience is more easily influenced by the cognition mode of both husband and wife. In terms of object effect, the husband’s social support can alleviate the wife’s fertility pressure by reducing her irrational fertility cognition, while the wife’s social support can indirectly affect the husband’s stress level by regulating her own cognition, reflecting the bidirectional interaction of the psychological process of the couple. The results of this study confirm the applicability of the “cognition-stress” theory model in the couple relationship, and suggest that the reconstruction of the cognitive pattern and the improvement of the emotional interaction process should be emphasized in the psychological intervention of infertile couples.
For most patients undergoing assisted reproductive therapy, the primary goal is to achieve pregnancy and have their own children, thereby enhancing marital happiness and quality of life [15]. Influenced by societal pressures and women’s aspirations for parental roles, childbearing becomes a pivotal life mission. However, infertility deals a severe blow, causing immense psychological stress [22]. In conclusion, we should proactively provide patients with medical information and psychosocial support, helping them expand their sources of social support and enhance their utilization of such support. Through targeted psychological interventions and guidance—such as mindfulness therapy, group cognitive therapy, and rational-emotive behavior therapy—we can alleviate patients’ fertility-related stress and guide them to replace irrational thought patterns and beliefs with rational ones.
① Implement the integrated psychological intervention for couples: in clinical practice, we should break through the traditional individual-centered psychological service mode, and include both spouses in the intervention system, so as to build a more resilient family coping system by enhancing the emotional support and cognitive coordination between couples.
② Promote the application of cognitive restructuring in the field of reproductive health: adopt cognitive behavioral therapy to systematically identify and correct irrational reproductive concepts in couples, and establish a scientific and reasonable reproductive cognitive framework to effectively alleviate emotional distress and psychological stress caused by cognitive bias.
③ Build a diversified social support network: integrate medical institutions, community resources, and peer support groups, expand the social support dimension of infertile couples through group intervention, family system interview, and other forms, and improve their psychological capital and social resources needed to cope with the pressure of fertility.
④ Gender differentiated clinical psychological assessment and intervention: in the process of diagnosis and treatment, we should pay full attention to the influence of gender factors on the psychological adaptation process, especially paying attention to the vulnerability of female patients in irrational cognition and stress response, and make a gender sensitive stratified intervention program to achieve accurate psychological support.
There were some limitations in this study. Firstly, the cross-sectional design employed in the research cannot completely eliminate the possibility of selection bias. Secondly, our measure of household income was aggregate and did not capture the individual incomes of husbands and wives. As suggested by the reviewer, the proportional contribution to household income is a potential key factor in intra-household bargaining power, and future studies would benefit from collecting this disaggregated data. Thirdly, the single-center convenience sampling method used, combined with the fact that most participants were Han urban residents, may limit the generalizability of the findings to rural areas, ethnic minority groups, or couples with diverse cultural backgrounds. In the future, the scope of research will be further expanded to carry out multi-region and multi-center joint research.
This study demonstrated deep integration between stress-buffering theory and family systems theory. Social support exerts its influence through dual pathways: direct buffering of stress and indirect regulation of cognition, while spousal interaction patterns further illustrate the holistic nature of family systems. The research has certain limitations: the sample focuses on urban infertile couples in China, requiring cautious generalization of findings; the cross-sectional design makes it difficult to clarify causal temporal relationships between variables. Future studies should expand to cross-cultural populations and employ longitudinal tracking designs to explore the dynamic evolution of support-stress relationships.
Data is available from the corresponding author on reasonable request.
YL: conceptualization, writing-original draft, formal analysis, funding acquisition, data curation. DZ: investigation, methodology, formal analysis, data curation. WC: investigation, methodology, writing-review & editing. FZ: conceptualization, supervision, project administration, writing-review & editing. LX: conceptualization, project administration, supervision, writing-review & editing. All authors contributed to critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was carried out in accordance with the guidelines of the Declaration of Helsinki. This study was reviewed and approved by the Ethics Committee of Women’s Hospital, School of Medicine, Zhejiang University (Approval Number: IRB-20220124-R). A written consent was signed by the patients.
The authors are grateful to the patients for their participation in this study.
This work was support by Medical and Health Technology Program of Zhejiang Province (Grant NO. 2025KY927).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.