



 , Linling Zhu 1,†, Dingheng Li 1, Hao Chen 2,*
, Linling Zhu 1,†, Dingheng Li 1, Hao Chen 2,*
1 Department of Gynecology, Hangzhou Women’s Hospital, 310008 Hangzhou, Zhejiang, China
2 Department of Pathology, Hangzhou Women’s Hospital, 310008 Hangzhou, Zhejiang, China
†These authors contributed equally.
Abstract
Pseudomyxoma peritonei (PMP) is a rare peritoneal malignancy that is typically managed with cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC). However, prolonged abdominal drainage in these patients may lead to catheter entrapment due to encapsulation by fibrous tissue.
A 48-year-old patient with PMP underwent CRS with placement of an abdominal drain. On postoperative day 10, the drain was found to be entrapped, and multiple removal attempts failed due to significant resistance and patient discomfort. To avoid reoperation, a 5 mm hysteroscope served as an endoscopic platform. It was introduced through the drainage lumen, which allowed precise dissection of the encapsulating fibrous tissue under direct visualization and subsequent successful tube removal. Histopathologic examination confirmed the presence of fibrotic tissue with inflammatory infiltration.
To our knowledge, this report is the first to describe the endoscopic management of an entrapped abdominal drain via the drain lumen, establishing this approach as a viable and minimally invasive alternative to reoperation. This case further highlights the need to reconsider drain design in patients with PMP, who show a predisposition to this complication due to intense fibrogenesis.
Keywords
- pseudomyxoma peritonei
- hysteroscopy
- entrapment
- abdominal drainage
- minimally invasive surgery
- endoscopy
Pseudomyxoma peritonei (PMP) is a rare and complex disease characterized by the progressive accumulation of mucinous ascites within the peritoneal cavity [1], most commonly originating from appendiceal or ovarian mucinous neoplasms [2]. Despite its histologically low-grade appearance, the disease exhibits a pronounced tendency for diffuse peritoneal dissemination. Current management relies on cytoreductive surgery (CRS) combined with hyperthermic intraperitoneal chemotherapy (HIPEC). This approach aims to eliminate both macroscopic tumor deposits and microscopic residual disease [3, 4]. The postoperative course in patients with PMP often requires prolonged abdominal drainage to support recovery and facilitate subsequent HIPEC. However, extended drainage carries a risk of catheter entrapment, wherein the tube becomes progressively encased by fibrous tissue within the abdominal cavity. This condition can cause significant patient discomfort and complicate drain removal. Conventional management typically involves reoperation, which increases risks and prolongs recovery time.
The hysteroscope, an endoscopic platform with a small diameter, flexibility, and high-resolution optics, offers distinct advantages for complex surgical challenges [5]. Herein, we present a case of a patient with PMP who developed an entrapped abdominal drain following CRS. After multiple extraction methods failed, we utilized the hysteroscope as a readily available endoscopic platform to dissect the embedded tissue under direct visualization and remove the tube. This experience illustrates the potential of repurposing established endoscopic equipment for novel clinical challenges, highlighting the clinical value of minimally invasive strategies in optimizing patient recovery.
A 48-year-old woman (body mass index [BMI] 22.4 kg/m2), with no significant surgical history or comorbidities underwent complete CRS for PMP. Intraoperative exploration revealed approximately 500 mL of gelatinous ascites and extensive peritoneal dissemination. Numerous miliary implants involved the omentum, visceral peritoneum, and bowel surfaces. Adhesiolysis was required due to dense adhesions throughout the abdominal cavity. The CRS procedure then encompassed a comprehensive resection of all involved tissues, including omentectomy, appendectomy, total hysterectomy with bilateral salpingo-oophorectomy, pelvic lymph node dissection, and peritonectomy. Following thorough lavage and hemostasis, a cribriform pelvic drainage tube (model: M10B; diameter: 1 cm; material: medical-grade silicone; manufacturer: Guangdong XianLai Medical Equipment Co., Ltd., Maoming, Guangdong, China; website: http://sunlightmed.cn/; lot No.: 20210301; Fig. 1) was placed in the left pelvic cavity. The tube was positioned along the left paracolic gutter, with its tip in the pouch of Douglas, and secured to the skin with sutures. Pathological examination confirmed a low-grade mucinous neoplasm of appendiceal origin.
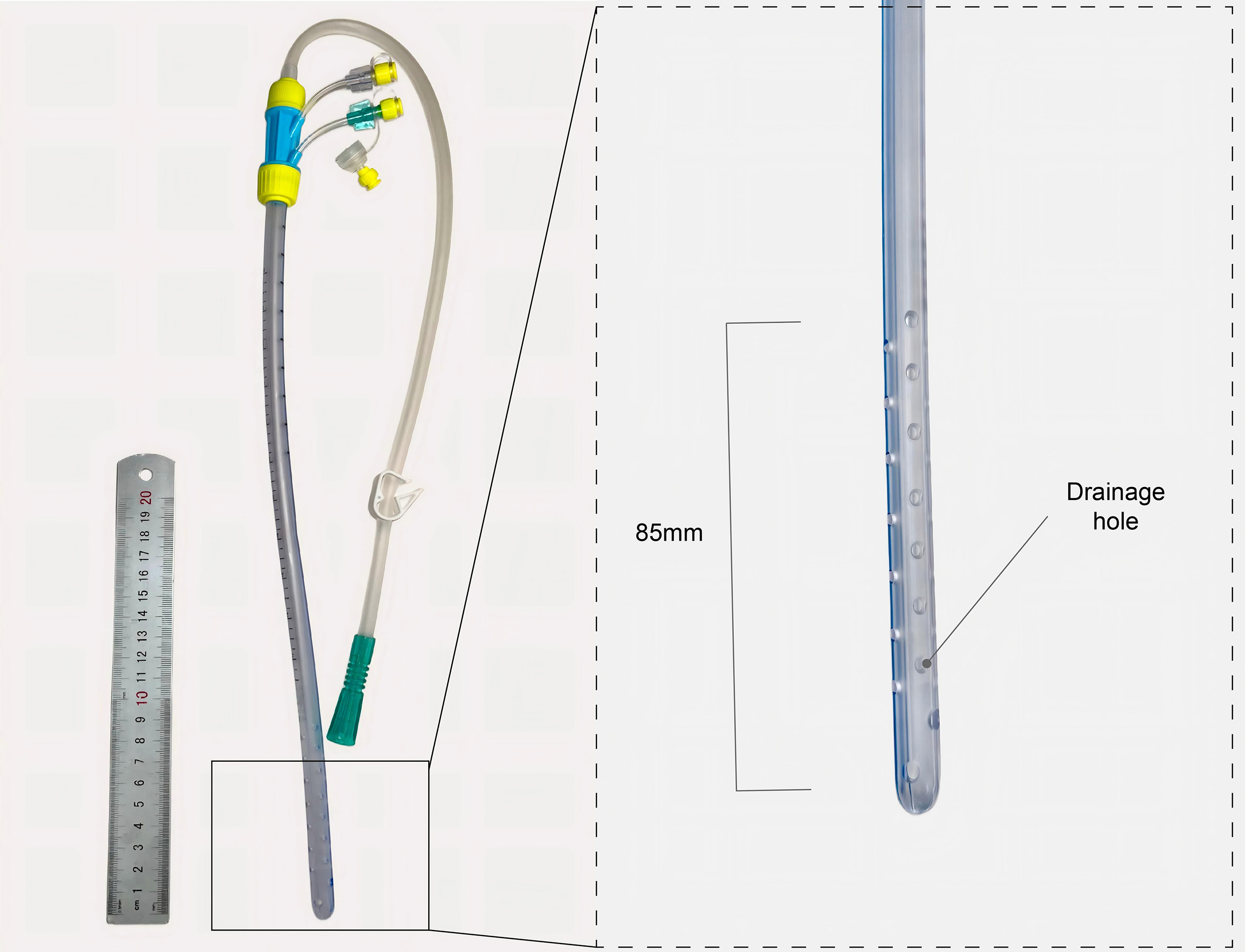 Fig. 1.
Fig. 1.
Cribriform drainage tube used in the case.
By postoperative day 10, the patient was asymptomatic and showed no drain
output. During attempted removal, the cribriform drain was found to be firmly
entrapped within the abdominal cavity. Multiple methods were attempted to remove
the tube, including manual compression, saline flushing, and gentle traction.
However, all attempts failed due to significant resistance and severe pain.
Bedside ultrasonography revealed a 2.4
To avoid reoperation, we performed transluminal endoscopic removal under conscious sedation in the operating room. We utilized a 5-mm office hysteroscope (GIMMI Office Hysteroscopy; GIMMI GmbH, Tuttlingen, Germany; www.gimmi.com) for its narrow diameter, which allowed direct introduction through the existing drain lumen—a route not feasible with a standard 10-mm laparoscope (Fig. 2A). The external portion of the tube was transected, and the endoscope was advanced without distension medium. Endoscopic examination identified fibrotic tissue entrapped within the cribriform openings (Fig. 2B), with no evidence of intestinal involvement. Video 1 demonstrates the key steps of the subsequent dissection and removal. Under direct visualization, the adherent tissue was dissected and removed using hysteroscopic scissors and grasping forceps, enabling complete and uneventful extraction of the drain (Fig. 2C). The total procedure lasted 15 minutes, with an estimated blood loss of 5 mL. The patient was monitored for two hours post-procedure and reported no abdominal pain or other complications. Repeat ultrasonography confirmed the absence of hemoperitoneum.
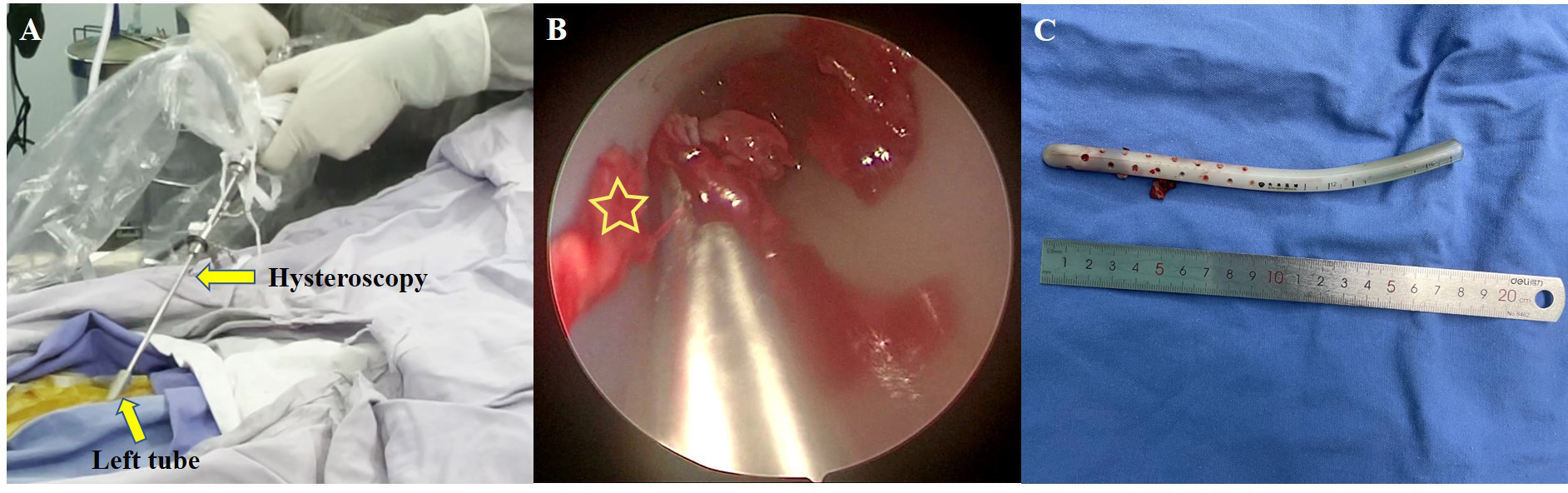 Fig. 2.
Fig. 2.
Endoscopic removal process. (A) Hysteroscope advanced through the drainage tube lumen (arrow). (B) Endoscopic view showing fibrous tissue (asterisk) entrapped within the tube’s side holes. (C) Extracted drainage tube.
Endoscopic view during removal of the entrapped abdominal drain. The image clearly shows fibrous tissue entrapped within the cribriform openings. Video associated with this article can be found, in the online version, at https://doi.org/10.31083/CEOG46511.
Pathological examination of the retrieved tissue confirmed fibrous stroma infiltrated by lymphocytes, plasma cells, and eosinophils, alongside areas of mucin deposition and collagenization. These findings indicated an encapsulating process dominated by fibrocollagenous proliferation (Fig. 3).
 Fig. 3.
Fig. 3.
Histopathology of tissue from the drainage tube
(Original magnification: 20
The patient had an uneventful recovery and was discharged on postoperative day 12 following the initial CRS, 2 days following drain removal. The abdominal incisions were healed well, with no signs of infection. As the patient declined HIPEC, no further drainage was required. At 3-year follow-up, she remained asymptomatic, with no clinical or radiological evidence of tumor recurrence.
Postoperative drain or HIPEC catheter entrapment represents a significant, yet frequently underestimated, challenge in managing PMP [6]. Our case demonstrates that drain entrapment can occur even in the absence of HIPEC, underscoring its direct association with the disease’s underlying pathophysiology. The propensity for drain entrapment in patients with PMP is multifactorial and stems from the disease’s unique biological environment. The primary contributing factors include: (1) histologically, low-grade PMP is characterized by band-like or island-like tumor architecture, sparse cellularity, and mild dysplasia, producing highly viscous and gelatinous ascites that readily congeal and obstruct the drainage tube [7]; and (2) vascular changes, including endothelial injury and inflammation, further promote adhesion of surrounding substances, thereby increasing the risk of drain entrapment [8].
Furthermore, drain design may affect the risk of entrapment. The cribriform pattern of side holes, while intended to improve drainage efficiency, creates anchor points for tissue ingrowth. In the profibrotic environment of PMP, this design facilitates robust tissue incorporation by providing a scaffold for mature fibrous tissue formation. This case supports consideration of smoother, less perforated tube designs to potentially reduce the incidence of entrapment in these patients. Beyond physical design, adjunct measures such as early ambulation, timely tube removal, prophylactic low-molecular-weight heparin administration, and aseptic flushing may further reduce adhesion risks [6]. These clinical strategies, however, require validation in dedicated cohort studies.
Despite the clinical significance of this complication, evidence regarding optimal management of entrapped drains remains limited. Standard practice often requires reoperation [9, 10], which carries risks of increased morbidity, delayed recovery, and extensive surgical trauma. In our case, conventional methods such as flushing and traction failed. This failure likely reflects the unique mechanical challenge posed by extensive tissue ingrowth through the cribriform openings, creating a firm interlock that cannot be disrupted by noninvasive methods.
The hysteroscope, repurposed from its traditional gynecological applications, proved effective as an endoscopic platform for managing this complex intra-abdominal complication. Its small diameter, flexibility, and high-resolution imaging enabled precise visualization and management of the entrapped drain. Using this endoscopic approach, we successfully visualized the embedded tissue, dissected it under direct vision, and completed tube extraction without the need for formal reoperation. This minimally invasive strategy reduced patient discomfort and minimized the risk of additional complications. Although other ultra-slim endoscopes, such as ureteroscopes or cystoscopes, could theoretically provide similar access, the hysteroscope represents the most readily available and functionally suitable system within our gynecological specialty unit.
This novel application demonstrates the potential to adapt established endoscopic equipment for managing complex postoperative scenarios. It suggests that, in cases where conventional extraction fails, a minimally invasive endoscopic approach tailored to available institutional resources can effectively prevent the need for reoperation. Future comparative studies of different endoscopic platforms for managing similar complications could help establish standardized recommendations.
It is paramount to emphasize that this endoscopic technique is contraindicated if there is any suspicion of bowel involvement. Preoperative ultrasonography is essential to exclude this scenario, and the procedure must be halted immediately if visual inspection reveals any tissue resembling intestinal mucosa or if the findings are ambiguous. In such cases, laparoscopic or open surgical exploration remains the standard of care.
However, several limitations must also be acknowledged. First, this endoscopic approach requires specialized equipment (e.g., 4- or 5-mm 30° hysteroscope) and surgical expertise, which may be not be available in resource-limited settings. Second, as a single case, the generalizability of this technique requires validation in larger patient cohorts. Finally, the patient had not received HIPEC. The definitive diagnosis was established during CRS at our gynecological specialty center, which does not have HIPEC capabilities. The patient declined postoperative referral to a specialized cancer center for HIPEC. This deviation from the standard PMP management protocol may influence long-term oncological outcomes, although it does not diminish the technical success and immediate clinical benefits of the endoscopic approach described.
This endoscopic approach provides an effective, minimally invasive strategy for managing entrapped abdominal drainage tubes in patients with PMP. This technique allows precise dissection under direct visualization while avoiding the need for reoperation. As the first reported use of transluminal endoscopy for this specific complication, it represents a valuable clinical alternative when conventional methods fail. This case demonstrates the potential to adapt established endoscopic techniques for managing complex surgical scenarios.
PMP, pseudomyxoma peritonei; CRS, cytoreductive surgery; HIPEC, hyperthermic intraperitoneal chemotherapy.
All data in this manuscript can be made available based on reasonable request to the corresponding author.
YD and LZ designed the study and drafted the original manuscript. DL performed the research. HC contributed to the acquisition, analysis, and interpretation of the histopathological data and to the critical review and editing of the manuscript. All authors contributed to editorial changes in the manuscript. All authors read and approved the final version of the manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was conducted in accordance with the Declaration of Helsinki. The research protocol was approved by the Ethics Committee of Hangzhou Women’s Hospital (Ethic approval number: 2025-A-97), and all participants provided written informed consent.
Not applicable.
This research was funded by the Zhejiang Provincial Medical and Health Technology Plan (2022RC236, 2023KY205) and the Hangzhou Municipal Special Fund for the Development of the Biomedicine and Health Industry (2023WJC327).
The authors declare no conflict of interest.
During the preparation of this work, the authors used ChatGPT-3.5 in order to check spell and grammar. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/CEOG46511.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.