






 , Diellza Lipovica 2,†, Shpëtim Thaçi 1,*
, Diellza Lipovica 2,†, Shpëtim Thaçi 1,* , Drilon Deliu 2, Mentor Sopjani 1,*
, Drilon Deliu 2, Mentor Sopjani 1,*1 Faculty of Medicine, University of Prishtina, 10 000 Prishtina, Kosova
2 Department Gynecology and Obstetrics, University Clinical Center of Kosova, 10 000 Prishtina, Kosova
†These authors contributed equally.
Abstract
Placenta previa (PP) is a serious obstetric condition associated with maternal and neonatal morbidity, particularly in settings with increasing cesarean delivery rates. Data describing birth patterns and clinical characteristics of PP from Southeast Europe remain limited.
This retrospective descriptive study included all deliveries at the University Clinical Center of Kosova (UCCK) between January 1 through December 31, 2023. Maternal age, pregnancy order, singleton or multiple delivery, delivery mode, as well as PP diagnosis and subtype were extracted from medical records. The data were summarized with descriptive statistics and are presented as counts and percentages.
A total of 7743 deliveries were recorded. Birth frequency declined progressively as gravidity increased, and singleton pregnancies predominated (96.97%). Mean maternal age increased with higher gravidity. PP was identified in 52 deliveries (0.67%). Central PP was the most frequent subtype (67.3%), and all PP cases were delivered by cesarean section. Advanced maternal age (≥30 years) was observed in 78.8% of PP cases, and 42.3% had a history of previous cesarean delivery.
In this large single-center retrospective study, PP was uncommon but predominantly presented as central PP, which often required a cesarean delivery. Advanced maternal age and a history of prior cesarean delivery were frequently observed among affected women. These findings underscore the importance of careful prenatal monitoring and delivery planning in pregnancies exhibiting these risk factors.
Keywords
- placenta previa
- birth patterns
- maternal age
- cesarean delivery
- gravidity
Maternal and neonatal health outcomes remain a significant global public health concern, especially in low- and middle-income countries where access to comprehensive prenatal and obstetric care is limited. The World Health Organization reports that timely and effective prenatal, intrapartum, and postnatal care can significantly decrease maternal and neonatal morbidity and mortality, particularly in settings with limited resources [1]. In this context, descriptive population-based data on pregnancy characteristics and obstetric complications are essential for informing health systems and clinical practice.
Placenta previa (PP) is a serious obstetric condition in which the placenta implants in the lower segment of the uterus and partially or completely covers the internal cervical os. This condition raises the risk of antepartum hemorrhage, preterm delivery, and operative birth, and in severe cases, it may require major procedures such as cesarean delivery or hysterectomy [2, 3, 4]. The reported global incidence of PP ranges between 0.3% and 0.8% of pregnancies, although considerable variation has been observed across populations. This variation reflects differences in maternal demographics, reproductive patterns, and obstetric practices [2].
Previous studies have reported that PP occurs more frequently among women of advanced maternal age, those with higher parity, a history of cesarean delivery or uterine surgery, and pregnancies conceived using assisted reproductive technologies [5, 6]. Alongside rising cesarean section rates worldwide, research attention has increasingly focused on abnormal placentation, including PP and placenta accreta spectrum (PAS) disorders. However, most available evidence originates from high-income countries, and data from Southeast Europe remain limited. Kosova is an intriguing context due to its shifting reproductive trends, altering maternal age distribution, and the rising application of surgical obstetric interventions in the post-conflict era. Despite these demographics and healthcare changes, comprehensive hospital-based data on birth patterns and the clinical characteristics of PP in this population remain limited.
The aim of the present study was to describe birth patterns, maternal age trends, and the incidence and clinical characteristics of PP among deliveries at the University Clinical Center of Kosova (UCCK), the country’s sole tertiary referral hospital, over a one-year period. By providing population-specific descriptive and comparative data, this study seeks to address the limited regional literature and support improved antenatal risk stratification and obstetric care planning.
This single-center, retrospective, cross-sectional observational study was conducted at the Department of Gynecology and Obstetrics at UCCK, the only tertiary referral hospital in the country. The study comprised all deliveries that occurred at UCCK from January 1 through December 31, 2023.
All women who delivered at UCCK during the study period met the eligibility
criteria for inclusion. Deliveries were defined as births that occurred at
Gravidity was defined as the total number of pregnancies, including current pregnancy, live births, abortions, and intrauterine fetal deaths. Birth multiplicity was categorized as singleton, twin, or triplet delivery. PP was defined as placental implantation partially or completely covering the internal cervical os, diagnosed antenatally by transabdominal and/or transvaginal ultrasonography and/or confirmed intraoperatively at cesarean delivery. PP was classified as central (complete), partial, marginal, or low-lying according to standard clinical definitions. The following variables were extracted from medical records: maternal age at delivery, gravidity, mode of delivery (vaginal or cesarean section), birth multiplicity, neonatal birth weight, and neonatal Apgar scores at 1 and 5 minutes. Maternal comorbidities were recorded, including diabetes mellitus, hypertensive disorders of pregnancy, anemia, and hypothyroidism. Obstetric history included previous cesarean delivery, prior uterine surgery, infertility history, and use of assisted reproductive technology. Intrapartum and postpartum interventions, such as blood transfusion and hysterectomy, were also recorded.
No formal comparison group analysis was performed. Deliveries were analyzed descriptively, and results were presented for the overall delivery population as well as for the PP subgroup.
Data were collected from medical records, entered into Microsoft Excel (Office 2020 version; Microsoft Corporation, Redmond, WA, USA), and summarized using descriptive statistics. Categorical variables are presented as counts and percentages.
During the study period, a total of 7743 deliveries were recorded. The number of
deliveries decreased progressively with increasing pregnancy order: first
pregnancy (n = 3001), second (n = 2311), third (n = 1541), fourth (n = 635),
fifth (n = 185), and higher-order pregnancies (
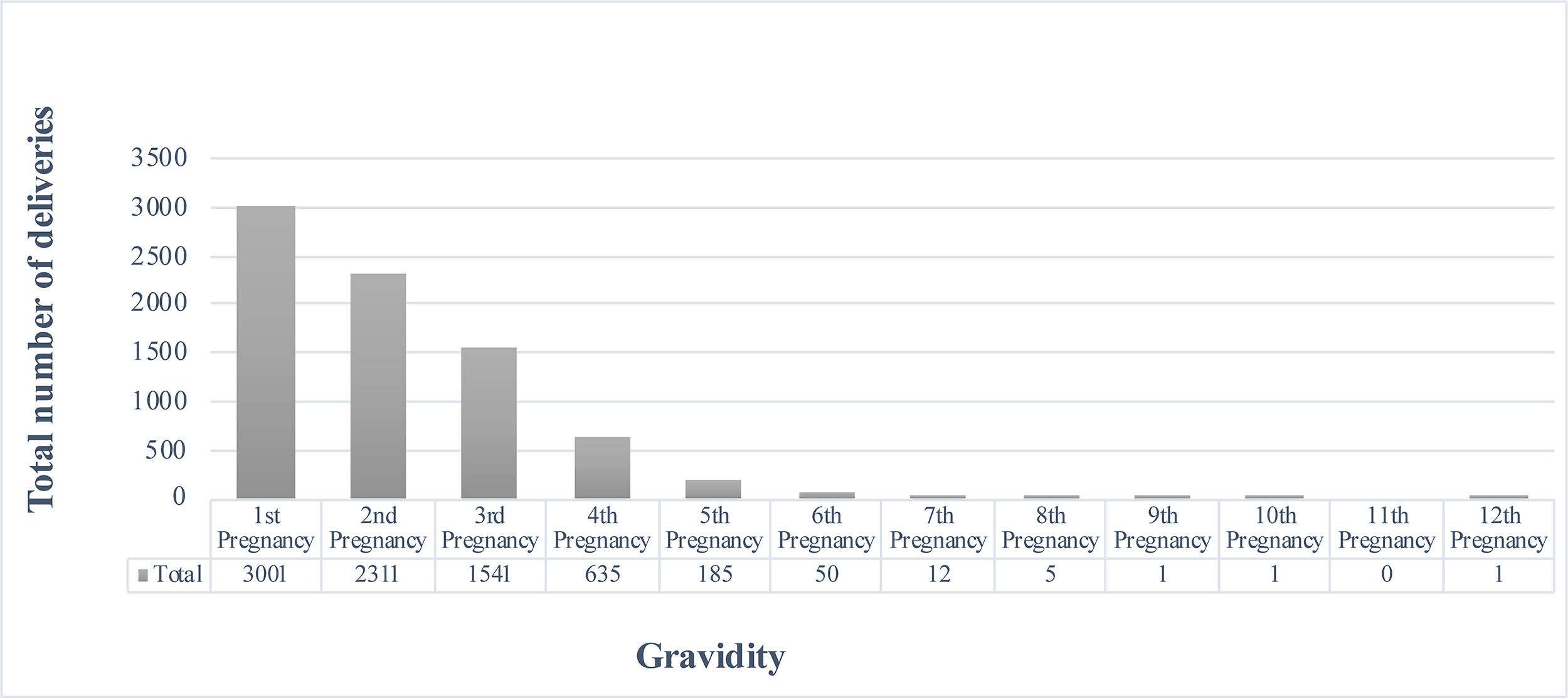 Fig. 1.
Fig. 1.
Distribution of deliveries by gravidity. This figure shows the distribution of births by gravidity. First pregnancies accounted for the highest number of deliveries (n = 3001), and delivery counts decreased with increasing gravidity. Counts represent the number of deliveries recorded during the study period and exclude pregnancies that ended before the delivery.
Singleton deliveries accounted for the vast majority of births (96.97%) across all pregnancy orders. This pattern may be influenced by maternal age and other reproductive factors; however, further studies are required to clarify the underlying determinants. The data indicate that a limited number of women had more than four children. Both biological factors and social decisions may influence this pattern. Deliveries of twins and triplets were rare and occurred primarily in lower-order pregnancies. Most twin deliveries occurred between the first and fourth pregnancies, while triplet births were rare and mostly observed in early pregnancy orders. Multiple births were not observed in higher-order pregnancies, except for a single triplet delivery in the sixth pregnancy order (Fig. 2). These findings align with established reproductive patterns [7]: fertility and the probability of multiple births peak in earlier pregnancies and decline thereafter.
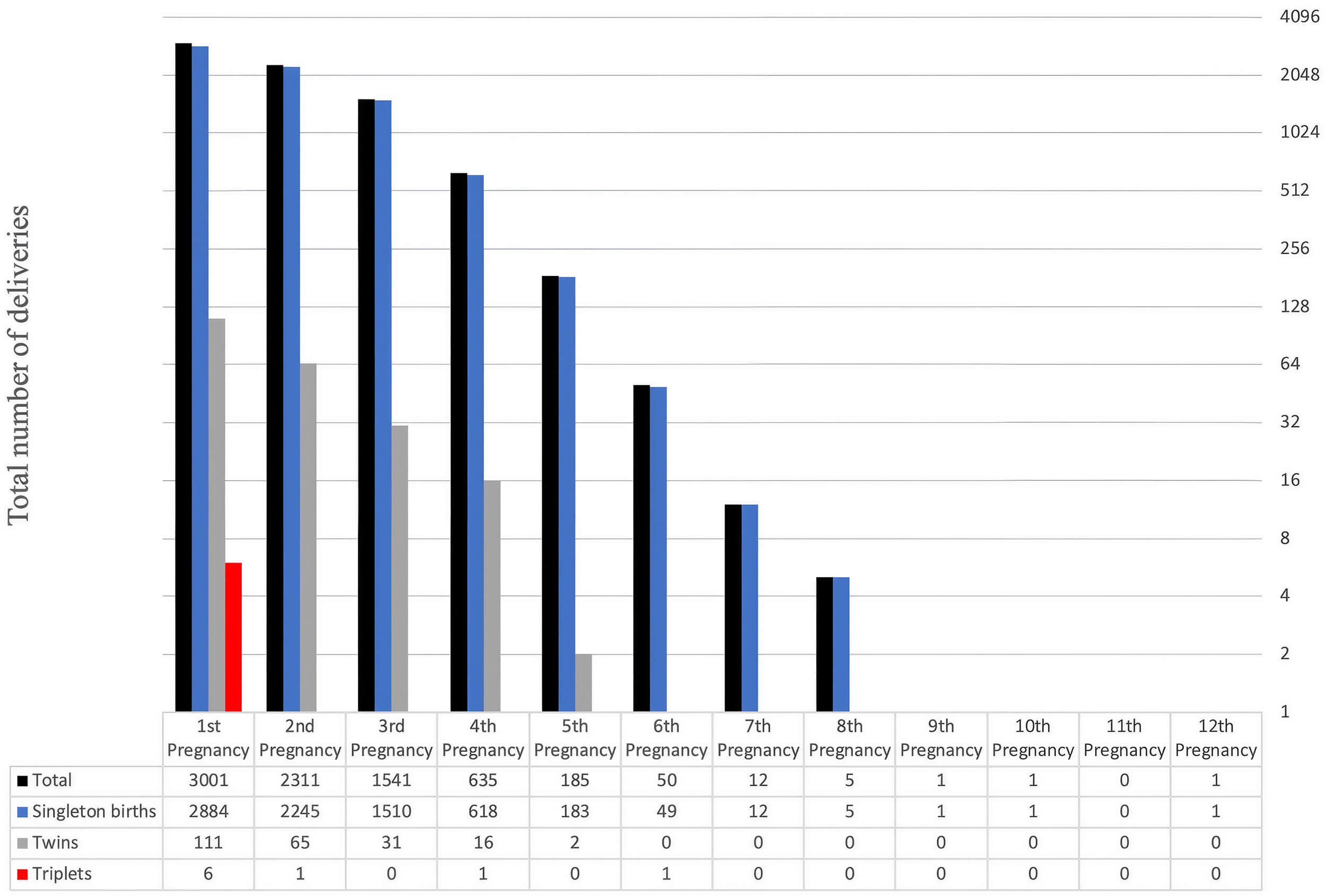 Fig. 2.
Fig. 2.
Distribution of birth multiplicity by gravidity. The figure shows the number of fetuses per pregnancy, categorized as singleton, twin, and triplet births, based on pregnancy order. The most frequent result of all pregnancies occurs as singleton births. The occurrence of twins primarily occurred in early pregnancies and became extremely rare after the fourth pregnancy. Triplet births remained extremely rare because they usualy occur during the initial pregnancy order. Delivery counts decreased progressively with increasing pregnancy order, while multiple births became increasingly rare. Counts represent the number of deliveries.
The study substantiates that singleton births are the predominant throughout a woman’s reproductive years, irrespective of the number of pregnancies. The probability of multiple births diminishes considerably with each successive pregnancy. The data also indicate that a limited number of women have more than four children.
The mean maternal age increased progressively with higher pregnancy orders. The average maternal age at first delivery was 27.3 years and increased with each subsequent pregnancy, reaching the highest mean value at the tenth pregnancy order (43.0 years). Fluctuations observed in the highest pregnancy orders reflected the small numbers of deliveries within these categories (Fig. 3).
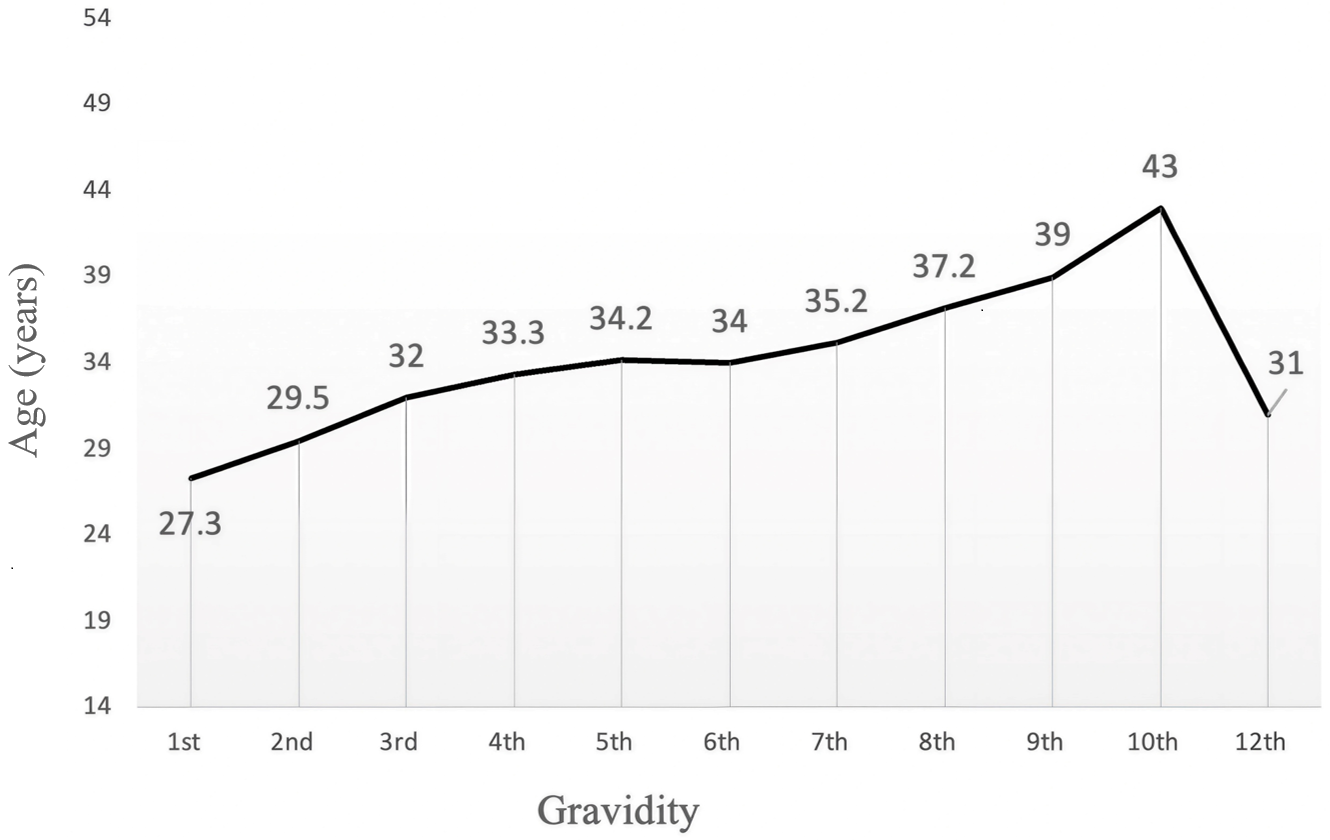 Fig. 3.
Fig. 3.
Mean maternal age at delivery by gravidity. The figure presents maternal age distribution for each pregnancy order. Maternal average age increased steadily with each pregnancy, beginning at 27.3 years during the first pregnancy order. The highest average maternal age was observed in the 10th pregnancy, at 43.0 years old. The data indicate that women tend to have higher-order pregnancies during their later reproductive years. The average maternal age drops to 31.0 years during the 12th pregnancy, reflecting the small number of recorded cases at this level and does not represent the typical pattern.
PP was identified in 52 of 7743 deliveries, corresponding to an incidence of 0.67%. All deliveries complicated by PP were performed by cesarean section, consistent with standard obstetric practice. Among deliveries without PP, both vaginal and cesarean deliveries were observed (Fig. 4). This highlights the critical role of clinical judgment in obstetrics. The consistency of our findings with clinical guidelines [e.g., American College of Obstetriciants and Gynecologists (ACOG) recommendations] strengthens their validity and reliability.
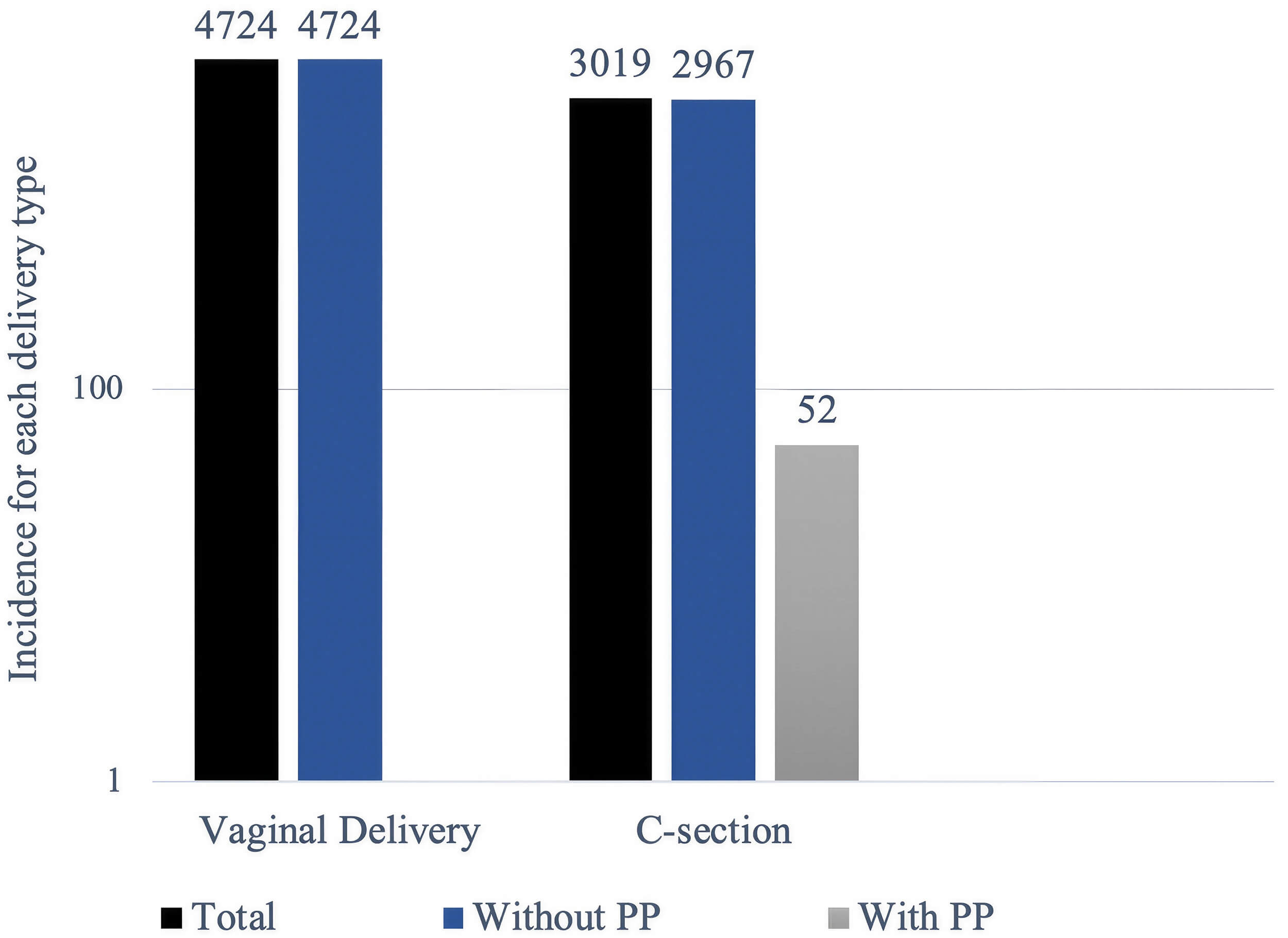 Fig. 4.
Fig. 4.
Mode of delivery among placenta previa (PP) and non-PP deliveries. The figure shows the distribution of vaginal births and cesarean sections per pregnancies with and without PP. The majority of deliveries in the overall population (n = 4724) involved vaginal delivery, whereas all PP required surgical intervention. The total number of cesarean sections was 3019, of which 52 involved a PP diagnosis. These findings demonstrate a strong clinical preference for cesarean delivery, with cesarean section used as the standard approach to protect both mother and child. Counts represent the number of deliveries. C-section, Caesarean section.
Several subtypes of PP have been described [8]. Among the 52 PP cases, central PP was the most frequent subtype (n = 35; 67.3%), followed by marginal (n = 13; 25.0%), partial (n = 3; 5.8%), and low-lying placenta (n = 1; 1.9%) (Fig. 5).
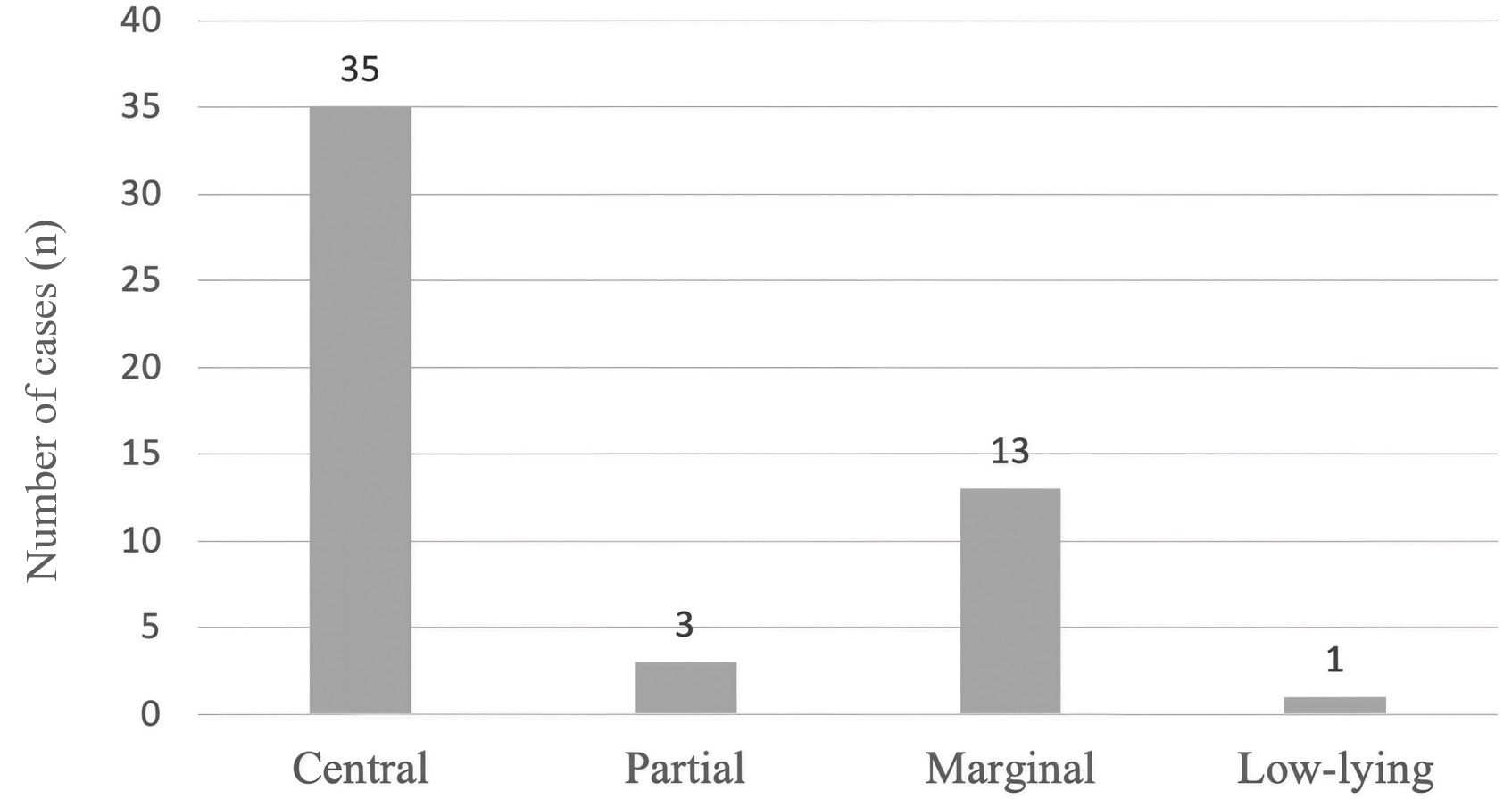 Fig. 5.
Fig. 5.
Distribution of PP subtypes among affected deliveries. Figure shows the distribution of PP subtypes among the 52 cases identified in this study. Central PP was the most common subtype (n = 35). Central PP, in which the placenta completely covers the cervical opening, carries the highest risk and almost typically requires cesarean delivery. Marginal PP, in which the placenta reaches the edge of the cervix without covering it, follows with 13 cases, while partial previa is much less common (3 cases). Low-lying placenta, in which the placenta is near but not touching the cervix, is the rarest in this dataset, with just 1 case.
Total abdominal hysterectomy (TAH) was performed in 6 cases, all of which occurred in women with central PP. No hysterectomies were performed in cases of marginal, partial, or low-lying PP (Fig. 6).
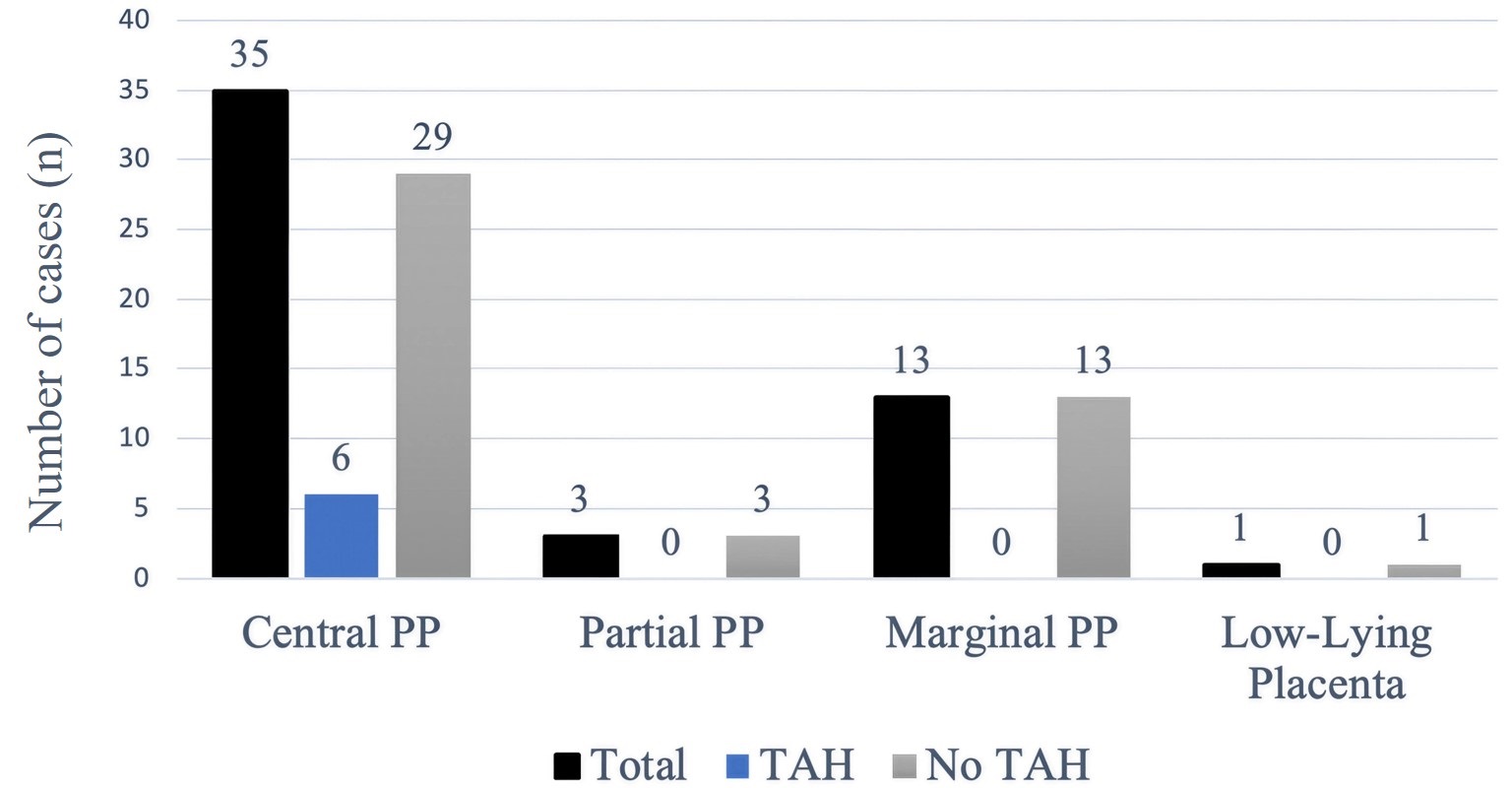 Fig. 6.
Fig. 6.
Distribution of PP subtypes according to hysterectomy status. The figure shows the relationship between PP subtype and the need for TAH. TAH represents a major surgical procedure for uterus removal and is performed when obstetric bleeding becomes unmanageable. Central PP, in which the placenta fully covers the birth canal, was the most frequent subtype (n = 35 cases) and led to the highest number of TAH procedures (6 women needed this surgery). The remaining PP types, including partial, marginal, and low-lying placenta, did not require any TAH procedures. The medical team managed these cases without needing TAH since no patient required this procedure. The medical team treated these cases with less invasive methods, which allowed all mothers to preserve their uterus, especially important for women who wish to maintain future fertility or prevent hysterectomy-related psychological distress. TAH, total abdominal hysterectomy.
Advanced maternal age (
| Delivery range | ||||||
| 1st pregnancy | 2nd pregnancy | 3rd pregnancy | 4th pregnancy | 5th pregnancy | ||
| Maternal age | 0 | 0 | 0 | 0 | 0 | |
| 20–29 years old | 3 | 6 | 2 | 0 | 0 | |
| 30–39 years old | 7 | 11 | 9 | 4 | 0 | |
| 2 | 2 | 2 | 3 | 1 | ||
| Total | 12 | 19 | 13 | 7 | 1 | |
| 52 | ||||||
Certain risk factors have been reported to increase the chances of developing PP [9, 10, 11]. Maternal and obstetric characteristics observed among PP cases are summarized in Table 2.
| Coexisting characteristics/conditions | Frequency | |
| n | % | |
| Maternal age |
41 | 78.8% |
| Prior cesarean section | 22 | 42.3% |
| Prior habitual abortions | 7 | 13.5% |
| Prior diagnosed infertility | 5 | 9.6% |
| Prior in vitro fertilization | 3 | 5.8% |
| Prior myomectomy | 2 | 3.8% |
| Prior cystectomy | 2 | 3.8% |
*Patients may have more than one coexisting characteristic; therefore, percentages do not sum to 100%. Values are presented as number (percentage). Observed characteristics are descriptive and do not represent independent risk factors. n, number of cases.
Advanced maternal age (
This retrospective observational study provides descriptive and comparative insights into birth patterns and the clinical characteristics of PP in a tertiary care center in Kosova. Overall, the analysis confirms several trends consistent with global reproductive patterns, including a progressive decline in birth frequency with increasing pregnancy order, a predominance of singleton births, and stable sex ratios across pregnancy orders [7]. The observed increase in maternal age with higher pregnancy orders reflects both biological factors and societal trends, including later-life childbearing and evolving family planning practices. These findings emphasize the importance of understanding local demographic patterns to guide prenatal care planning.
The overall incidence of PP in this cohort was 0.67%, consistent with previously reported global ranges of 0.3–0.8% [2]. Central PP was the most common subtype, accounting for 67.3% of PP cases. All women with central PP underwent cesarean delivery, and 6 cases (17.1%) involved hysterectomy. Given the small number of hysterectomy cases and the lack of pathological confirmation of PAS, these findings should be interpreted descriptively, without implying causality. The absence of hysterectomy in marginal, partial, and low-lying PP cases highlights the variability in clinical severity and the potential for fertility preservation in less severe presentations.
Advanced maternal age (
From a clinical perspective, these findings reinforce the importance of early detection of PP, careful prenatal monitoring, and appropriate planning for cesarean delivery. They also underline the need for early diagnosis, multidisciplinary treatment, and preparedness for surgical procedures in resource-limited settings [1]. The absence of hysterectomies in marginal, partial, and low-lying PP cases further underscores the range of severity associated with PP subtypes and the possibility for fertility preservation in less severe forms. This potential for fertility preservation in less severe types highlights the necessity for advanced treatment approaches and careful monitoring during pregnancy. By understanding the varying degrees of PP and their accompanying risks, healthcare providers can better assist affected women and improve outcomes for both mother and child.
Finally, this study provides population-specific descriptive data from Kosova, a region with limited hospital-based epidemiological information on PP. These findings may support regional antenatal care planning and contribute to the understanding of clinical characteristics of PP in Southeast European populations.
This study has several important limitations that should be considered when interpreting the findings. The study design is descriptive, and the absence of a non-PP comparison group limits the ability to estimate effect measures, test hypotheses, or draw conclusions about risk factors. Furthermore, the assessment of outcomes related to PAS and hysterectomy was constrained by incomplete documentation and a small number of events. Therefore, these findings should be interpreted cautiously and considered descriptive observations.
In this large single-center study, PP was uncommon and predominantly presented as central PP, which was associated with cesarean delivery in all cases. Maternal characteristics more frequently observed among women with PP included advanced age and a history of cesarean delivery. Furthermore, hysterectomy occurred in a small number of central PP cases and should be interpreted descriptively, without implying causality or generalizability. These findings emphasize the importance of careful prenatal surveillance, delivery planning, and individualized clinical management in pregnancies complicated by PP.
The data supporting the findings of this study are available from the first author (Berat Krasniqi) upon reasonable request.
BK, ST and MS designed the research study. BK, DL, ST, and DD performed the research. BK and MS provided help and advice on the research. DL and DD analyzed the data. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the Medical Faculty at the University of Prishtina (approval number: 217/2024).
All the authors are very grateful for the support provided by the University of Prishtina and UCCK.
This research received no external funding.
The authors declare no conflict of interest.
During the preparation of this work, the authors used “Grammarly” in order to check spelling and grammar. After using this tool, the authors reviewed and edited the content as needed. The author takes full responsibility for the content of the publication.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.